





Trust and Policy in Global Health Crises: A Review
The Personal-Policy Collision: Messaging, Trust, and Behavioral Response in a Global Health Crisis
Thomas Kieber-Emmons
- Department of Pathology, University of Arkansas for Medical Sciences, Little Rock AR, 72202
OPEN ACCESS
PUBLISHED: 31 May 2025
CITATION: Kieber-Emmons, T., 2025. The Personal-Policy Collision: Messaging, Trust, and Behavioral Response in a Global Health Crisis. Medical Research Archives, [online] 13(5).
https://doi.org/10.18103/mra.v13i5.6510
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i5.6510
ISSN 2375-1924
ABSTRACT
The Coronavirus disease 2019 (COVID-19) pandemic brought to light the complex interplay between individual behavior and institutional policy. During the global health crisis, it highlighted how public health messaging, levels of trust in authorities, and personal values shape behavioral responses. Here we review elements of the effectiveness and pitfalls of health communication strategies, the role of trust in government and healthcare systems, and how these factors influence individual compliance or resistance to public policy. By drawing on qualitative and quantitative insights from the literature, lessons are learned for more effective, culturally sensitive public health messaging and communication styles, and showcased for future public health emergencies.
Keywords
COVID-19, public health, messaging, trust, behavioral response
Introduction
The Coronavirus disease 2019 (COVID-19) pandemic forced individuals, communities and nations to navigate the many challenges posed by the spread of the virus. Public policy during a pandemic often requires difficult trade-offs, and these trade-offs resonate differently depending on one’s unique perspective and experience¹. Policies, while necessary for public health, often collided with perspectives of personal freedoms, individual and community economic needs, and social/cultural considerations. Governments had to quickly implement measures to limit the spread of the virus, such as lockdowns, mask mandates, travel restrictions, and eventually vaccine rollouts, creating tension between the public’s personal choices and the collective needs of society²–⁵. Personal experiences were shaped by a variety of factors, such as the severity of the virus in a region, personal health conditions, individual economic impact, and the level of trust in public health information. This collision created tension between the public’s personal choices and the collective needs of society. This complex intersection of personal and public health challenges, requires governments to balance public safety with individual and community socioeconomic well-being⁶–⁸.
Communication and messaging play a pivotal role in mediating the tension between individual choices and collective societal needs during a health crisis⁹–¹². Messaging focuses on the content of the information itself, while communication encompasses the entire process of sharing, receiving, and interpreting messages, including the channel and context. When messaging is clear, consistent, and empathetic, it can bridge the gap between personal autonomy and public responsibility by helping individuals understand why certain policies exist and how their behavior impacts others. However, when communication is confusing, inconsistent, overly technical, or delivered without cultural sensitivity, it can intensify the collision—people may feel alienated, mistrustful, or manipulated, leading to resistance or noncompliance. Messaging also frames the narrative: if it emphasizes solidarity and mutual care, it can align personal values with collective goals. But if it comes off as coercive or top-down, it may provoke defensiveness or skepticism, deepening the divide. In this way, messaging doesn’t just convey information—it actively shapes how people interpret the crisis and make choices within it.
The pandemic not only highlighted the fragile balance between public policy and personal experience but also illuminated the multifaceted challenges of aligning individual behaviors with collective health goals. This tension revealed the need for public health strategies that are not solely grounded in epidemiological data, but that also account for the psychological, cultural, and socioeconomic dimensions of individual decision-making. At the heart of this balancing act lies the role of trust—trust in government institutions, in scientific expertise, and in the information being communicated. The success or failure of health interventions often depended not just on the policies themselves, but on how those policies were conveyed and perceived. Thus, the pandemic underscored the essential role of communication—not merely as a tool for information dissemination, but as a dynamic process through which public understanding, emotional response, and behavioral compliance are shaped.
The aim and scope of this review is to highlight literature that underscores how trust and communication intersect with policy implementation and personal experience, offering critical insights for designing more responsive, equitable, and effective public health responses in future global crises. Four key areas are emphasized: (i) Public Health versus Personal Economic Consequences, (ii) Public Trust and Individual Responsibility, (iii) Messaging and Public Trust, and (iv) Communication and Personal Trust. These four domains warrant emphasis because they represent the core tensions and mechanisms that shaped individual and collective responses during the COVID-19 pandemic. First, the trade-off between public health and personal economic consequences reflects a critical axis of conflict, where policies aimed at controlling viral spread often led to job losses, financial instability, and broader
economic strain, disproportionately affecting marginalized populations. Second, public trust and individual responsibility are tightly interlinked; the effectiveness of health policies hinges on the extent to which individuals trust institutions and internalize responsibility for protecting community health. Third, messaging plays a vital role in cultivating or eroding public trust—clear, transparent, and empathetic communication fosters understanding and compliance, while inconsistent or politicized messaging can generate skepticism and resistance. Lastly, communication and personal trust underscore the relational and emotional dimensions of health governance; how people interpret, respond to, and emotionally process public health guidance is deeply rooted in their trust in both the messenger and the message. Together, these four domains encapsulate the interplay of structural, psychological, and communicative factors that must be examined to fully understand behavioral responses in a global health crisis and to inform more effective policy design in the future.
1. Public Health versus Personal Economic Consequences
Public health policy and personal health outcomes are two critical and interrelated aspects of society and individual well-being¹³–¹⁴. These domains frequently intersect, and decisions made in one area influence the other. They highlight the complex relationship between public health and personal and socioeconomic and health outcomes, especially in times of crisis¹⁵. Economic balance needs to consider that while public health measures may be necessary, they often come with significant economic costs¹⁶–¹⁷. The public health crisis led to widespread economic consequences—job losses, business closures, and financial hardship for many individuals¹⁸. Public policy therefore must balance public health measures with economic realities¹⁹–²¹ that impact individuals and communities²²–²³.
Globally, the pandemic tested healthcare systems, overwhelmed hospitals, and exposed gaps in infrastructure, especially in low-income areas¹⁷. Governments were also faced with urgent decisions about how to protect public health while managing the long-term mental health impacts of the pandemic²⁴–²⁶. Economic distress can worsen public health outcomes (e.g., stress, mental health issues, or lack of access to health services). Navigating the balance of these domains is key for ensuring both a healthy society and individual stability.
Policies that prioritize economic growth without addressing public health needs (e.g., underfunding healthcare systems) can also lead to worse health outcomes and increased long-term economic burdens²⁷. The ideal approach is often one that finds a balance: promoting policies that both protect public health and minimize economic harm²⁸. For example, providing financial support for individuals during health crises (e.g., unemployment benefits, paid sick leave) can help reduce personal economic consequences while still prioritizing public health goals. In the US, financial assistance was offered as a stimulus package to offset the economic impact of the pandemic²⁹.
Healthcare costs should be considered including the personal financial burden of accessing health services, including insurance premiums, out-of-pocket expenses for medical care, and long-term costs for chronic illness management³⁰–³¹. For the future, a well-funded, effective public health system can reduce the personal economic burden of healthcare costs³². Conversely, an inefficient or costly healthcare system can exacerbate the financial strain on individuals, especially in cases of chronic illness or major health emergencies³³. Some have estimated that a single-payer universal healthcare system would have saved 212,000 lives in 2020 alone³⁴.
A primary challenge of the healthcare system was ensuring equitable access to vaccines, treatments, and healthcare, particularly for vulnerable populations. The pandemic exposed deep-seated social inequalities³⁵, revealing gaps in public health infrastructure³⁶, particularly in low-income regions, and highlighted the importance of global cooperation in tackling health crises³⁷–³⁸. Due to the pandemic,
it was found probable that a significant portion of Americans that were uninsured were less likely to seek medical care for COVID-19 symptoms³⁹. People in marginalized and rural communities often face higher infection rates and more severe outcomes, partly due to preexisting health disparities and systemic factors such as limited access to healthcare, crowded living conditions, and employment in essential jobs that couldn’t be done remotely⁴⁰–⁴¹. Policy decisions must address issues of equity, as marginalized communities are typically disproportionately affected by both disease and the economic fallout⁴²–⁴³.
The COVID-19 pandemic had profound and lasting impacts on both public policy and personal economic circumstances. Going forward, both public policy and personal economic conditions need evolve to reflect the lessons learned from the pandemic⁴⁴. For example, Public Health systems are adapting to prioritize pandemic preparedness, leading to stronger public health frameworks⁴⁵–⁴⁶. In a post-COVID world, the economic landscape will likely continue to evolve, and people will need to adapt in various ways. The pandemic highlighted how important it is to have financial resilience. For some, the pandemic was a catalyst for personal reinvention or financial growth, while for others, it highlighted vulnerabilities that continue to affect their financial stability and job security. People may be more focused on building emergency savings, investing wisely, and diversifying income sources. COVID-19 also sparked creativity in terms of new business models. The pandemic exposed the importance of mental health and work-life balance, especially with the rise of burnout from remote work. The ultimate impact on personal economic well-being varies widely, depending on one’s industry, location, and access to resources. The pandemic has shown that the ability to pivot and diversify is key to thriving in an uncertain world. Moving forward, people need to adapt by being more flexible, tech-savvy, financially aware, and mindful of mental and physical well-being.
2. Public Trust and Individual Responsibility
Personal responsibility shifted significantly during the pandemic, influenced by both individual actions and broader societal expectations. COVID-19 reshaped daily life, creating psychological distress based upon the message and communication style⁴⁷. The personal perspective varied greatly depending on one’s experiences, values, and priorities, such as health risks, financial strain, social isolation, and uncertainty⁴⁸–⁴⁹. Individuals faced personal concerns about how to protect themselves and their loved ones while managing their daily life⁵⁰. Hence, the pandemic highlighted personal values, fears, and priorities⁵¹–⁵², influencing how individuals heard a message and perceived public policy⁵³–⁵⁴.
