





Trends in Rectal Prolapse Repair Rates in WA State
Population-adjusted Rates of Rectal Prolapse Repair in Washington State Over a Contemporary, 12-Year Time Period
Introduction
Rectal prolapse is a condition that more frequently affects women and the elderly, and can cause severe debilitation necessitating surgical intervention. Operations to address rectal prolapse are often tailored to the patient’s symptoms, medical condition, and prior procedures, but there is a lack of consensus regarding the ideal approach.¹⁻⁵ For instance, abdominal approaches have traditionally been advocated for younger, healthier patients, while perineal techniques are more commonly utilized for elderly and frail individuals.⁴˒⁷ With the wide adoption of minimally invasive surgery (MIS), the benefits of laparoscopic- or robotic-assisted rectal prolapse repairs have been demonstrated, though their effect on shifting the paradigms of rectal prolapse repair are not well established.²˒⁸˒¹⁰
Furthermore, there is a strong association between rectal prolapse and pelvic organ prolapse.¹¹⁻¹³ Consequently, concomitant operations for rectal and vaginal prolapse have increased, facilitated by multidisciplinary pelvic floor care.¹⁴⁻¹⁷ Pelvic prolapse can be successfully managed with vaginal or abdominal approaches. However, the patterns of concurrent pelvic organ and rectal prolapse repair as they compare to isolated rectal prolapse repair at the population level are not well described.
Specifically, this interplay between multiple operations and approaches, indications, and surgeon specialization can result in the appearance of variation and heterogeneity in outcomes. In order to better identify areas to reduce variation and better capture rectal prolapse repair outcomes, we felt it necessary to understand broad patterns of care at the population level.
Therefore, our objective was to assess rates of rectal prolapse repair in Washington (WA) State over a 12-year period. We hypothesize that in our state, the rates of rectal prolapse repair are comparable to other reported studies, with increases in concurrent rectal and vaginal prolapse repairs and in repairs being performed minimally invasively over time. Our secondary objective was to explore patient, surgeon, and hospital factors that may be affecting practice patterns of rectal prolapse repair.
Materials & Methods
This study was exempt from human subjects review by the Benaroya Research Institute Institutional Review Board.
DATA SOURCE
The Washington State Comprehensive Hospital Abstract Reporting System (CHARS) was used to create a retrospective cohort which identified patients who underwent a rectal prolapse operation and were admitted postoperatively. The CHARS is maintained through the Washington State Department of Health and captures all inpatient hospitalizations from all hospitals in the state.¹⁸ The CHARS data dictionary is publicly available at https://www.doh.wa.gov/, and includes diagnosis and procedural codes based on the Ninth revision of the International Classification of Diseases (ICD-9) and ICD-10 for admissions. Demographic variables, admission and discharge administrative details, payer status, and facility and operating physician identifiers were collected.
STUDY POPULATION
Hospitalizations from 2008 to 2019 with ICD-9 and ICD-10 diagnosis and procedure codes designating a rectal prolapse operation on the same record were included in the study cohort (Appendix 1). This timeframe was chosen to include both the ICD-9 and ICD-10 coding periods, but truncated in 2020 as the COVID-19 pandemic was expected to dramatically impact care of elective surgery, such as rectal prolapse repairs. The cohort was limited to patients 18 years and older.
OUTCOMES/DEFINITIONS
Annual rates of rectal prolapse repair (RPR) were identified in this cohort. Overall RPR was subdivided into RPR alone and concurrent rectal and vaginal prolapse repair (CRVR) in the female cohort. Isolated vaginal prolapse surgery was excluded in this analysis.
Because rectal prolapse repair can be performed via perineal or abdominal approaches, we defined these as 2 different subsets using ICD-9 and ICD-10 procedure codes. Additionally, because of the rise in minimally invasive approaches for pelvic surgery over the last decade, abdominal surgery was further divided into open and laparoscopic based on procedural codes (Appendix 1). Since there are no procedural codes specifically designating robotic use in the ICD-10 procedural dictionary, robotic (by ICD-9) and laparoscopic operations were grouped together and collectively reported as minimally invasive.
STATISTICAL ANALYSIS
Yearly population-based counts of rectal prolapse admissions with surgical procedures were used to calculate crude rates of RPR. To account for the changes in population in WA State during the period of the study, overall rates of RPR, RPR alone, and CRVR were adjusted for sex and age using the direct method and the US Census official counts and between census estimates as the reference.¹⁹ All population-based frequencies were reported as a frequency per 100,000 people.
