






Veress Needle Entry: Force Measurement in Laparoscopy
Force required for Veress needle entry using digital force gauge during laparoscopy: Pilot study
Erin Panarelli¹, Jacqueline Early¹, Jon Serino², Andrea Kliss², Skylar Gill², Lindsay Lawrence¹, Robert Samuelson¹, and Linus Chuang¹*
- Department of Obstetrics, Gynecology, and Reproductive Biology, Nuvance Health, Danbury, CT
- Department of Research and Innovation, Nuvance Health, Danbury, CT
OPEN ACCESS
PUBLISHED:30 November 2024
CITATION:Panarelli, E., Early, J., et al., 2024. Force required for Veress needle entry using digital force gauge during laparoscopy: Pilot study. Medical Research Archives, [online] 12(11).
https://doi.org/10.18103/mra.v12i11.5903
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i11.5903
ISSN 2375-1924
ABSTRACT
Study Objective: The primary objective is to determine the mean peak force required to penetrate through fascia for entry into the abdominal cavity for establishment of pneumoperitoneum with the Veress needle during laparoscopic surgery. The second objective is to identify if body mass index (BMI), history of abdominal surgeries, or smoking contributed to peak force required to penetrate through the fascia.
Design: Prospective observational study with women undergoing laparoscopic surgery with a Veress needle and a digital force gauge attached.
Setting: Women undergoing laparoscopic gynecological surgery at Danbury Hospital in Connecticut, United States.
Patients: Women between 18 and 90 years old who underwent scheduled laparoscopic surgery (n=22).
Interventions: A digital force gauge was attached to the handle of a Veress needle. The Veress needle was inserted into the abdomen by a gynecologist using standard techniques consistent with evidence-based recommendations. The digital force gauge continuously recorded the force required to penetrate the abdominal layers during the process of gaining abdominal entry.
Measurements: Graphical and numerical data obtained from the force gauge device during Veress needle penetration.
Main Results: The mean peak force required to gain entry to the abdominal cavity was 1007 gram-force (gF) (n=22, SD=298). Force data varied widely within samples with a range of 1083 gF (min=409, max=1493). There were no significant differences in the peak force among groups stratified by age, (p = 0.327), BMI (p = 0.650), number of previous abdominal surgeries (p = 0.142), smoking status (p = 0.287), and laparoscopic entry location (0.870).
Conclusions: This study highlights the variability in insertional force to gain access to the abdomen during operative laparoscopy. These results led to the initiation of an objective method for teaching safe laparoscopic entry using a Veress needle in a simulation lab for the department of Obstetrics and Gynecology.
Introduction
Minimally invasive surgery has become the standard of care for most gynecologic procedures¹. Since the onset of laparoscopy, several abdominal entry techniques have been developed using either an open or closed technique. The Veress needle closed technique has been highly favored by gynecologists worldwide².
Complications with laparoscopy varies between 0.1% and 1.3%³. However, more than 50% of all laparoscopic injuries happen during abdominal entry³,⁴. A Cochrane review demonstrated that closed Veress needle entry is not associated with higher rates of major complications compared to open abdominal entry or direct entry techniques⁵.
It is vital that new surgeons learn to safely use the Veress needle to avoid complications. Simulation training appears to improve the laparoscopic performance among trainees in obstetrics and gynecology⁶,⁷. In one Feh study, 100% of obstetrics residents and surgical simulation trainees recommend and consider it useful for their future practice⁸.
To create a simulation program, the force required for Veress needle entry needs to be determined and how this force varies with clinical factors. The primary objective of this pilot study is to determine the mean peak force required to penetrate through fascia for entry into the abdominal cavity to establish pneumoperitoneum with the Veress needle. The second objective was to identify if body mass index (BMI), history of abdominal surgeries, or smoking contributed to the peak force. By finding the mean pressure required to penetrate fascia, a replica could be designed for training residents and surgeons to use the Veress needle for gaining abdominal entry.
