





Vaccination Trends in Diabetic Adults: A 20-Year Study
Preventive Care Practices: A Retrospective Database Study of Influenza and Pneumococcal Vaccination Among Adults with Diabetes
¹Shalom Onyinye Katas MD; ²Inelefo Roger Iyayi MD; ³Princess Okoronkwo PharmD; ⁴Derek Olatunde Olagbemi, MBBS, LMCC; ⁵Tinade Oladayo Adeakin-Dada MD, LMCC, PGCertCR; ⁶Oluwadamilola Daniel Odutola MD; ⁷Paul Akhere Momodu; ⁸Stephen N. Utulor MD; ⁹Uzodimma Joseph Nwadiingwe MBBS; ¹⁰Oluwabusayo Monsurat Osundiji MD; ¹¹Okelue E. Okobi MD
- School of Medicine, International University of the Health Sciences (IUHS) Basseterre, St. Kitts & Nevis
- Department of Medicine and Surgery, University of Benin, Edo State, Nigeria
- Department of Pharmacy, D’youville University, Buffalo, NY
- College of Medicine, University of Lagos, Lagos, Nigeria
- Department of Medicine, Windsor University School of Medicine, St Kitts and Nevis
- Department of Internal Medicine Medical University of South Carolina, SC, USA
- Department of Medicine, International University of the Health Sciences Basseterre, St Kitts and Nevis
- Department of Medicine, International University of the Health Sciences (IUHS) School of Medicine, Basseterre, St Kitts and Nevis
- Department of Medicine, University of Nigeria Teaching Hospital Ituku, Nigeria
- Department of Medicine, St Martinus University, Curacao, Netherland Antilles
- Department of Family Medicine, Larkin Community Hospital (PSC), Miami, FL, USA
OPEN ACCESS
PUBLISHED:31 July 2024
CITATION: Katas, SO., Iyayi, IR., et al., 2024. Preventive Care Practices: A Retrospective Database Study of Influenza and Pneumococcal Vaccination Among Adults with Diabetes. Medical Research Archives, [online] 12(7). https://doi.org/10.18103/mra.v12i7.5745
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i7.5745
ISSN 2375-1924
ABSTRACT
Background: Diabetes mellitus is a prevalent chronic disease that significantly increases the risk of complications from infections such as influenza and pneumococcal disease. Despite established recommendations for vaccination, coverage rates among adults with diabetes remain suboptimal. This study aims to analyze trends in influenza and pneumococcal vaccination rates among adults with diabetes using the United States Diabetes Surveillance System (USDSS) database.
Methods: This retrospective database study utilized data from the USDSS from 2000 to 2022, which provides comprehensive nationwide data on diabetes care. The study population included adults aged 18 and above with a documented diagnosis of diabetes. Data were extracted on demographic variables (age, sex, race/ethnicity), clinical characteristics (type of diabetes, duration of diabetes, comorbid conditions), and vaccination records. Descriptive statistics summarized demographic and clinical characteristics, while temporal trends in vaccination rates were analyzed using graphical representations.
Results: Over the past two decades, influenza vaccination rates among adults with diabetes increased from 41.4% in 2000 to 56.7% in 2019, reflecting improved awareness and healthcare practices, though slightly dipping to 54.2% in 2022. In contrast, pneumococcal vaccination rates showed more variability, starting at 29.3% in 2000, peaking at 39.4% in 2018, and declining to 30.2% in 2022, indicating challenges in maintaining high coverage. Influenza vaccination rates showed an overall increasing trend across all demographic groups: rates among Hispanic individuals increased from 32.1% in 2000 to 55.4% in 2022, non-Hispanic Whites from 43.4% to 52.7%, and non-Hispanic Blacks from 39.2% to 44.5%. Pneumococcal vaccination rates also increased but displayed more variability; Hispanic rates peaked at 33.3% in 2016, non-Hispanic Whites at 45.6% in 2019, and non-Hispanic Blacks at 41.7% in 2017. Higher educational attainment was consistently associated with higher vaccination rates for both vaccines.
Conclusions: This study highlights significant improvements in influenza and pneumococcal vaccination rates among adults with diabetes over the past two decades. However, disparities remain, particularly among racial and educational groups. Targeted strategies are necessary to address these disparities and enhance vaccination coverage, ultimately reducing the risk of severe infections in this vulnerable population.
Keywords
Preventive care, influenza, pneumococcal, vaccination trends, epidemiology, racial disparities, educational disparities, USDDS database, adults with diabetes.
INTRODUCTION
Diabetes mellitus, a chronic metabolic disorder characterized by hyperglycemia, poses significant morbidity and mortality risks globally. Among its various complications, the susceptibility to infections, particularly influenza and pneumococcal diseases, is notably heightened due to compromised immune responses. Preventive care practices, such as vaccination, are crucial in mitigating these risks and improving health outcomes among individuals with diabetes.
Vaccination against influenza and pneumococcal diseases is an essential component of comprehensive diabetes management. Influenza can lead to severe complications in diabetic patients, including exacerbation of hyperglycemia, pneumonia, and even death. Similarly, pneumococcal infections can result in invasive diseases like bacteremia, meningitis, and severe pneumonia, conditions to which diabetic individuals are more susceptible.
Before it was fully understood, the emergence of SARS-CoV-2 led to widespread illness and death in North America and beyond due to respiratory infections. Given the ongoing global impact of COVID-19, it was important to evaluate the use of vaccines aimed at preventing influenza and pneumonia, which are also common respiratory illnesses.
