

Vertebral Artery Entrapment during Cervical Rotation
A Case Report: Entrapment of the Vertebral Artery between the Skull and the First Cervical Vertebra during Head and Neck Rotation
Bertel Rune Kaale, 1; Tony McArthur 2; Kristoffer Kaale 3
- Manual therapist, PhD. Firda Fysikalsk Medisinsk Senter AS, 6823 Sandane, Norway.
- DCR. Superintendent Radiographer. Firda Fysikalsk Medisinsk Senter AS, 6823 Sandane, Norway.
- Physiotherapist, with Master of Clinical Physiotherapy. Firda Fysikalsk Medisinsk Senter AS, 6823 Sandane, Norway.
Correspondence: [email protected]
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Kaale, BR., McArthur, T., et al., 2024. A Case Report: Entrapment of the Vertebral Artery between the Skull and the First Cervical Vertebra during Head and Neck Rotation. Medical Research Archives, [online] 12(11). https://doi.org/10.18103/mra.v12i11.5940
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.5940
ISSN: 2375-1924
Abstract
Introduction: Entrapment of the Vertebral Artery between the skull and the first cervical vertebra during head and neck rotation may be difficult to assess, much less quantify. Prior investigations have demonstrated that a dynamic axial Computer Tomography scan, while the patient maximally rotates the head right and left, can be used to evaluate and quantify the amount of residual overlap between the inferior articulating facet of the first cervical vertebra and the superior facet of the second vertebra, as an index of ligamentous laxity at the joint. In the present Case Report, we assessed the possibility of entrapment of the Vertebral Artery between the skull and the bow of the first cervical vertebra during hyper-rotation of the cervical spine. By combining the results from a dynamic axial Computer Tomography scan of the upper cervical spine with an Angiography, the results enabled the interpreter to evaluate the course of the blood vessels through and past the skeleton during cervical spine hyper-rotation.
Methods: The Angiography images were obtained with the patient scanned in specific positions on the scanning table as directed and positioned by the supervising clinician. 3D Volumetric Angiography scans were reviewed using RadiAntViewer software using both 3D and cross-sectional imaging techniques.
Result: This Case Report demonstrated a unilateral compression of the Vertebral Artery, left side with the head and neck in right rotation, estimated to 47 % of the total lumen. In neutral position, the lumen of the Vertebral Arteries, right and left side, were completely open.
Discussion: This result suggests a potential point of mechanical stress where the skull could be impinging on nearby structures, possibly affecting neurological and/or vascular components. The findings from these images suggest a relationship between cervical spine movement and potential vascular complications. The described compression appears to be related to over-rotation of the first cervical vertebra along with hyperextension of the skull.
Conclusion: This case report highlights the relationship between upper cervical spine biomechanics and vertebral artery compression, showing that combined rotation and extension can lead to unphysiological compression between the skull and first vertebra. It underscores the value of positional cervical spine CT and CTA as useful tools for diagnosing potential vertebral artery compression.
Keywords: Dynamic cervical CT scan; Dynamic cervical CT Angiography; Vertebral Artery compression; atlas-axis rotational test (A-ART); upper cervical spine instability.
Introduction
Neck injury with cervical spine instability can be accompanied by Vertebrobasilar pathology. Rotational vertebral artery syndrome is caused by vertebrobasilar insufficiency due to dynamic and reversible occlusion of the vertebral artery. Head and neck rotation can lead to vertebral artery compression at the atlantoaxial or sub-axial levels in the spine. As to rotational vertebral artery vertigo, the exact area of the arterial compression may be identified through appropriate methods such as Magnetic Resonance Angiography and Computed Tomography Angiography.
In October 2012, the International Federation of Orthopedic Manipulative Physical Therapists (IFOMPT) developed and approved a framework for a safer clinical assessment of the cervical spine. This framework focuses on evaluating the potential for Cervical Arterial dysfunction. Cervical spine injuries with Cervical Arterial dysfunction can be a serious condition, and it needs to be considered ahead of all cervical treatment.