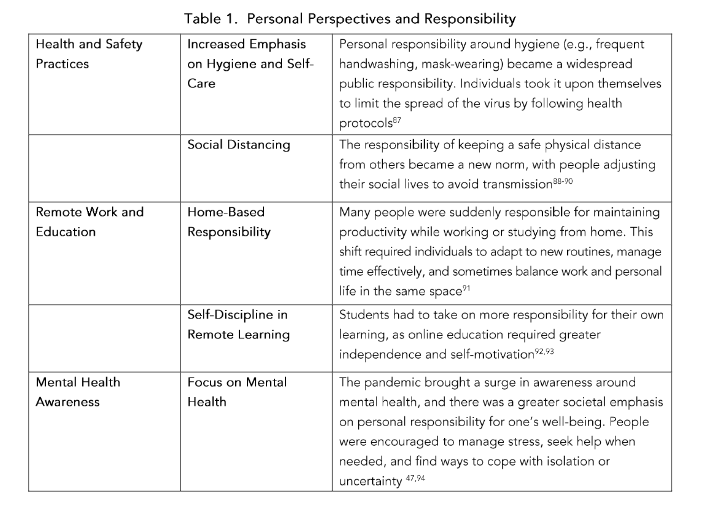
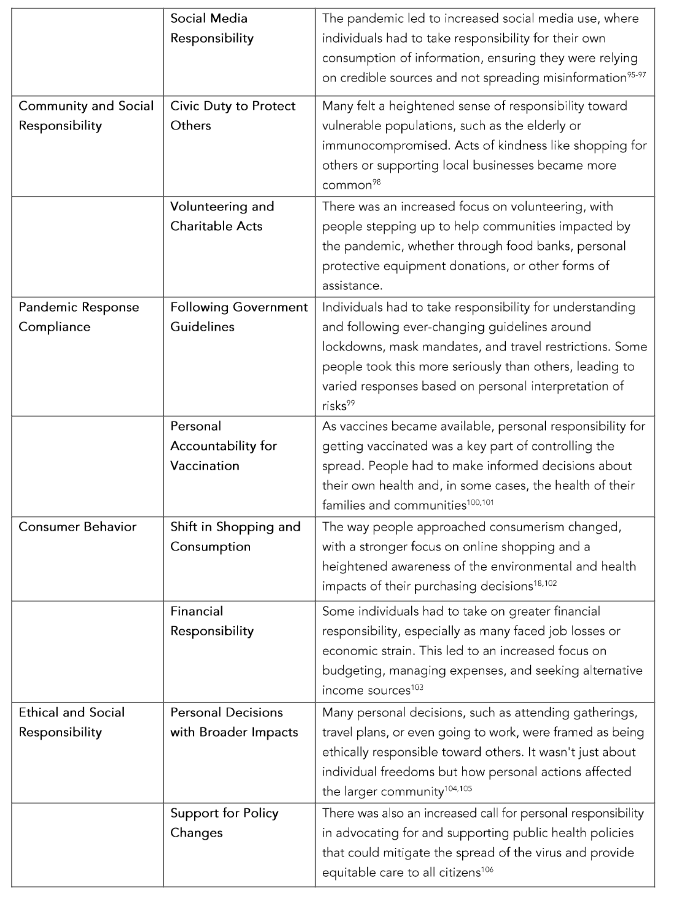
While some individuals prioritized personal freedoms and questioned mandates, others emphasized the need for solidarity in the face of the global crisis, understanding that collective action was necessary to overcome the pandemic⁵⁵. Individual responsibility seems therefore to be reflective of emotional status and education⁵⁶–⁵⁷. Personal responsibility for health has been framed as a contested criterion⁵⁸. Underlying the concept of personal choice is consideration of freedom and societal debt which is not necessarily aligned⁵⁸. However, during a Pandemic, personal and social responsibilities can co-exist which can influence and determine health care priority based on personal responsibility (Table 1).
Personal responsibility during COVID-19 expanded beyond the individual to include communal and societal aspects⁵⁹–⁶¹. It required individuals to adapt to rapidly changing circumstances, take ownership of their health, and consider the well-being of others. People who prioritize personal freedom might see public health policies as intrusive, while those who prioritize collective safety might view them as necessary protective measures for society at large⁶². Consequently, there needs to be careful consideration of legal and ethical frameworks in messaging. Because of the global nature of
pandemics, international and national laws should be considered when implementing pandemic-related restrictions⁶³. Rights such as freedom of movement, privacy, and expression need to be weighed against the need to protect the public and communicated thoughtfully. Ethical dilemmas are important to discuss in open forums without confirmation bias. Decisions about how to allocate scarce resources (e.g., ventilators, vaccines) often involve ethical trade-offs.
Trust in government and public health recommendations plays a significant role in how policies are received⁶⁴. The pandemic affected everyone differently, with different people experiencing varying levels of risk and hardship⁶⁵. Some individuals may have felt that governments overreached or made decisions without sufficient transparency, undermining trust⁶⁶. Others may feel that individual freedoms were disrespected, such as the right to choose whether to follow mask mandates or get vaccinated⁶⁷. Ultimately, the pandemic underscored the need for coordinated global action, trust in authorities, and a balance between individual rights and collective action⁶⁸–⁶⁹. It also sparked broader debates on government roles, individual autonomy, and solidarity, with lessons learned to guide future health crises⁷⁰.
Public health officials and Governments must consider how to mitigate such impacts, especially for vulnerable populations⁷¹. The pandemic highlighted and often worsened social inequalities, with marginalized communities bearing the brunt of both the health crisis and its economic fallout. Personal experiences of these inequalities—whether in terms of healthcare access, job security, or housing instability—can shape one’s stance on government intervention and public policy. A person from a disadvantaged background might feel that government intervention is critical to provide support in the form of financial aid, healthcare access, and social services, arguing for more robust public policy. Conversely, an individual with greater economic resources may believe that the market and personal responsibility should play a larger role in navigating the pandemic’s effects. Public trust can increase when leaders and health organizations show empathy for people’s struggles—whether they are dealing with illness, economic hardship, or social isolation⁷². Ensuring that social safety nets are strong and that these communities are supported is an essential part of a balanced response.
The liberties of individuals need to be considered in public health measures⁷³. However, the public health response to the pandemic also needed to prioritize population health. It was argued that populations have a collective right to public health, meriting the restriction of individual liberties where necessary and proportionate to protecting public health⁷⁴–⁷⁵. Measures like quarantine, vaccination mandates, mask-wearing, and social distancing were considered necessary to slow the spread of disease. Given the gravity of the pandemic, indirect evidence of benefit combined with the low risk of harm was considered to outweigh the absence of direct evidence⁷⁶. However, these measures were thought to infringe on personal freedoms, leading to debates about how far governments should go in enforcing these policies⁷⁵. While a majority of individuals followed mask mandates, there was a portion of those who did not⁷⁷. It seems this negative attitude resulted from a perception of ineffectiveness and psychological reactance⁷⁷. A growing body of research is showing that health messages are often more effective when they are tailored to match important characteristics of the recipient⁷⁸–⁷⁹.
There is individual confirmation bias as people are prone to misinterpreting evidence about vaccines, for example, in ways that reflect their underlying beliefs⁸⁰. Hence, confirmation bias is an important consideration in messaging and in communication style. Striking a balance between ensuring public safety and respecting personal freedoms can be challenging and need fine tuning for the future. For example, it is clear masking, and social distancing can thwart transmission of a virus as evidenced of reduction of flu numbers during the pandemic⁸¹. Even before COVID-19, data supported the utility of masking to reduce viral transmission of influenza⁸². Hence, better tailored messaging of such associations
could have helped convey trust. However, each person also has a responsibility to contribute positively to these spaces by avoiding harmful language and respectfully disagreeing with others.
Individuals may take a nationalistic view, emphasizing the importance of prioritizing their own country’s needs³. Public policy decisions during COVID-19 have often pitted national interests against global cooperation³⁸. Countries have had to weigh the importance of securing vaccines and resources for their own citizens versus the moral responsibility to help other nations facing severe challenges. Others may argue from a humanitarian perspective, believing that helping poorer nations will ultimately benefit everyone in the global fight against the virus⁸⁴. The importance of personal responsibility in preventing the spread of infectious diseases is now clearer.
The pandemic forced many to confront mental health challenges. The isolation and uncertainty brought by COVID-19 made individuals more aware of the importance of resilience, mental well-being, and the need to maintain social connections, even if virtually⁸⁵. The development and rollout of COVID-19 vaccines sparked debates about vaccine hesitancy. While many embraced vaccinations as essential for community health, others raised concerns about safety and efficacy⁸⁶. This has led to a more critical reflection on the relationship between science, trust, and public health. Many have reevaluated their lifestyle and social habits. The pandemic forced individuals to adjust to remote work, virtual socializing, and redefined public spaces. Post-COVID, some individuals continue to value the flexibility of working from home and maintaining a greater work-life balance. The post-COVID world will likely see a continued focus on public health systems’ capacity to manage infectious diseases, while personal responsibility for health will remain key. There will be more collaboration between governments, healthcare providers, and individuals to manage future health threats and create a healthier, more equitable society.
3. Messaging and Public Trust
Probably the most important component of dealing with a pandemic is communication and messaging whether it’s from governments, organizations, scientists, politicians, medical professionals or individuals. During the COVID-19 pandemic, messaging (both official and social) played a critical role in shaping public behavior and individual trust in health guidelines. The pandemic created a challenging environment where the balance between public health messaging, trust in institutions, and personal beliefs was often tested. Messaging around COVID-19 played a critical role in shaping public trust, adherence to public health guidelines, and overall responses to the pandemic¹⁰⁷–¹⁰⁸. Clear and transparent communication about the need for certain policies is essential to maintain trust. When individuals understand the rationale behind policies, they are more likely to comply voluntarily¹⁰⁹. Fear and confusion in messaging often lends to the spread of misinformation and disinformation¹¹⁰.
The way governments, health organizations, and even the media communicated about the virus, its spread, and the measures to protect public health had a significant impact on the public’s willingness to trust the information and follow recommended actions. Both public health authorities and the public had to adapt and display responsiveness to messaging. As the pandemic progressed, public health authorities had to adapt their strategies. This was especially true when new variants of the virus emerged or when vaccines became widely available⁵,¹¹¹–¹¹². Public trust could be maintained when authorities communicated that adaptations were based on new evidence and evolving understanding of the virus¹¹³. The public generally appreciated honest updates and explanations for why things were changing, even if the situation was complex and fluid¹¹⁴.
Yet, the spread of misinformation can undermine public health efforts and erode trust in health authorities. Governments and organizations had to develop, distribute, and monitor vaccines at an unprecedented pace, all while managing public trust and navigating misinformation about the virus¹¹⁵. Efforts to counter false narratives and promote accurate information must be a priority to avoid polarization¹¹⁶. In many countries, COVID-19 became highly politicized. Political polarization and social media played a significant role in influencing the effectiveness of messaging, sometimes undermining public trust¹¹⁷. Different political factions often presented contrasting messages about the virus, which contributed to confusion and division¹¹⁸. Politicized messaging hurt public trust, especially when leaders downplayed the severity of the virus or opposed public health measures¹¹⁹. Consequently, public health officials needed to work to keep their messaging non-partisan and focused on scientific facts to maintain public trust across political lines.
False dichotomy analysis of key issues surrounding COVID-19 suggest that several false dichotomies were used to polarize debates while oversimplifying complex issues¹²⁰. These authors urge a nuanced understanding of the science and caution against black-or-white messaging, all-or-nothing guidance, and one-size-fits-all approaches. Still the messaging around COVID-19 policies demonstrated the importance of delicate balance between communicating facts, showing empathy, and responding to public concerns¹²¹. Some research suggests that messaging and communication style in and of itself does not lead to higher levels of trust and compliance but depend on existing high levels of trust with authorities¹²². This focuses attention to public relations by emphasizing the importance of establishing credibility prior to crises¹²².
Building trust also requires effort and a recognition that scientific work isn’t just about generating knowledge—it’s about helping the public understand its implications and limitations, rebuilding trust in science¹²³. While messaging that focused on science and expertise, while being adaptable to new information, and helped establish authority and trustworthiness¹²⁴, trust in science still took a hit¹²⁵. COVID-19 messaging was heavily reliant on scientific
data, but early in the pandemic, there was still much unknown about the virus. This left space for speculation, which could erode public trust¹²⁶. Weak or early-stage studies often received disproportionate attention, leading to confusion and sometimes misguided policy decisions¹²⁷. Given the urgency of the pandemic, the pressure to publish and find solutions quickly led to many studies being rushed or released with less rigorous methodologies, including small sample sizes, non-randomized designs, and lack of control groups¹²⁸. Despite these flaws, some of these studies were cited widely and sometimes used to influence policy, media narratives, or public health guidelines.