Specific trends and statewide variation were explored by subsets of age, surgical approaches, facility, and county of residence. Number of surgeons providing rectal prolapse repair in each county were also collected to determine correlation with rates of repair. Fluctuations in rates of smaller counties were addressed by focusing this exploratory analysis to a subgroup of admissions in 6 counties, which represented 92% of all hospital admissions in this dataset. The distance travelled in miles from the patient’s residence to treating facility was estimated using zip-codes and their corresponding latitude and longitude coordinates.
Data were summarized using frequency distributions for categorical variables and mean ± standard deviation for continuous variables. Categorical variables were compared using Pearson χ² statistic. Trends in admission for overall rates and by age for 2008-2019 was conducted using one-way ANOVA. A p-value of less than 0.05 was considered statistically significant. Statistical analysis was performed using Microsoft Excel [Microsoft Excel for Office 365 MSO], R (R Core Team, 2019), and IBM SPSS Statistics for Windows, Version 16.0.
Results
PATIENT DEMOGRAPHICS
There were 2,755 hospitalizations (mean age 60.5±16.3 years, 93% female) for RPR that were identified (Table 1). These were performed by 240 surgeons at 52 hospitals in WA State over the study period. Seventy-five percent (n=2,070) of all repairs were in patients older than 50, and 41.7% (n=1,148) in patients 65 and older. Almost one-third of all patients (n=918) underwent CRVR. Combined repair was more frequent in the younger demographic, with 68% (n=621) of CRVR in patients 64 and younger.
RATES OF RECTAL PROLAPSE REPAIR
Age- and sex-adjusted rates for all patients undergoing any type of rectal prolapse repair (RPR+CRVR) went from 3.72/100,000 people in 2008 to 3.25/100,000 in 2019 (p=0.003), without meaningful change in RPR or CRVR rates individually (Figure 1). For females age 65 to 79 years, rates of RPR+CRVR went from 0.77/100,000 in 2008 to 1.09/100,000 in 2019 (p=0.09) and remained stable in females age 80+ years with 0.47/100,000 and 0.49/100,000 in 2008 and 2019, respectively (p=0.945). There was no meaningful change in RPR or CRVR subgroups in these age subsets.
SURGICAL APPROACH
A perineal approach was used 31% of the time (Table 1) and was more common for RPR (36%) than for CRVR (22%, p<0.001). The proportion of RPR+CRVR cases using perineal approaches initially rose over the study period, peaking in 2014 before a subsequent decline (Figure 2). In addition, the proportion of abdominal rectal prolapse repairs approached through a minimally invasive approach as compared to open increased from 32.5% in 2008 to 65.4% in 2019 (p<0.001).