The subject of this Case Report was a healthy female (NN), born in 1981. In July 2020, NN experienced a fall where she hit the low lumbar spine and the ilio-sacral joint (IS). The initial complaints were solely located to the lumbar spine/ IS joint, right side. NN sought consultation with a therapist three days later. During the initial session, she reported pain and functional deficits in the lower spine/IS area only and reported no pain or dysfunction in the thoracic or cervical spine/head regions. NN received nevertheless manipulations techniques for both the lumbar, thoracic and cervical spine. For the cervical spine, NN was treated in both prone and supine positions. No imaging was done prior to the manipulation.
NN underwent a total of five treatment sessions. Initially, there were no symptoms in the head or neck area. After the first cervical manipulation treatment, NN reported severe onset of symptoms in the neck/ head, arms and feet, together with breathing problems. Despite four additional therapist follow-up sessions, NN’s cervical/ head and extremities-symptoms worsened after each session. Eventually, NN declined further treatment. These five treatment sessions occurred over a span of 20 days in 2020.
Status January 2024: NN experienced the deep burning pain to both legs and arms had become chronic. The pain in the neck and the dizziness had worsened over the years from 2020 to 2024. Rotation of the head and neck aggravated the symptoms, especially rotation to the right side. With rotation right, NN experienced a strong pulsation left side in the upper cervical spine, which lead to pressure like pain in the head with blurry vision.
NN had been through Magnetic Resonance Imaging (MRI) scan of the cervical spine, with head and neck in neutral position, 3 times from 2020 to 2023. All 3 MRI scans showed normal findings. A computer tomography (CT) scan in 2023 showed a spina bifida of the first cervical vertebra (C1).
Clinical examination in 2023 revealed pathological hyper-rotation between the first and second cervical vertebra (C1-C2) right/ left side. Clinical tests with the head and neck in right/ left rotated positions aggravated the neck pain and the dizziness. A new dynamic cervical MRI was requested (January 2024), with the head and neck in both neutral and right/ left rotated positions.
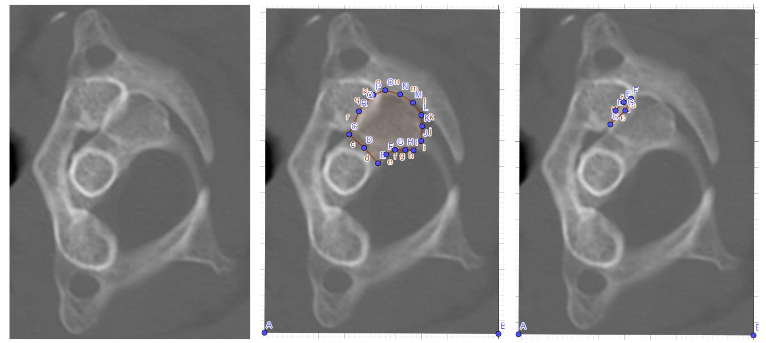
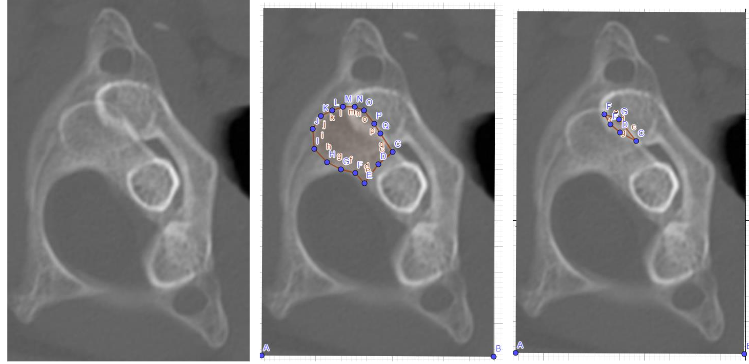
The results showed a C1-C2 hyper-rotation close to subluxation, with C1-C2 facets rest-coverage right side 4% and left side 8% (Figures 1,2). Normal C1-C2 facets rest-coverage during rotation C1-C2 has in 2 previous scientific works been estimated to be 30%.
The aim of this study was to investigate whether increased rotation in the upper cervical spine could lead to compression of the Vertebral Artery. To further elucidate this potential cause of NN’s symptoms, especially considering the vascular considerations associated with C1-C2 instability, a Computer Tomography Angiography (CTA) was requested.
Methods
NN was placed on the CT table with head and neck both in neutral, and in maximal right/ left rotation. The neutral head and neck position gave no stress on the soft tissue/ vessels in the neck. With rotated head and neck positions, the soft tissue and vessels were put under stress.
