

Unconscious Integration Therapy for Depression: Study Results
The Direct Approach to the Unconscious/Personal Integration Therapy Method in depression: therapeutic results and phenomenological foundation
Maria Clara Jost¹, Eunides Almeida¹, Tommy Akira Goto², Márcio Albeny Gallo¹
- Renate Jost de Moraes Educational and Research Institute / Humanistic Integral Health Foundation.
- Federal University of Uberlândia – MG-Brazil (UFU).
OPEN ACCESS
PUBLISHED: 31 May 2026
CITATION: Jost, MC., Almeida, E., et al., 2026. The Direct Approach to the Unconscious/Personal Integration Therapy Method in depression: therapeutic results and phenomenological foundation. Medical Research Archives, [online] 14(5). https://doi.org/10.18103/mra.v14i5.7391
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v14i5.7391
ISSN 2375-1924
ABSTRACT
Background: A growing body of empirical studies supports the relevance of intersubjective, narrative, and self-reflective processes in the genesis and treatment of depression. The results obtained in the psychotherapeutic process of the Direct Approach to the Unconscious Method in a Personal Integration Therapy allow for the clarification and understanding of the psychic process of configuration of depression and its possibilities of reconfiguration.
Aims: To investigate the maintenance of results obtained in participants submitted to the Direct Approach to the Unconscious Method within Personal Integration Therapy; to understand how primary intersubjective bonds are configured; and to describe the experiential processes involved in the participants’ reconfigurations.
Methods: This mixed-methods study administered the Beck Depression Inventory (Second Edition) at the beginning and at the end of the psychotherapeutic process to all participants. Subsequently, the Beck Depression Inventory–II was administered to a selected group (n = 27) for longitudinal analysis, conducted three and six months after completion of the psychotherapeutic process. The nonparametric Friedman test was used, complemented by the Wilcoxon signed-rank test with Bonferroni correction for post hoc analyses. Qualitative data were collected throughout the psychotherapeutic process itself, and the evidenced content was analyzed through Psychological-Phenomenological analysis.
Results: In the previous study, individual trajectory analyses indicated strong treatment effects at post-treatment. Across follow-up assessments, treatment gains showed partial attenuation but remained below baseline levels overall. Mean symptom reduction relative to baseline was 48.2% at 3 months and 52.7% at 6 months. The pattern of “Continuous Improvement” predominated over time, observed in 74.1% of participants, suggesting stabilization of results and consolidation of changes in the dynamics of meaning within lived-experience.
Conclusion: Depression suffering cannot be fully reduced to a naturalistic psychophysical understanding, as they involve the structural unity and self-formation processes of the Human Person within intersubjective contexts. Phenomenological Psychology provides intelligibility to this phenomenon, and the said Method may contribute as an intervention tool for the understanding and treatment of depressive suffering.
Keywords
- Depression
- Psychotherapy
- Phenomenological Psychology
- Personal Integration Therapy
- Intersubjectivity
1. Introduction
In a recent study (Jost MC, Marra C, Goto TA, Almeida E, Gallo M, 2025, in press) we presented the results of a mixed-methods study — quantitative and qualitative — which aimed to verify the efficiency and effectiveness of the Direct Approach to the Unconscious Method (ADI) used in the psychological clinic by Personal Integration Therapy (TIP), the ADI/TIP Method, a clinical intervention proposal grounded in phenomenological and anthropological assumptions.
This methodology is positioned as an evidence-based practice in psychology (EBPP), defined as a scientifically sustainable psychotherapy in the context of depressive syndrome, according to postdoctoral research and within the empirical and methodological limits of the adopted design. It was created and developed by Jost de Moraes (1936-2013), based on her experiential clinical-psychological investigation initiated in the 1970s, which subsequently grounded its anthropological-phenomenological foundations in the analyses of E. Husserl and E. Stein. These analyses offer a conceptual horizon for understanding subjectivity as a unity of meaning, despite requiring mediation between phenomenological description and clinical application.
In her investigations, Jost de Moraes criticized the biologizing attitude of Psychology and Medicine, which reduces the person to the psychophysical dimension, thereby obscuring the dimension of meaning and the historicity of experience. At this point, her position converges with Husserl’s critique of objectivizing sciences, which denounce the “decapitation of the human.” In response, Jost de Moraes proposes the notion of the “psychonoosomatic,” affirming the unity of the person and the centrality of the noological dimension, following Franklian terminology.
The ADI/TIP Method proposes a direct, experiential, and intuitive approach, understood not as the absence of mediation, but as a refusal of interpretative interventions, privileging the explication of lived-experiences as they present themselves to the subject’s consciousness. Its procedures aim at the explication of affective-emotional registers (meanings) that are not thematized but implicated in the flow of experience, thereby enabling the reconfiguration of the meanings attributed to what is lived.
Jost de Moraes developed specific diagnostic-therapeutic resources that enable access to primordial subjective and intersubjective meanings, described as unconscious insofar as they are not immediately thematized within experience, allowing understanding of events and intersubjective relationships, and enabling changes in non-constructive configurations of meaning. In elaborating this psychotherapeutic dynamic, the author aimed to contribute to the “process of humanization” of the Human Person, a question that encompasses the demand of “becoming oneself,” thereby confirming Stein’s assertions.
In the previous study (n = 341), data collection was conducted in two stages, using the Beck Depression Inventory–II (BDI-II) for quantitative analysis and the Generic Change Indicators Scale (GCIs) for qualitative analysis (Jost MC, Marra C, Goto TA, Almeida E, Gallo M, 2025, in press).
Statistical analyses provided robust evidence of the clinical efficacy of the ADI/TIP Method in reducing depressive symptoms, considering the diversity of the sample, the significant reduction in scores (Z = -15.74; p < 0.001; d = -0.85), the high treatment response rate (96.5%), and the high statistical power. In this study, the results demonstrated an average reduction of 80.5% in depression scores. These findings opened new perspectives for understanding depressive illness.
Qualitative analysis indicated that psychic suffering can be described as being configured through the impact of lived experience on subjectivity, mobilizing the constitution of meanings that may acquire pathological significance. This understanding converges with phenomenology, according to which experience is always constituted in terms of meaning, involving an I situated within the intersubjective and cultural world.