SARS-CoV-2 infection increases the risk of thromboembolism and is more likely to induce cardiorespiratory failure in patients with diabetes mellitus than in patients without diabetes mellitus. All of these mechanisms are now believed to contribute to the poor prognosis of patients with diabetes mellitus complicated by COVID-19. Noale et al conducted a web-based survey in 2020 and found that the adult and older respondents who had received an anti-pneumococcal vaccination in the previous year had a lower probability of having a positive SARS-CoV-2 test compared with their non-vaccinated counterparts. The influenza vaccination also reflected this trend albeit in only the participants aged <65 years. This further justifies the need to promote immunization of diabetics against pneumonia.
In a Japanese study of hospitalized patients ≥65 years of age during 2014–2018, 1355 patients were retrospectively enrolled. These comprised 1045 who had not been vaccinated against S. pneumoniae and 315 who had. Prior pneumococcal vaccination was associated with shorter hospital stays and reduced all-cause in-hospital mortality.
Despite guidelines recommendations, vaccination rates among adults with diabetes often fall short of public health targets. A survey by Dallagiacoma et al. reported that self-reported seasonal influenza immunization coverage among diabetic patients was 36%, but only 21.7% according to regional immunization registries, well below the 75% target. Diabetologists were the most trusted source of vaccine information (85.3%). Various factors, including socio-demographic variables, healthcare access, and awareness levels, influence vaccination uptake. Previous studies have highlighted disparities in vaccination rates, with lower rates observed among certain racial and ethnic groups, lower socioeconomic strata, and regions with limited healthcare infrastructure. A scoping review by Mastrovito et al. found that influenza vaccination, recommended for those ≥6 months, reduces mortality and hospitalizations in diabetics but rarely meets the WHO’s 75% coverage target. Higher vaccination rates are linked to advanced age, comorbidities, and healthcare provider advice, while fear of side effects and vaccine effectiveness concerns are barriers. A questionnaire-based study conducted by Karagun et al., reported that patients relied mainly on doctors for vaccine information. Vaccination awareness was influenced by comorbidities and educational status, highlighting the importance of doctor-centred promotion programs. Understanding these disparities is crucial for developing targeted interventions to improve vaccination coverage.
The United States Diabetes Surveillance System (USDSS) database provides a robust platform for examining preventive care practices among adults with diabetes across the United States. It encompasses a wide range of demographic, clinical, and behavioral data, allowing for a comprehensive analysis of vaccination patterns and associated factors. By leveraging this database, this study aims to provide a detailed retrospective analysis of influenza and pneumococcal vaccination rates among adults with diabetes, identifying key determinants and disparities in vaccination uptake.
This study focuses on analyzing preventive care practices, specifically influenza and pneumococcal vaccination, among adults with diabetes using data from the USDSS database. The objectives include determining the prevalence of influenza and pneumococcal vaccination among adults with diabetes, identifying demographic, socio-economic, and clinical factors associated with vaccination uptake, and assessing temporal trends in vaccination rates over recent years. By achieving these objectives, the study aims to provide valuable insights into the current state of preventive care practices among diabetic individuals and inform future public health strategies.
METHODS
STUDY DESIGN AND DATA SOURCE
This retrospective database study utilized the USDSS database, which provides comprehensive nationwide data on diabetes care, including preventive care practices. The study focused on adults aged 18 and older with a documented diagnosis of diabetes from 2000 to 2022. The USDSS database was selected for its extensive collection of longitudinal data on diabetes management and associated health outcomes, making it particularly suitable for analyzing trends in vaccination practices over a significant period.
STUDY INCLUSION AND EXCLUSION CRITERIA
The study population comprised adults diagnosed with diabetes. Inclusion criteria were as follows: (1) age 18 years or older, (2) documented diagnosis of diabetes, and (3) availability of vaccination records for both influenza and pneumococcal vaccines. Exclusion criteria included: (1) missing data on vaccination status, (2) individuals younger than 18 years, and (3) incomplete demographic information. These criteria ensured a well-defined and representative sample of adults with diabetes, facilitating accurate analysis of vaccination trends.
DATA EXTRACTION AND VARIABLES
Data were extracted from the USDSS database on several key variables, including demographic factors (age, sex, race/ethnicity), clinical characteristics (type of diabetes, duration of diabetes, comorbid conditions), and vaccination records. The primary outcomes were the receipt of influenza and pneumococcal vaccinations. Secondary outcomes included temporal trends in vaccination rates over the study period and differences in vaccination rates based on demographic and clinical characteristics. This comprehensive dataset allowed for a detailed examination of factors influencing vaccination practices among adults with diabetes.
DATA ANALYSIS
Descriptive statistics were employed to summarize the demographic and clinical characteristics of the study population. Temporal trends in vaccination rates from 2000 to 2022 were analyzed to identify significant changes over time, with graphical representations used to visualize these trends. Comparative analyses were conducted to assess differences in vaccination rates based on demographic and clinical variables, providing insights into disparities and identifying target areas for intervention.
ETHICAL CONSIDERATIONS
The USDSS database is de-identified and publicly available, thus individual informed consent was not required. According to 45 CFR 46.102, the Institutional Review Board (IRB) acknowledges such analysis as not constituting human subject research due to the absence of personally identifiable information. Consequently, no IRB review was necessary for this secondary data analysis. This ethical consideration ensured compliance with regulatory standards while facilitating the utilization of valuable public health data for research purposes.