Table 1: Demographics of inpatient rectal prolapse repair admissions in WA from 2008-2019
| Variable | Total Prolapse N=2,755 | Rectal Prolapse Repair (RPR) n=1,837 | Concurrent Rectal and Vaginal Repair (CRVR) n=918 | p* |
|---|---|---|---|---|
| n / % | n / % | n / % | ||
| Gender | <0.001 | |||
| Female | 2561 / 92.96 | 1643 / 89.44 | 918 / 100.00 | |
| Age group | <0.001 | |||
| <50 years | 685 / 24.86 | 419 / 22.81 | 266 / 28.98 | |
| 50-64 years | 922 / 33.47 | 567 / 30.87 | 355 / 38.67 | |
| 65-79 years | 779 / 28.28 | 529 / 28.80 | 250 / 27.23 | |
| 80+ years | 369 / 13.39 | 322 / 17.53 | 47 / 5.12 | |
| Ethnicity§ | <0.001 | |||
| American Indian/Alaskan Native | 18 / 0.65 | 16 / 0.87 | 2 / 0.22 | |
| Asian | 42 / 1.52 | 27 / 1.47 | 15 / 1.63 | |
| Black/African American | 24 / 0.87 | 17 / 0.93 | 7 / 0.76 | |
| Hispanic Origin | 47 / 1.71 | 34 / 1.85 | 13 / 1.42 | |
| Native Hawaiian/Pacific Islander | 4 / 0.15 | 4 / 0.22 | 0 / 0.00 | |
| White | 1836 / 66.64 | 1254 / 68.26 | 582 / 63.40 | |
| Insurance | <0.001 | |||
| Medicare/Medicaid/Other Govt | 1365 / 49.55 | 1024 / 55.74 | 341 / 37.15 | |
| HMO/Commercial | 1342 / 48.71 | 777 / 42.30 | 565 / 61.55 | |
| Self/Charity | 48 / 1.74 | 36 / 1.96 | 12 / 1.31 | |
| Surgical Procedures | ||||
| Perineal | 862 / 31.29 | 659 / 35.87 | 203 / 22.11 | <0.001 |
| Abdominal | 1893 / 68.71 | 1178 / 64.13 | 715 / 77.89 | <0.001 |
| Open | 981 / 35.61 | 464 / 25.26 | 517 / 56.32 | <0.001 |
| Laparoscopic | 684 / 24.83 | 510 / 27.76 | 174 / 18.95 | <0.001 |
| Use of Mesh† | 95 / 3.45 | 79 / 4.30 | 16 / 1.74 | <0.001 |
| Admission Type§ | <0.001 | |||
| Elective | 2640 / 95.83 | 1729 / 94.12 | 911 / 99.23 | |
| Emergent/Urgent | 113 / 4.10 | 108 / 5.88 | 5 / 0.54 |
*Note: χ2 p value comparison rectal prolapse only and rectal/vaginal prolapse combination groups
§Note: Portion of data missing or not provided
†Note: Mesh codes only designate cases from 2015 onward. Total reflects cases from 2015-2019
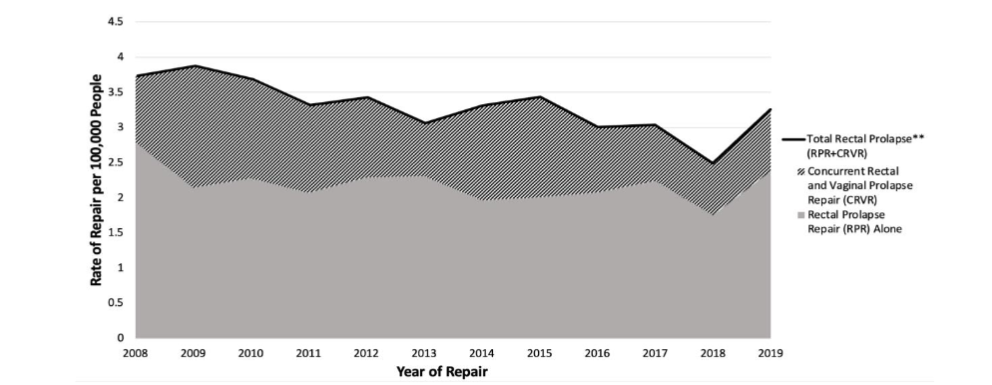
Figure 1
Adjusted rates* of inpatient rectal prolapse procedures by prolapse type in Washington State from 2008-2019.
*Age- and sex-adjusted rates based on annual Washington State census;
**Total rectal prolapse is the summation of all vaginal and rectal prolapse admissions.
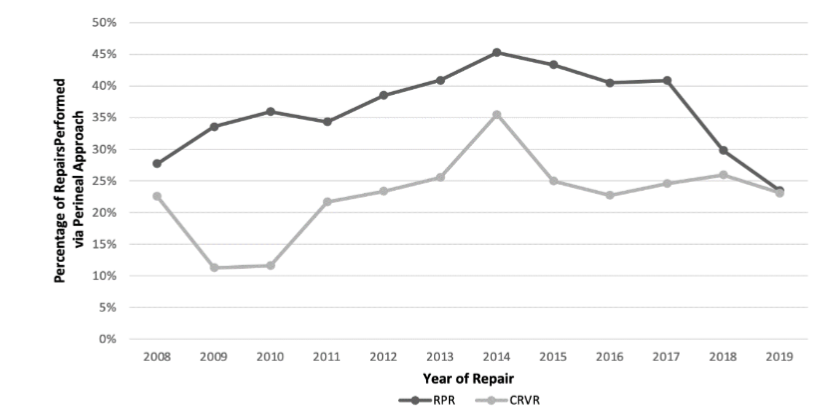
Figure 2
Proportion of rectal prolapse procedures approached via a perineal approach in Washington State from 2008-2019.
RPR = rectal prolapse repair alone; CRVR = concurrent rectal and vaginal prolapse repair.