That study (Jost MC, Marra C, Goto TA, Almeida E, Gallo M, 2025, in press), drawing on Husserl, emphasized that the first appropriations of meaning occur in the body (Leib), including experiences later described by participants through references to intrauterine or early relational contexts. It was further reinforced that the I is a unity constituted by a dual layer: the I of affections, oriented by the laws of passive or psychic causality; and the I of actions, governed by motivational laws that reveal a subjectivity of a strictly spiritual character. This means that all psychic acts are inherently intertwined with the body and are built “upon an immediately embodied psyche” as the somatic foundation of the “sensible.”
Therapeutic change is understood as a reconfiguration of meanings, through the explication of structures previously implicated in experience, enabling the emergence of more integrated and healthier intersubjective lived-experiences.
This research follows a growing body of empirical studies supporting the relevance of intersubjective, narrative, and self-reflective processes in the genesis and treatment of depression. These studies demonstrate that the subjective experience of depression is highly contextualized, shaped by personal and cultural narratives, as well as power relations in medical interpretations. They also highlight that the term “depression” does not correspond to a fixed entity, but rather to a social and subjective construct, whose meaning is co-constructed in therapeutic and social interactions.
Other researchers, such as Bianciardi, Ongaretto, De Stefano, Siracusano, and Niolu, have observed correlations between depression and anxiety and insecure maternal attachment style. This, in turn, has been associated with dyadic adjustment (relationship quality) in the parental couple. Similarly, Wan and Green, Bellina, Grazioli, Garzitto, Mauri, Molteni, Brambilla, Nobile and Maguire, Ross and O’Reilly have demonstrated the mediating role of intergenerational transmission of psychic problems, highlighting the complex role of family influences and parental behavior in the transmission of psychopathology from parents to children. These findings, among others, confirm the existence of interdependent links between parental psychiatric symptomatology, relational parental behavior, and the symptomatology observed in children.
It is thus observed that the empirical and empirical-clinical recognition of this phenomenon is already established; however, there is still a lack of clarity regarding how this phenomenon is constituted. The psychological-clinical practice of the ADI/TIP Method, together with its theoretical-phenomenological grounding, may contribute to clarifying the process of psychopathological onset in depression and the possibility of its restructuring. This contribution is not limited to this mental illness, as the results of these investigations allow for extension to other forms of psychic suffering.
Based on these premises, investigating the ADI/TIP Method psychotherapeutic process is an important contribution to the understanding of both the diagnosis and recovery of this form of psychic suffering. Thus, whereas in the previous study the focus was to verify the efficiency and effectiveness of this psychotherapeutic method, the present study aims to: a) investigate the maintenance of outcomes in participants submitted to the ADI/TIP Method at 3- and 6-month follow-up intervals; b) understand how primary parental, conjugal, and familial intersubjective bonds are configured from their genesis; c) apprehend the processes that enable the reconfiguration of subjectivity and intersubjective bonds.
With these purposes, we present the results of a prospective mixed-methods longitudinal study conducted by the Federal University of Uberlândia (UFU-MG), Brazil (as approved by the “Certificate of Appreciation for Ethical Presentation” CAAE: 80587317.2.0000.5152) which, based on a sample of 341 participants: a) evaluated the sustainability of the quantitative results obtained in BDI-II scores through 3- and 6-month follow-up assessments; and b) examined the qualitative results of the Psychological-Phenomenological investigation regarding the impact of primary intersubjective parental (conjugal) and familial dynamics on the configuration and reconfiguration of depressive suffering among participants.
1.1 The Psychotherapeutic Process
Jost de Moraes, in developing her psychotherapeutic methodology, engaged theoretically with several authors, initially Frankl (1905-1997), Jung (1875-1961), Bergson (1859-1941) and Husserl (1859-1938). The author sought to ground, from a psychic and anthropo-philosophical standpoint, the clinical-psychological need to consider the person in the totality of their ontological dimensions: lived body, psyche, and spirit.
The proposal of a direct psychotherapeutic approach implies enabling the person to use their intuitive apprehension experientially to grasp events, meanings, and significations of unconscious psychic contents, privileging the explication of lived-experiences as they are given to the subject’s consciousness. Subsequently, its proponents expanded academic research, demonstrating the articulation between the observed clinical phenomenon and the phenomenology of Husserl and Edith Stein.
The notion of the “unconscious,” as described by Jost de Moraes, does not correspond to the Freudian concept of the unconscious. The descriptions of lived-experiences, intuitively perceived by patients, are closer to the notion of the phenomenological unconscious in the psychic sphere, insofar as Husserl does not posit it as an autonomous instance, but as pre-reflective layers of intentional life in which meanings are constituted without the active I. In his analyses of passive syntheses, Husserl addresses the unconscious as a dimension of consciousness that is not reducible to reflective awareness, whose content becomes evident when it emerges from the associative synthesis occurring in the flow of intentional consciousness. In Husserl, there is no separation between conscious and unconscious as distinct domains or “opposing forces,” but a unitary flow of lived-experiences, differentiated by degrees of affection and thematization, corresponding to a gradual deepening of psychic contents linked to their affective force.
Similarly, from a broader perspective, the “noölogical unconscious,” as termed by Jost de Moraes, is defined as everything that circulates within human interiority, understood as a dynamic totality of meanings. These contents are linked to events lived in the “external world” (psychophysical level) and to their meanings and significations unfolding in the “internal world,” which includes the dimension of free self-positioning (psychospiritual level) as well as universal and personal potentialities, thus exceeding the notion of a conditioned psychic unconscious. This contribution elevates the unconscious from a mere repository of drives or repressed contents to a dynamic dimension of intentional life, permeated by meaning and freedom.
1.2 Basic Methodological Procedures
Jost de Moraes, in her empirical-experiential research, developed specific methodological procedures to enable both the “direct” and “conscious” approach to the unconscious layer of consciousness and the clinical investigation of its psychic contents. These procedures—“therapeutic questioning,” “directional inversion,” and “objectivization of context and content”—are applied in an articulated and simultaneous manner. This methodology requires the use of “therapeutic questioning,” following the millennia-old proposal of Socratic “maieutics” (470–399 BC). In this case, however, the “questioning” is directed not toward the layer of intellectual logical-causal reasoning, but toward the layer of intuitive apprehension of consciousness, allowing a direct, spontaneous, immediate, and comprehensive apprehension of affective-emotional events and their contents of meaning, in line with Bergson’s and Husserl’s descriptions of intuitive modes of knowing.