The CT Angiography (CTA) scans were obtained from above the base of the skull to T1/T2. The CT images were generated on a Toshiba (Canon Healthcare Aquilion Prism) CT scanner; typical parameters were 100 kVp and 50 mAs with a 0.5-sec scan rotation time. Bone, soft tissue and CTA image filter convolutions (FC) were used, and the patients were scanned without gantry angulation. The scans were a helical acquisition of 0.5mm x 80 slices with a pitch of 0.8 and reconstructed as 0.5 mm axial slices every 0.25mm.
| CT Angiography injection protocol |
|---|
| 80mls of Omnipaque 350 intravenous contrast medium injected at 5ml/s, bolus tracked on the pulmonary trunk. |
CTA images were obtained with the patient scanned in specific positions on the scanning table as directed and positioned by the supervising clinician. 3D Volumetric CT scans were reviewed using RadiAntViewer software using both 3D and cross-sectional imaging techniques.
| Volumetric CTA Protocol | Parameters- Dedicated Volumetric CTA Cervical Spine |
|---|---|
| Anatomic coverage | Above foramen magnum to T2 |
| Collimation (mm)* | 0.5; Rotation time (sec) 0.4 |
| Exposure factors | 100 kV 50 MAs Automatic modulation |
| Table Pitch | 0.8 |
| Imaging and reconstruction planes | Axial mm (0.5/0.25); coronal and sagittal mm (2.0); three-dimensional volume mm (0.50). |
Results
With the cervical spine/ head in neutral position, the results from the CT Angiography showed no pathological changes in/with the blood vessels in the cervical spine or in the lower part of the skull. However, when the head and neck were rotated to the right side, the scan revealed entrapment of the left Vertebral Artery. With the head and neck in left rotation, there was no evidence of entrapment of the right Vertebral Artery.
To compare the cross-sectional area of the artery in its neutral and rotated positions, we applied the formula for the area of a circle: Area = π * r². Where π is the constant value 3.14 and r is the radius, which we find by dividing the diameter in two. While the artery is circular in the neutral position, we recognize that it became distorted during compression. However, for comparison purposes, we still used the circular formula in both cases. We used the shortest diameter from Figures 3 and 4, which were 3.23 mm in Figure 3 and 2.22 mm in Figure 4, respectively.
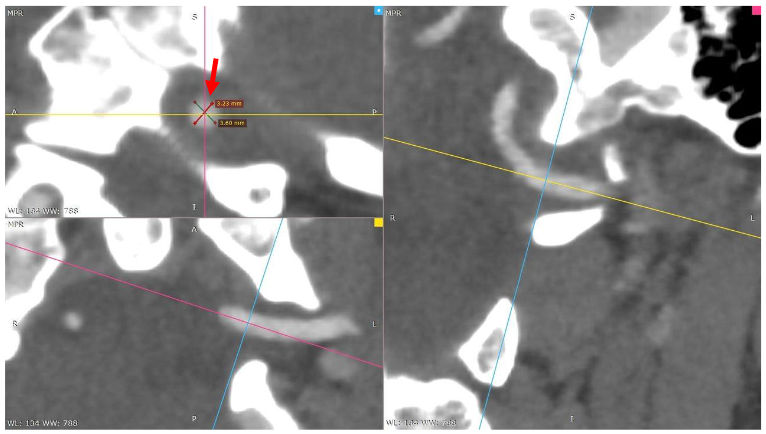
Diameter (D) = 3.23 mm
Radius (r) = D/2 = 3.23/2 = 1.615 mm
Area (A) = π * (1.615)² = 8.152 mm²
Multi-planar reconstructions of the left vertebral artery (neutral position) show no vessel luminal compression. Red arrow.
