





Tirzepatide and Semaglutide: Impact on OSA in Obesity
Tirzepatide and Semaglutide for the Treatment of Obstructive Sleep Apnea and Obesity: A Retrospective Analysis
Onur Baser1, Yuanqing Lu2, Shuangrui Chen2, Erdem Baser3
OPEN ACCESS
PUBLISHED: 31 January 2025
CITATION: Baser, O., Lu, Y., et al., 2025. Tirzepatide and Semaglutide for the Treatment of Obstructive Sleep Apnea and Obesity: A Retrospective Analysis. Medical Research Archives, [online] 13(1). https://doi.org/10.18103/mra.v13i1.6236
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i1.6236
ISSN 2375-1924
Abstract
Background: Obesity is the leading risk factor for obstructive sleep apnea. Weight loss can improve both sleep quality and overall health. New anti-obesity medications (AOMs), including semaglutide and tirzepatide, offer promising options for managing obesity and may be potential treatment options for obstructive sleep apnea.
Methods: We conducted a retrospective claims analysis using Kythera Labs data from November 2022 to June 2024. Patients with obesity and evidence of AOM utilization were identified based on diagnosis and prescription claim(s) for Zepbound or Wegovy (identification period, 1 Nov. 2023–31 Dec. 2023) and had at least 6 months to measure incidence of obstructive sleep apnea. Patients with obesity were classified into two cohorts: an AOM cohort that received tirzepatide (Zepbound) or semaglutide (Wegovy) during the identification period (index date = first AOM claim) and a non-AOM cohort with no evidence of AOM use during the study period. Random index dates were selected within the AOM cohort’s range and included a 1% random sample of eligible patients. OSA risk was assessed during the follow-up period using Cox regression.
Results: We identified 20,384 patients with obesity and AOM use (semaglutide, 17,859; tirzepatide, 2,525) and 85,018 patients with obesity in the non-AOM cohort. Compared with the non-AOM cohort, the AOM cohort had a higher percentage with a Chronic Disease Score ≥2 (52.25% vs 8.44%; p<.001). However, the incidence of obstructive sleep apnea was lower in the AOM cohort (3.12%) than the non-AOM cohort (12.56%; p<.001). Subgroup analysis of the AOM cohort showed that tirzepatide users had a slightly lower incidence of obstructive sleep apnea than semaglutide users (2.65% vs 3.18%) (p=.0303). After adjusting for sociodemographic and clinical characteristics, the AOM cohort showed a 40% lower likelihood of obstructive sleep apnea than the non-AOM cohort (hazard ratio=0.60, p<.0001). However, there was no statistically significant difference in the risk of obstructive sleep apnea between tirzepatide and semaglutide users (p=.1664).
Conclusions: This study reveals a significant association between AOM use and a lowered risk of obstructive sleep apnea after adjustment for demographic and clinical variables.
Keywords: obstructive sleep apnea, anti-obesity medications, obesity, tirzepatide, semaglutide
Introduction
Obstructive sleep apnea and obesity are two interrelated health conditions that have become increasingly prevalent worldwide, posing significant public health challenges. Obstructive sleep apnea is characterized by recurrent episodes of upper airway collapse during sleep, leading to intermittent hypoxia and sleep fragmentation. The prevalence of OSA has risen in parallel with the global obesity epidemic, suggesting a strong association between these two conditions. In the adult population, the prevalence of OSA is estimated to be 25% and as high as 45% in subjects with obesity. The elevated prevalence of OSA in individuals with obesity extends to the pediatric population, with recent data revealing a 46% prevalence among children with obesity compared with 33% in children from general pediatric clinics. Obesity is a major risk factor for the development and progression of OSA. For every 10% increase in body weight, the risk of OSA increases six-fold. In obese individuals, excess adipose tissue around the pharyngeal airway reduces the airway lumen size and increases its propensity for collapse during sleep. Additionally, obesity alters upper airway muscle function and lung volumes, further contributing to airway instability. A 10% weight loss can result in a more than 20% improvement in OSA severity. Conversely, OSA may contribute to weight gain and obesity through various mechanisms, including disruption of appetite-regulating hormones and reduced physical activity due to fatigue. This bidirectional relationship creates a vicious cycle that can exacerbate both conditions.
The understanding of OSA and its implications on disease pathophysiology has undergone rapid evolution in recent years. Current evidence suggests that OSA exerts deleterious effects on multiple organ systems, with particular relevance to cardiovascular disease. Notably, OSA has been implicated in the etiology of hypertension. Furthermore, it has been associated with the progression of several established medical conditions, including congestive heart failure, atrial fibrillation, diabetes mellitus, and pulmonary hypertension. Based on the available research and recent developments, it appears that both direct pharmacological effects and indirect effects through weight loss can improve sleep apnea. However, the most significant advancements have been made in the realm of weight loss drugs that indirectly impact sleep apnea. In particular, recent advancements in pharmacological interventions for obesity have shown promising results in addressing OSA indirectly. Tirzepatide, a novel dual GIP and GLP-1 receptor agonist, has demonstrated significant efficacy in reducing sleep apnea severity in adults with OSA and obesity. In clinical trials, tirzepatide achieved a mean apnea-hypopnea index reduction of up to 63%, with meaningful improvements in sleep apnea symptoms both with and without positive airway pressure therapy. Similarly, semaglutide, another GLP-1 receptor agonist, has shown potential in weight management and may have implications for OSA treatment. This retrospective analysis aims to examine the effects of tirzepatide and semaglutide on OSA and obesity, exploring their potential as novel therapeutic options for managing these interconnected health challenges.