In parallel, the resources of objectivization of context and content are employed, linked to ways in which the I relate to itself and to others, as well as to modes of positioning in the face of adverse situations, enabling the identification of the meaning configured in the lived event. These procedures, articulated and systematically applied, allow the person to undergo a “Circular Process” composed of: (1) a “diagnostic phase”; (2) a “diagnostic-therapeutic phase”; (3) a “therapeutic phase,” referred to by Jost de Moraes as “decoding”; and (4) the “‘positivation’ and ‘verification’ phases.”
This may lead to the emergence of contents described as unconscious memory within the participants’ experiential field, distinct from other intentional acts such as recollection, imagination, and fantasy, themes described by Husserl while analyzing the markers of passive registers of the unconscious. Thus, interpretations and explanatory-causal uses of conscious recollection are avoided, as the patient describes what is perceived experientially and in a “presentified” manner. The “presentification” of psychic contents inscribed and retained in the unconscious layer of consciousness, as well as their “awakening” into consciousness, was also examined by Husserl in his analyses of the originary constitution of time.
It is important to emphasize that, in this psychotherapeutic process, the most significant nuclei of contents of psychic suffering expressed by patients reveal affective-emotional situations linked to primary affective references, whose configured meanings—self-concepts, hetero-concepts, and contextual concepts—branch into other subjective and intersubjective situations throughout life. In this study, this method also allows access to the genesis of self-configurations and hetero-configurations, their pathological dynamics, and the motivations implicit in these problem-situations. Thus, a set of “psychonoosomatic” formations emerges, mobilizing distortions of the “I” from the intrauterine stage onward.
This clinical-theoretical possibility converges with the results of analyses by Stein, which distinguish, among the many lived-experiences, those that are originary and those that emerge as motivated by these primary lived-experiences. It also finds correspondence in the analyses of Husserl, which describe a primordiality forming in an originary state, a “pre-I,” affected, still “within the maternal flesh,” by the relational patterns of its earliest affective references, in the interrelation established between the parents themselves and between the parents and the child.
Accordingly, this framework allows the structuring of a short-term clinical-psychological intervention consisting of 10 to 15 sessions, preceded by a preparatory phase and with the possibility of therapeutic reinforcement.
2. Methods
2.1 Participants
For the exploratory follow-up analysis, a subsample of 27 participants was included based on availability and willingness to continue in the study, representing 7.9% of the original sample. The aim was to examine the maintenance of improvements in depressive symptoms, assessed using the Beck Depression Inventory (BDI-II), at 3- and 6-month follow-ups. The follow-up group had a mean age of 29.67 years (SD = 8.22), was predominantly male (77.8%), and had a high level of education (40.7% undergraduate; 51.9% postgraduate).
2.2 Data Collection
Beck Depression Inventory (BDI-II): a self-report inventory with 21 items, structured and validated to assess the level of depressive intensity according to the scores: minimal (0 to 11), mild (12 to 19), moderate (20 to 35), and severe (36 to 63).
Transcription of sessions and descriptions of observed changes: a) intra-sessions and extra-sessions. The sessions were conducted by psychologists with at least five years of training in the ADI/TIP Method, under continuous supervision to ensure adherence to the protocol.
2.3 Procedures
Participants voluntarily sought out the social clinic of the Integral Humanistic Health Foundation (FUNDASINUM) and the TIPClínica and signed the Informed Consent Form (ICF). The Beck Depression Inventory (BDI-II) was applied at the beginning and end of the psychotherapeutic process to all participants. Subsequently, the BDI-II was applied to the selected group (n = 27) for longitudinal analysis, which occurred three and six months after the completion of the psychotherapeutic process.
Qualitative data collection occurred throughout the psychotherapeutic process itself — ten sessions of the ADI/TIP Method, each lasting 50 minutes — and the evidenced content was analyzed through psychological-phenomenological analysis.
2.4 Research Stages and Evaluations
The procedures began with a medical evaluation and were therefore divided into four phases:
- Initial application of the BDI-II to all participants
- Application of the psychotherapeutic procedure of the ADI/TIP Method
- Final application of the BDI-II to all participants
- Application of the BDI-II to selected participants three months (longitudinal phase 01) and six months (longitudinal phase 02) after the conclusion of the psychotherapeutic process of the ADI/TIP Method.
The results obtained in the BDI-II were tabulated and analyzed using the Statistical Package for the Social Sciences (SPSS) software. For the longitudinal analysis, the non-parametric Friedman statistical test was used, complemented by the Wilcoxon test with Bonferroni correction for post hoc analyses.
3. Results
3.1 Longitudinal Changes in Depressive Symptoms
Descriptive statistics are presented in Table 1. Overall, depressive symptoms showed a sharp reduction at post-treatment, followed by a partial increase at the 3-month follow-up and stabilization at 6 months, remaining below baseline levels.