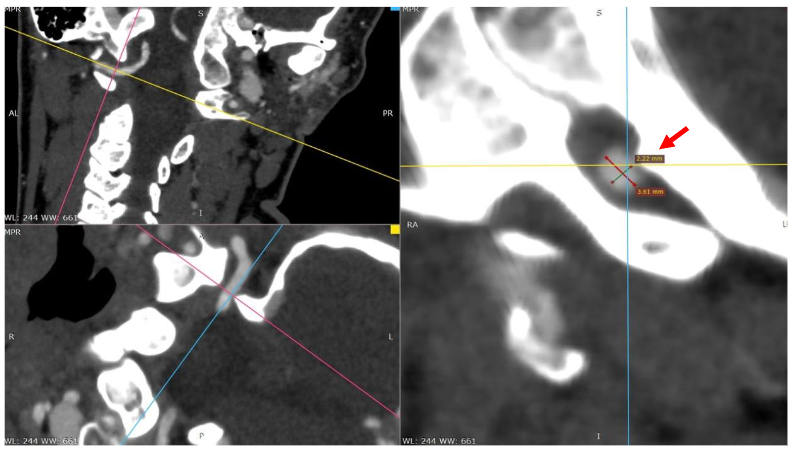
Diameter (D) = 2.22 mm
Radius (r) = D/2 = 2.22/2 = 1.11 mm
Area (A) = π * (1.11)² = 3.877 mm²
Multi-planar reconstructions of the left vertebral artery show vessel luminal narrowing due to bony compression superiorly from the base of the skull.
AREA REDUCTION CALCULATION
The area reduction is calculated as:
Reduction Ratio = A in rotation / A in neutral * 100 = 3.877 / 8.152 * 100 = 47.6%
| Summary | Diameter (mm) | Radius (mm) | Area (mm²) | Area reduction (%) |
|---|---|---|---|---|
| Neutral | 3.23 | 1.615 | 8.15 | 0% |
| Compressed (Rotated) | 2.22 | 1.11 | 3.88 | 47.6% |
This analysis indicates that the lumen area of the left Vertebral Artery observed in right rotated head- and neck position is 47 percent less than with the head- and neck in neutral position, which implies a considerable narrowing of the artery when positioned in the rotated position (Table 2). It is important to note that the morphology of the narrowed artery is not strictly circular; rather, it may exhibit an elliptical or irregular shape owing to the deformations and pressure variances that occur during the rotation process.
Discussion
This Case Report demonstrates a deviation from the normal biomechanics in the upper cervical spine, with a hyper-rotation of the C1-C2. The facets are close to luxation, where only the cortical rim of both C1 and C2 make the rest-facets contact area. This C1-C2 facets deviation fits into the Fielding and Hawkins’s classification system, as Type 2 rotational instability. The biconvex nature of the C1-C2 joint during rotation, makes the C0-1-2 complex drop, facilitate the flexion and extension of the skull down on the C1 segment. This Case had a C1-C2 facets rotational rest-coverage of 4% and 8%, which may be explained by weakened soft tissue structure due to a spina bifida C1 in combination with soft tissue injury after multiple cervical manipulations with negative outcome. The ligament laxity enhances the range of motion for C1-C2 in rotation and C0-C1 in extension, making a bone knot on the skull compress the Vertebral Artery un-physiological against the bow of C1.
The combination of the right rotation of the C1 vertebra and hyperextension of the skull onto the C1 vertebra, resulted in an abnormal compressive site for the left Vertebral Artery.
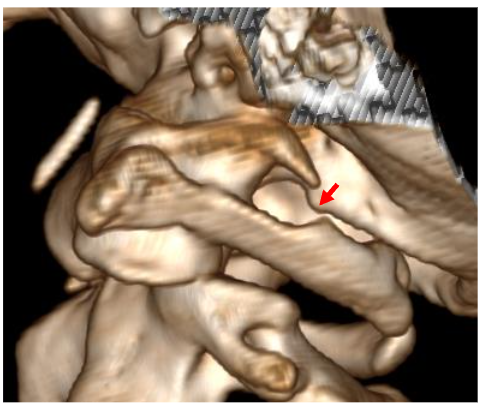
This image shows a 3D CT reconstruction with a focus on the craniovertebral junction and the relationship between the skull (C0) and the first cervical vertebra (C1). Result: The red arrow indicates that the skull has moved anteriorly and downward against the left side of C1 and created a compression site. This suggests a potential point of mechanical stress where the skull could be impinged on nearby structures, possibly affecting neurological or vascular components.