FACILITY, PROVIDER, AND DISTANCE TRAVELLED
Eighty-seven percent (n=2,383) of rectal prolapse repairs were performed across 15 sites (Figure 3). Patients tended to be treated at hospitals near their home whether the repair was RPR or CRVR, with 75% living within 20 miles of the treating facility. Out of the top 15 treating hospitals, only one tertiary care hospital in King County had >95% of their patients from 20+ miles away. In the 6 most populated counties in the state, in which these 15 sites are located, adjusted rates of RPR and CRVR individually varied both by county and by number of providers (Figure 4), with rates of prolapse repairs performed having two- to three-fold variation between counties.
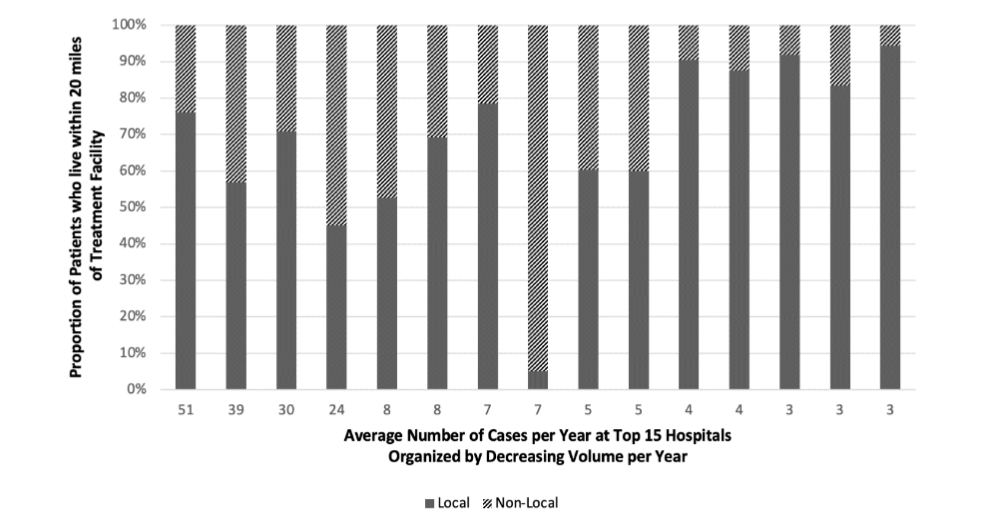
Figure 3
Proportion of patients receiving care locally (within 20 miles) at top 15 Washington State facilities by average annual volume of rectal prolapse repair.
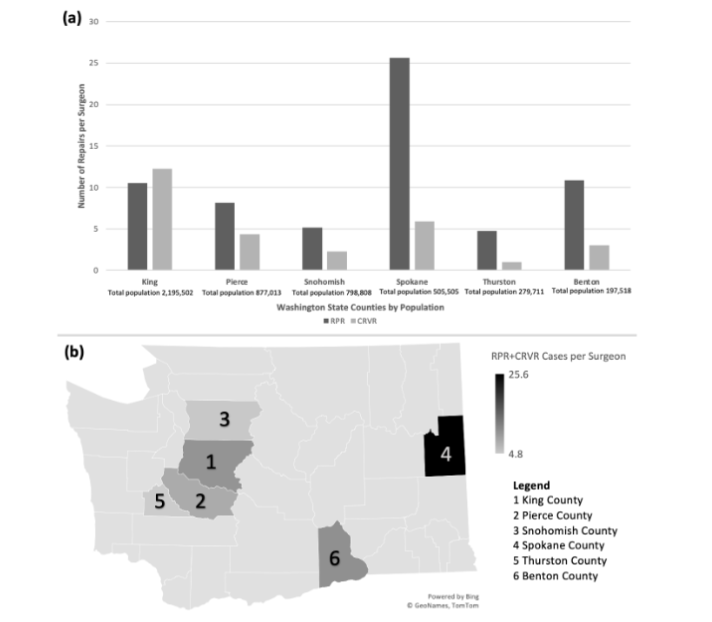
Figure 4
Average number of prolapse repairs by surgeon in top 6 most populated Washington State counties
(a) by rectal prolapse repair alone (RPR) vs concurrent rectal and vaginal prolapse repair (CRVR) and
(b) by total rectal prolapse (RPR+CRVR).