| Mean | SD | Min | Max | |
|---|---|---|---|---|
| Initial BDI-II | 15.22 | 7.57 | 4 | 34 |
| Post-treatment BDI-II | 3.07 | 3.33 | 0 | 13 |
| 3-month follow-up | 7.89 | 6.62 | 0 | 20 |
| 6-month follow-up | 7.19 | 6.15 | 0 | 25 |
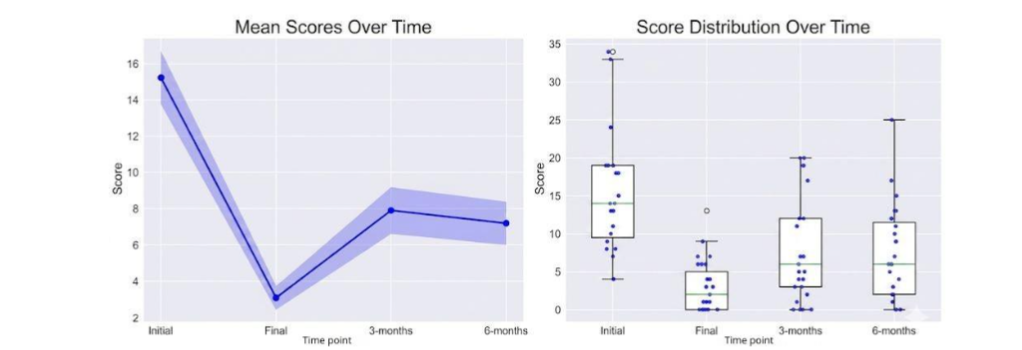
To examine differences in depressive symptoms across time (baseline, post-treatment, and follow-ups), a Friedman nonparametric test was conducted (n = 27). The results indicated significant differences in BDI-II scores across time points (χ²(3) = 47.08, p < .0001). Post-hoc analyses revealed that all pairwise comparisons were significant (p < .01), except for the comparison between the 3- and 6-month follow-ups (p = .484), suggesting stabilization. The largest effect size was observed between baseline (initial) and post-treatment scores (d = 1.82), indicating a strong immediate reduction in depressive symptoms. Detailed results of pairwise comparisons are presented in Table 2.
| Comparison | Mean Differences | z-value | W | p-value | Cohen’s d |
|---|---|---|---|---|---|
| Initial vs. Final | 12.15 | -4.541 | 0.0 | p < .0001 | 1.819 |
| Initial vs. 3 months | 7.33 | -2.895 | 68.5 | p = .0030 | 0.645 |
| Initial vs. 6 months | 8.04 | -4.324 | 9.0 | p < .0001 | 1.294 |
| Final vs. 3 months | -4.81 | -3.207 | 55.5 | p = .0023 | -0.672 |
| Final vs. 6 months | -4.11 | -4.108 | 18.0 | p = .0003 | -0.762 |
| 3 months vs. 6 months | 0.70 | -0.985 | 148.0 | p = .4843 | 0.084 |
3.2 Treatment Response Trajectories and Follow-up Outcomes
Individual trajectory analyses indicated strong treatment effects at post-treatment. All participants (100%) showed some level of improvement, with a mean reduction of approximately 79.8% in depressive symptoms relative to baseline. Most participants achieved substantial clinical gains, with 92.6% showing at least a 50% reduction in symptoms and 74.1% achieving reductions of 75% or more.
Across follow-up assessments, treatment gains showed partial attenuation but remained below baseline levels overall. Mean symptom reduction relative to baseline was 48.2% at 3 months and 52.7% at 6 months. Relapse rates, defined as loss of more than 50% of the initial improvement, were 37% at 3 months and decreased to 29.6% at 6 months, suggesting some stabilization of treatment effects over time.
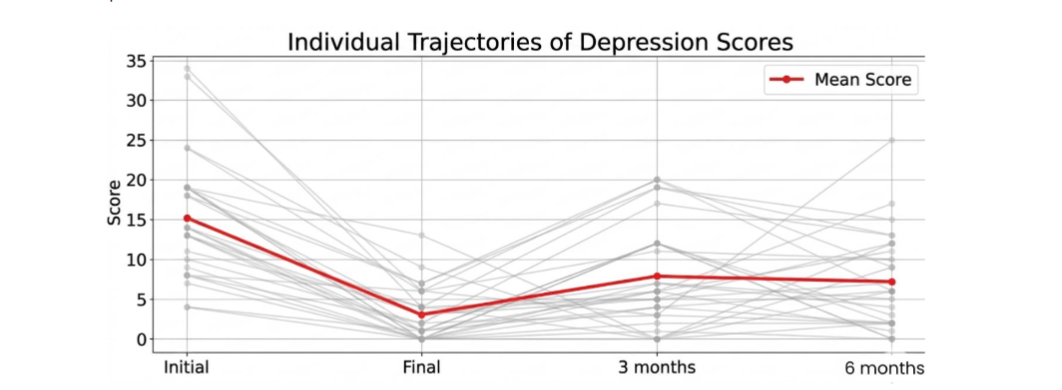
Reliable Change Index (RCI) analyses supported these findings. Most participants demonstrated reliable improvement at post-treatment, with no cases of reliable deterioration. At follow-ups, the proportion of participants maintaining reliable improvement decreased, while most showed no reliable change. Only one participant showed reliable deterioration at the 3-month follow-up, and none at 6 months. Mean RCI values remained negative across all time points, indicating overall improvement relative to baseline.
| Time point | Reliable Improvement | No Reliable Change | Reliable Deterioration | Mean RCI |
|---|---|---|---|---|
| Post-treatment | 17 (63.0%) | 10 (37.0%) | 0 (0.0%) | -2.59 |
| 3-month follow-up | 10 (37.0%) | 16 (59.3%) | 1 (3.7%) | -1.56 |
| 6-month follow-up | 9 (33.3%) | 18 (66.7%) | 0 (0.0%) | -1.71 |
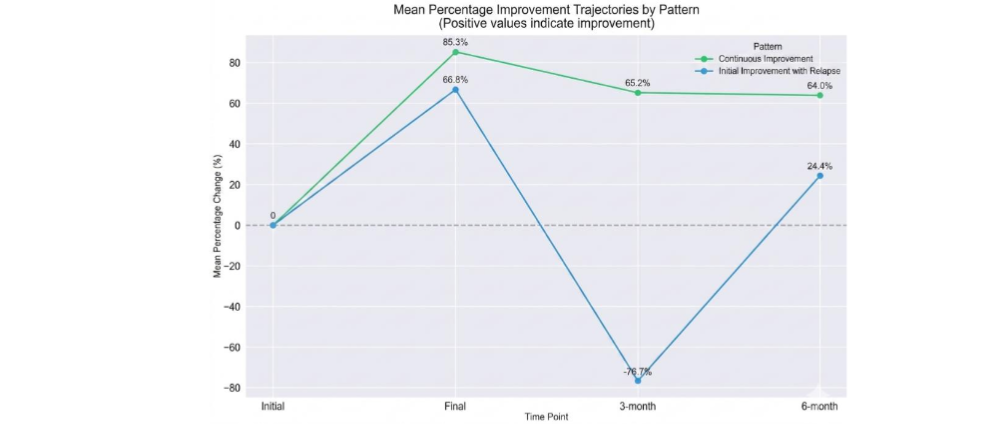
To further characterize individual response patterns, participants were grouped according to symptom trajectories. Two patterns emerged: (1) continuous improvement (74.1%), characterized by large reductions at post-treatment (85.3%) followed by partial loss (65.2%) and stabilization of gains (64.0%); and (2) initial improvement with relapse (25.9%), in which early improvement (66.8%) was followed by symptom worsening at 3 months (-76.7%) and partial recovery at 6 months (24.4%). These trajectories are illustrated in Figure 3.