Methods
We conducted a retrospective cohort study using Kythera Medicare closed claims data from 1 November 2022 to 1 June 2024. Kythera data include medical and claims information with 79% coverage of all U.S. patients, available in both open-claims and closed-claims versions. This data set encompasses approximately 310 million patients, 6.1 million practitioners, 1.6 million organizations, and 1.4 million facilities, generating 40 billion healthcare claims. While Kythera includes commercial, Medicare, and Medicaid patients, this study focused on the commercial segment, which randomly included 170 million total commercial enrollees. The data included unique de-identified patient numbers, age, gender, types of insurance (Fee-for-Service vs. managed care), zip codes, diagnoses according to the International Classification of Diseases (ICD-10), Current Procedural Terminology codes, and National Drug Codes for medications. Each patient is assigned a unique identifier, linking all encounters and enabling longitudinal analysis. The details of the data have been published elsewhere, and the healthcare outcomes derived from these data were compared with other data sets for validity and consistency.
Study design is presented in Figure 1. We identified two cohorts: patients with obesity using tirzepatide (Zepbound) or, semaglutide (Wegovy) and a randomly chosen 1% of patients with obesity who did not use any medical therapy for obesity. For the anti-obesity medication (AOM) cohort, patients who had one or more pharmacy claims for Zepbound or Wegovy between 1 November 2023, and 31 December 2023, were identified (identification period). The first prescription claim was considered the treatment initiation date for the AOM group. We also included patients with at least one claim with a diagnosis of obesity (ICD-10 CM: E66.9, E66.09, E66.1, E66.8, and Z68.3) before the index date and continuous medical and pharmacy benefits for 12 months pre-index date. For the non-AOM group, patients with at least one claim for obesity diagnosis were identified between 1 November 2023, and 31 December 2023. Patients included in this group had continuous medical and pharmacy benefits for 12 months pre-index date. The index date was randomly assigned for patients with obesity in the non-AOM group.
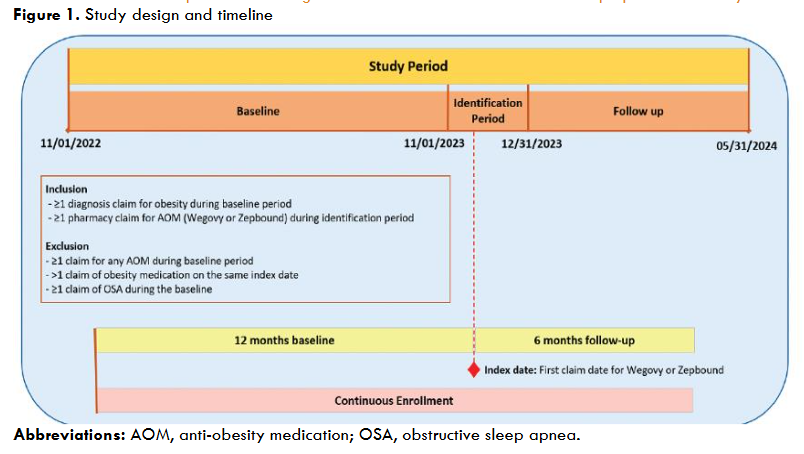
The AOM group excluded patients prescribed obesity medications during the baseline period, those with multiple AOM claims on the index date, and individuals with sleep apnea during baseline. Similarly, the non-AOM group excluded patients prescribed obesity medications throughout the study period, as well as those with sleep apnea at baseline. To manage sample size, 1% of eligible non-AOM patients were randomly selected for the final cohort. Excluded obesity medications for both groups encompassed orlistat, phentermine/topiramate, naltrexone/bupropion, and surgical interventions such as endoscopic sleeve gastroplasty, intragastric balloon placement, adjustable gastric banding, gastric sleeve, and gastric bypass. Diabetes was identified using ICD-10-CM codes (E11.44, E11.8, E11.649, E11.65, E11.9) during the baseline period, while OSA was diagnosed in both cohorts during follow-up using ICD-10-CM codes M15, M16, M17, M18, and M19.
At baseline (1 October 2022–31 November 1, 2023), several clinical and demographic factors were examined. The relevant fields in the Kythera commercial claims data served as the basis for the gender (female or male) and age (18–40, 41–60, 61–80, and ≥80 years) categories. We applied a previously established summary measure of socioeconomic status (SES) for each U.S. zip code with information on income, education, and occupation from the 5-year estimates for the U.S. Census data for 2021. Subjects were sorted and categorized into terciles (low, medium, and high) based on their summary SES scores. To account for variations in total comorbidities between patients, the updated Charlson Comorbidity Index (CCI), Elixhauser Index, and Chronic Disease Score (CDS) were used. The CCI is a weighted index that predicts the one-year mortality risk for patients with various comorbid conditions, assigning scores to different medical conditions and summing them to provide a total score that reflects the patient’s overall comorbidity burden. The CDS is a well-established measure of overall comorbidity based on current medication use. The score rises as more chronic diseases are being treated and the treatment plan becomes more complicated. The Elixhauser Comorbidity Index is a comprehensive measure of patient comorbidities used in healthcare to predict various outcomes and assess the overall severity of a patient’s condition. The higher the score, the higher the predicted hospital resource use and mortality rate. Comorbidities specific to OSA such as hypertension, hyperlipidemia, diabetes, cardiovascular disease, chronic obstructive pulmonary disease (COPD), depression, gastroesophageal reflux disease, metabolic disorders, somnolence, and stroke were identified using appropriate ICD-10 codes.