RESULTS
Over the past two decades, the analysis of influenza and pneumococcal vaccination rates among adults with diabetes reveals significant trends in preventive care practices. The influenza vaccination rate has shown a steady increase. Beginning at 41.4% in 2000, it reached a peak of 56.7% in 2019, indicating a positive trend toward greater immunization coverage. This upward trajectory reflects a growing awareness and improved healthcare practices focused on the importance of influenza vaccination for diabetic patients. The percentages dipped slightly in the subsequent years but remained relatively high at 54.2% in 2022, underscoring the sustained efforts in promoting flu vaccination (Table 1).
In contrast, the pneumococcal vaccination rates have exhibited more variability. Starting at 29.3% in 2000, the rate experienced fluctuations, dipping to a low of 25.8% in 2001, and peaking at 39.4% in 2018. However, the most recent data indicates a decline to 30.2% in 2022. This inconsistency suggests that while there have been periods of improvement, maintaining high pneumococcal vaccination rates has been challenging. The peak in 2015 and 2018 shows potential progress, yet the recent decline highlights the need for renewed focus and strategies to enhance vaccination rates among adults with diabetes (Table 1).
| Year | Influenza Vaccine Total – Percentage | Influenza Vaccine Total – 95% Lower Limit | Influenza Vaccine Total – 95% Upper Limit | Pneumococcal Vaccines Total – Percentage | Pneumococcal Vaccines Total – 95% Lower Limit | Pneumococcal Vaccines Total – 95% Upper Limit |
|---|---|---|---|---|---|---|
| 2000 | 41.4 | 37.9 | 45.1 | 29.3 | 26.2 | 32.7 |
| 2001 | 40.1 | 37 | 43.3 | 25.8 | 23.6 | 28.1 |
| 2002 | 41.4 | 37.8 | 45.2 | 26.4 | 23.7 | 29.4 |
| 2003 | 43.6 | 40.2 | 47.1 | 29.1 | 26.3 | 32.1 |
| 2004 | 42.2 | 38.7 | 45.7 | 30.2 | 27.3 | 33.4 |
| 2005 | 38.4 | 34.9 | 42 | 33.3 | 30.1 | 36.7 |
| 2006 | 45.2 | 41.6 | 48.7 | 30.4 | 27.7 | 33.4 |
| 2007 | 41.1 | 37.4 | 45 | 31.6 | 28.2 | 35.3 |
| 2008 | 46.7 | 42.2 | 51.2 | 33.3 | 29.6 | 37.3 |
| 2009 | 47.2 | 43.2 | 51.3 | 32.9 | 29.7 | 36.2 |
| 2010 | 50.9 | 47.3 | 54.5 | 36.9 | 34 | 39.9 |
| 2011 | 52 | 48.7 | 55.2 | 38.9 | 35.9 | 42 |
| 2012 | 46.6 | 43.2 | 49.9 | 35 | 31.9 | 38.2 |
| 2013 | 51.6 | 48.3 | 54.9 | 38.6 | 35.7 | 41.5 |
| 2014 | 51.3 | 47.9 | 54.6 | 35.5 | 32.6 | 38.4 |
| 2015 | 51 | 47.3 | 54.7 | 39.1 | 35.4 | 43 |
| 2016 | 49.6 | 45.7 | 53.6 | 39 | 35.5 | 42.7 |
| 2017 | 50.5 | 46.7 | 54.2 | 38.1 | 34.9 | 41.4 |
| 2018 | 52.4 | 48.6 | 56.2 | 39.4 | 36.2 | 42.8 |
| 2019 | 56.7 | 52.7 | 60.5 | 38.9 | 35.2 | 42.7 |
| 2020 | 53.2 | 48.8 | 57.5 | 35.5 | 32.4 | 38.7 |
| 2021 | 55 | 51.1 | 58.9 | 35.2 | 31.7 | 38.8 |
| 2022 | 54.2 | 50.5 | 57.8 | 30.2 | 27.5 | 33 |
Based on gender
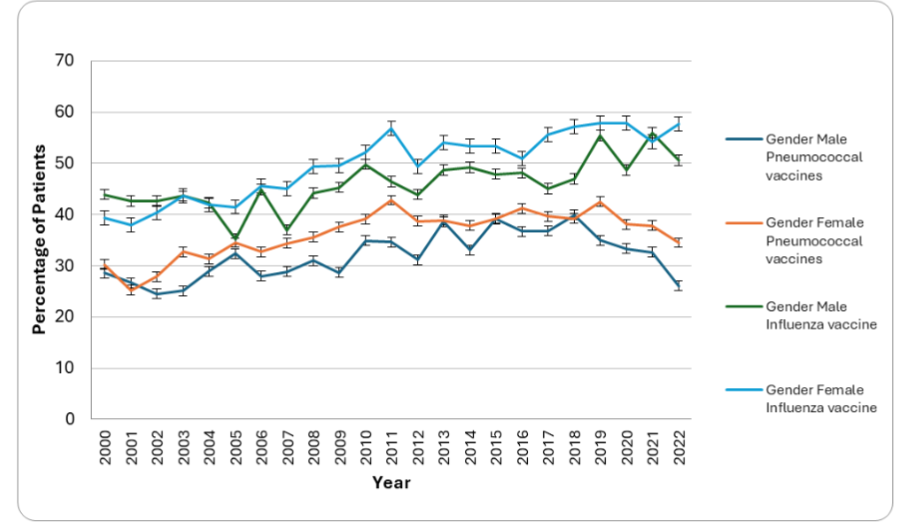
The analysis of gender-based trends in influenza and pneumococcal vaccination rates among adults with diabetes reveals distinct patterns over the years. From 2000 to 2022, pneumococcal vaccination rates for both genders showed considerable variability. Males began with a vaccination rate of 28.6% in 2000, peaking at 39.9% in 2018 before declining to 26.1% in 2022. Females started at 30.2% in 2000, experienced peaks at 42.8% in 2011 and 42.5% in 2019, and then decreased to 34.5% in 2022. Throughout the period, females generally maintained higher pneumococcal vaccination rates compared to males, though both groups showed significant fluctuations.