Materials & Methods
STUDY DESIGN AND PARTICIPANTS
A prospective observational study was conducted to include women who were 18 years or older undergoing a scheduled gynecological laparoscopic surgery at Danbury Hospital. Women who were pregnant, unable to provide informed consent for the study or had a communicable disease, such as Human Immunodeficiency Virus (HIV), Methicillin-Resistant Staphylococcus Aureus (MRSA), Clostridium Difficile (C. difficile), were excluded. This study was conducted from August 10, 2019 to January 22, 2020 at Danbury Hospital and approved by Biomedical Research Alliance of New York (BRANY).
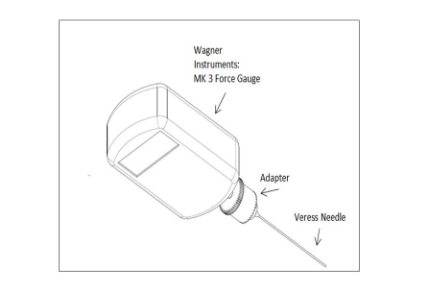
A Mark-10 Series 5 digital force gauge was used to directly measure the force used upon Veress needle entry (Figure 1). Patients were placed in standard dorsal lithotomy position, the elevation of abdomen and angle of entry varied based upon the patient’s BMI. After the patients were prepped and draped in sterile fashion, the Mark-10 Series 5 digital force gauge, adapter, and cord was draped with an ultra-sound probe cover. The Veress needle was then secured to the force adapter. The gauge was connected to a laptop with Mark-10 software documenting the continuous force applied to the Veress needle.
Fig 1: The Mark-10 Series 5 digital force gauge, adapter and Veress needle configuration used for data collection.
Location of laparoscopic entry at either the umbilicus or Palmer’s point was at the discretion of the experienced operating surgeon. The operating surgeon remained the same for every patient. Standard Veress needle insertion technique was used by elevation of the abdomen and angle of entry determined by patient’s body habitus and was performed by attending surgeon and senior Residents. The force gauge was reset to zero just prior to insertion. Insufflation with carbon dioxide gas was initiated after confirmation of intraperitoneal placement noted by low initial pressures². If additional attempts were needed, data from the force gauge was collected with each attempt.
Force vs time data exported from the force gauge software was analyzed using Microsoft Excel (Figure 2). The peak force and time required for entry were recorded. In addition, the variation in the force reading after zeroing the gauge but before a load was applied was compensated for by subtracting the average force reading from time zero to the time the surgeon began to press the needle to the skin.
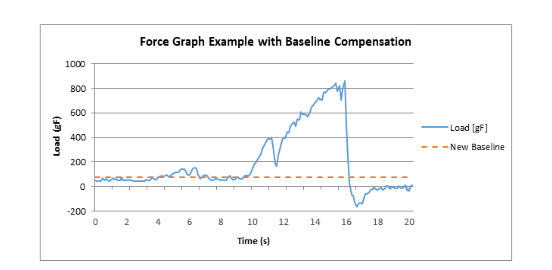
Figure 2: Example force vs time graph. Force measured by force gauge over 18 second interval (blue). Calculated baseline from average force reading after device was zeroed but before force was applied from 0 to 8.3 seconds (red). Relative minimum at 10.4 seconds, large decrease in force from 14.3 to 14.5 seconds.
VARIABLES
The primary outcome was the mean peak force required to penetrate through fascia for entry into the abdominal cavity to establish pneumoperitoneum with the Veress needle. Secondary outcome variables included age, BMI, smoking, past surgical history, location of entry (umbilicus or Palmer’s point), intra-operative complications, and time required to obtain Veress needle entry.
STATISTICAL METHODS
Analysis of Variance (ANOVA) was used to test for differences in mean peak force required to by age, BMI, number of prior abdominal surgery, and smoking history. A two-tailed t-test assuming equal variance was used to test for difference in mean peak force between subjects with entry at umbilicus and entry at Palmer’s Point.
Results
PARTICIPANTS
This study consented 22 patients undergoing laparoscopic gynecologic surgery. The patients were predominantly white (86.4%) with three Hispanic patients (13.6%). The sample had no underweight patients, five normal weight patients (22.7%), six overweight patients (27.3%), and eleven obese patients (50.0%). The sample was composed of three current smokers (13.6%), eleven former smokers (50.0%), and eight non-smokers (36.4%) (Table 1). There were no complications with the Veress needle and no intra-operative complications for the enrolled patients.