The groups were analyzed descriptively by demographic and clinical variables at baseline. A subgroup analysis was conducted by comparing the variables by medication type (i.e., Zepbound or Wegovy). For categorical variables, numbers and percentages were given; for continuous variables, means and standard deviations were given. For continuous and categorical variables, Student’s t-tests and Pearson chi-square tests were employed, respectively, to assess if there were statistically significant differences between the cohorts at the 5% level. Standardized differences were computed for each variable.
During the follow-up period, the incidence of OSA and the risk of OSA between the cohorts were determined. The follow-up period was defined as the period from the index date to the end of the study period. The Cox regression model and Aalen’s additive regression model were utilized to compare the risk of OSA between the groups. The Cox regression model, a predominant approach for time-to-event analysis, operates under the assumption that the treatment effect on the likelihood of OSA is proportional over time. To explore whether the treatment effect exhibits an additive nature, which implies temporal variation, Aalen’s model was also employed in the analysis. The conventional Cox analysis does not provide insights into additive effects, potentially leading to the loss of valuable information and the masking of significant effects. For example, a treatment’s impact on the development of OSA might not appear significant in a Cox analysis; however, an additive model could reveal a significant effect during the first year, which subsequently diminishes in later years. Likelihood ratio tests were employed to compare differences between two groups, and Wald tests were utilized to compare differences between three or more groups. All analyses were conducted using Pyspark and SparkR on Databricks and the R software package.
Results
We identified 20,384 patients with obesity and AOM use (semaglutide: 17,859; tirzepatide: 2,525) and 85,018 patients with obesity in the non-AOM cohort.
| Cohort | Patients |
|---|---|
| AOM | 20,384 |
| Non-AOM | 85,018 |
The average patient age was 45.49 years in the AOM cohort and 51.14 years in the non-AOM group (p < .0001). Both cohorts had a higher proportion of female patients (82.53% vs. 58.73%, p < .0001). High-comorbidity patients were defined as those with a comorbidity score of ≥2. Individuals in the AOM cohort had a significantly higher proportion of patients with a high CCI (6.71% vs. 5.23%, p < .0001), CDS (52.25% vs. 8.44%, p < .0001) and Elixhauser Score (61.94% vs. 15.81%, p < .0001). The AOM cohorts tended to live in higher SES score areas than the non-AOM cohort 37.61% vs. 32.29%, p < .0001). The most prevalent baseline OSA-related comorbidity in both the AOM and non-AOM groups was hypertension (33.84 % vs. 12.49%, p < .0001). The following comorbidities were found in greater proportions in patients receiving AOM than in those not on AOM: hypertension (33.84% vs 12.49%, p < .0001), depression (21.64% vs. 3.50%, p < .0001), hyperlipidemia (18.79% vs 6.24%, p < .0001), gastroesophageal reflux disease (16.58% vs 3.50%, p < .0001), COPD (11.79% vs 3.39%, p < .0001), cardiovascular disease (7.27% vs 4.28%, p < .0001), metabolic disorders (3.87% vs. 0.30%, p < .0001), somnolence (0.39% vs 0.04%, p < .0001), and Stroke (0.35% vs 0.21%, p = .0002). Nonetheless, diabetes (4.81% vs 6.58%, p < .0001) were found in greater proportion in patients in the non-semiglutide cohort than in the semaglutide cohort.
| Characteristics | With AOM (Wegovy or Zepbound) (N = 20,384) | Without AOM (N = 85,018) | P Value | Std. Diff. |
|---|---|---|---|---|
| Age, y (mean, SD) | 45.49 (12.45) | 51.14 (18.39) | <.0001 | 0.3247 |
| Age group, n (%) | 18-40 y 7,016 (34.42) | 18,948 (22.29) | <.0001 | 0.2833 |
| 41-60 y 10,821 (53.09) | 32,176 (37.85) | <.0001 | 0.3124 | |
| 61-80 y 2,349 (11.52) | 26,190 (30.81) | <.0001 | 0.4404 | |
| 80+ y 35 (0.17) | 3,663 (4.31) | <.0001 | 0.2257 | |
| Gender (n, %) | Male 3,562 (17.47) | 35,082 (41.26) | <.0001 | 0.5033 |
| Female 16,822 (82.53) | 49,935 (58.73) | <.0001 | 0.5034 | |
| Comorbidity scores (n, %) | Charlson Comorbidity Score ≥2 1,368 (6.71) | 4,446 (5.23) | <.0001 | 0.0649 |
| Chronic Disease Score ≥2 10,651 (52.25) | 7,174 (8.44) | <.0001 | 1.3176 | |
| Elixhauser Score ≥2 12,625 (61.94) | 13,441 (15.81) | <.0001 | 1.1794 | |