Another notable issue was the speed at which research was disseminated—sometimes in preprints or media outlets without thorough peer review¹²⁹. This made it easier for flawed research to gain traction. In some cases, findings that were later refuted or revised continued to shape public discourse, as the initial sensational headlines stuck with people more than the later corrections¹³⁰. (https://retractionwatch.com/retracted-coronavirus-covid-19-papers/). Additionally, there was a tendency for social media and different interest groups to latch onto studies that supported their existing positions, exemplifying confirmation bias¹²⁵,¹³¹. For instance, early research on hydroxychloroquine or masks, before large-scale, rigorous studies provided more clarity, created significant divisions in public opinion and policy decisions¹³²–¹³³. These early studies weren’t necessarily “bad,” but the context in which they were interpreted often led to inflated claims. The result is that some of the limitations, such as small sample sizes or the lack of generalizability, were downplayed in favor of drawing broad conclusions. In turn, this leads to an ongoing conversation about how future public health crises can better balance the need for speed with the need for rigor in research while managing misinformation¹²¹.
When experts fail to communicate their findings and explain their reasoning in an accessible and transparent way, it creates a vacuum where misinformation and distrust can thrive. When scientific advice appeared to change, it created doubt about the reliability of health experts¹³⁴. Communicating the science behind decisions—such as the basis for lockdowns, social distancing, or the development of vaccines—is essential for maintaining public trust. It is important to realize that a decline of public trust in scientific experts is often due to a lack of communication and not a distrust in science itself or scientists themselves¹³⁵. This is a significant challenge in today’s world, where scientific knowledge and expertise play a crucial role in decision-making, yet many people feel disconnected from or skeptical of those who hold that expertise because of a lack of clear messaging and communication approach.
Apart from local government organizations’ engagement strategies in COVID-related posts on social media¹³⁶, regular public engagement from scientists could have served to bridge this gap¹²³. Scientists often work in highly specialized fields, and the language they use can be difficult for the public to understand. This sometimes creates a barrier that makes people feel disconnected from the scientific process. However, when scientists take the time to explain their findings in clear, accessible language and engage in ongoing dialogue, it helps demystify their work and shows that their findings aren’t just abstract concepts but have real-world implications.
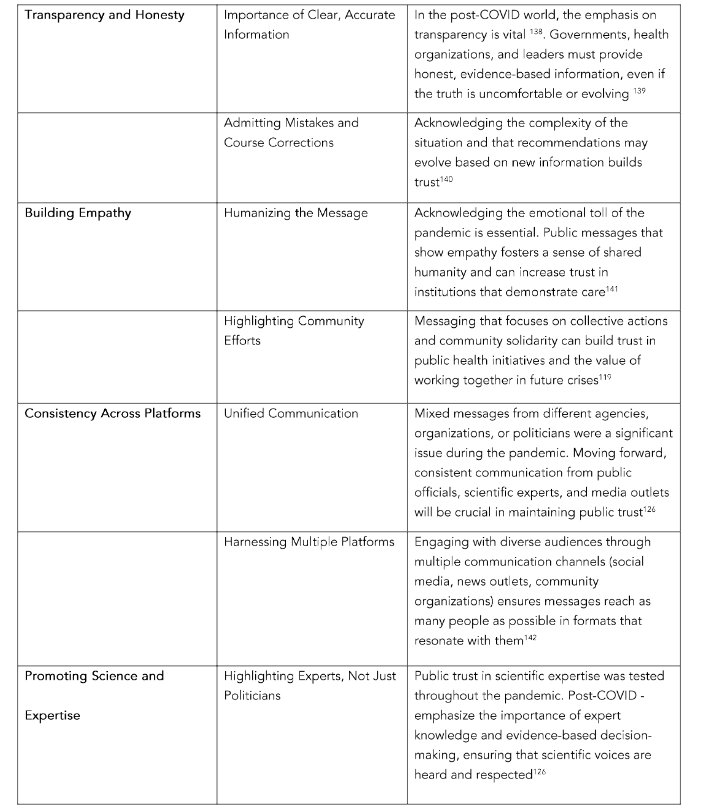
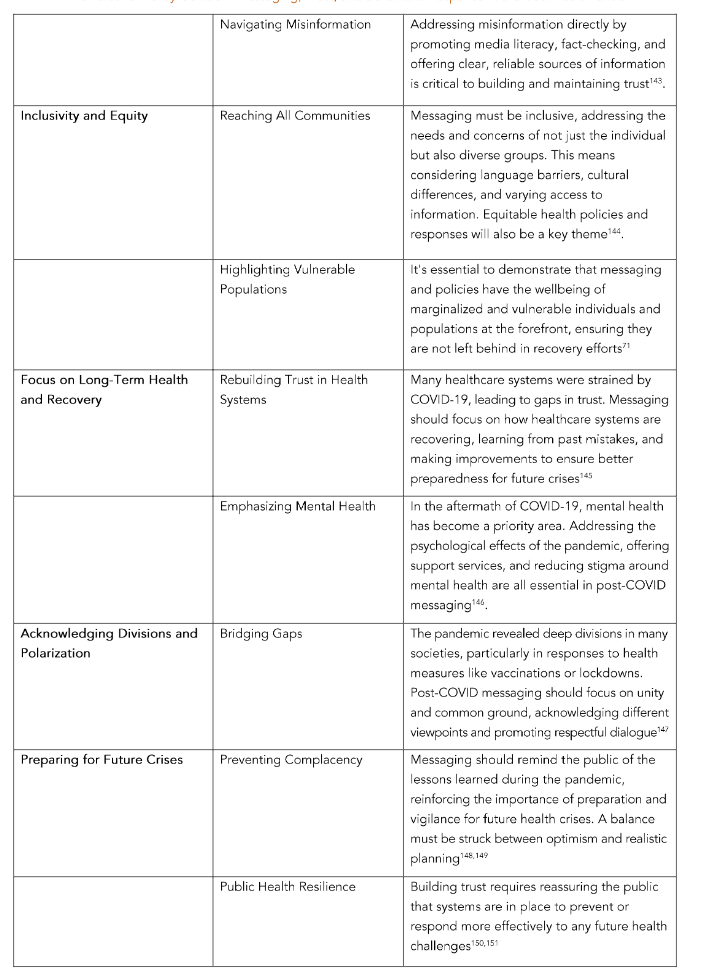
Post-pandemic messaging and public trust are deeply interconnected, as the pandemic has reshaped how people engage with information and institutions. Effective messaging in the post-pandemic era is crucial for rebuilding and maintaining individual and public trust, especially in areas like healthcare, public policy, and scientific research. Hence, clear messaging translating scientific results into tangible action that people can relate to in their daily lives is needed¹³⁷. Post-pandemic messaging and communication should be rooted in transparency, empathy, and a commitment to rebuilding trust. As people process the aftermath of the pandemic, institutions that embrace these principles will be better positioned to engage the public, reduce misinformation, and support recovery efforts. The goal is to create a more informed,
resilient society that can navigate future challenges with greater unity and confidence. Table 2 illustrates a few key themes and considerations for post-pandemic messaging.
Table 2. Key Themes to Foster Trust for Individuals and the Public
4. Communication and Personal Trust
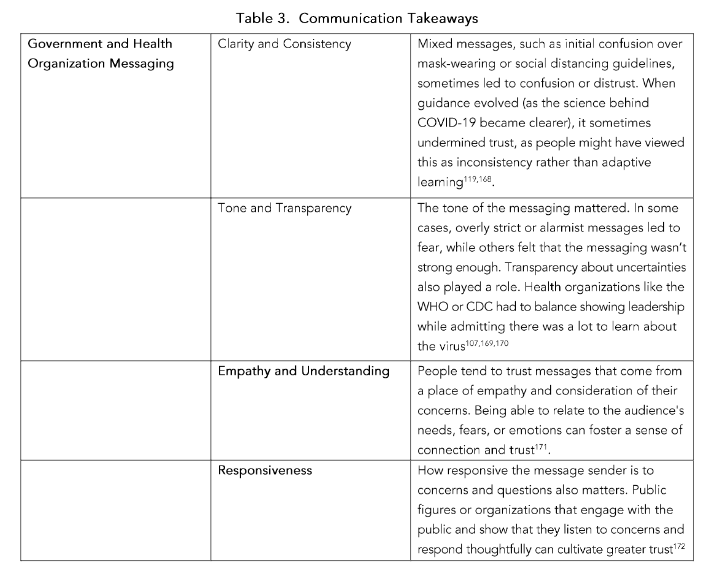
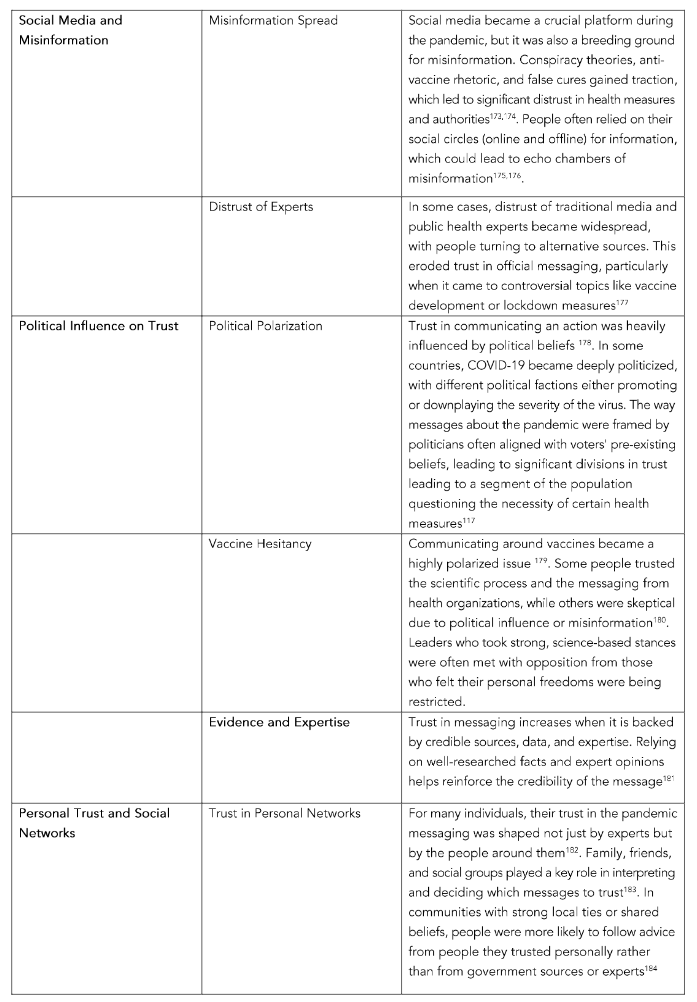
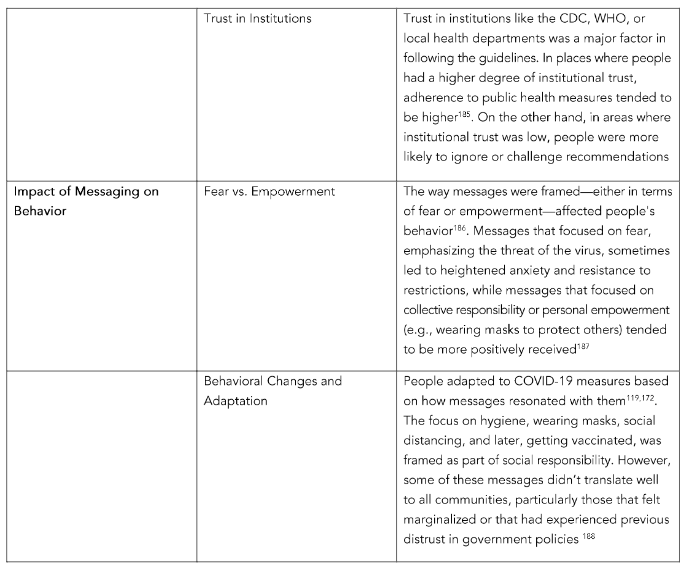
A challenge emerged as the virus spread and new data highlighted, requiring public health agencies and governments to adjust their strategies. Messaging that failed to acknowledge the diversity of experiences could alienate certain groups¹⁵². Table 3 illustrates key takeaways for effective communication in health-related campaigns. Sometimes, adjustments in policies or in presented information were seen as a lack of transparency, especially when certain early warnings about the virus were downplayed¹⁵³. When authorities were open about what was known and what wasn’t, it fostered trust¹⁵⁴. However, downplaying risks, failing to disclose challenges in managing the pandemic, or ignoring cultural experiences created skepticism and mistrust in the messaging¹⁵⁵.