Table 1. Descriptive statistics for prospective, observational study of peak force required to gain entry to the abdominal cavity using a Veress needle in patients undergoing scheduled laparoscopic surgery at Danbury Hospital, CT, 2019–2020. (n = 22)
| Variable | Count (%) |
|---|---|
| Age | 45 – 54 years (n = 4) (18.2%) |
| 56 – 67 years (n = 7) (31.8%) | |
| ≥ 68 years (n = 11) (50%) | |
| BMI | Normal (18.5 – 24.9) (n = 5) (22.7%) |
| Overweight (25 – 29.9) (n = 6) (27.3%) | |
| Obese (≥ 30) (n = 11) (50%) | |
| Race/Ethnicity | American Indian/Alaska Native (n = 0) (0%) |
| Asian (n = 0) (0%) | |
| Native Hawaiian/Pacific Islander (n = 0) (0%) | |
| Black or African American (n = 19) (86.4%) | |
| Hispanic or Latino (n = 3) (13.6%) | |
| Smoking Status | Current Smoker (n = 0) (0%) |
| Former Smoker (n = 1) (4.5%) | |
| Never Smoker (n = 21) (95.5%) |
TRENDS IN PEAK FORCE
Two large outliers were excluded from the analyzed data set (peak forces: 2489, 2034). Among the included participants, the mean peak force required to gain entry to the abdominal cavity was 1007 gf (n = 22, SD = 298). Force data varied widely within samples with a range of 1083 gf (min = 409, max = 1493) (figure 3). Mean time required to gain entry was 5.6 seconds (SD = 3.1). There were no statistically significant differences in mean peak force by age (p = 0.327), BMI (p = 0.650), number of prior abdominal surgery (p = 0.142), smoking history (p = 0.287), and entry location (p = 0.870) (table 2).
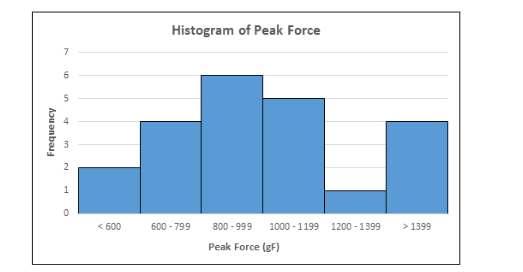
Table 2. Inferential statistics for prospective, observational study of peak force required to gain entry to the abdominal cavity using a Veress needle in patients undergoing scheduled laparoscopic surgery at Danbury Hospital, CT, 2019-2020. (n = 22)
| Variable | Mean Peak Force (SD) | p-value |
|---|---|---|
| Age | 0.327ᵃ | |
| ≤ 43 years | 963.20 (465.88) | |
| 44 – 55 years | 1252.13 (238.57) | |
| 56 – 67 years | 908.37 (176.31) | |
| ≥ 68 years | 993.20 (299.44) | |
| Body Mass Index | 0.650ᵃ | |
| Normal (18.6 – 24.9) | 1088.50 (227.7) | |
| Overweight (25 – 29.9) | 1050.24 (414.15) | |
| Obese (> 30) | 948.04 (267.61) | |
| Smoking History | 0.287ᵃ | |
| Current Smoker | 1179.77 (269.49) | |
| Former Smoker | 1076.53 (344.95) | |
| Never Smoker | 910.98 (256.12) | |
| Number of Prior Abdominal Surgeries | 0.142ᵃ | |
| 0 Past Abdominal Surgeries | 1088.82 (259.88) | |
| 1 Past Abdominal Surgery | 886.31 (292.80) | |
| ≥ 2 Past Abdominal Surgeries | 1178.00 (283.84) | |
| Veress Needle Entry Site | 0.870ᵇ | |
| Umbilicus | 1016.82 (316.00) | |
| Left Upper Quadrant (Palmer’s Point) | 994.85 (287.87) |
ᵃANOVA
ᵇTwo-tailed t-test assuming equal variance
Discussion
Competency with abdominal entry using the Veress needle is an important surgical skill due to the increased prevalence of laparoscopic surgery and the need for surgeon expertise in this technique. Most complications that occur from Veress needle use are likely related to excess force and/or excess time applying force with Veress needle to obtain abdominal entry⁷,¹⁰,¹¹. Our analysis suggests that peak force required to obtain abdominal entry is both highly varied and difficult to predict using patient characteristics.