| SES (n, %) | Low 5,736 (28.14) | 28,412 (33.42) | <.0001 | 0.1129 |
| Medium 6,599 (32.37) | 27,438 (32.27) | 0.7834 | 0.0021 | |
| High 7,667 (37.61) | 27,452 (32.29) | <.0001 | 0.1130 | |
| Baseline OSA-related comorbidities (n, %) | Hypertension 6,898 (33.84) | 10,619 (12.49) | <.0001 | 0.5888 |
| Hyperlipidemia 3,831 (18.79) | 5,308 (6.24) | <.0001 | 0.4531 | |
| Diabetes 981 (4.81) | 5,594 (6.58) | <.0001 | 0.0731 | |
| Cardiovascular diseases 1,481 (7.27) | 3,635 (4.28) | <.0001 | 0.1393 | |
| COPD 2,404 (11.79) | 2,884 (3.39) | <.0001 | 0.3894 | |
| Depression 4,412 (21.64) | 3,282 (3.86) | <.0001 | 0.7100 | |
| GERD 3,379 (16.58) | 2,979 (3.50) | <.0001 | 0.5625 | |
| Metabolic disorders 789 (3.87) | 259 (0.30) | <.0001 | 0.3631 | |
| Somnolence 79 (0.39) | 32 (0.04) | <.0001 | 0.1080 | |
| Stroke 71 (0.35) | 175 (0.21) | .0002 | 0.0295 | |
| Incidence (n, %) | OSA 635 (3.12) | 10,682 (12.56) | <.0001 | 0.3075 |
Comparison of the Zepbound and Wegovy cohorts indicated a small age difference (45.38 vs 46.28, p = .0003) between the groups. Female patients were predominant in both cohorts, with a greater proportion in the Wegovy cohort than in the Zepbound cohort (82.65% vs. 81.66%, p = .2229). Patients in the Zepbound cohort had a higher CDS than those in the Wegovy cohort (58.81% vs. 51.32%, p < .0001). More patients living in high-SES score areas were in the Zepbound cohort than in the Wegovy cohort (40.75% vs. 37.17%, p = .0005). The most common comorbidity in the Wegovy cohort was depression (21.83% vs. 20.32%, not significant). The Wegovy cohort had diabetes (4.94% vs 3.88%, p = .0195), and metabolic disorders (3.66% vs 5.35%, p < .0001) in higher proportions than the Zepbound cohort. Besides, hypertension, hyperlipidemia, cardiovascular disease, COPD, gastroesophageal reflux disease, somnolence, and stroke are not significant.
| Characteristics | Wegovy (N = 17,859) | Zepbound (N = 2,525) | P Value | Std. Diff. |
|---|---|---|---|---|
| Age, y (mean, SD) | 45.38 (12.54) | 46.28 (11.83) | .0003 | 0.0729 |
| Age group, n (%) | 18-40 y 6,217 (34.81) | 799 (31.64) | .0017 | 0.0667 |
| 41-60 y 9,391 (52.58) | 1,430 (56.63) | .0001 | 0.0812 | |
| 61-80 y 2,057 (11.52) | 292 (11.56) | .9456 | 0.0015 | |
| ≥80 y 32 (0.18) | 3 (0.12) | .4928 | 0.0146 | |
| Gender, n (%) | Male 3,099 (17.35) | 463 (18.34) | .2229 | 0.0259 |
| Female 14,760 (82.65) | 2,062 (81.66) | .2229 | 0.0259 | |
| Comorbidity scores, n (%) | Charlson Comorbidity Score ≥2 1,218 (6.82) | 150 (5.94) | .0983 | 0.0352 |
| Chronic Disease Score ≥2 9,166 (51.32) | 1,485 (58.81) | <.0001 | 0.1501 | |
| Elixhauser Score ≥2 11,058 (61.92) | 1,567 (62.06) | .8913 | 0.0029 | |
| SES, n (%) | Low 5,105 (28.59) | 631 (24.99) | .0002 | 0.0800 |
| Medium 5,777 (32.35) | 822 (32.55) | .8355 | 0.0044 | |
| High 6,638 (37.17) | 1,029 (40.75) | .0005 | 0.0740 | |
| Baseline OSA-related comorbidities, n (%) | Hypertension 6,066 (33.97) | 832 (32.95) | .3127 | 0.0215 |
| Hyperlipidemia 3,367 (18.85) | 464 (18.38) | .5658 | 0.0122 | |
| Diabetes 883 (4.94) | 98 (3.88) | .0195 | 0.0497 | |
| Cardiovascular diseases 1,288 (7.21) | 193 (7.64) | .4343 | 0.0166 | |
| COPD 2,131 (11.93) | 273 (10.81) | .1023 | 0.0347 | |
| Depression 3,899 (21.83) | 513 (20.32) | .0835 | 0.0368 | |
| GERD 2,958 (16.56) | 421 (16.67) | .8892 | 0.0030 | |
| Metabolic disorders 654 (3.66) | 135 (5.35) | <.0001 | 0.0874 | |
| Somnolence 66 (0.37) | 13 (0.51) | .2714 | 0.0234 | |
| Stroke 59 (0.33) | 12 (0.48) | .2474 | 0.0246 | |
| OSA incidence, n (%) | 568 (3.18) | 67 (2.65) | .1536 | 0.0303 |
Table 4 provides Cox regression results for the risk of OSA in the AOM and non-AOM cohorts. Among individuals with obesity, AOM use was associated with a 40% reduction in the risk of OSA compared with no AOM (hazard ratio [HR] = 0.60, p < .0001). Female patients were 41% less likely to have OSA than male patients (HR = 0.59, p < .0001). Patients between the ages of 61 and 80 years had a 226% higher risk of OSA than those 80 years and older (HR = 3.26, p <.0001). Patients between the ages of 41 and 60 years had an 129% higher risk of OSA than those aged 80 years and older (HR = 2.29, p < .0001). People living in high-SES score areas are 7% more likely to have OSA than people living in middle-SES score areas (HR = 1.07, p = .0043). High CDS (≥2) (HR = 1.29, p < .001), cardiovascular disease (HR = 1.19, p = .0010), and somnolence (HR = 3.31, p < .0001) were associated with an increased risk of OSA.