Influenza vaccination rates exhibited a more consistent upward trend for both genders. Males’ rates increased from 43.9% in 2000 to a peak of 55.9% in 2021, settling at 50.6% in 2022. Female rates rose from 39.3% in 2000, with a significant peak at 57.9% in 2020, remaining high at 57.7% in 2022. Females consistently showed higher influenza vaccination rates than males, with the gap widening notably in the latter years. Overall, the data highlights a more robust and sustained improvement in influenza vaccination rates for both genders, while pneumococcal vaccination rates have been more erratic, particularly for males.
Based on age group
For influenza vaccination, the 18-44 age group saw an increase from 31.5% in 2000 to a peak of 49.5% in 2019, before slightly decreasing to 44.9% in 2022. The 45-64 age group experienced a steady rise from 44.2% in 2000 to 62% in 2013, stabilizing around 59.3% in 2022. The 65-74 age group maintained relatively high rates, starting at 65.1% in 2000 and reaching 76% in 2021, before a slight decline to 71.4% in 2022. The 75+ age group had the highest vaccination rates, beginning at 70.2% in 2000, peaking at 80% in 2020, and settling at 77% in 2022.
For pneumococcal vaccination, the 18-44 age group started with low rates at 19.6% in 2000, peaking at 28% in 2019, but then dropping to 13.6% in 2022, indicating a concerning decline. The 45-64 age group saw fluctuating rates, beginning at 29.2% in 2000, peaking at 45.4% in 2013, and decreasing to 38.6% in 2022. The 65-74 age group showed relatively stable rates, starting at 55.4% in 2000, peaking at 72.5% in 2017, and settling at 63.5% in 2022. The 75+ age group had the highest rates, starting at 64.6% in 2000, peaking at 78.8% in 2017, and decreasing to 71% in 2022.
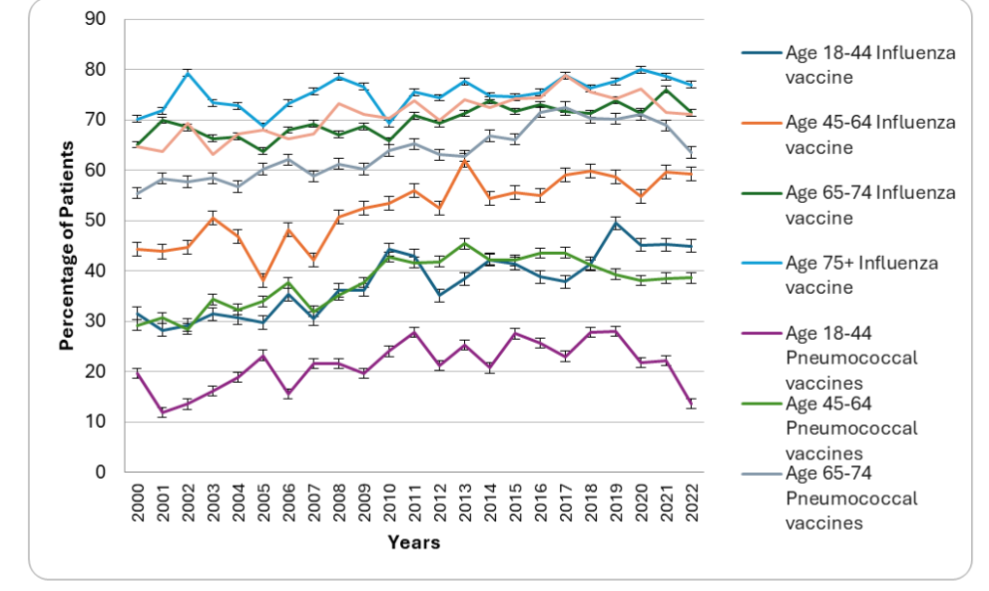
Overall, while influenza vaccination rates have generally increased across all age groups, pneumococcal vaccination rates have shown more variability, particularly in the 18-44 and 45-64 age groups. The data suggests that while older adults (65+) have better vaccination coverage, there is a need for targeted strategies to improve and maintain pneumococcal vaccination rates, especially among younger adults with diabetes.