3.3 Demographic Predictors of Treatment Response
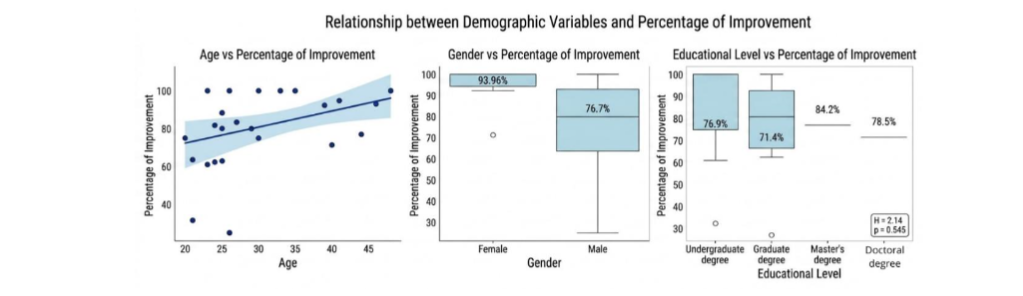
Exploratory analyses examined associations between demographic variables and treatment improvement. Associations between demographic variables and percentage of symptom improvement (initial to post-treatment) were examined using nonparametric tests. A significant difference was observed for gender (Mann–Whitney U = 29.0, p = 0.048), with women showing greater mean improvement (M = 93.96%, SD = 11.46%) than men (M = 76.66%, SD = 20.61%).
Age was positively but non-significantly associated with improvement (Spearman’s ρ = 0.31, p = 0.117). Educational level was not significantly related to treatment response (Kruskal-Wallis H = 2.14, p = 0.545), with similar levels of improvement observed across educational groups.
4 Psychological-Phenomenological Analyses of Clinical Cases
Phenomenological analysis applied to psychology, as developed by Amedeo Giorgi and Daniel Sousa, requires the explication of a rigorous procedure comprising: (a) grasping the global meaning of the lived-experience; (b) discriminating units of meaning; (c) transforming these units into psychologically relevant expressions; and (d) determining the general structure of psychological meanings. To this procedure, one may add—as proposed by Goto—the identification of psychic lived-experiences as modes of givenness of experience, which makes it possible to render intelligible the dynamics of the constitution of subjectivity within intersubjectivity. It is important to specify that such identification does not authorize direct inference of empirical contents but should be understood as an eidetic reconstruction of the conditions of possibility of experience.
5 Discussion
The results of the longitudinal analyses of this investigation showed that, although some regression occurred after three months—a phenomenon widely described in the depression literature, stabilization and improvement (d = 0.084, p = 0.4843) were observed between three and six months, with maintenance of therapeutic gains. The most relevant finding is not merely statistical; rather, it is the predominance of the “Continuous Improvement” pattern, observed in 74.1% of participants, which suggests the consolidation of transformations in the dynamics of meaning in subjective experience, rather than mere symptom reduction.
5.1 Intersubjectivity as a Requirement for the Constitution of Psychic Life
The interpretation of the results requires rigorous epistemological grounding, as outlined by Phenomenological Psychology. Within this horizon, psychic life cannot be understood as a closed system of causalities, but rather as an intentional structure in the process of constitution, whose intelligibility depends on the analysis of the correlations between lived-experience, meaning, and world.
Phenomenological analysis of the clinical material allowed the identification of units of meaning linked to the impact of lived-experiences on the configuration of subjectivity. In determining the general structure of meanings, structuring nuclei of depressive suffering were identified, understood as originary configurations of meaning that organize the experience of the “I” and the “other” over time.
In this regard, as noted in previous research, and similarly in the present study, participants described affective-emotional experiences occurring in the intrauterine stage and early childhood, primarily related to conflictual intersubjective dynamics between parental figures. These dynamics involved an intrafamilial psychic inheritance, whose meanings were described as disorganizing and pathological.
It is necessary to introduce an important conceptual distinction: from a phenomenological perspective, this is not a “transmission of psychic contents” in a substantial sense, but rather an intersubjective constitution of meanings within shared horizons. This reformulation is essential to avoid a relapse into explanatory models of a causal or substantialist type. In general, the psychic contents reported by participants were associated with situations involving various forms of unethical behavior, such as incest, sexual abuse, power relations, abandonment, betrayal, murder, theft, and lying, among others, confirming, in clinical practice, themes also examined by Kaës, Kaës and Faimberg and Eiguer.
Moreover, these transgenerational psychic contents appeared not only as indicators of different modes of pathological formation, but above all as distinct psychic strategies through which psychic suffering is structured, composing a psychic material that circulates within the unconscious and serves as a reference for the psychic formation of descendants. Therefore, the way parents relate demonstrates that intersubjectivity, as the primary environment of self-formation for the child’s psyche, is built upon what derives from other “I”s within the ancestral intrafamilial fabric. Accordingly, one cannot speak of intersubjectivity without considering the family fabric that precedes descendants and within which their psyches are likewise woven.
This phenomenon was likewise observed in the clinical experience of Jost de Moraes when the author identified that the dynamics of parental conjugality, shaped by the intrafamilial psychic inheritance of each spouse, constitute one of the most significant contexts for the psychic formation of descendants.