| Characteristics | HR | Confidence Interval | P Value |
|---|---|---|---|
| Treatment | Yes 0.60 | 0.55 0.66 | <.0001 |
| No 1.00 | 1.00 1.00 | 1.00 | |
| Age group | 18-40 y 0.87 | 0.78 0.97 | .0107 |
| 41-60 y 2.29 | 2.08 2.51 | <.0001 | |
| 61-80 y 3.26 | 2.97 3.58 | <.0001 | |
| ≥80 y 1.00 | 1.00 1.00 | 1.00 | |
| Gender | Female 0.59 | 0.57 0.61 | <.0001 |
| Male 1.00 | 1.00 1.00 | 1.00 | |
| Comorbidity scores | Charlson Comorbidity Score ≥2 1.29 | 1.15 1.46 | <.0001 |
| Chronic Disease Score ≥2 0.56 | 0.52 0.59 | <.0001 | |
| Elixhauser Score ≥2 0.55 | 0.51 0.60 | <.0001 | |
| SES | Low 0.96 | 0.92 1.01 | .1138 |
| Medium 1.07 | 1.02 1.12 | .0043 | |
| High 1.00 | 1.00 1.00 | 1.00 | |
| Comorbidities | Hypertension 0.63 | 0.58 0.68 | <.0001 |
| Hyperlipidemia 0.60 | 0.55 0.66 | <.0001 | |
| Diabetes 0.68 | 0.61 0.75 | <.0001 | |
| Cardiovascular diseases 1.19 | 1.07 1.32 | .0010 | |
| COPD 0.96 | 0.86 1.07 | .4543 | |
| Depression 1.05 | 0.95 1.16 | .3216 | |
| GERD 0.80 | 0.72 0.88 | <.0001 | |
| Metabolic disorders 0.79 | 0.59 1.07 | .1307 | |
| Somnolence 3.31 | 2.06 5.34 | <.0001 | |
| Stroke 0.66 | 0.40 1.06 | .0871 |
Aalen’s additive regression results are presented in Figure 2. Consistent with Cox regression, AOM treatment is associated with a reduced likelihood of OSA. The treatment plot shows that there is a continuous reduction in the likelihood of OSA during the follow-up.
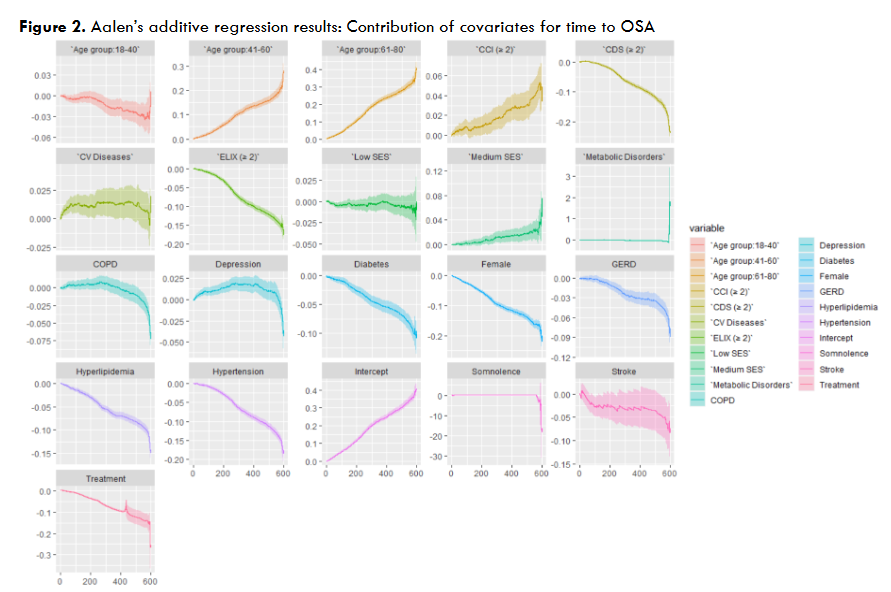
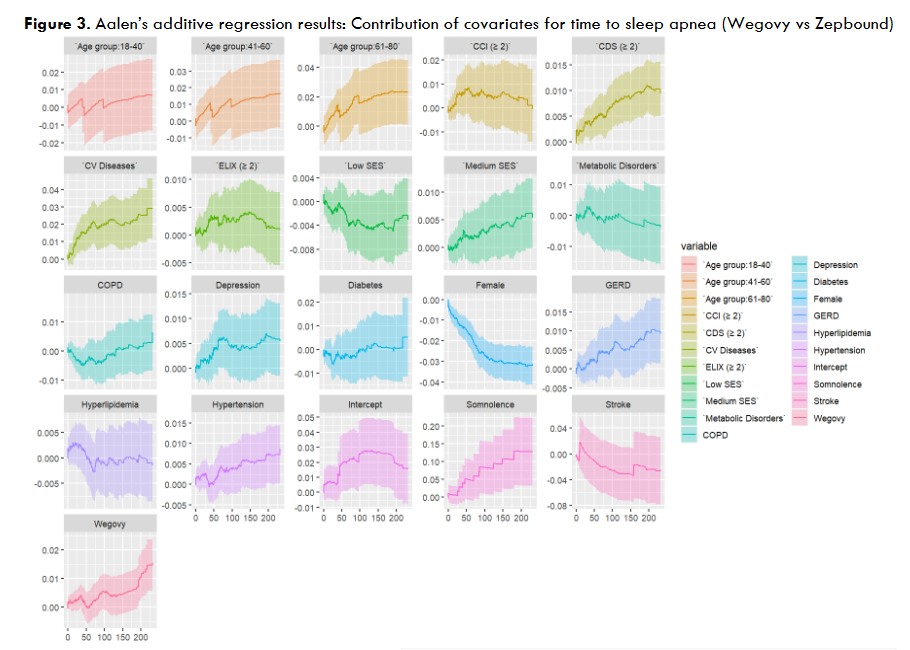
Table 5 shows the Cox regression results for the subgroup analysis comparing Wegovy with Zepbound. Compared with Zepbound, Wegovy was associated with a higher OSA, but this difference was not statistically significant. (HR=1.20, 95% CI 0.93-1.54, p<.1664). Aalen’s additive regression showed that after around 6 months of usage, Zepbound has a significant advantage over Wegovy in decreasing likelihood of OSA.