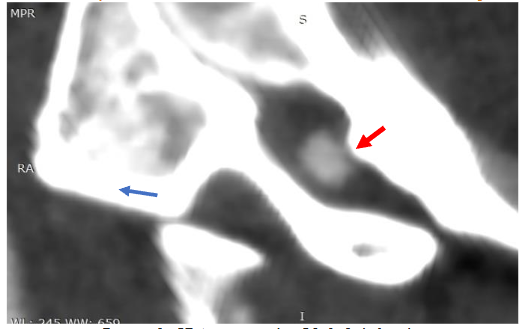
Like Figure 5, it shows the same right-side rotation of C1 on C2. Result: The blue arrow illustrates the direction of C1’s rotation on C2. The red arrow signifies where the movement of the skull impacts the left Vertebral Artery. This likely indicates that the hyper-rotation of C1-C2 can lead to vascular compromise, where the artery is compressed between bony structures of the skull-C1.

The CT Angiography findings indicate a significant bony nodule on the skull at the compression site, where it exerts pressure against the anterior aspect of the C1 vertebra (red arrow). This compression affects the left Vertebral Artery, which can impede blood flow and potentially lead to vascular complications.
Different pathological changes to the Vertebral Artery are well described in the literature. This Case Report shows that C0-1-2 instability may create a compression site between two bony structures of skull and the bow of the first vertebra. It is reasonable to believe that NN’s dizziness, head pressure and blurred vision may have its origin from intermittent Vertebral Artery compression. These symptoms are provoked every time NN rotates the head and neck to the right side. This intermittent stenosis or occlusion of the artery may be the reason for NN’s feeling of pulsatility, which may be explained by the difference in the systolic and diastolic velocities in the circulation of the blood. Repeated artery compression with occlusion may act as morphological risk factor for wall dissection. Vascular compression syndromes are characterized by external compression of primarily healthy arteries and/or veins as well as accompanying nervous structures, carrying the risk of subsequent structural vessel wall and nerve damage. NN reported frequently posterior headache and neck pain, with blurred vision. Such clinical manifestations should lead to a follow up regarding possible trans-ischemic attacks (TIA) and artery dissections.
This Case had 3 times cervical MRI scan, with no abnormal findings. The spina bifida C1 was overlooked the first 2 times, before a CT scan was done in between the 2nd and 3rd MRI scan. The lack of findings regarding the extent of dynamic C1-C2 rotation is understandable, since only MRI sequences with neutral head- and neck-positions were performed.
This Case Report emphasizes and puts the spotlight on the clinical and radiological methodology. The clinical and radiological understanding has developed over time from static cervical CT and MRI scan with neutral head- and neck positions, to a more dynamic radiological approach.
Conclusion
This case report demonstrates a link between alterations in upper cervical spine biomechanics and direct bony compression of the vertebral artery. It highlights how combined rotation and extension of the upper cervical spine can lead to unphysiological compression of the vertebral artery between the skull and the first vertebra. Furthermore, the findings emphasize the importance of positional cervical spine CT and CTA as useful diagnostic tools for identifying potential vertebral artery compression.
Conflicts of interest statement: The authors have no conflicts of interest to declare.
Funding Statement: The project has had no external fundings.
Acknowledgement: None.
References
- Baumann A, Trager RJ, Curtis D, Chen M, Baldwin K. Screening for Vertebrobasilar pathology and upper cervical instability by physical therapists treating neck pain: a retrospective chart review. J Man Manip Ther. Oct 2023;31(5):376-382. doi:10.1080/10669817.2023.2192998
- Hayes P, Gerlock AJ, Jr., Cobb CA. Cervical spine trauma: a cause of vertebral artery injury. J Trauma. Oct 1980;20(10):904-5. doi:10.1097/00005373-198010000-00018
- Li Y, Peng B. Pathogenesis, Diagnosis, and Treatment of Cervical Vertigo. Pain Physician. Jul-Aug 2015;18(4):E583-95.
- Hara H, Nagashima H, Koike G, Sakai K, Kobayashi S. Unusual spontaneous entrapment of a dissecting aneurysm of the vertebral artery–case report. Neurol Med Chir (Tokyo). Apr 1991;31(4):206-9. doi:10.2176/nmc.31.206
- Yamamoto S, Toyota S, Nakamura H, Mori K, Taki T, Yoshimine T. Traumatic Entrapment of the Vertebral Artery Demonstrated by a 3D Angiographic Study. World Neurosurg. Nov 2016;95:623.e5-623.e9. doi:10.1016/j.wneu.2016.06.067
- Davis DD, Munakomi S, Kane SM. Rotation Vertebral Artery Syndrome. StatPearls. StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC.; 2024.