Family psychoanalysis also describes processes of intergenerational transmission and considers that the subject is both individual and group-based, and that the family is configured as an intersubjective matrix for the emergence of psychic life. However, it differs epistemologically from Phenomenological Psychology and the ADI/TIP Method, insofar as phenomenology reinterprets such phenomena not as a transfer of contents, but as a constitution of meanings within shared intersubjective horizons. This perspective is supported by the analyses of Stein, for whom communal life constitutes the locus of formation of subjectivity; that is, living with others entails a dynamic interweaving of actions, affections, and position-takings, through which subjects co-form one another.
As such, intersubjectivity is understood as a foundational basis for the formation of psychic reality, shaped within intersubjective bonds and groupings through dynamic unconscious processes, so that each individual bears the mark, in terms of structure and content, of the unconscious of others. It is further considered that the family group that precedes the subject constitutes the originary space of intersubjectivity, understood as a psychic cradle, a primary group, and a basic matrix in the production of subjectivity.
Phenomenological Psychology highlights generative constitution as succession, traditionality, and communal intersubjective dynamics, beginning in intrauterine life and extending into adulthood through different modes of appropriation of material shared across generations, from corporeality to psychospiritual life. It enables an understanding of subjectivity as situated within a historical chain of meaning, in which tradition, culture, and intersubjectivity constitute the horizon of its formation. It also elucidates the generative nexus, infinitely open between nature and culture, showing how biological, psychic, and spiritual life, from the outset, is immersed in culture and in the chain of generations, encompassing both preexisting and contemporary family and social bonds.
Likewise, it clarifies that the organic body constitutes the substratum and condition of possibility for “the experience of a lived-body” (Leib) as an experience and dynamic animated by a “psychospiritual and personal subjectivity.” This issue is fundamental for understanding intersubjective experience as enacted by personal subjectivity, whose acts impact psychophysical dynamics.
Within this framework, it becomes evident that, from the prenatal stage onward, the body and the psyche develop and are constituted through the interrelation between aspects of nature and culture, and are affected by other “I”s that constitute this same space. Given that human psychic life is grounded in intersubjectivity, intentionality is a fundamental lawfulness of psychic life, structuring both its subjective and intersubjective dimensions. Psychic life thus appears as contextualized and carries with it exteriority in its historicity, as a narrative of a familial and cultural horizon that is always shared, expressing intentionality in the continuity of past and of traditions, in the chain of generations, and in spiritual and cultural activity.
In this study, participants described how their position-takings in relation to lived events are permeated by meanings attributed to experience and to themselves, composing contents that, although harmful, may become inscribed in psychic and bodily life. These contents “tonalize” personal life, potentially altering both its dynamism and self-perception, thereby giving rise to a wide range of symptomatology corresponding, in this context, to depression. It is also necessary to note that experience and lived-experience reveal the dynamic interplay of three fundamental elements that express intentionality in psychic life: the I that observes an object, the object observed, and the act in which the I lives each event and directs itself toward an object in a personal manner. From this perspective, psychic life appears open to existence, within which contents of meaning become inscribed through the relation between the I and the world, and between the I and other “I”s. This means that the “vital energy” that sustains body and soul is incited by the surrounding world, and that psychic states are not indifferent to what returns to the interior of the human being.
In the present analysis, a continuous interrelation has already been identified between lived-experience, configured contents of meaning, the conformation of these meanings to psychic reality, and depressive symptoms. It is now emphasized that, at the center of this movement, lies the person’s position-taking, which, as noted, is an essential element for understanding the possibility of altering the dynamism of psychophysical life.
In this regard, Stein explains that, on the one hand, not all contents appropriated in experience lead the person to “be in oneself,” while on the other hand, repositioning through lived intersubjective experience can also operate upon the psyche and its states in a different way. In other terms, psychic states, as lived-experiences, cannot be explained by purely causal laws, since what is lived expresses, at the same time, the intentional character of experiencing.
Accordingly, the constitution of intersubjectivity and of egological subjectivity (at a pre-reflective level), from “transcendental birth,” that is, “from the still unborn pre- or proto-infantile body (vorkindliche Monade ou Urkind),” indicates those experiences grounded in the intrauterine phase. These “correspond to perceptual horizons, givens, and sensory fields,” within which “the human being is a pre-ego, a unity of affects, primary associations, and innate bodily and biophysical instincts,” entirely inseparable from culture.
At this stage, primary contact occurs between the proto-infantile and a world that precedes it, whose history is shaped by tradition and culture: “The whole process, from prenatal tendencies to reason and universal intersubjectivity (…) is preceded by prior experiences that are habitual, tendencies, impulses, and inclinations inherited from the generations that preceded it through its parents.”
More specifically, Husserl describes the existence of experiences grounded in the intrauterine stage, arising from a first affection of the I (proto-infantile), which appropriates the inheritance that precedes it, transmitted through its parents. The author clarifies that psychorganic predispositions are already present, but distinguishes two moments concerning the modes of appropriation of transmitted psychic material: the pre-egological moment, in which the first appropriations begin in the body and extend to the psychic layer, operating passively; and the egological moment, corresponding to the life of awakened consciousness, in which appropriation occurs in an objective manner.
The experiences described by participants confirm the results of these analyses of generative phenomenology, demonstrating that the transmissibility of psychic life occurs through lived intersubjective experience, since it is only possible by virtue of an act that enables contact with the subjectivity of the other (alter-ego), allowing it to be felt, grasped, known, and accessed as the object or content of the other’s experiences: the concept of empathy (Einfühlung). However, nature, at each stage of life, has a singular mode of appropriating what is shared, depending on the development of its structures, and is therefore only possible after birth.
Nonetheless, it is undeniable that, even before birth, the shared world already acts upon and affects human nature in its hyletic dimension, and that transmissibility and appropriation operate differently within the passive structures of psychophysical life, rooted in lived bodily materiality as the primary mode of pre-reflective intentionality in relation to the horizon of the world.
At the core of psychic transmission, psychic indeterminism becomes evident when phenomenological analyses reveal the structure of the human person, showing that subjectivity has a dual aspect governed by distinct yet coexisting laws: the soul is both psychic and spiritual, that is, “psychospiritual.”