| Characteristics | HR | Confidence Interval | P Value |
|---|---|---|---|
| Treatment | Wegovy 1.20 | 0.93 1.54 | 0.1664 |
| Zepbound 1.00 | 1.00 1.00 | 1.00 | |
| Age group | 18-40 y 1.17 | 0.43 3.15 | 0.7631 |
| 41-60 y 1.72 | 0.64 4.62 | 0.2819 | |
| 61-80 y 1.98 | 0.72 5.38 | 0.1833 | |
| ≥80 y 1.00 | 1.00 1.00 | 1.00 | |
| Gender | Female 0.47 | 0.39 0.55 | <.0001 |
| Male 1.00 | 1.00 1.00 | 1.00 | |
| Comorbidity scores | Charlson Comorbidity Score ≥2 1.03 | 0.76 1.41 | 0.8370 |
| Chronic Disease Score ≥2 1.40 | 1.18 1.65 | <.0001 | |
| Elixhauser Score ≥2 1.14 | 0.92 1.42 | 0.2295 | |
| SES | Low 0.88 | 0.72 1.08 | 0.2332 |
| Medium 1.16 | 0.97 1.39 | 0.1044 | |
| High 1.00 | 1.00 1.00 | 1.00 | |
| Comorbidities | Hypertension 1.19 | 0.99 1.44 | 0.0679 |
| Hyperlipidemia 0.98 | 0.81 1.18 | 0.8072 | |
| Diabetes 1.06 | 0.75 1.48 | 0.7563 | |
| Cardiovascular diseases 1.53 | 1.19 1.97 | 0.0010 | |
| COPD 1.06 | 0.84 1.35 | 0.6172 | |
| Depression 1.18 | 0.97 1.44 | 0.0942 | |
| GERD 1.25 | 1.04 1.52 | 0.0198 | |
| Metabolic disorders 0.91 | 0.59 1.40 | 0.6635 | |
| Somnolence 4.93 | 2.71 8.97 | <.0001 | |
| Stroke 0.68 | 0.21 2.16 | 0.5149 |
Discussion
There exists a bidirectional relationship between obesity and OSA. Obesity is considered a major risk factor for the development and progression of OSA. The prevalence of OSA in patients with obesity or severe obesity patients is nearly twice that of normal-weight adults. Furthermore, the higher prevalence of OSA in individuals with obesity is not limited to adults; recent data show that children with obesity have a 46% prevalence of OSA when compared with children seen in a general pediatric clinic (33%). The converse is also true: those with OSA are at risk for obesity. Inadequate sleep during the night and daytime sleepiness predispose patients to weight gain. Given the rising prevalence of obesity and bidirectional relationship between obesity and OSA, effective management strategies are crucial for reducing the associated OSA burden.
Recent progress in AOMs, especially semaglutide and tirzepatide, has demonstrated encouraging outcomes in managing obstructive sleep apnea in individuals with obesity. Tirzepatide, a dual GIP and GLP-1 receptor agonist, demonstrated remarkable efficacy in the SURMOUNT-OSA trial, reducing moderate-to-severe OSA severity by 62.8% compared to placebo. Similarly, semaglutide has shown potential in managing OSA through significant weight reduction. In a 104-week trial, once-weekly subcutaneous semaglutide at 2.4 mg led to a mean change in body weight of -15.2% compared to -2.6% with placebo. This substantial weight loss is particularly relevant for OSA management, as obesity is a significant risk factor for the condition. These findings suggest that AOMs like tirzepatide and semaglutide could represent a breakthrough in treating obesity-related OSA, potentially offering an effective approach for management when combined with positive airway pressure (PAP) therapy.
Although the AOM cohort had a higher percentage with a Chronic Disease Score ≥2 than the non-AOM cohort (52.25% vs 8.44%; p<.001), our analysis revealed that AOM utilization is associated with a substantial reduction in the likelihood of developing OSA. Overall, patients in the AOM cohort exhibited a 40% lower risk of OSA than those not using these medications (HR=0.60, p<.0001) after adjusting for sociodemographic and clinical characteristics. The incidence of OSA was lower in the AOM cohort than in the non-AOM cohort (3.12% vs 12.56%; p <.001). These findings align with previous research indicating the efficacy of tirzepatide and semaglutide in achieving meaningful weight loss and improving health outcomes.
While both tirzepatide and semaglutide were effective in reducing OSA incidence, no statistically significant difference was observed between the two medications. However, Aalen analyses suggested that tirzepatide might confer a slightly greater advantage, particularly after six months of treatment (p=.1664). These results warrant further investigation to determine whether specific patient subgroups might benefit more from one medication over the other.