Discussion
At the state level, rates of rectal prolapse repair across all age groups are stable, with one-third of repairs being performed for concurrent rectal and vaginal prolapse over the past 12 years. The majority of CRVR patients are younger compared to those undergoing RPR alone. The rise in abdominal surgery in this cohort corresponds to an increase in transabdominal approach for concurrent repairs and more frequent utilization of minimally invasive techniques. These collective findings may have several explanations.
The stability of rectal prolapse rates over more than a decade identified in this cohort differs from that of other studies, which have demonstrated increasing rates nationally in both rectal prolapse repair alone and concurrent rectal and vaginal prolapse repairs.¹⁷˒²⁰˒²¹ With an aging population in which the incidence of rectal prolapse is higher, wide adoption of minimally invasive techniques that are associated with lower morbidity, and heightened awareness of disease burden with increased shared decision-making between multidisciplinary providers and patients, the expectation would be an increase in procedures performed. However, prior studies did not directly adjust for age- and sex- changes in the population, so it may be that the “stable” rates reflected in this study might suggest that surgeons are meeting the need of the evolving population in WA state.
During the study period, there was a near doubling in frequency of minimally invasive procedures performed for rectal prolapse, with a simultaneous fall in perineal procedures, both of which were most pronounced in the later years of the cohort. Perineal approaches, most commonly the Altemeier’s procedure (perineal rectosigmoidectomy) or Delorme’s procedure, have been preferred for elderly, high-risk patients. However, the safety of minimally-invasive techniques, such as laparoscopic ventral rectopexy, have been assessed in elderly patients over 80 years with comparable morbidity and mortality to perineal procedures.²² Additionally, following the PROSPER trial, more recent studies have shown an increasing preference for laparoscopic approaches.²³ The choice of performing a laparoscopic procedure is gaining popularity in the elderly population, with improved continence and long term outcomes following this technique.²⁴ In this cohort, the proportion of cases approached minimally invasively in patients 65 and older increased from 17% to 38.2%, and in patients 80 and older increased from 6.8% to 13.8%. Compared to open and perineal repairs, laparoscopic repair is associated with less pain, shorter length of stay, and decreased morbidity.²⁵˒²⁶ Furthermore, this uptick in MIS comes during an era in which all surgeons are being trained in minimally invasive approaches,²⁷ so the use of laparoscopy and robotics in future generations of providers is expected to persist. The shift to MIS colorectal procedures has been previously demonstrated in our state, specifically in pelvic colorectal surgery. In one regional collaborative, which represents a majority of hospitals in WA state, a robotic approach was used in 71% of rectopexies.²⁸ Additionally, robotic-assisted surgery has shown promising results, specifically in multidisciplinary, robotic-assisted CRVR where initial studies have shown excellent short-term outcomes with low 2-year recurrence rates and significant relief of functional pelvic floor symptoms.²⁹ Because robotic procedures are not explicitly identified by ICD-9 and ICD-10 procedure codes, the proportion of robotic compared to laparoscopic surgery was not explicitly evaluated in this cohort.
Despite being considered a benign condition, rectal prolapse repair is performed because of debilitating symptoms, and anatomic correction can result in dramatic improvement of fecal incontinence and obstructive defecation. Still, much remains unknown about what ultimately drives patients to seek care and undergo surgery. This cohort showed that most patients in WA state undergo their operation within 20 miles of their home. Accordingly, the majority of operations are matched to counties where the majority of the population resides (Figure 4b).
The distance patients travel for repair is relevant because access to high-quality surgery centers remains a challenge nationally, with as much as 10% of the US population living greater than 30 miles from a major surgical hospital.³⁰ Furthermore, evidence has shown that patients have strong preference for local care. Finlayson et al. found that for patients undergoing elective surgery, nearly 75% of patients would prefer local surgery even if travel to a regional center would lead to lower operative mortality risk.³¹ A survey in 2020 showed that 51% of patients take location of the hospital into consideration when choosing where to receive care.³² Travel burden may also affect centralization of care. A state-wide analysis in New York described that if patients with rectal cancer were limited to resection at high volume centers, mean travel time would significantly increase and may cause undue burden on patients.³³ The data presented herein suggests that rectal prolapse, at least in the current state, is a disease for which patients are not travelling far from home to be treated.