While facts and guidelines are critical, showing understanding of the fears and concerns is equally important¹⁵⁶. Consequently, empathy and reassurance can help people feel heard and understood during crisis. Compassionate communication can help calm anxiety, making people feel supported rather than judged¹⁵⁷–¹⁵⁸. A tone that acknowledges the struggles and sacrifices people are facing helps build a stronger connection. Unfortunately, the tone of the messaging during the pandemic from leaders and health officials varied widely¹⁵⁹–¹⁶⁰.
Although there are valuable lessons to be learned from literature on patient-provider communication, communication between public health authorities and the general-public operates on a different level. Therefore, public health authorities must deliver targeted, customized messaging. In some countries, the messaging was more authoritative and urgent, while in others, it was more relaxed or politicized¹⁰⁸. In general, the tone needed to be empathetic, acknowledging the fear and uncertainty people felt. Public health officials who delivered messages with empathy and reassurance helped maintain public trust¹⁶¹.
From a personal perspective communication that provides transparency, clarity, and consistency is critical for building trust in pandemic messaging¹⁶². Transparency helps to reduce fear and uncertainty by providing accurate and timely information¹⁶³. When messaging is consistent, it reinforces the guidance and recommendations, making it easier for people to follow and feel confident in the decisions they’re making. Additionally, clarity is key. If messages are confusing or too complex, they can create skepticism or lead to misinformation.
One of the biggest obstacles to trust during the pandemic was the spread of misinformation and disinformation. Much of this type of information was brought about through social media and sharing among many¹⁴². Social media became a major platform for information (and misinformation) during the pandemic¹⁶⁴. Influencers played a role in shaping public opinion. Influences on social media ran rampant. False claims about cures, vaccines, or the virus’s origins spread rapidly through social media and news outlets¹⁶⁵. The prevalence of misinformation undermined trust in reliable sources of information. When people were exposed to conflicting narratives, particularly from social media or fringe groups, it became difficult to discern which sources were trustworthy. Efforts to combat misinformation—like fact-checking and promoting accurate sources—were necessary to maintain public trust, but misinformation often spread faster than efforts to counteract it¹⁶⁶–¹⁶⁷. However, results also show that while interventions can successfully reduce belief in false information, they can negatively impact the credibility of information¹⁶⁷.
Trust in information often depended on the credibility of the source. Social media platforms were pressured to regulate content to prevent misinformation, but their effectiveness was sometimes questioned¹⁶⁷. Social media offers a platform for people to connect, but it can also be a breeding ground for negativity, bullying, and toxic behavior¹⁴². In the age of instant news, misinformation and rumors spread easily. Social media users have a responsibility to fact-check what they share and to avoid spreading false or misleading information.
The communication takeaways are vital lessons learned from the pandemic, shaping how we approach communication in future crises, health messaging, and day-to-day interactions. Post-COVID communication should prioritize honesty, empathy, inclusivity, and a clear, consistent message that empowers people with the knowledge they need to navigate a rapidly changing world. It’s about learning from past mistakes and applying those lessons to ensure a more informed, prepared, and unified society moving forward. Post-COVID messaging should focus not only on the recovery of systems and infrastructure but also on individual and societal healing. Messages that offer hope, renewal, and optimism can be powerful. As the world recovers from the pandemic, messaging should reinforce the importance of long-term health strategies and pandemic preparedness, ensuring that lessons learned are applied to future crises.
Overall, the pandemic highlighted the importance of clear, consistent, and transparent messaging in fostering trust. Trust in health officials, governmental bodies, and personal social networks was crucial in determining how individuals responded to the pandemic. Messages that considered local contexts and offered clear, actionable guidance were more effective than those that created confusion or were seen as politically driven. It also underlined the role that misinformation, political views, and personal beliefs can have on public health efforts. Moving forward, learning how to communicate effectively in times of crisis—and how to build trust in institutions—will be critical for managing future public health challenges.
Table 3. Communication TakeawayS
Conclusion
The COVID-19 pandemic has been a unique confluence of personal and public health challenges, forcing individuals to make difficult decisions about their health while highlighting systemic inequalities and the need for global cooperation in responding to health crises. The intersection of personal and public health challenges in a COVID-19 world highlights the delicate balance between individual rights and collective responsibility. In the early stages of the pandemic, information about COVID-19 was rapidly evolving. Public health focuses on the health of populations, seeking to prevent disease, promote wellness, and ensure equitable access to healthcare. This sometimes led to conflicting messages, particularly about preventive measures like mask-wearing, social distancing, or the effectiveness of certain treatments. Inconsistent messaging from health authorities, government leaders, and media outlets created confusion.
The policy quandary at the heart of the crisis was not just about statistics or public health models—it was about the impact on real people, with complex lives with varying concerns, making it an intensely personal matter for many. For many, the question becomes: How do we balance the lives at risk from the virus with the financial and mental health challenges caused by prolonged restrictions? An individual who loses their job or faces financial instability due to restrictions might argue for a quicker reopening, prioritizing economic recovery. However, someone with vulnerable health conditions or who has lost loved ones to the virus might support stronger lockdowns to preserve public health, even at the cost of economic hardships.Striking the right balance between individual responsibilities and collective responsibilities is a dynamic and evolving challenge in the face of pandemics. It involves navigating complex ethical, legal, and social considerations. Future pandemic preparedness must focus on building trust, equity, and flexibility, while also ensuring the protection of both individual freedoms and public health.
Conflict of Interest
None
Funding Source
None
References
1. Norheim OF, Abi-Rached JM, Bright LK, et al. Difficult trade-offs in response to COVID-19: the case for open and inclusive decision making. Nat Med. 2021;27(1):10-13. doi: 10.1038/s41591-41020-01204-41596.
2. Martin S, Vanderslott S. “Any idea how fast ‘It’s just a mask!’ can turn into ‘It’s just a vaccine!'”: From mask mandates to vaccine mandates during the COVID-19 pandemic. Vaccine. 2022;40(51):7488-7499. doi: 7410.1016/j.vaccine.2021.7410.7031. Epub 2021 Oct 7428.
3. Bardosh K, de Figueiredo A, Gur-Arie R, et al. The unintended consequences of COVID-19 vaccine policy: why mandates, passports and restrictions may cause more harm than good. BMJ Glob Health. 2022;7(5):e008684. doi: 008610.001136/bmjgh-002022-008684.
4. Attwell K, Rizzi M, McKenzie L, et al. COVID-19 vaccine Mandates: An Australian attitudinal study. Vaccine. 2022;40(51):7360-7369. doi: 7310.1016/j.v accine.2021.7311.7056. Epub 2021 Nov 7330.
5. Grubaugh ND, Hodcroft EB, Fauver JR, Phelan AL, Cevik M. Public health actions to control new SARS-CoV-2 variants. Cell. 2021;184(5):1127-1132. doi: 1110.1016/j.cell.2021.1101.1044. Epub 2021 Jan 1129.
6. Moti UG, Goon DT. Novel Coronavirus Disease: A delicate balancing act between health and the economy. Pak J Med Sci. 2020;36(COVID19-S4): S134-S137. doi: 110.12669/pjms.12636.COVI D12619-S12664.12751.
7. Whitsel LP, Ajenikoko F, Chase PJ, et al. Public policy for healthy living: How COVID-19 has changed the landscape. Prog Cardiovasc Dis. 2023; 76:49-56.(doi):10.1016/j.pcad.2023.1001.1002. Epub 2023 Jan 1020.
8. Alizadeh H, Sharifi A, Damanbagh S, Nazarnia H, Nazarnia M. Impacts of the COVID-19 pandemic on the social sphere and lessons for crisis management: a literature review. Nat Hazards. 2023;10:1-26.
9. Chiu KH, Sridhar S, Yuen KY. Preparation for the next pandemic: challenges in strengthening surveillance. Emerg Microbes Infect. 2023;12(2):22 40441. doi: 2240410.2241080/22221751.2222202 3.22240441.
10. Serchen J, Cline K, Mathew S, Hilden D. Preparing for Future Pandemics and Public Health Emergencies: An American College of Physicians Policy Position Paper. Ann Intern Med. 2023;176 (9):1240-1244. doi: 1210.7326/M1223-0768. Epub 2023 Jul 1225.
11. Peng W, Berry EM. Coping with the Challenges of COVID-19 Using the Sociotype Framework: A Rehearsal for the Next Pandemic. Rambam Maimonides Med J. 2021;12(1):e0005. doi: 0010.5041/RMMJ.10425.
12. Sachs JD, Karim SSA, Aknin L, et al. The Lancet Commission on lessons for the future from the COVID-19 pandemic. Lancet. 2022;400(1035 9):1224-1280. doi: 1210.1016/S0140-6736(1222) 01585-01589. Epub 02022 Sep 01514.
13. Braveman P, Gottlieb L. The social determinants of health: it’s time to consider the causes of the causes. Public Health Rep. 2014;129 Suppl 2(Suppl 2):19-31. doi: 10.1177/0033354914 1291S00333549141206.
14. Ruggeri K, Garcia-Garzon E, Maguire Á, Matz S, Huppert FA. Well-being is more than happiness and life satisfaction: a multidimensional analysis of 21 countries. Health Qual Life Outcomes. 2020;18(1):192. doi: 110.1186/s12955-12020-01423-y.
15. Lu X, Lin Z. COVID-19, Economic Impact, Mental Health, and Coping Behaviors: A Conceptual Framework and Future Research Directions. Front Psychol. 2021;12:759974. (doi):10.3389/fpsyg.202 1.759974. eCollection 752021.
16. Turner HC, Sandmann FG, Downey LE, et al. What are economic costs and when should they be used in health economic studies? Cost Eff Resour Alloc. 2023;21(1):31. doi: 10.1186/s12962-12023-00436-w.
17. Emanuel EJ, Persad G, Upshur R, et al. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N Engl J Med. 2020;382(21):2049-2055. doi: 2010.1056/NEJMsb2005114. Epub 2002020 Mar 2005123.