Additionally, our findings suggest how demographic and socioeconomic factors could influence OSA risk. Female patients demonstrated a lower likelihood of developing OSA than males, consistent with existing literature on gender differences in OSA prevalence. Age was another significant determinant; older adults faced a markedly higher risk than younger cohorts. Patients 61 to 80 years of age appear to face the highest risk of OSA among all age groups. They had a 226% higher risk of OSA than those 80 and older (HR = 3.26, p <.0001) and a 91% higher risk than those aged 41 to 60 years (HR = 2.29, p<.0001). Previous studies also showed that OSA prevalence increases with age, with individuals over 65 at higher risk than any other group. Consistent with previous research, SES also emerged as a key variable, with individuals in medium-SES regions showing an elevated risk than those in high-SES areas. Previous research showed that lower SES is consistently associated with an increased risk of OSA in both adults and children.
The economic burden of OSA is substantial, with undiagnosed OSA estimated to cost the United States approximately $149.6 billion in 2015. This impact extends beyond direct healthcare costs, as patients with OSA were at a higher risk of unintentional injuries, including falls and substance poisoning, traffic injury, and suffocation, than those without OSA. In intentional injury, patients with OSA had a 6.68- and 10.88-fold greater risk of suicide and abuse or homicide-related injury, respectively, than individuals without OSA. A diagnosis of a sleep disorder was associated with approximately 8 additional office visits, 18 additional prescriptions, and an incremental increase in health care expenditures of almost $7,000 per individual per year. Recent studies have shown promising results for AOMs in addressing both obesity and OSA, highlighting the potential of AOMs to leading to substantial cost savings in healthcare systems.
Anti-obesity medications, through their significant impact on weight reduction, present a promising approach to addressing OSA in individuals with obesity. Our study demonstrates the potential of AOMs, particularly tirzepatide and semaglutide, in mitigating OSA risk among patients with obesity. These medications offer a dual benefit by targeting both obesity and its associated comorbidities, potentially improving sleep quality and overall health outcomes. As OSA affects an estimated 30 million adults in the United States alone, integrating AOMs into comprehensive obesity management strategies could play a crucial role in alleviating this widespread health issue. This approach aligns with the broader goals of enhancing respiratory function, improving cardiovascular health, and reducing healthcare costs associated with OSA treatment. By addressing the root cause of obesity-related OSA, AOMs may contribute to more sustainable and effective treatment options, ultimately improving the quality of life for millions of affected individuals.
LIMITATIONS
Several notable limitations warrant consideration. Our results suggest a correlation between AOM utilization and decreased likelihood of OSA development. However, it is crucial to emphasize that this relationship is associative rather than causal given the absence of randomization between the study groups. The study’s reliance on commercial data for analyzing OSA likelihood introduces potential biases. Notably, the data set lacked information on ethnicity, which is particularly significant given that previous research indicates African American race was associated with 33% higher rates of OSA. Consequently, if the SES score does not adequately account for racial disparities, the estimates may be skewed. Another limitation of the study is the exclusion of physical activity data from the analysis. Previous research shows that physical activity would be beneficial for patients with obesity in reducing OSA risk. Ideally, these factors should have been reported and included in the analysis for both AOM and non-AOM groups.
The use of administrative data sets introduces several constraints to the study. These data sets may suffer from inaccurate coding of patient clinical diagnoses and procedures, as well as limited clinical information restricted to conditions and treatments defined by ICD-10-CM codes. As the analysis was conducted on commercial data not initially designed for research purposes, some information is inevitably missing. It is important to note that a diagnosis code on a medical claim does not necessarily confirm the presence of disease, as it might be incorrectly coded or used as rule-out criteria rather than an actual diagnosis. The use of ICD-10 codes for diagnosing OSA might be insufficient to identify patients accurately. Incorporating biologics and additional OSA treatments could improve patient identification accuracy.
Conclusion
Our study indicates that the use of the recently approved AOMs tirzepatide (Zepbound) and semaglutide (Wegovy) is associated with a significantly reduced risk of OSA among patients with obesity. While a slight difference in OSA incidence was observed between tirzepatide and semaglutide users, this difference did not reach statistical significance. These findings suggest that AOMs may serve as effective interventions for managing obesity and potentially lowering the risk of OSA. However, it is crucial to interpret these results with caution, considering the limitations inherent in observational studies. Long-term studies are needed to assess the sustained effects of these medications on OSA outcomes and evaluate their safety profile over extended periods.
Declarations
FUNDING
This study was not funded.
CONFLICT OF INTEREST
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
AUTHOR CONTRIBUTIONS
O.B. provided the supervision, conceptualization, methodology, validation, and visualization of the research and participated in the writing process from the original draft preparation to the reviewing and editing of the manuscript. Y.L. participated validation and in the writing process from the original draft preparation to the reviewing and editing of the manuscript. S.C. participated in the writing process from the original draft preparation to the reviewing and editing of the manuscript. E.B. participated in analysis, investigation of the data software, validation, and in reviewing and editing of the manuscript.
ACKNOWLEDGMENTS
The authors thank Amy Endrizal for assistance in editing the manuscript.
INSTITUTIONAL REVIEW BOARD STATEMENT
Ethics approvals were not required as the data were from an anonymous, de-identified database compliant with HIPAA.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from Kythera Labs. Due to restrictions on the availability of these data, which were used under license for the current study, they are not publicly available. However, data may be made available from the corresponding author, Onur Baser, upon reasonable request and with permission of Kythera Labs.
References
- Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8-27.
- Romero-Corral A, Caples SM, Lopez-Jimenez F, Somers VK. Interactions between obesity and obstructive sleep apnea: implications for treatment. Chest. 2010;137(3):711-719.
- Meyer EJ, Wittert GA. Approach the patient with obstructive sleep apnea and obesity. J Clin Endocrinol Metab 2024;109(3):e1267-e1279.