While distance appears to be a relevant issue in RPR, it is clear that there remain some unaddressed factors driving care. For instance, if rates of RPR were purely based on a larger population having a higher incidence of rectal prolapse, the number of rectal prolapse repairs would be expected to correlate with the county population. Instead, across the 6 most-populated counties, this study found variation (in some cases two- to three-fold) in number of procedures, number of surgeons, and the average number of RPR or CRVR performed per surgeon. This suggests there is an opportunity to better understand surgeons’ thresholds to offer repair for rectal prolapse, or patients’ threshold to accept it, as well as the impact of surgeon specialization or regionalization at driving both number of procedures and outcomes.
The use of state-wide inpatient data to assess for trends in rectal prolapse provides information regarding real-world, contemporary clinical practice and management patterns. However, our study has several limitations. The CHARS database is used for billing and administrative purposes, and data is not collected for research. Thus, it is not rich in clinical variables, and no information on pre-operative work up, imaging, and disease-specific details such as specifics around the anatomy of the prolapse that may have contributed to surgeon decision-making are recorded in this database. Also importantly, no data is provided regarding functional outcomes, quality of life, complications, and recurrence. Additionally, there is a risk of misclassification of subgroups within our cohort using ICD-9 and ICD-10 Procedure Coding System (PCS) codes rather than Current Procedural Terminology (CPT) codes, which have historically been used for population studies of rectal prolapse.¹⁶˒¹⁷ In the CHARS database, CPT codes are not captured. However, during the transition from ICD-9 to ICD-10 codes, major shifts in procedures or approaches were not seen, suggesting that important subsets were not being missed by the coding transition. Finally, we were unable to identify trends for the use of mesh in rectal prolapse repair over the study period as there were no distinguishable ICD-9 procedure codes to reflect this information. As a result, this data is limited to a 4-year period, during which the proportion of mesh use increased from 3.3% in 2015 to 23.4% in 2019. Other studies have reported an increase in adoption of mesh and suggest its use may lead to a more durable repair.³⁴˒³⁵
Conclusion
This study highlights the evolution of rectal prolapse surgery at the state population level. In Washington State, there have been stable age- and sex-adjusted rates of rectal prolapse repair, with one-third of all repairs performed for concurrent rectal and vaginal prolapse over the past 12 years. There has been a broad shift towards a minimally invasive, abdominal approach. Most patients receive operations at facilities close to home, and while the bulk of operations occur in high-population areas, there appears to be significant variation in the number of surgeons and procedures offered across the state. These patterns of care are important to understand, and further studies regarding how this relates to cost and patient outcomes are underway.
Disclosure:
Dr. Vlad V. Simianu has received educational and travel support from Intuitive Surgical, Inc. and is a consultant for C-SATS. Dr. Celine R. Soriano, Dr. Justina Tam, Ms. Hannah Koenig, Dr. Jennifer A. Kaplan, Dr. Kathleen Kobashi, Dr. Hyung Chan Kim, and Dr. Una Lee have no conflicts of interest or financial ties to disclose.
Acknowledgements:
None.
Funding:
There was no funding source for this project.
Ethics approval:
This study was exempt from human subjects review by the Benaroya Research Institute Institutional Review Board.
Previous Presentation:
Presented virtually as Presentation on Demand during the 2021 American Society of Colon and Rectal Surgeons Annual Scientific Meeting in San Diego, CA, April 24 – 28, 2021.
References
1. Azimuddin K, Khubchandani IT, Rosen L, Stasik JJ, Riether RD, Reed JF 3rd. Rectal prolapse: a search for the “best” operation. Am Surg. 2001; 67(7):622-627.