Based on ethnicity
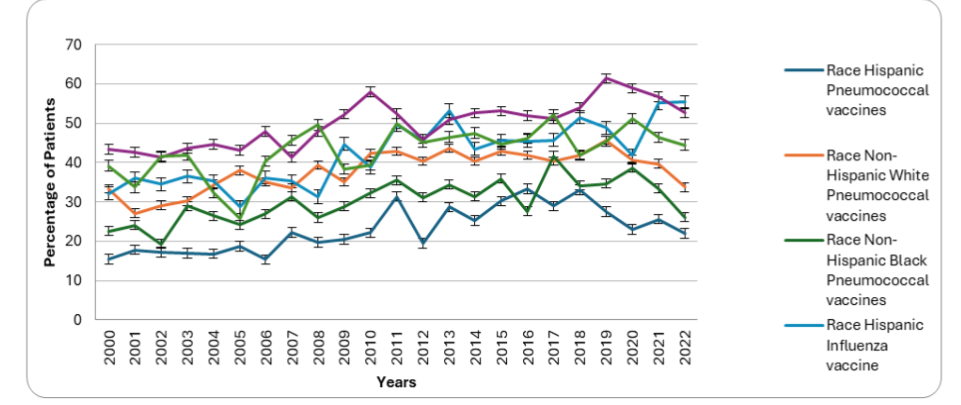
The analysis of trends based on ethnic groups reveals notable variations over the years. For pneumococcal vaccination, Hispanic rates increased from 15.4% in 2000 to a peak of 33.3% in 2016 before declining to 22% in 2022. Non-Hispanic White rates began at 33.3% in 2000, peaked at 45.6% in 2019, and dropped to 33.7% in 2022. Non-Hispanic Black rates started at 22.5% in 2000, increased to 41.7% in 2017, but declined to 26.1% in 2022.
For influenza vaccination, Hispanic rates rose from 32.1% in 2000 to 55.4% in 2022, with significant increases in 2011 and 2013. Non-Hispanic White rates increased from 43.4% in 2000, peaked at 61.4% in 2019, and then slightly decreased to 52.7% in 2022. Non-Hispanic Black rates showed an upward trend from 39.2% in 2000 to a peak of 52.1% in 2017 before declining to 44.5% in 2022. Overall, while influenza vaccination rates have generally increased across all racial groups, pneumococcal vaccination rates have shown more variability.
Based on academic level
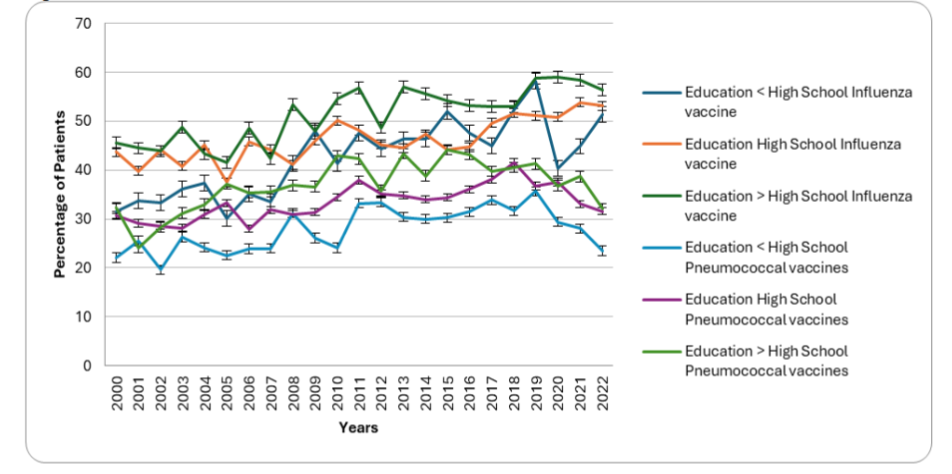
The analysis of education-based trends reveals notable disparities over the years, underscoring the impact of educational levels on vaccination behaviors. Influenza vaccination rates varied significantly across different educational groups. Among adults with less than a high school education, rates rose from 31.5% in 2000 to a peak of 58.2% in 2019, settling slightly lower at 51.4% by 2022. Those with a high school education experienced a gradual increase from 43.7% in 2000 to a peak of 53.9% in 2021, stabilizing at 53.2% in 2022. In contrast, adults with more than a high school education consistently exhibited the highest rates, starting at 45.6% in 2000, peaking at 59% in 2020, and then decreasing slightly to 56.4% in 2022.
Pneumococcal vaccination trends showed greater variability across educational groups. Those with less than a high school education began at 22.1% in 2000, peaked at 35.7% in 2019, but declined to 23.5% by 2022. The high school-educated group saw fluctuating rates, starting at 30.8% in 2000, reaching a high of 41.6% in 2018, and then decreasing to 31.6% in 2022. Conversely, adults with more than a high school education demonstrated more stable rates, starting at 32.3% in 2000, peaking at 44.2% in 2015, and settling at 32.1% in 2022. Overall, higher educational attainment correlated with higher vaccination rates for both influenza and pneumococcal vaccines among adults with diabetes.
DISCUSSION
This study provides a comprehensive analysis of influenza and pneumococcal vaccination rates among adults with diabetes, utilizing data from the USDDS database spanning two decades. The findings reveal significant trends, disparities, and implications for preventive care practices in this high-risk population, aligning with and extending upon previous studies in the field.
Previous studies have consistently highlighted the importance of vaccination in preventing influenza and pneumococcal diseases among adults with diabetes. A survey by Dallagiacoma et al. found that self-reported influenza immunization coverage among diabetic patients was 36%, dropping to 21.7% based on regional registries, far below the 75% target. The survey also revealed that among patients, 36.2% were pro-vaccine, 30.7% hesitant, 17.9% uninformed, and 15.1% anti-vaccine. Diabetologists were identified as the most trusted information source (85.3%). This study underscores the need for tailored vaccination campaigns and hospital-based programs involving diabetes specialists.