18. Das D, Sarkar A, Debroy A. Impact of COVID-19 on changing consumer behaviour: Lessons from an emerging economy. Int J Consum Stud. 2022; 46(3):692-715. doi: 610.1111/ijcs.12786. Epub 12022 Feb 12714.
19. Gostin LO, Wiley LF. Governmental Public Health Powers During the COVID-19 Pandemic: Stay-at-home Orders, Business Closures, and Travel Restrictions. JAMA. 2020;323(21):2137-2138. doi: 2110.1001/jama.2020.5460.
20. Liebst LS, Ejbye-Ernst P, de Bruin M, Thomas J, Lindegaard MR. No evidence that mask-wearing in public places elicits risk compensation behavior during the COVID-19 pandemic. Sci Rep. 2022;12(1):1511. doi: 1510.1038/s41598-41022-05270-41593.
21. Binka M, Adu PA, Jeong D, et al. The Impact of Mask Mandates on Face Mask Use During the COVID-19 Pandemic: Longitudinal Survey Study. JMIR Public Health Surveill. 2023;9:e42616. (doi):10.2196/42616.
22. Asamani JA, Alugsi SA, Ismaila H, Nabyonga-Orem J. Balancing Equity and Efficiency in the Allocation of Health Resources-Where Is the Middle Ground? Healthcare (Basel). 2021;9(10):1257. doi: 1210.3390/healthcare9101257.
23. Andraska EA, Alabi O, Dorsey C, et al. Health care disparities during the COVID-19 pandemic. Semin Vasc Surg. 2021;34(3):82-88. doi: 10.1053/j.s emvascsurg.2021.1008.1002. Epub 2021 Aug 1059.
24. Jeffers A, Meehan AA, Barker J, et al. Impact of Social Isolation during the COVID-19 Pandemic on Mental Health, Substance Use, and Homelessness: Qualitative Interviews with Behavioral Health Providers. Int J Environ Res Public Health. 2022;19(19):12120. doi: 12110.13390/ijerph19191 2120.
25. Clemente-Suárez VJ, Martínez-González MB, Benitez-Agudelo JC, et al. The Impact of the COVID-19 Pandemic on Mental Disorders. A Critical Review. Int J Environ Res Public Health. 2021;18 (19):10041. doi: 10010.13390/ijerph181910041.
26. Bourmistrova NW, Solomon T, Braude P, Strawbridge R, Carter B. Long-term effects of COVID-19 on mental health: A systematic review. J Affect Disord. 2022;299:118-125. (doi):10.1016/j.j ad.2021.1011.1031. Epub 2021 Nov 1016.
27. Bauer UE. Community Health and Economic Prosperity: An Initiative of the Office of the Surgeon General. Public Health Rep. 2019;134 (5):472-476. doi: 410.1177/0033354919867727. Epub 0033354919862019 Aug 0033354919867716.
28. Kass NE. An ethics framework for public health. Am J Public Health. 2001;91(11):1776-1782. doi: 1710.2105/ajph.1791.1711.1776.
29. Asebedo SD, Quadria TH, Gray BT, Liu Y. The Psychology of COVID-19 Economic Impact Payment Use. J Fam Econ Issues. 2022;43(2):239-260. doi: 210.1007/s10834-10021-09804-10831. Epub 12021 Nov 10820.
30. Crowley R, Daniel H, Cooney TG, Engel LS. Envisioning a Better U.S. Health Care System for All: Coverage and Cost of Care. Ann Intern Med. 2020; 172(2 Suppl):S7-S32. doi: 10.7326/M7319-2415.
31. Rajabi M, Rezaee M, Omranikhoo H, et al. Cost of Illness of COVID-19 and Its Consequences on Health and Economic System. Inquiry. 2022;59:469580221144398.(doi):10.1177/00469580221144398.
32. Yerramilli P, Chopra M, Rasanathan K. The cost of inaction on health equity and its social determinants. BMJ Glob Health. 2024;9(Suppl 1): e012690. doi: 012610.011136/bmjgh-012023-012690.
33. Hanson K, Brikci N, Erlangga D, et al. The Lancet Global Health Commission on financing primary health care: putting people at the centre. Lancet Glob Health. 2022;10(5):e715-e772. doi: 710.1016/S2214-1109X(1022)00005-00005. Epub 02022 Apr 00004.
34. Galvani AP, Parpia AS, Pandey A, et al. Universal healthcare as pandemic preparedness: The lives and costs that could have been saved during the COVID-19 pandemic. Proc Natl Acad Sci U S A. 2022;119(25):e2200536119. doi: 220053 6110.2200531073/pnas.2200536119. Epub 22005 32022 Jun 2200536113.
35. McNamara T, Mann K, Mathai J. COVID-19: Health Inequities Exposed and How We Can Do Better. HCA Healthc J Med. 2022;3(3):209-211. doi: 210.36518/32689-30216.31437. eCollection 32022.
36. Crowley R, Mathew S, Hilden D. Modernizing the United States’ Public Health Infrastructure: A Position Paper From the American College of Physicians. Ann Intern Med. 2023;176(8):1089-1091. doi: 1010.7326/M1023-0670. Epub 2023 Jul 1018.
37. Kokudo N, Sugiyama H. Call for international cooperation and collaboration to effectively tackle the COVID-19 pandemic. Glob Health Med. 2020;2(2):60-62. doi: 10.35772/ghm.32020.01019.
38. Javed S, Chattu VK. Strengthening the COVID-19 pandemic response, global leadership, and international cooperation through global health diplomacy. Health Promot Perspect. 2020; 10(4): 300-305. doi: 310.34172/hpp.32020.34148. eCollection 32020.
39. Ramgobin D, McClafferty B, Kramer C, Golamari R, McGillen B, Jain R. Papering over the cracks: COVID-19’s amplification of the failures of employer-based health insurance coverage. J Community Hosp Intern Med Perspect. 2021;11(1):1 07-110. doi: 110.1080/20009666.20002020.2 1851869.
40. Estrada LV, Levasseur JL, Maxim A, Benavidez GA, Pollack Porter KM. Structural Racism, Place, and COVID-19: A Narrative Review Describing How We Prepare for an Endemic COVID-19 Future. Health Equity. 2022;6(1):356-366. doi: 310.1089/heq.2021.0190. eCollection 2022.
41. Moore JT, Pilkington W, Kumar D. Diseases with health disparities as drivers of COVID-19 outcome. J Cell Mol Med. 2020;24(19):11038-11045. doi: 11010.11111/jcmm.15599. Epub 12020 Aug 11020.
42. Nana-Sinkam P, Kraschnewski J, Sacco R, et al. Health disparities and equity in the era of COVID-19. J Clin Transl Sci. 2021;5(1):e99. doi: 10.1017/c ts.2021.1023.
43. Melvin SC, Wiggins C, Burse N, Thompson E, Monger M. The Role of Public Health in COVID-19 Emergency Response Efforts From a Rural Health Perspective. Prev Chronic Dis. 2020;17:E70. (doi):10.5888/pcd5817.200256.
44. Crow DA, DeLeo RA, Albright EA, et al. Policy learning and change during crisis: COVID-19 policy responses across six states. Rev Policy Res. 2023;40(1):10-35. doi: 10.1111/ropr.12511. Epub 12022 Oct 12519.
45. Williams BA, Jones CH, Welch V, True JM. Outlook of pandemic preparedness in a post-COVID-19 world. NPJ Vaccines. 2023;8(1):178. doi: 110.1038/s41541-41023-00773-41540.
46. Yassin N, Saleh S. The World after COVID-19: Reflections on Global Health and Policy. Ann Glob Health. 2021;87(1):72. doi: 10.5334/aogh.29 02. eCollection 2021.
47. Manchia M, Gathier AW, Yapici-Eser H, et al. The impact of the prolonged COVID-19 pandemic on stress resilience and mental health: A critical review across waves. Eur Neuropsychopharmacol. 2022;55:22-83. (doi):10.1016/j.euroneuro.2021.10 10.1864. Epub 2021 Oct 1029.
48. Okazaki S, Lee CS, Prasai A, Chang DF, Yoo N. Disaggregating the data: Diversity of COVID-19 stressors, discrimination, and mental health among Asian American communities. Front Public Health. 2022;10:956076.(doi):10.3389/fpubh.2022.95607. eCollection 952022.
49. Ryu S, Fan L. The Relationship Between Financial Worries and Psychological Distress Among U.S. Adults. J Fam Econ Issues. 2023;44(1):16-33. doi: 10.1007/s10834-10022-09820-10839. Epub 12022 Feb 10831.
50. Isasi F, Naylor MD, Skorton D, Grabowski DC, Hernández S, Rice VM. Patients, Families, and Communities COVID-19 Impact Assessment: Lessons Learned and Compelling Needs. NAM Perspect. 2021;2021:10.31478/202111c.(doi):10.31478/202111c. eCollection 202021.
51. Cuadrado E, Arenas A, Moyano M, La Gamma M. Development and Validation of the COVID-19 Worries and Fears Scale. Int J Public Health. 2022; 67:1604600.(doi):10.3389/ijph.2022.1604600. eCollection 1602022.
52. Huang F, Ding H, Liu Z, et al. How fear and collectivism influence public’s preventive intention towards COVID-19 infection: a study based on big data from the social media. BMC Public Health. 2020;20(1):1707. doi: 1710.1186/s12889-12020-09674-12886.
53. Dieckmann NF, Gregory R, Satterfield T, Mayorga M, Slovic P. Characterizing public perceptions of social and cultural impacts in policy decisions. Proc Natl Acad Sci U S A. 2021;118(24): e2020491118. doi: 2020491110.2020491073/pna s.2020491118.
54. Kwon S, Joshi AD, Lo CH, et al. Association of social distancing and face mask use with risk of COVID-19. Nat Commun. 2021;12(1):3737. doi: 3710.1038/s41467-41021-24115-41467.
55. Schönweitz FB, Zimmermann BM, Hangel N, et al. Solidarity and reciprocity during the COVID-19 pandemic: a longitudinal qualitative interview study from Germany. BMC Public Health. 2024;24(1):23. doi: 10.1186/s12889-12023-17521-12887.
56. Delmastro M, Paciello M. Depression, reduced education, and bias perceptions as risk factors of beliefs in misinformation. Sci Rep. 2022; 12(1):16408. doi: 16410.11038/s41598-16022-20640-16407.
57. van der Linden S. Misinformation: susceptibility, spread, and interventions to immunize the public. Nat Med. 2022;28(3):460-467. doi: 410.1038/s41591-41022-01713-41596. Epub 42022 Mar 41510.
58. Traina G, Feiring E. Priority setting and personal health responsibility: an analysis of Norwegian key policy documents. J Med Ethics. 2022;48(1):39-45. doi: 10.1136/medethics-2019-105612. Epub 102020 Mar 105612.
59. Winblad U, Swenning AK, Spangler D. Soft law and individual responsibility: a review of the Swedish policy response to COVID-19. Health Econ Policy Law. 2022;17(1):48-61. doi: 10.1017/S17441 33121000256. Epub 1744133121002021 Aug 1744133121000210.