2. Bordeianou L, Paquette I, Johnson E, et al. Clinical Practice Guidelines for the Treatment of Rectal Prolapse. Dis Colon Rectum. 2017;60(11): 1121-1131. doi:10.1097/DCR.0000000000000889
3. Russell MM, Read TE, Roberts PL, et al. Complications after rectal prolapse surgery: does approach matter? Dis Colon Rectum. 2012;55(4): 450-458. doi:10.1097/DCR.0b013e31823f86b8
4. Senapati A, Gray RG, Middleton LJ, et al. PROSPER: a randomised comparison of surgical treatments for rectal prolapse. Colorectal Dis. 2013; 15(7):858-868. doi:10.1111/codi.12177
5. Cirocco WC. In search of the optimal operation for rectal prolapse: the saga continues…. Tech Coloproctol. 2019;23(1):1-2. doi:10.1007/s10151-019-01937-8
6. Riansuwan W, Hull TL, Bast J, Hammel JP, Church JM. Comparison of perineal operations with abdominal operations for full-thickness rectal prolapse. World J Surg. 2010;34(5):1116-1122. doi:10.1007/s00268-010-0429-0
7. Alwahid M, Knight SR, Wadhawan H, Campbell KL, Ziyaie D, Koch SMP. Perineal rectosigmoidectomy for rectal prolapse-the preferred procedure for the unfit elderly patient?. 10 years experience from a UK tertiary centre. Tech Coloproctol. 2019;23(11): 1065-1072. doi:10.1007/s10151-019-02100-z
8. Kariv Y, Delaney CP, Casillas S, et al. Long-term outcome after laparoscopic and open surgery for rectal prolapse: a case-control study [published correction appears in Surg Endosc. 2006 Feb;20(2): 343]. Surg Endosc. 2006;20(1):35-42. doi:10.1007/s00464-005-3012-2
9. Byrne CM, Smith SR, Solomon MJ, Young JM, Eyers AA, Young CJ. Long-term functional outcomes after laparoscopic and open rectopexy for the treatment of rectal prolapse. Dis Colon Rectum. 2008;51(11):1597-1604.
doi:10.1007/s10350-008-9365-6
10. Perrenot C, Germain A, Scherrer ML, Ayav A, Brunaud L, Bresler L. Long-term outcomes of robot-assisted laparoscopic rectopexy for rectal prolapse. Dis Colon Rectum. 2013;56(7):909-914. doi:10.1097/DCR.0b013e318289366e
11. Dekel A, Rabinerson D, Rafael ZB, Kaplan B, Mislovaty B, Bayer Y. Concurrent genital and rectal prolapse: two pathologies–one joint operation. BJOG. 2000;107(1):125-129. doi:10.1111/j.1471-0528.2000.tb11589.x
12. Altman D, Zetterstrom J, Schultz I, et al. Pelvic organ prolapse and urinary incontinence in women with surgically managed rectal prolapse: a population-based case-control study. Dis Colon Rectum. 2006;49(1):28-35. doi:10.1007/s10350-005-0217-3
13. González-Argenté FX, Jain A, Nogueras JJ, Davila GW, Weiss EG, Wexner SD. Prevalence and severity of urinary incontinence and pelvic genital prolapse in females with anal incontinence or rectal prolapse. Dis Colon Rectum. 2001;44(7):920-926. doi:10.1007/BF02235476
14. Higgins EW, Yandell PM, Shull BL, Kuehl TJ, Papaconstantinou HT. Coexistent rectal and vaginal prolapse: Report of a case series of combined surgical repair utilizing a perineal approach. Int Urogynecol J Pelvic Floor Dysfunct [Internet]. 2009;20(3):S462–3. https://www.embase.com/records?subaction=viewrecord&rid=1&page=1&id=L70076782
15. Geltzeiler CB, Birnbaum EH, Silviera ML, et al. Combined rectopexy and sacrocolpopexy is safe for correction of pelvic organ prolapse. Int J Colorectal Dis. 2018;33(10):1453-1459. doi:10.1007/s00384-018-3140-5
16. Catanzarite T, Klaristenfeld DD, Tomassi MJ, Zazueta-Damian G, Alperin M. Recurrence of Rectal Prolapse After Surgical Repair in Women With Pelvic Organ Prolapse. Dis Colon Rectum. 2018;61(7):861-867. doi:10.1097/DCR.0000000000001023
17. Speed JM, Zhang CA, Gurland B, Enemchukwu E. Trends in the Diagnosis and Management of Combined Rectal and Vaginal Pelvic Organ Prolapse. Urology. 2021;150:188-193. doi:10.1016/j.urology.2020.05.010
18. Comprehensive Hospital Abstract Reporting System (CHARS): Washington State Department of Health. https://doh.wa.gov/dataandstatisticalreports/healthcareinwashington/hospitalandpatientdata/hospitaldischargedatachars. Accessed 18 Aug 2020