According to Husserl, the meaning of things in the life-world points to the genesis of the activities of a creative subjectivity, since meaning refers to a subjectivity capable of constituting meaning. Thus, everything that is already given in the experience of the community as a “product of the spirit,” that is, as a “cultural object,” points to a layer of subjectivity that is active, distinct from the psychic layer, conceived as a purely passive sphere. The creative subject implies that the spirit objectified as culture refers, in its origin, to the spirit of the person “in the life of the soul.” The genesis of what is specifically spiritual therefore differs from the psychic dimension of passivity, insofar as it points to a life that unfolds in acts that have the “I” as their center.
This layer of consciousness, termed active consciousness, is regarded as a higher level pertaining exclusively to the human being, since it concerns the entirety of personal life and, from there, the whole of social and historical life and work that extends beyond singular individuals. Simple receptivity, which corresponds to the lower and passive stages of psychic life, namely the passive layer of consciousness, is a non-perceptual experience (unge-wahrendes) that occurs prior to perceptive experience (gewahrenden erfahren), that is, before any active participation of the I. The same applies to the passive feeling of affectively turning toward or away from what presents itself in the world.
This means that each act, such as I perceive, I apprehend, I consider, or I theorize, originating from the I-center, presupposes that what is apprehended was already present within the passive receptivity of consciousness (termed the unconscious), in the form of affection and excitation, yet had not been apprehended within the field of consciousness of this active I-center. In this domain, the physical body, in the sense of animal experience, does not exist only as a purely physical causality in its relation to the objective world. The life of the soul cannot be reduced to a real unity resulting from inductive causality, since at a higher level the inductive and causal character does not constitute the real being of what pertains to the spiritual layer of the soul.
As previously indicated, the soul has a dual structure: a life in which passive faculties are constituted, such as perception, feeling, pleasure, pain, and memory, and a life of active faculties, including perception and intellectual operations such as gathering, comparing, distinguishing, universalizing, concluding, and proving.
According to Stein, there is a psychic causality and, alongside it, a motivational causality proper to spiritual life, which introduces a principle of indeterminacy and openness in the constitution of subjectivity. The latter is, in its essence, entirely irreducible to inductive causality, even though the latter coexists with it and plays a role in psychic life.
The coexistence of these laws makes it possible to understand the transmissibility of psychic life and depressive states beyond psychic determinism and inductive causality as conceived by the Natural Sciences. Indeed, as reiterated by Husserl, it is a mistake to reduce the life of the soul to a biopsychic parallelism that assumes its structural and ontological form to be identical to that of the physical body and its laws.
In light of these considerations, the clinical results can be understood with greater rigor, since the observed processes of self-configuration and reconfiguration do not result from mechanical modification of psychic contents, but from a repositioning of the I in relation to lived events and appropriated psychic inheritance. It becomes clear that understanding depressive illness requires the intelligibility of psychic life, encompassing intersubjectivity, within which the phenomenon of the transmissibility of psychic life between subjects and generations takes place.
The phenomenon of intergenerational psychic transmission is identified in the clinical experience of Jost de Moraes as a natural, constitutive, and universal process that occurs in intersubjective relations, with parents serving as the primary psychoaffective references in the psychic formation of their children. This means that their psychic formation is built upon the psychic chain of preceding generations, and that parents are among the principal transmitters of psychic life from earlier generations, whether in a conscious or unconscious mode.
Taken together, subjectivity is both heir to and constituted within an intersubjective narrative of preceding generations. However, this does not amount to an absolute and closed psychic determinism, as shown by the studies of Almeida, as well as Almeida and Goto. Indeed, through the clinical investigation of the ADI/TIP Method, it becomes evident how psychic inheritance is presented and appropriated from the gestational stage onward, becoming part of the child’s psychic formation.
Finally, these analyses allow us to consider that no human phenomenon, including depressive illness, can be reduced to a rigid inductive causality if the aim is to grasp it in its full scope. The phenomenological perspective, by apprehending subjectivity in its structural totality, makes it possible for what is properly human to emerge: the capacity to constitute meaning and to reposition oneself in relation to it. In this regard, Husserl affirms that when the scientist directs their gaze toward subjective phenomena with the precision and rigor of a science of the spirit, what is most elevated in the Human Person emerges and, consequently, the soul in its totality.
5.2 Intersubjectivity: From Repositioning to Psychic Change
To understand the results of the quantitative changes, it is necessary to recognize that self-formation and the reconfiguration of the I, as explicated by Phenomenological Psychology and described by participants, indicate that lived-experiences (properties) typical of active life (spiritual-I) are foundational and self-determining in their interface with psychic lived-experiences (properties) in relation to intersubjectivity, generativity, and depression. This assertion helps to grasp, throughout the psychotherapeutic process and in the sustained maintenance of the gains achieved, a continuous dynamism in the flow of structural lived-experiences and their correlates, as well as in the connections of subjective and intersubjective meanings.
It is understood that both psychic lived-experiences and their contents do not remain rigid and unaltered throughout existence, as they are subject to the aspiration toward fulfillment, perfection, and being oneself, as well as to the motivations arising from lived experiences and, finally, to the creative agency that imparts to them their particular tonal quality.
The act of change, as a creative act, emerges within the sphere of spiritual motivation, in which the I, as the center of decision, can reconfigure its relation to the sedimented meanings of experience. This is a form of motivational causality, linked to will and freedom, insofar as it refers to the aspiration toward and realization of values and purposes, among which the demand to “become oneself” stands out. In this way, the creative act traverses the self-configuration and, equally, the reconfiguration of oneself, since it occurs with the active participation of a personal core, the personal I. Jost de Moraes confirms phenomenological analyses by observing that it is not the psyche that modifies the psyche in psychotherapy, but rather that only from the humanistic (spiritual) dimension, precisely through the Personal I, does the human being possess the freedom, decision, strength, and capacity to transform psychological reality.
Against this background, within the phenomenon of clinical experience related to events that mobilize therapeutic change, subjects are enabled to deepen their perception of themselves and of others involved in the problem-situation, promoting movements of openness toward new horizons of understanding. This process enables new apprehensions of what is lived and allows for the “decoding” and repositioning of psychic and existential registers previously configured in a pathological manner.