60. Ahmed A, Jackson J. RACE, RISK, AND PERSONAL RESPONSIBILITY IN THE RESPONSE TO COVID-19. Columbia Law Review. 2021;121 (3):47-70.
61. Low LL, Tong SF, Ang JY, et al. Social responsibility perspective in public response to the COVID-19 pandemic: a grounded theory approach. BMC Public Health. 2022;22(1):469. doi: 410.118 6/s12889-12022-12819-12884.
62. Flood CM, MacDonnell V, Thomas B, Wilson K. Reconciling civil liberties and public health in the response to COVID-19. FACETS. 2020;5:887-898.
63. Taylor RCR. The global governance of pandemics. Sociol Health Illn. 2021;43(6):1540-1553. doi: 1510.1111/1467-9566.13293. Epub 12021 Jul 13219.
64. Shanka MS, Menebo MM. When and How Trust in Government Leads to Compliance with COVID-19 Precautionary Measures. J Bus Res. 2022; 139:1275-1283. (doi):10.1016/j.jbusres.2021.1010.1 036. Epub 2021 Oct 1029.
65. Kanewischer E, Mueller C, Pylkkanen M, Tunks S. Hardships & Resilience: Families in a Pandemic. Fam J Alex Va. 2022;30(3):366-375. doi: 310.1177/10664807211054182.
66. Mansoor M. Citizens’ trust in government as a function of good governance and government agency’s provision of quality information on social media during COVID-19. Gov Inf Q. 2021;38(4): 101597. doi: 101510.101016/j.giq.102021.101597. Epub 102021 Jun 101523.
67. Teixeira da Silva JA. Mandatory COVID-19 Vaccines versus Personal Freedoms: An Imperfect Balance. Oman Med J. 2022;37(4):e378. doi: 310.5 001/omj.2022.5050. eCollection 2022 Jul.
68. Nihlén Fahlquist J. The moral responsibility of governments and individuals in the context of the coronavirus pandemic. Scand J Public Health. 2021;49(7):815-820. doi: 810.1177/140349482199 0250. Epub 1403494821992021 Feb 1403494821 990256.
69. Resilience in the times of COVID: what the response to the COVID pandemic teaches us about resilience principles.
70. Sekalala S, Forman L, Habibi R, Meier BM. Health and human rights are inextricably linked in the COVID-19 response. BMJ Glob Health. 2020; 5(9):e003359. doi: 003310.001136/bmjgh-002020-003359.
71. Tan SY, Foo C, Verma M, et al. Mitigating the impacts of the COVID-19 pandemic on vulnerable populations: Lessons for improving health and social equity. Soc Sci Med. 2023;328:116007. (doi):10.1016/j.socscimed.2023.116007. Epub 112 023 Jun 116002.
72. Lansing AE, Romero NJ, Siantz E, et al. Building trust: Leadership reflections on community empowerment and engagement in a large urban initiative. BMC Public Health. 2023;23(1):1252. doi: 1210.1186/s12889-12023-15860-z.
73. Bayer R. The continuing tensions between individual rights and public health. Talking Point on public health versus civil liberties. EMBO Rep. 2007; 8(12):1099-1103. doi: 1010.1038/sj.embor.7401134.
74. Meier BM. Advancing health rights in a globalized world: responding to globalization through a collective human right to public health. J Law Med Ethics. 2007;2007 Winter;35(4):545-555.
75. Tomori C, Evans DP, Ahmed A, Nair A, Meier BM. Where is the “Public” in American Public Health? Moving from individual responsibility to collective action. EClinicalMedicine. 2022;45:101341. (doi):10.1016/j.eclinm.2022.101341. eCollection 102022 Mar.
76. Ho A, Huang V. Unmasking the Ethics of Public Health Messaging in a Pandemic. J Bioeth Inq. 2021;18(4):549-559. doi: 510.1007/s11673-11021-10126-y. Epub 12021 Sep 11624.
77. Taylor S, Asmundson GJG. Negative attitudes about facemasks during the COVID-19 pandemic: The dual importance of perceived ineffectiveness and psychological reactance. PLoS One. 2021;16(2):e0246317. doi: 0246310.024137 1/journal.pone.0246317. eCollection 0242021.
78. Kreuter MW, Sugg-Skinner C, Holt CL, et al. Cultural tailoring for mammography and fruit and vegetable intake among low-income African-American women in urban public health centers. Prev Med. 2005;41(1):53-62. doi: 10.1016/j.ypme d.2004.1010.1013. Epub 2004 Nov 1026.
79. Updegraff JA, Sherman DK, Luyster FS, Mann TL. The effects of message quality and congruency on perceptions of tailored health communications. J Exp Soc Psychol. 2007;43(2):249-257. doi: 210.1 016/j.jesp.2006.1001.1007.
80. Malthouse E. Confirmation bias and vaccine-related beliefs in the time of COVID-19. J Public Health (Oxf). 2023;45(2):523-528. doi: 510.1093/p ubmed/fdac1128.
81. Olsen SJ, Azziz-Baumgartner E, Budd AP, et al. Decreased influenza activity during the COVID-19 pandemic-United States, Australia, Chile, and South Africa, 2020. Am J Transplant. 2020;20(12): 3681-3685. doi: 3610.1111/ajt.16381.
82. Brienen NC, Timen A, Wallinga J, van Steenbergen JE, Teunis PF. The effect of mask use on the spread of influenza during a pandemic. Risk Anal. 2010;30(8):1210-1218. doi: 1210.1111/j.1539-6924.2010.01428.x. Epub 02010 May 01420.
83. Beaton E, Gadomski M, Manson D, Tan KC. Crisis Nationalism: To What Degree Is National Partiality Justifiable during a Global Pandemic? Ethical Theory Moral Pract. 2021;24(1):285-300. doi: 210.1007/s10677-10021-10160-10670. Epub 12021 Feb 10614.
84. Jecker NS. Achieving Global Vaccine Equity: The Case for an International Pandemic Treaty. Yale J Biol Med. 2022;95(2):271-280. eCollection 2022 Jun.
85. Bertollo AG, Braga GC, Tonin PT, Luzardo AR, Bagatini MD, Ignácio ZM. The Impact of Stress from Social Isolation during the COVID-19 Pandemic on Psychiatric Disorders: An Analysis from the Scientific Literature. Brain Sci. 2023;13(10):1414. doi: 1410.3390/brainsci13101414.
86. Romer D, Winneg KM, Jamieson PE, Brensinger C, Jamieson KH. Misinformation about vaccine safety and uptake of COVID-19 vaccines among adults and 5-11-year-olds in the United States. Vaccine. 2022;40(45):6463-6470. doi: 6410.1016/j.v accine.2022.6409.6046. Epub 2022 Sep 6422.
87. Chiu NC, Chi H, Tai YL, et al. Impact of Wearing Masks, Hand Hygiene, and Social Distancing on Influenza, Enterovirus, and All-Cause Pneumonia During the Coronavirus Pandemic: Retrospective National Epidemiological Surveillance Study. J Med Internet Res. 2020;22(8):e21257. doi: 21210.22196/21257.
88. Yu Y, Lau JTF, Lau MMC. Levels and factors of social and physical distancing based on the Theory of Planned Behavior during the COVID-19 pandemic among Chinese adults. Transl Behav Med. 2021;11(5):1179-1186. doi: 1110.1093/tbm/ibaa1146.
89. Sikali K. The dangers of social distancing: How COVID-19 can reshape our social experience. J Community Psychol. 2020;48(8):2435-2438. doi: 2410.1002/jcop.22430. Epub 22020 Aug 22416.
90. Mercer KH, Mollborn S. Distinction through distancing: Norm formation and enforcement during the COVID-19 pandemic. Social Science & Medicine. 2023;338.
91. Xiao Y, Becerik-Gerber B, Lucas G, Roll SC. Impacts of Working From Home During COVID-19 Pandemic on Physical and Mental Well-Being of Office Workstation Users. J Occup Environ Med. 2021;63(3):181-190. doi: 110.1097/JOM.0000000 000002097.
92. Singh P, Bala H, Dey BL, Filieri R. Enforced remote working: The impact of digital platform-induced stress and remote working experience on technology exhaustion and subjective wellbeing. J Bus Res. 2022;151:269-286. (doi):10.1016/j.jbusre s.2022.1007.1002. Epub 2022 Jul 1011.
93. Quesada-Pallarès C, Sánchez-Martí A, Ciraso-Calí A, Pineda-Herrero P. Online vs. Classroom Learning: Examining Motivational and Self-Regulated Learning Strategies Among Vocational Education and Training Students. Front Psychol. 2019;10:2795.(doi):10.3389/fpsyg.2019.02795. eCollection 02019.
94. Kamble S, Joshi A, Kamble R, Kumari S. Influence of COVID-19 Pandemic on Psychological Status: An Elaborate Review. Cureus. 2022;14(10): e29820. doi: 29810.27759/cureus.29820. eCollection 22022 Oct.
95. Ferreira Caceres MM, Sosa JP, Lawrence JA, et al. The impact of misinformation on the COVID-19 pandemic. AIMS Public Health. 2022;9 (2):262-277. doi: 210.3934/publichealth.2022018. eCollection 2022022.
96. Joseph AM, Fernandez V, Kritzman S, et al. COVID-19 Misinformation on Social Media: A Scoping Review. Cureus. 2022;14(4):e24601. doi: 24610.27759/cureus.24601. eCollection 22022 Apr.
97. Warnke L, Maier A-L, Gilbert DU. Social media platforms’ responses to COVID-19-related mis- and disinformation: the insufficiency of self-governance. Journal of Management and Governance. 2024;28:1079-1115.
98. Johnson S, Roberts S, Hayes S, et al. Understanding Pandemic Solidarity: Mutual Support During the First COVID-19 Lockdown in the United Kingdom. Public Health Ethics. 2023;16(3):245-260. doi: 210.1093/phe/phad1024. eCollection 2023 Nov.
99. Martinelli L, Kopilaš V, Vidmar M, et al. Face Masks During the COVID-19 Pandemic: A Simple Protection Tool With Many Meanings. Front Public Health. 2020;8:606635. (doi):10.3389/fpubh.202 0.606635. eCollection 602020.
100. Olick RS, Shaw J, Yang YT. Ethical Issues in Mandating COVID-19 Vaccination for Health Care Personnel. Mayo Clin Proc. 2021;96(12):2958-2962. doi: 2910.1016/j.mayocp.2021.2910.2020.
101. McKee C, Bohannon K. Exploring the Reasons Behind Parental Refusal of Vaccines. J Pediatr Pharmacol Ther. 2016;21(2):104-109. doi: 110.5863/1551-6776-5821.5862.5104.
102. Gu S, Ślusarczyk B, Hajizada S, Kovalyova I, Sakhbieva A. Impact of the COVID-19 Pandemic on Online Consumer Purchasing Behavior. Theor Appl Electron Commer Res. 2021;16:2263-2281.
103. Bai R. Impact of financial literacy, mental budgeting and self control on financial wellbeing: Mediating impact of investment decision making. PLoS One. 2023;18(11):e0294466. doi: 0294410.0 291371/journal.pone.0294466. eCollection 0292023.
104. Gonzalez KF, Bull MT, Muñoz-Herrera S, Robledo LF. Determinant Factors in Personal Decision-Making to Adopt COVID-19 Prevention Measures in Chile. Int J Environ Res Public Health. 2021;18(15):8131. doi: 8110.3390/ijerph18158131.