19. Washington Data & Research Population Estimates. https://www.ofm.wa.gov/washington-data-research/population-demographics/population-estimates/estimates-april-1-population-age-sex-race-and-hispanic-origin
20. Rogers AC, McCawley N, Hanly AM, Deasy J, McNamara DA, Burke JP. Trends in the treatment of rectal prolapse: a population analysis. Int J Colorectal Dis. 2018;33(4):459-465. doi:10.1007/s00384-018-2971-4
21. El-Dhuwaib Y, Pandyan A, Knowles CH. Epidemiological trends in surgery for rectal prolapse in England 2001-2012: an adult hospital population-based study. Colorectal Dis. 2020;22(10):1359-1366. doi:10.1111/codi.15094
22. Wijffels N, Cunningham C, Dixon A, Greenslade G, Lindsey I. Laparoscopic ventral rectopexy for external rectal prolapse is safe and effective in the elderly. Does this make perineal procedures obsolete?. Colorectal Dis. 2011;13(5): 561-566. doi:10.1111/j.1463-1318.2010.02242.x
23. Gunner CK, Senapati A, Northover JM, Brown SR. Life after PROSPER. What do people do for external rectal prolapse?. Colorectal Dis. 2016; 18(8):811-814. doi:10.1111/codi.13255
24. Young MT, Jafari MD, Phelan MJ, et al. Surgical treatments for rectal prolapse: how does a perineal approach compare in the laparoscopic era?. Surg Endosc. 2015;29(3):607-613. doi:10.1007/s00464-014-3707-3
25. Clark CE 3rd, Jupiter DC, Thomas JS, Papaconstantinou HT. Rectal prolapse in the elderly: trends in surgical management and outcomes from the American College of Surgeons National Surgical Quality Improvement Program database. J Am Coll Surg. 2012;215(5):709-714. doi:10.1016/j.jamcollsurg.2012.07.004
26. Lee SH, Lakhtaria P, Canedo J, Lee YS, Wexner SD. Outcome of laparoscopic rectopexy versus perineal rectosigmoidectomy for full-thickness rectal prolapse in elderly patients. Surg Endosc. 2011; 25(8):2699-2702. doi:10.1007/s00464-011-1632-2
27. McCoy AC, Gasevic E, Szlabick RE, Sahmoun AE, Sticca RP. Are open abdominal procedures a thing of the past? An analysis of graduating general surgery residents’ case logs from 2000 to 2011. J Surg Educ. 2013;70(6):683-689. doi:10.1016/j.jsurg.2013.09.002
28. Unruh KR, Bastawrous AL, Bernier GV, et al. Evaluating the Regional Uptake of Minimally Invasive Colorectal Surgery: a Report from the Surgical Care Outcomes Assessment Program. J Gastrointest Surg. 2021;25(9):2387-2397. doi:10.1007/s11605-020-04875-1
29. van Zanten F, van der Schans EM, Consten ECJ, et al. Long-term Anatomical and Functional Results of Robot-Assisted Pelvic Floor Surgery for the Management of Multicompartment Prolapse: A Prospective Study. Dis Colon Rectum. 2020;63(9): 1293-1301. doi:10.1097/DCR.0000000000001696
30. Diaz A, Schoenbrunner A, Cloyd J, Pawlik TM. Geographic Distribution of Adult Inpatient Surgery Capability in the USA. J Gastrointest Surg. 2019;23(8):1652-1660. doi:10.1007/s11605-018-04078-9
31. Finlayson SR, Birkmeyer JD, Tosteson AN, Nease RF Jr. Patient preferences for location of care: implications for regionalization. Med Care. 1999;37(2):204-209. doi:10.1097/00005650-199902000-00010
32. Ellis RJ, Yuce TK, Hewitt DB, et al. National Evaluation of Patient Preferences in Selecting Hospitals and Health Care Providers. Med Care. 2020;58(10):867-873. doi:10.1097/MLR.0000000000001374
33. Xu Z, Aquina CT, Justiniano CF, et al. Centralizing Rectal Cancer Surgery: What Is the Impact of Travel on Patients?. Dis Colon Rectum. 2020;63(3):319-325. doi:10.1097/DCR.0000000000001581
34. Consten EC, van Iersel JJ, Verheijen PM, Broeders IA, Wolthuis AM, D’Hoore A. Long-term Outcome After Laparoscopic Ventral Mesh Rectopexy: An Observational Study of 919 Consecutive Patients. Ann Surg. 2015;262(5):742-748. doi:10.1097/SLA.0000000000001401
35. van Iersel JJ, Paulides TJ, Verheijen PM, Lumley JW, Broeders IA, Consten EC. Current status of laparoscopic and robotic ventral mesh rectopexy for external and internal rectal prolapse. World J Gastroenterol. 2016;22(21):4977-4987. doi:10.3748/wjg.v22.i21.4977