Additionally, Bechini et al.’s meta-analysis found that influenza vaccination significantly reduced mortality and lowered pneumonia-related hospitalizations. A five-year cross-sectional study using the NHI General Scheme’s claims database analyzed healthcare utilization and demographic factors alongside vaccine reimbursements to evaluate pneumococcal vaccination rates. Despite the rising prevalence of chronic conditions and immunocompromised cases, pneumococcal vaccination coverage dropped from 12.9% to 2.9%, contrasting with stable influenza coverage at 45.0%. Factors linked to pneumococcal vaccination included immunocompromised status (OR 4.72), influenza vaccination (OR 2.36–3.42), and frequent healthcare visits. These findings indicate that urgent measures are needed to boost vaccination rates among high-risk adults. These results support the push for universal influenza vaccination for individuals with diabetes.
Our findings corroborate and extend upon these studies by offering a detailed longitudinal analysis of vaccination trends across demographic subgroups, including age, gender, race, and educational attainment. Our study confirms an overall increasing trend in influenza and pneumococcal vaccination rates among adults with diabetes, although previous studies reported inconsistent trends and large populations of adults with diabetes remain unvaccinated. This aligns with broader public health efforts aimed at increasing immunization coverage among high-risk populations.
For instance, a study by Hung et al. similarly reported increasing influenza vaccination rates over time but highlighted disparities across demographic groups. From 2007–08 to 2017–18, influenza vaccination rates among U.S. adults aged ≥18 years with diabetes ranged from 62.6% to 64.8%. In the 2017–18 season, coverage was notably higher among those with diabetes (64.8%) compared to those without (43.9%). Diabetes independently correlated with higher vaccination prevalence, with factors such as higher income, more physician visits, healthcare access, and unemployment influencing rates. Despite recommendations, over one-third of adults with diabetes remain unvaccinated, underscoring the need for focused strategies to improve influenza vaccination coverage in this population.
In contrast, a study by Alzahrani et al. reported suboptimal compliance with vaccination recommendations for diabetic patients, with vaccination rates of 12.9%, 14.2%, and 15.2%. This study highlights the need for healthcare institutions to work closely with primary care physicians to develop more effective and comprehensive vaccination programs that improve adherence among diabetic patients.
Our study, in line with previous research, identifies significant disparities in vaccination rates among different demographic groups. Older adults consistently exhibited higher vaccination rates for both influenza and pneumococcal vaccines, reflecting their increased vulnerability to severe outcomes from vaccine-preventable diseases. However, disparities by race and educational attainment persist, highlighting ongoing challenges in achieving equitable vaccine uptake.
Research emphasizes the critical role of healthcare provider recommendations in improving vaccination rates among adults with diabetes. Our study underscores this finding, showing higher vaccination rates among individuals with regular healthcare access and those receiving provider recommendations. This highlights the need for healthcare system interventions that support provider education and patient engagement to enhance vaccine uptake.
A scoping review by Mastrovito et al. found that influenza vaccination for individuals aged ≥6 months significantly reduces mortality and hospitalizations in people with diabetes. Education and pharmacist interventions were crucial in promoting vaccination. Efforts are needed to increase vaccination rates through education and healthcare provider involvement.
Ronny et al. utilized North Carolina Behavioral Risk Factor Surveillance System data to analyze trends from 2011 to 2018 in influenza and pneumonia vaccination adherence among adults aged 18 and older. They found that adults with diabetes consistently showed higher adherence rates compared to those without diabetes, with rates remaining stable over the study period. Factors such as non-Hispanic white ethnicity, older age, poorer health status, insurance coverage, and non-smoking were associated with higher influenza vaccination rates among adults with diabetes. However, rates for both vaccinations remained below recommended levels, particularly among African Americans, younger adults, the uninsured, and smokers. These findings highlight vulnerable populations in need of targeted interventions to improve vaccination uptake.
STRENGTHS AND LIMITATIONS
This retrospective database study provides valuable insights into influenza and pneumococcal vaccination practices among adults with diabetes, utilizing robust data from a large dataset. By analyzing trends over multiple years and considering demographic and health factors, the study offers a comprehensive view of vaccination adherence in this high-risk population. The findings highlight consistent higher adherence rates among adults with diabetes compared to those without, which underscores the potential effectiveness of targeted vaccination efforts in this group. The study’s focus on preventive care practices is timely and essential for improving public health strategies to reduce influenza and pneumonia-related complications in diabetic adults.
However, the study is limited by its reliance on retrospective data, which may be subject to biases inherent in database analyses, such as missing or incomplete records. The study’s findings may not fully capture individual patient behaviors or barriers to vaccination that are not reflected in the dataset. Additionally, the study’s geographical and temporal scope may limit the generalizability of findings to broader populations or different healthcare settings. Future research could benefit from incorporating qualitative methods to better understand patient perspectives and experiences related to vaccination decision-making. Despite these limitations, the study provides critical evidence supporting the need for targeted interventions to enhance vaccination rates among adults with diabetes, thereby improving overall preventive care practices in this vulnerable population.