There are several limitations to our study that should be noted. First, this was a pilot study, and therefore the sample size was small and may not be generalizable. Inferences should only be made in the context of the sample characteristics. Additionally, due to a small sample size, our analyses may have been underpowered to identify differences in mean peak force between patient groups.
However, the use of force data can lay the foundation for the development of a simulation program in which training surgeons can practice. The key to creating a successful training program would be the identification of a surface material which requires a similar mean and variance in peak force to be punctured with a Veress needle. The surgical trainee would attempt to puncture the surface material with the Veress needle without contacting a fragile object below (e.g. a water balloon). In the future, we will use these results to create a simulation program. As potential simulation programs can increase residence surgical skills and would allow new surgeons to become familiar with the technique required to safely gain abdominal entry with a Veress needle.
Conflict of Interest:
The authors have no conflicts of interest to disclose.
Disclosures:
The authors have no conflicts of interest to disclose.
Sources Of Funding:
There was no funding obtained for this study.
Date and Number of IRB:
4/25/2019 – Protocol Number: 15-02-389-337(c15)
Acknowledgements:
We would like to acknowledge the faculty and staff in the Department of Obstetrics and Gynecology and the staff in the Operating Room at Danbury Hospital. We would like to acknowledge Dr. Jim Yu and Dr. Mai-Lihn Vu for their help with this project. Also we would like to acknowledge Rakhee Agarwal for her review of the manuscript.
Data Availability Statement:
The datasets generated during and/or analyzed during the current study are available in the institutional database and not publicly available.
Statement Prior Presentation:
This research was not presented prior.
Precis
The variability of Veress needle insertion force supports the need for residents to be trained through gynecological simulation for a large range of possible forces.
References
1. Cleary SP. Minimally Invasive Liver Surgery: Has it Achieved the Standard of Care? Ann Surg Oncol. 2018 May;25(5):1105-1107. doi: 10.1245/s10434-018-6380-2. Epub 2018 Feb 21. PMID: 29468605.
2. Vilos GA, Ternamian A, Dempster J, Laberge PY. Laparoscopic entry: A review of techniques, technologies, and complications. J Obstet Gynaecol Can. 2007; 29:433.
3. Alkatout I. Complications of Laparoscopy in Connection with Entry Techniques. J Gynecol Surg. 2017;33(3):81-91.
4. Vilos G. The ABCs of a safer laparoscopic entry. J Minim Invasive Gynecol. 2006; 13(3): 249-51.
5. Ahmad G, Baker J, Finnerty J, Phillips K, Watson A. Laparoscopic entry techniques (Review). Cochrane Database of Systemic Reviews. 2019;1: 1-142.
6. Ahlborg L, Hedman L, Nisell H, Felländer-Tsai L, Enochsson L. Simulator training and non-technical factors improve laparoscopic performance among OBGYN trainees. Acta Obstet Gynecol Scand. 2013; 92:1194-1201.
7. Larsen C, Soerensen J, Grantcharov T, et al. Effect of virtual reality training on laparoscopic surgery: randomized controlled trial. BMJ. 2009; 338:b1802.
8. Kerbage Y, Rouiles J, Estrade JP, et al. Surgical training through simulation dedicated to French Ob-gyn residents. Evaluation and satisfaction. J Gynecol Obstet Hum Reprod. 2021; 50: 102076.
9. Dunne N, Booth MI, Dehn TC. Establishing pneumoperitoneum: Verres or Hasson? The debate continues. Ann R Coll Surg Engl. 2011;93(1) :22-24. doi:10.1308/003588411X12851639107557
10. Taye MK, Fazal SA, Pegu D, Saikia D. Open Versus Closed Laparoscopy: Yet an Unresolved Controversy. J Clin Diagn Res. 2016;10(2):QC04-QC7. doi:10.7860/JCDR/2016/18049.7252
11. Moreno DG, Pereira CAM, Sant Anna RK, et al. Laparoscopic Insertion of Various Shaped Trocars in a Porcine Model. JSLS. 2019;23(2):e2019.00002. doi:10.4293/JSLS.2019.00002