In the process of therapeutic change, both the re-signification of the same lived event, previously valued as negative and now transformed into a constructive valence, and the experience of other events centered on trust, love, belonging, recognition, and appreciation, produce a subjective and intersubjective opening of a spiritual nature. As a consequence, changes are observed in psychic states, in perceptions of reality and of oneself, as well as significant transformations in modes of relating to others and to life. Such experiences correspond to the psychic and existential needs of the human being for a healthy development, insofar as they introduce contents that reconfigure psychophysical reality and motivate the person to be rooted in oneself and to reconstruct affective bonds in an ethical and non-pathological manner.
6 Conclusions
Depressive illness cannot be reduced to a naturalistic psychophysical account that excludes subjectivity in its totality as a psychospiritual unity, with its distinct properties and laws in unity with the lived body. Apprehending this structural unity, together with its process of self-formation grounded in intersubjectivity, proves essential for addressing the psychic and existential needs of the person, which are decisive for healthy psychophysical development.
Phenomenological Psychology provides the necessary framework to render depressive suffering intelligible. The quantitative and qualitative findings further demonstrate the significant contribution of the ADI/TIP Method as an instrument for understanding and treating depressive suffering. It is suggested that longitudinal studies with a longer time span and a larger number of participants be increased.
Conflict of Interest Statement: The authors have no conflicts of interest to declare.
Funding Statement: The authors received no funding for the work.
Acknowledgements: We thank all the professionals who participated in this research, and especially the psychologists who contributed to the psychotherapeutic sessions.
References
- Jost MC, Goto TA, Almeida E. Research advances on intervention in depressive suffering: direct approach to the unconscious method in a personal integration therapy. European Society of Medicine. 2025;13(5):1-13. https://doi.org/10.18103/mra.v13i5.6558.
- Jost MC, Goto TA. Psicoterapia, mudança, novas intervenções: o Método ADI/TIP – uma nova possibilidade de psicoterapia? [tese de pós-doutorado]. Uberlândia, Minas Gerais (Brasil): Universidade Federal de Uberlândia; 2018.
- Jost de Moraes R. As chaves do inconsciente. SPES; 1985/2016.
- Jost de Moraes R. O inconsciente sem fronteiras. Santuário; 1995/2008.
- Jost MC, Goto TA. Depression, Psychotherapie und Veränderung: die ADI/TIP-Methode, Psychologie und Phänomenologie. SFU Forschungsbulletin SFU. Research Bulletin. 2021;9(1):42-64. https://doi.org/10.15135/2021.9.1.42-64.
- Stein E. La estructura de la persona humana. Biblioteca de Autores Cristianos; 1932-1933/2007.
- Husserl E. A criança. A primeira empatia. Revista da Abordagem Gestáltica: Phenomenological Studies. 1935/2017;23(3):375-377. https://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1809-68672017000300013.
- Husserl E. Psychologie phénoménologique. Vrin; 1925/2001.
- Almeida E, Goto TA. Transgeracionalidade, subjetividade e conjugalidade: pesquisa psicológico-fenomenológica sobre transmissão psíquica e cultural entre gerações na práxis do Método ADI/TIP. In Sidoncha U, Feron O, Sidoncha I (orgs.). Fenomenologia e Cultura. Praxis; 2022.
- Lewis SE. The social construction of depression. University of Glasgow; 1996.
- Fonagy P, Luyten P. Attachment, mentalization, and the self. In Livesley WJ, Larstone R. Handbook of personality disorders: theory, research, and treatment. The Guilford Press; 2018.
- Liljenfors R. Mentalization and intersubjectivity: towards a theoretical clarification. Psychoanalytic Psychology. 2015;32(4):593-615. https://psycnet.apa.org/doi/10.1037/a0037129.
- Cano-López JB, García-Sancho E, Fernández-Castilla B, Salguero JM. Empirical evidence of the metacognitive model of rumination and depression: a systematic review and meta-analysis. Clinical Psychology Review. 2022;91:102116. https://doi.org/10.1007/s10608-021-10260-2.
- Solem S, Hagen R, Hoksnes JJ, Hjemdal, O. The metacognitive model of depression: an empirical test. Cognitive Therapy and Research. 2016;40:800-807. https://doi.org/10.1016/j.psychres.2016.05.056.
- Bianciardi E, Ongaretto F, De Stefano A, Siracusano A, Niolu C. The mother-baby bond: role of past and current relationships. Children (Basel). 2023;10(3):421. doi: 10.3390/children10030421.
- Wan MW, Green J. The impact of maternal psychopathology on child-mother attachment. Arch Womens Ment Health. 2009;12(3):123-34. doi: 10.1007/s00737-009-0066-5.
- Bellina M, Grazioli S, Garzitto M, Mauri M, Rosi E, Molteni M, Brambilla P, Nobile M. Relationship between parenting measures and parents and child psychopathological symptoms: a cross-sectional study. BMC Psychiatry. 2020;20(1):377. doi: 10.1186/s12888-020-02778-8.
- Maguire A, Ross E, O’Reilly D. Parental mental health and risk of poor mental health and death by suicide in offspring: a population-wide data-linkage study. Epidemiol Psychiatr Sci. 2022;31:e25. doi: 10.1017/S2045796022000063.
- Jost MC, Almeida E. L’Amore come strumento di trasformazione “psiconoosomatica”. Il metodo ADI/TIP di Renate Jost de Moraes: una psicoterapia integrativa della persona umana. La Sapienza della Croce. 2020;XXXV(2);307-322.
- Jost MC, Goto TA. Intervenção clínica no sofrimento depressivo: Método ADI/TIP, Psicologia e Fenomenologia dos afetos. Psicologia: Teoria e Pesquisa. 2022;38:e38422. https://doi.org/10.1590/0102.3772e38422.pt.
- Husserl E. Husserliana XI. In Husserl E, Fleischer M (orgs.), Analysis of Passive Synthesis. From Lecture and Research Manuscripts. Nijhoff; 1918-1926/1966.
- Osswald A. La fundamentación pasiva de la experiencia. Un estúdio sobre la fenomenología de Edmund Husserl. Plaza y Valdés; 2018.
- Stein E. Introducción a la filosofia. In Stein E. Escritos filosóficos: etapa fenomenológica. Monte Carmelo; 1916/2005.