IMPLICATIONS FOR PRACTICE AND POLICY
The findings from our study have several implications for healthcare practice and policy aimed at improving preventive care practices among adults with diabetes. The findings of our study carry significant implications for healthcare practice and policy, particularly in enhancing preventive care for adults with diabetes. Tailored public health campaigns are crucial to address vaccination disparities among demographic groups, employing culturally sensitive strategies to educate and dispel misconceptions. Provider training on vaccination guidelines and communication skills is essential to combat vaccine hesitancy. Integrating vaccination reminders into electronic health records and diabetes management protocols can ensure consistent vaccine discussions during healthcare visits. Addressing barriers like cost and accessibility through policy interventions is vital for improving vaccine uptake, especially among minority groups. Future research should focus on longitudinal studies and qualitative inquiries to monitor trends, evaluate policy impacts, and develop effective interventions to promote vaccination among adults with diabetes.
CONCLUSION
This study contributes to the growing body of evidence supporting the importance of vaccination in preventing influenza and pneumococcal diseases among adults with diabetes. By addressing disparities, enhancing healthcare provider engagement, and implementing targeted public health interventions, significant strides can be made in improving vaccination coverage and reducing the burden of vaccine-preventable diseases in this vulnerable population. Continued efforts in research, policy development, and healthcare delivery are essential to achieving equitable vaccine access and uptake among adults with diabetes across diverse demographic backgrounds.
Disclaimers: This article has not been submitted to other publications and/or presented at conferences or meetings.
Source(s) of fund support: None.
Funding Statement: The research received no specific funding from any source.
Data Availability: The data used in this study was from publicly available published research papers.
Conflict of interest: All authors declare no conflicts of interest.
Regulatory Approval or Research Subject Protection Requirements: This manuscript does not require regulatory approval.
Ethical approval: This Paper does not require ethical approval.
Author contribution: All authors played several overlapping contributory roles such as Conceptualization, design, cross-referencing, and fact-checking; Formal Analysis and interpretation of data; project administration, curation, visualization, writing – original draft, writing – review & editing; supervision, oversight, and leadership, correspondence, data curation, quality control, internal review, communications, data collection and archiving, software, literature search, validation, and approval.
REFERENCES
- Sun J, Hu W, Ye S, Deng D, Chen M. The Description and Prediction of Incidence, Prevalence, Mortality, Disability-Adjusted Life Years Cases, and Corresponding Age-Standardized Rates for Global Diabetes. J Epidemiol Glob Health. 2023 Sep;13(3):566-576. doi: 10.1007/s44197-023-00138-9. Epub 2023 Jul 3. PMID: 37400673; PMCID: PMC10469163.
- Karagun B, Evran M, Odabas F, Akkus G, Kurtaran B, Sert M, Tetiker T. Awareness of Vaccination against Respiratory Tract Diseases, Including Pneumonia, Influenza, and COVID-19 in Patients with Diabetes Mellitus. Int J Clin Pract. 2022 Aug 10;2022:1389137. doi: 10.1155/2022/1389137. PMID: 36016827; PMCID: PMC9366267.
- Sözen M, Karatoprak AP, Demirhan Y, Nasırlıer GÇ, Selek A, Gezer E, Çetinarslan B, Cantürk Z, Tarkun İ, Köksalan D, Azak E. Awareness of influenza and pneumococcal vaccines in diabetic patients. J Diabetes Metab Disord. 2021 May 7;20(1):757-763. doi: 10.1007/s40200-021-00812-4. PMID: 33996650; PMCID: PMC8104465.
- Al-Sayyar A, Hulme KD, Thibaut R, Bayry J, Sheedy FJ, Short KR, Alzaid F. Respiratory Tract Infections in Diabetes – Lessons From Tuberculosis and Influenza to Guide Understanding of COVID-19 Severity. Front Endocrinol (Lausanne). 2022 Jul 26;13:919223. doi: 10.3389/fendo.2022.919223. PMID: 35957811; PMCID: PMC9363013.
- Silverii GA, Gabutti G, Tafuri S, Sarti F, Pratesi A, Clerico A, Fornengo R, Greco C, Irace C, Sordi V, Sorice GP, Cavallo M, Ponziani MC, Mannucci E, Dicembrini I; SID-AMD-SItI Working Group on Diabetes, Vaccines. Diabetes as a risk factor for pneumococcal disease and severe related outcomes and efficacy/effectiveness of vaccination in diabetic population. Results from meta-analysis of observational studies. Acta Diabetol. 2024 Apr 29. doi: 10.1007/s00592-024-02282-5. Epub ahead of print. PMID: 38684540.
- Lim S, Bae JH, Kwon HS, Nauck MA. COVID-19 and diabetes mellitus: from pathophysiology to clinical management. Nat Rev Endocrinol. 2021;17(1):11-30. doi:10.1038/s41574-020-00435-4.
- Noale M, Trevisan C, Maggi S, et al. The Association between Influenza and Pneumococcal Vaccinations and SARS-Cov-2 Infection: Data from the EPICOVID19 Web-Based Survey. Vaccines (Basel). 2020;8(3):471. Published 2020 Aug 23. doi:10.3390/vaccines8030471.
- Naito T, Suzuki M, Kanazawa A, et al. Pneumococcal vaccination reduces in-hospital mortality, length of stay and medical expenditure in hospitalized elderly patients. J Infect Chemother. 2020;26(7):715-721. doi:10.1016/j.jiac.2020.03.016.
- Alcusky MJ, Pawasauskas J. Adherence to Guidelines for Hepatitis B, Pneumococcal, and Influenza Vaccination in Patients With Diabetes. Clin Diabetes. 2015 Jul;33(3):116-22. doi: 10.2337/diaclin.33.3.116. PMID: 26203204; PMCID: PMC4503939.