105. Kliger D, Levy M, Rachevski I. Wellbeing: Decision making and behavior during COVID-19. Journal of Behavioral and Experimental Economics. 2024;109.
106. Smith MHJ, Earl J, Dawson L. The Ethics of Personal Behaviors for Preventing Infectious Diseases in a Post-COVID-19 Pandemic World. Public Health Rep. 2023;138(5):822-828. doi: 810.1177/00333549231184931. Epub 00333549 231182023 Jul 00333549231184921.
107. van der Bles AM, van der Linden S, Freeman ALJ, Spiegelhalter DJ. The effects of communicating uncertainty on public trust in facts and numbers. Proc Natl Acad Sci U S A. 2020; 117(14):7672-7683. doi: 7610.1073/pnas.1913678 117. Epub 1913672 020 Mar 1913678123.
108. Hyland-Wood B, Gardner J, Leask J, Ecker UKH. Toward effective government communication strategies in the era of COVID-19. HUMANITIES AND SOCIAL SCIENCES COMMUNICATIONS. 2021;8(30):1-11.
109. Martela F, Nelli H, M. RR, and Vansteenkiste M. Motivating voluntary compliance to behavioural restrictions: Self-determination theory–based checklist of principles for COVID-19 and other emergency communications. European Review of Social Psychology. 2021;32(2):305-347.
110. Rocha YM, de Moura GA, Desidério GA, de Oliveira CH, Lourenço FD, de Figueiredo Nicolete LD. The impact of fake news on social media and its influence on health during the COVID-19 pandemic: a systematic review. Z Gesundh Wiss. 2021;9:1-10.
111. Machado BAS, Hodel KVS, Fonseca L, et al. The Importance of Vaccination in the Context of the COVID-19 Pandemic: A Brief Update Regarding the Use of Vaccines. Vaccines (Basel). 2022;10(4): 591. doi: 510.3390/vaccines10040591.
112. Santangelo OE, Provenzano S, Di Martino G, Ferrara P. COVID-19 Vaccination and Public Health: Addressing Global, Regional, and Within-Country Inequalities. Vaccines (Basel). 2024;12(8): 885. doi: 810.3390/vaccines12080885.
113. Dubé È, Labbé F, Malo B, Pelletier C. Public health communication during the COVID-19 pandemic: perspectives of communication specialists, healthcare professionals, and community members in Quebec, Canada. Can J Public Health. 2022; 113(Suppl 1):24-33. doi: 10.17269/s41997-17022-00697-17267. Epub 12022 Sep 17221.
114. Lee A, Morling JR, Bhopal RS. COVID19 – Why open and honest public dialogue is needed. Public Health. 2020;188:A1-A2. (doi):10.1016/j.pu he.2020.1009.1008. Epub 2020 Sep 1018.
115. Filip R, Gheorghita Puscaselu R, Anchidin-Norocel L, Dimian M, Savage WK. Global Challenges to Public Health Care Systems during the COVID-19 Pandemic: A Review of Pandemic Measures and Problems. J Pers Med. 2022;12(8):1295. doi: 1210.3 390/jpm12081295.
116. Polyzou M, Kiefer D, Baraliakos X, Sewerin P. Addressing the spread of health-related misinformation on social networks: an opinion article. Front Med (Lausanne). 2023;10:1167033. (doi):10.3 389/fmed.2023.1167033. eCollection 1162023.
117. Kerr J, Panagopoulos C, van der Linden S. Political polarization on COVID-19 pandemic response in the United States. Pers Individ Dif. 2021;179:110892.(doi):10.1016/j.paid.2021.110892. Epub 112021 Apr 110891.
118. Stroebe W, vanDellen MR, Abakoumkin G, et al. Politicization of COVID-19 health-protective behaviors in the United States: Longitudinal and cross-national evidence. PLoS One. 2021;16(10): e0256740. doi: 0256710.0251371/journal.pone.0 256740. eCollection 0252021.
119. Porat T, Nyrup R, Calvo RA, Paudyal P, Ford E. Public Health and Risk Communication During COVID-19-Enhancing Psychological Needs to Promote Sustainable Behavior Change. Front Public Health. 2020;8:573397. (doi):10.3389/fpubh.202 0.573397. eCollection 572020.
120. Escandón K, Rasmussen AL, Bogoch, II, et al. COVID-19 false dichotomies and a comprehensive review of the evidence regarding public health, COVID-19 symptomatology, SARS-CoV-2 transmission, mask wearing, and reinfection. BMC Infect Dis. 2021;21(1):710. doi: 710.1186/s12879-12021-06357-12874.
121. Kisa S, Kisa A. A Comprehensive Analysis of COVID-19 Misinformation, Public Health Impacts, and Communication Strategies: Scoping Review. J Med Internet Res. 2024;26:e56931.( doi):10.2196/5 6931.
122. Gamerdinger A, Just SN, Lantz PMV.
123. Hunter P. The communications gap between scientists and public: More scientists and their institutions feel a need to communicate the results and nature of research with the public. EMBO Rep. 2016;17(11):1513-1515. doi: 1510.15 252/emb r.201643379. Epub 201642016 Oct 201 643377.
124. Skirbekk H, Magelssen M, Conradsen S. Trust in healthcare before and during the COVID-19 pandemic. BMC Public Health. 2023;23(1):863. doi: 810.1186/s12889-12023-15716-12886.
125. Caplan AL. Regaining Trust in Public Health and Biomedical Science following Covid: The Role of Scientists. Hastings Cent Rep. 2023;53(Suppl 2):S105-S109. doi: 110.1002/hast.1531.
126. Kreps SE, Kriner DL. Model uncertainty, political contestation, and public trust in science: Evidence from the COVID-19 pandemic. Sci Adv. 2020;6(43):eabd4563. doi: 4510.1126/sciadv.abd4 563. Print 2020 Oct.
127. Alvarez E, Bielska IA, Hopkins S, et al. Limitations of COVID-19 testing and case data for evidence-informed health policy and practice. Health Res Policy Syst. 2023;21(1):11. doi: 10.1186/s12961-12023-00963-12961.
128. Zdravkovic M, Berger-Estilita J, Zdravkovic B, Berger D. Scientific quality of COVID-19 and SARS CoV-2 publications in the highest impact medical journals during the early phase of the pandemic: A case control study. PLoS One. 2020;1 5(11):e0241826. doi: 0241810.0241371/journal.po ne.0241826. eCollection 0242020.
129. van Schalkwyk F, Dudek J. Reporting preprints in the media during the COVID-19 pandemic. Public Underst Sci. 2022;31(5):608-616. doi: 610.1177/09636625221077392. Epub 09636 625221072022 Feb 09636625221077323.
130. Capodici A, Salussolia A, Sanmarchi F, Gori D, Golinelli D. Biased, wrong and counterfeited evidences published during the COVID-19 pandemic, a systematic review of retracted COVID-19 papers. Qual Quant. 2022;29:1-33.
131. Gabarron E, Oyeyemi SO, Wynn R. COVID-19-related misinformation on social media: a systematic review. Bull World Health Organ. 2021; 99(6):455-463A. doi: 410.2471/BLT.2420.276782. Epub 272021 Mar 276719.
132. Schilling WHK, Mukaka M, Callery JJ, et al. Evaluation of hydroxychloroquine or chloroquine for the prevention of COVID-19 (COPCOV): A double-blind, randomised, placebo-controlled trial. PLoS Med. 2024;21(9):e1004428. doi: 1004410.100 1371/journal.pmed.1004428. eCollection 1002024 Sep.
133. Bundgaard H, Bundgaard JS, Raaschou-Pedersen DET, et al. Effectiveness of Adding a Mask Recommendation to Other Public Health Measures to Prevent SARS-CoV-2 Infection in Danish Mask Wearers : A Randomized Controlled Trial. Ann Intern Med. 2021;174(3):335-343. doi: 310.732 6/M7320-6817. Epub 2020 Nov 7318.
134. Au L, Eyal G. Whose Advice is Credible? Claiming Lay Expertise in a Covid-19 Online Community. Qual Sociol. 2022;45(1):31-61. doi: 10.1007/s11133-11021-09492-11131. Epub 12021 Nov 11133.
135. Cologna V, Mede NG, Berger S, et al. Trust in scientists and their role in society across 68 countries. Nat Hum Behav. 2025;20(10):024-02090.
136. Love R, Darics E, Palmieri R. Engaging the public: English local government organisations’ social media communications during the COVID‐19 pandemic. Applied Corpus Linguistics. 2023;3(8).
137. Erismann S, Pesantes MA, Beran D, et al. How to bring research evidence into policy? Synthesizing strategies of five research projects in low-and middle-income countries. Health Res Policy Syst. 2021;19(1):29. doi: 10.1186/s12961-12020-00646-12961.
138. Rotulo A, Kondilis E, Thwe T, et al. Mind the gap: Data availability, accessibility, transparency, and credibility during the COVID-19 pandemic, an international comparative appraisal. PLOS Glob Public Health. 2023;3(4):e0001148. doi: 0001110.0 001371/journal.pgph.0001148. eCollection 0002023.
139. Osti T, Valz Gris A, Corona VF, et al. Public health leadership in the COVID-19 era: how does it fit? A scoping review. BMJ Lead. 2024;8(2):174-182. doi: 110.1136/leader-2022-000653.
140. Koffman J, Gross J, Etkind SN, Selman L. Uncertainty and COVID-19: how are we to respond? J R Soc Med. 2020;113(6):211-216. doi: 210.117 7/0141076820930665.
141. Linvill JS, Onosu GO. Stories of Leadership: Leading with Empathy through the COVID-19 Pandemic. Sustainability. 2023;15(7708):1-22.
142. Liao CH. Exploring the Influence of Public Perception of Mass Media Usage and Attitudes towards Mass Media News on Altruistic Behavior. Behav Sci (Basel). 2023;13(8):621. doi: 610.3390/b s13080621.
143. Rodrigues F, Newell R, Rathnaiah Babu G, Chatterjee T, Sandhu NK, Gupta L. The social media Infodemic of health-related misinformation and technical solutions. Health Policy and Technology. 2024;13(2):1-5.
144. Latif AS. The Importance of Understanding Social and Cultural Norms in Delivering Quality Health Care-A Personal Experience Commentary. Trop Med Infect Dis. 2020;5(1):22. doi: 10.3390/tr opicalmed5010022.
145. Saulnier DD, Duchenko A, Ottilie-Kovelman S, Tediosi F, Blanchet K. Re-evaluating Our Knowledge of Health System Resilience During COVID-19: Lessons From the First Two Years of the Pandemic. Int J Health Policy Manag. 2023;12: 6659.(doi):10.34172/ijhpm.32022.36659. Epub 32022 Dec 34176.
146. Serafini G, Parmigiani B, Amerio A, Aguglia A, Sher L, Amore M. The psychological impact of COVID-19 on the mental health in the general population. QJM. 2020;113(8):531-537. doi: 510.10 93/qjmed/hcaa1201.
147. Roels NI, Estrella A, Maldonado-Salcedo M, Rapp R, Hansen H, Hardon A. Confident futures: Community-based organizations as first responders and agents of change in the face of the Covid-19 pandemic. Social Science and Medicine. 2022;2 94:1-15.