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. New England journal of medicine. 1993;328(17):1230-1235.
- Rudnick EF, Walsh JS, Hampton MC, Mitchell RB. Prevalence and ethnicity of sleep-disordered breathing and obesity in children. Otolaryngology–Head and Neck Surgery. 2007;137(6):878-882.
- Tai JE, Phillips CL, Yee BJ, Grunstein RR. Obstructive sleep apnoea in obesity: A review. Clin Obes. 2024;14(3):e12651.
- Somers VK, White DP, Amin R, et al. Sleep apnea and cardiovascular disease: An American heart association/American college of cardiology foundation scientific statement from the American heart association council for high blood pressure research professional education committee, council on clinical cardiology, stroke council, and council on cardiovascular nursing in collaboration with the national heart, lung, and blood institute national center on sleep disorders research (national institutes of health). Circulation. 2008;118(10):1080-1111.
- Parish JM, Somers VK. Obstructive sleep apnea and cardiovascular disease. Elsevier; 2004:1036-1046.
- Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. New England Journal of Medicine. 2000;342(19):1378-1384.
- Jaganathan N, Kwon Y, Healy WJ, Taskar V. The Emerging Role of Pharmacotherapy in Obstructive Sleep Apnea. Journal of otorhinolaryngology, hearing and balance medicine. 2024;5(2):12.
- Malhotra A, Grunstein RR, Fietze I, et al. Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity. N Engl J Med. 2024;
- Baser O, Samayoa G, Yapar N, Baser E, Mete F. Use of open claims vs closed claims in health outcomes research. J Health Econ Outcomes Res. 2023;10(2):44.
- Baser O, Isenman L, Baser S, Samayoa G. Impact of semaglutide on osteoarthritis risk in patients with obesity: a retrospective cohort study. Obes Sci Pract. 2024:e762.
- Baser O, Samayoa G, Rodchenko K, Isenman L, Baser E, Yapar N. The association between weight loss medications and cardiovascular complications. Obesity (Silver Spring). 2024;32(7):1401-1409. doi:10.1002/oby.24037
- Baser O, Rodchenko K, Vivier E, Baser I, Lu Y, Mohamed M. The impact of approved anti-obesity medications on osteoarthritis. Exp Opin Pharmacother. 2024;25(11):1565-1573.
- Birkmeyer NJ, Gu N, Baser O, Morris AM, Birkmeyer JD. Socioeconomic status and surgical mortality in the elderly. Med Care. 2008;46(9):893-899.
- Charlson ME, Carrozzino D, Guidi J, Patierno C. Charlson comorbidity index: a critical review of clinimetric properties. Psychother Psychosom. 2022;91(1):8-35.
- Putnam KG, Buist DS, Fishman P, et al. Chronic disease score as a predictor of hospitalization. Epidemiology. 2002;13(3):340-346.
- Aalen O, Scheike TH. Aalen’s additive regression model. Wiley StatsRef: Statistics Reference Online. 2014;
- Romero-Corral A, Caples SM, Lopez-Jimenez F, Somers VK. Interactions between obesity and obstructive sleep apnea: implications for treatment. Chest. Mar 2010;137(3):711-9. doi:10.1378/chest.09-0360
- Jehan S, Zizi F, Pandi-Perumal SR, et al. Obstructive Sleep Apnea and Obesity: Implications for Public Health. Sleep Med Disord. 2017;1(4)
- Eli Lilly and Company. Tirzepatide reduced sleep apnea severity by up to nearly two-thirds in adults with obstructive sleep apnea (OSA) and obesity. Eli Lilly and Company. 2024, https://investor.lilly.com/news-releases/news-release-details/tirzepatide-reduced-sleep-apnea-severity-nearly-two-thirds
- Garvey WT, Batterham RL, Bhatta M, et al. Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial. Nature Med. 2022/10/01 2022;28(10):2083-2091. doi:10.1038/s41591-022-02026-4
- Geer JH, Hilbert J. Gender Issues in Obstructive Sleep Apnea. Yale J Biol Med. 2021;94(3):487-496.
- Franklin KA, Lindberg E. Obstructive sleep apnea is a common disorder in the population—a review on the epidemiology of sleep apnea. J Thorac Dis. 2015;7(8):1311.
- Guglielmi O, Lanteri P, Garbarino S. Association between socioeconomic status, belonging to an ethnic minority and obstructive sleep apnea: a systematic review of the literature. Sleep Medicine. 2019;57:100-106.
- Watson NF. Health Care Savings: The Economic Value of Diagnostic and Therapeutic Care for Obstructive Sleep Apnea. J Clin Sleep Med. 2016;12(8):1075-1077. doi:10.5664/jcsm.6034
- Cheng AC, Wu GJ, Chung CH, et al. Effect of Obstructive Sleep Apnea on the Risk of Injuries-A Nationwide Population-Based Cohort Study. Int J Environ Res Public Health. 2021;18(24)doi:10.3390/ijerph182413416
- Huyett P, Bhattacharyya N. Incremental health care utilization and expenditures for sleep disorders in the United States. J Clin Sleep Med. 2021;17(10):1981-1986. doi:10.5664/jcsm.9392
- Wang R, Dong Y, Weng J, et al. Associations among neighborhood, race, and sleep apnea severity in children. A six-city analysis. Ann Am Thorac Soc 2017;14(1):76-84.
- Liu Y, Yang L, Stampfer MJ, Redline S, Tworoger SS, Huang T. Physical activity, sedentary behaviour and incidence of obstructive sleep apnoea in three prospective US cohorts. Eur Resp J. 2022;59(2)