- Dallagiacoma G, Allora A, Salvati S, Cocciolo G, Capraro M, Lamberti A, Senatore S, Gentile L, Gianfredi V, Laurenzi A, Molinari C, Caretto A, Faccini M, Signorelli C, Scavini M, Odone A. Type 1 Diabetes Patients’ Practice, Knowledge and Attitudes towards Influenza Immunization. Vaccines (Basel). 2021 Jun 29;9(7):707. doi: 10.3390/vaccines9070707. PMID: 34210044; PMCID: PMC8310009.
- Mercan Baspinar M, Demirali A. The Uptake of Pneumococcal and Seasonal Influenza Vaccinations Based on Perceptions and Attitudes Toward the COVID-19 Vaccine Among Patients With Diabetes. Cureus. 2024 Mar 26;16(3):e56943. doi: 10.7759/cureus.56943. PMID: 38665703; PMCID: PMC11044189.
- Mastrovito B, Lardon A, Dubromel A, Nave V, Beny K, Dussart C. Understanding the gap between guidelines and influenza vaccination coverage in people with diabetes: a scoping review. Front Public Health. 2024 Apr 19;12:1360556. doi: 10.3389/fpubh.2024.1360556. PMID: 38706547; PMCID: PMC11066301.
- United States Diabetes Surveillance System (2024). Accessed: June 21, 2024. Available at: https://gis.cdc.gov/grasp/diabetes/DiabetesAtlas.html
- 45 CFR 46 (2024). Accessed: June 21, 2024. Available at: https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/index.html
- Bechini A, Ninci A, Del Riccio M, Biondi I, Bianchi J, Bonanni P, Mannucci E, Monami M. Impact of Influenza Vaccination on All-Cause Mortality and Hospitalization for Pneumonia in Adults and the Elderly with Diabetes: A Meta-Analysis of Observational Studies. Vaccines (Basel). 2020 May 30;8(2):263. doi: 10.3390/vaccines8020263. PMID: 32486233; PMCID: PMC7349976.
- Wyplosz B, Fernandes J, Sultan A, Roche N, Roubille F, Loubet P, Fougère B, Moulin B, Duhot D, Vainchtock A, Raguideau F, Lortet-Tieulent J, Blanc E, Moïsi J, Goussiaume G. Pneumococcal and influenza vaccination coverage among at-risk adults: A 5-year French national observational study. Vaccine. 2022 Aug 5;40(33):4911-4921. doi: 10.1016/j.vaccine.2022.06.071. Epub 2022 Jul 7. PMID: 35811205.
- Thewjitcharoen Y, Butadej S, Malidaeng A, Yenseung N, Nakasatien S, Lekpittaya N, Kittipoom W, Krittiyawong S, Himathongkam T. Trends in influenza and pneumococcal vaccine coverage in Thai patients with type 2 diabetes mellitus 2010-2018: Experience from a tertiary diabetes center in Bangkok. J Clin Transl Endocrinol. 2020 May 11;20:100227. doi: 10.1016/j.jcte.2020.100227. PMID: 32395432; PMCID: PMC7212954.
- Demirci I, Haymana C, Salman S, Tasci I, Corapcioglu D, Kirik A, Yetkin İ, Altay M, Sabuncu T, Bayram F, Satman I, Sonmez A; TEMD Study Group. Rates and associates of influenza and pneumococcus vaccination in diabetes mellitus: A nationwide cross-sectional study (TEMD vaccination study). World J Diabetes. 2021 Dec 15;12(12):2107-2118. doi: 10.4239/wjd.v12.i12.2107. PMID: 35047124; PMCID: PMC8696642.
- Hung MC, Lu PJ, Srivastav A, Cheng YJ, Williams WW. Influenza vaccination coverage among adults with diabetes, United States, 2007-08 through 2017-18 seasons. Vaccine. 2020 Sep 29;38(42):6545-6552. doi: 10.1016/j.vaccine.2020.08.008. Epub 2020 Aug 18. PMID: 32819730; PMCID: PMC9063722.
- Alzahrani Z, Bashrahil B, Alzahrani MS, Alghamdi N, Nooh M, Alsolami H, Alghamdi AF, Alabbasi AA, Khan MA, Alzahrani AM. Trends In Hepatitis B, Influenza, And Pneumococcal Vaccination In Diabetic Patients. 2022. Doi: https://doi.org/10.21203/rs.3.rs-1427594/v1
- Lin C, Mullen J, Smith D, Kotarba M, Kaplan SJ, Tu P. Healthcare Providers’ Vaccine Perceptions, Hesitancy, and Recommendation to Patients: A Systematic Review. Vaccines (Basel). 2021 Jul 1;9(7):713. doi: 10.3390/vaccines9070713. PMID: 34358132; PMCID: PMC8310254.
- Almasri L, Holtzclaw BJ. Assessing Vaccine Protection for Older Adults with Diabetes: A Systematic Review. West J Nurs Res. 2022 Jun;44(6):582-597. doi: 10.1177/01939459211005710. Epub 2021 Apr 13. PMID: 33845695.
- Bell R, Imai S, Rafferty A, Little NRG, Winterbauer N, Luo H. Influenza and Pneumonia Vaccinations among North Carolina Adults with Diabetes. Am J Health Behav. 2021 Mar 1;45(2):216-225. doi: 10.5993/AJHB.45.2.2. PMID: 33888183.