148. Rao A, Sabri N, Guo S, Raschid L, Lerman K. Public Health Messaging on Twitter During the COVID-19 Pandemic: Observational Study. J Med Internet Res. 2025;27:e63910. (doi):10.2196/63910.
149. Leach M, MacGregor H, Scoones I, Wilkinson A. Post-pandemic transformations: How and why COVID-19 requires us to rethink development. World Dev. 2021;138:105233. (doi):10.1016/j.worl ddev.2020.105233. Epub 102020 Oct 105216.
150. Correia T. Trust Building in Public Health Approaches: The Importance of a “People-Centered” Concept in Crisis Response. Risk Manag Healthc Policy. 2024;17:1903-1908. (doi):10.2147/RMHP.S 471250. eCollection 472024.
151. Bollyky TJ, Petersen MB. A practical agenda for incorporating trust into pandemic preparedness and response. Bull World Health Organ. 2024;102(6):440-447. doi: 410.2471/BLT.2 423.289979. Epub 282024 Apr 289930.
152. Sauer MA, Truelove S, Gerste AK, Limaye RJ. A Failure to Communicate? How Public Messaging Has Strained the COVID-19 Response in the United States. Health Secur. 2021;19(1):65-74. doi: 10.1089/hs.2020.0190.
153. Jirmanus LZ, Valenti RM, Griest Schwartzman EA, et al. Too Many Deaths, Too Many Left Behind: A People’s External Review of the U.S. Centers for Disease Control and Prevention’s COVID-19 Pandemic Response. AJPM Focus. 2024;3(4):100 207. doi: 100210.101016/j.focus.102024.100207. eCollection 102024 Aug.
154. Zhou Y, Zhang A, Liu X, et al. Protecting public’s wellbeing against COVID-19 infodemic: The role of trust in information sources and rapid dissemination and transparency of information over time. Front Public Health. 2023;11:1142230. (doi):10.3389/fpubh.2023.1142230. eCollection 1142023.
155. Harris OO, Perry TE, Johnson JK, et al. Understanding the concept of trust and other factors related to COVID-19 vaccine intentions among Black/African American older adults prior to vaccine development. SSM Qual Res Health. 2023;3:100230. (doi):10.1016/j.ssmqr.2023.10023. Epub 102023 Feb 100234.
156. Li J, Pandian V, Fong DYT, et al. Fear in general populations: A cross-sectional study on perceived fear of common diseases, COVID-19, life events, and environmental threats in 30 countries. J Glob Health. 2024;14:05019. (doi):10.7189/jog h.7114.05019.
157. Andersson C, Mellner C, Lilliengren P, et al. Cultivating Compassion and Reducing Stress and Mental Ill-Health in Employees-A Randomized Controlled Study. Front Psychol. 2021;12:748140. (doi):10.3389/fpsyg.2021.748140. eCollection 742021.
158. Julia GJ, Romate J, Allen JG, Rajkumar E. Compassionate communication: a scoping review. Frontiers in Communication. 2024;8:1-19.
159. Zheng H, Goh DH, Lee EWJ, Lee CS, Theng YL. Understanding the effects of message cues on COVID-19 information sharing on Twitter. J Assoc Inf Sci Technol. 2022;73(6):847-862. doi: 810.100 2/asi.24587. Epub 22021 Oct 24515.
160. Monzani D, Vergani L, Pizzoli SFM, Marton G, Pravettoni G. Emotional Tone, Analytical Thinking, and Somatosensory Processes of a Sample of Italian Tweets During the First Phases of the COVID-19 Pandemic: Observational Study. J Med Internet Res. 2021;23(10):e29820. doi: 2981 0.22196/29820.
161. Holroyd TA, Oloko OK, Salmon DA, Omer SB, Limaye RJ. Communicating Recommendations in Public Health Emergencies: The Role of Public Health Authorities. Health Secur. 2020;18(1):21-28. doi: 10.1089/hs.2019.0073.
162. Nadkarni A, Levy-Carrick NC, Kroll DS, Gitlin D, Silbersweig D. Communication and Transparency as a Means to Strengthening Workplace Culture During COVID-19. NAM Perspect. 2021;2021:10.31478/202103a. (doi):10.31478/202 103a. eCollection 202021.
163. Lee Y, Li JYQ. The role of communication transparency and organizational trust in publics’ perceptions, attitudes and social distancing behaviour: A case study of the COVID‐19 outbreak. Journal of Contingencies and Crisis Management. 2021;29(4):368-384. doi: 310.1111/1468-5973.12354. Epub 12021 Feb 12357.
164. Reveilhac M. The deployment of social media by political authorities and health experts to enhance public information during the COVID-19 pandemic. SSM Popul Health. 2022;19:101165. (doi):10.1016/j.ssmph.2022.101165. Epub 102022 Jul 101168.
165. Gisondi MA, Barber R, Faust JS, et al. A Deadly Infodemic: Social Media and the Power of COVID-19 Misinformation. J Med Internet Res. 2022;24(2):e35552. doi: 35510.32196/35552.
166. Li J, Chang X. Combating Misinformation by Sharing the Truth: a Study on the Spread of Fact-Checks on Social Media. Inf Syst Front. 2022; 11:1-15.
167. Hoes E, Aitken B, Zhang J, Gackowski T, Wojcieszak M. Prominent misinformation interventions reduce misperceptions but increase scepticism. Nat Hum Behav. 2024;8(8):1545-1553. doi: 1510.1 038/s41562-41024-01884-x. Epub 42024 Jun 41510.
168. Zhang YSD, Young Leslie H, Sharafaddin-Zadeh Y, Noels K, Lou NM. Public Health Messages About Face Masks Early in the COVID-19 Pandemic: Perceptions of and Impacts on Canadians. J Community Health. 2021;46(5):903-912. doi: 910.1 007/s10900-10021-00971-10908. Epub 12021 Feb 10920.
169. Spalluto LB, Planz VB, Stokes LS, et al. Transparency and Trust During the Coronavirus Disease 2019 (COVID-19) Pandemic. J Am Coll Radiol. 2020;17(7):909-912. doi: 910.1016/j.jacr.20 20.1004.1026. Epub 2020 May 1011.
170. Forman R, Atun R, McKee M, Mossialos E. 12 Lessons learned from the management of the coronavirus pandemic. Health Policy. 2020;124 (6):577-580. doi: 510.1016/j.healthpol.2020.100 5.1008. Epub 2020 May 1015.
171. Zheng S, Masuda T, Matsunaga M, et al. Cultural differences in social support seeking: The mediating role of empathic concern. PLoS One. 2021;16(12):e0262001. doi: 0262010.0261371/jo urnal.pone.0262001. eCollection 0262021.
172. Zey E, Windmann S. Effects of Message Framing, Sender Authority, and Recipients’ Self-Reported Trait Autonomy on Endorsement of Health and Safety Measures during the Early COVID-19 Pandemic. Int J Environ Res Public Health. 2021; 18(15):7740. doi: 7710.3390/ijerph18157740.
173. Yang Z, Luo X, Jia H. Is It All a Conspiracy? Conspiracy Theories and People’s Attitude to COVID-19 Vaccination. Vaccines (Basel). 2021;9 (10):1051. doi: 1010.3390/vaccines9101051.
174. Stolle LB, Nalamasu R, Pergolizzi JV, Jr., et al. Fact vs Fallacy: The Anti-Vaccine Discussion Reloaded. Adv Ther. 2020;37(11):4481-4490. doi: 4410.1007/s12325-12020-01502-y. Epub 12020 Sep 12323.
175. Modgil S, Singh RK, Gupta S, Dennehy D. A Confirmation Bias View on Social Media Induced Polarisation During Covid-19. Inf Syst Front. 2021;2 0:1-25.
176. Kanchan S, Gaidhane A. Social Media Role and Its Impact on Public Health: A Narrative Review. Cureus. 2023;15(1):e33737. doi: 33710.37 759/cureus.33737. eCollection 32023 Jan.
177. Han R, Xu J, Pan D. How Media Exposure, Media Trust, and Media Bias Perception Influence Public Evaluation of COVID-19 Pandemic in International Metropolises. Int J Environ Res Public Health. 2022;19(7):3942. doi: 3910.3390/ijerph19 073942.
178. Lee AH. Social Trust in Polarized Times: How Perceptions of Political Polarization Affect Americans’ Trust in Each Other. Polit Behav. 2022; 44(3):1533-1554. doi: 1510.1007/s11109-11022-09787-11101. Epub 12022 Mar 11118.
179. Mønsted B, Lehmann S. Characterizing polarization in online vaccine discourse-A large-scale study. PLoS One. 2022;17(2):e0263746. doi: 0263710.0261371/journal.pone.0263746. eCollection 0262022.
180. Cacciatore MA. Misinformation and public opinion of science and health: Approaches, findings, and future directions. Proc Natl Acad Sci U S A. 2021;118(15):e1912437117. doi: 1912437110.191 2431073/pnas.1912437117.
181. Majerczak P, Strzelecki A. Trust, Media Credibility, Social Ties, and the Intention to Share towards Information Verification in an Age of Fake News. Behav Sci (Basel). 2022;12(2):51. doi: 10.339 0/bs12020051.
182. Seyd B, Hamm JA, Jennings W, McKay L, Valgarðsson V, Anness M. ‘Follow the science’: Popular trust in scientific experts during the coronavirus pandemic. Public Underst Sci. 2025; 34(1):2-18. doi: 10.1177/09636625241253968. Epub 09636625241252024 Jun 09636625241253912.
183. Shen AK, Browne S, Srivastava T, Kornides ML, Tan ASL. Trusted messengers and trusted messages: The role for community-based organizations in promoting COVID-19 and routine immunizations. Vaccine. 2023;41(12):1994-2002. doi: 1910.101 6/j.vaccine.2023.1902.1045. Epub 2023 Feb 1916.
184. Moussaïd M, Kämmer JE, Analytis PP, Neth H. Social influence and the collective dynamics of opinion formation. PLoS One. 2013;8(11):e78433. doi: 78410.71371/journal.pone.0078433. eCollection 0072013.
185. Hill PL, Allemand M, Burrow AL. Trust in purpose, or trust and purpose?: Institutional trust influences the association between sense of purpose and COVID-19 vaccination. J Psychosom Res. 2023; 165:111119. (doi):10.1016/j.jpsychores.2022.111119. Epub 112022 Dec 111116.
186. Gursoy D, Ekinci Y, Can AS, Murray JC. Effectiveness of message framing in changing COVID-19 vaccination intentions: Moderating role of travel desire. Tour Manag. 2022;90:104468. (doi):10.1016/j.tourman.2021.104468. Epub 102021 Dec 104468.
187. Lin SS, McDougall GJ, Peramsetty RN, McDonough IM. Hope messages influence health behavior intentions more than fear messages: An experimental study during COVID-19. Nurs Outlook. 2024;72(4):102185. doi: 102110.101016/j.outloo k.102024.102185. Epub 102024 May 102122.
188. Gillibrand S, Kapadia D, Watkinson R, Issa B, Kwaku-Odoi C, Sanders C. Marginalisation and distrust in the context of the COVID-19 vaccination programme: experiences of communities in a northern UK city region. BMC Public Health. 2024; 24(1):853. doi: 810.1186/s12889-12024-18308-12880.