- Wang Y, Jiao H, Peng H, Liu J, Ma L, Wang J. Study of Vertebral Artery Dissection by Ultrasound Superb Microvascular Imaging Based on Deep Neural Network Model. J Healthc Eng. 2022;2022:9713899. doi:10.1155/2022/9713899
- Rushton A, Rivett D, Carlesso L, Flynn T, Hing W, Kerry R. International framework for examination of the cervical region for potential of Cervical Arterial Dysfunction prior to Orthopaedic Manual Therapy intervention. Man Ther. Jun 2014;19(3):222-8. doi:10.1016/j.math.2013.11.005
- Scholten-Peeters GG, van Trijffel E, Hutting N, Castien RF, Rooker S, Verhagen AP. Risk reduction of serious complications from manual therapy: are we reducing the risk?: correspondence to: International framework for examination of the cervical region for potential of cervical arterial dysfunction prior to orthopaedic manual therapy intervention by A. Rushton et al. Man Ther. Dec 2014;19(6):e5-6. doi:10.1016/j.math.2014.01.007
- Kaale BR, McArthur TJ, Barbosa MH, Freeman MD. Post-Traumatic Atlanto-Axial Instability: A Combined Clinical and Radiological Approach for the Diagnosis of Pathological Rotational Movement in the Upper Cervical Spine. J Clin Med. Feb 12 2023;12(4) doi:10.3390/jcm12041469
- Mönckeberg JE, Tomé CV, Matías A, Alonso A, Vásquez J, Zubieta JL. CT scan study of atlantoaxial rotatory mobility in asymptomatic adult subjects: a basis for better understanding C1-C2 rotatory fixation and subluxation. Spine. May 20 2009;34(12):1292-5. doi:10.1097/BRS.0b013e3181a4e4e9
- Fielding JW, Hawkins RJ. Atlanto-axial rotatory fixation. (Fixed rotatory subluxation of the atlanto-axial joint). J Bone Joint Surg Am. Jan 1977;59(1):37-44.
- Scapinelli R. Three-dimensional computed tomography in infantile atlantoaxial rotatory fixation. J Bone Joint Surg Br. May 1994;76(3):367-70.
- Roche CJ, O’Malley M, Dorgan JC, Carty HM. A pictorial review of atlanto-axial rotatory fixation: key points for the radiologist. Clin Radiol. Dec 2001;56(12):947-58. doi:10.1053/crad.2001.0679
- Swartz EE, Floyd RT, Cendoma M. Cervical spine functional anatomy and the biomechanics of injury due to compressive loading. J Athl Train. Jul-Sep 2005;40(3):155-61.
- Takekawa H, Tsukui D, Kobayasi S, Suzuki K, Hamaguchi H. Ultrasound diagnosis of carotid artery stenosis and occlusion. J Med Ultrason (2001). Oct 2022;49(4):675-687. doi:10.1007/s10396-022-01259-7
- Han J, Chen J, Tong X, et al. Morphological characteristics associated with ruptured intracranial vertebral artery dissecting aneurysms. J Neurointerv Surg. Apr 2023;15(4):321-324. doi:10.1136/neurintsurg-2022-018744
- Czihal M, Banafsche R, Hoffmann U, Koeppel T. Vascular compression syndromes. Vasa. Nov 2015;44(6):419-34. doi:10.1024/0301-1526/a000465
- Arnold M, Bousser M. Clinical manifestations of vertebral artery dissection. Front Neurol Neurosci. 2005;20:77-86. doi:10.1159/000088152
- Kaale BR, Krakenes J, Albrektsen G, Wester K. Clinical assessment techniques for detecting ligament and membrane injuries in the upper cervical spine region–a comparison with MRI results. Man Ther. Oct 2008;13(5):397-403. doi:10.1016/j.math.2007.03.007
- Kaale BR, Krakenes J, Albrektsen G, Wester K. Active range of motion as an indicator for ligament and membrane lesions in the upper cervical spine after a whiplash trauma. J Neurotrauma. Apr 2007;24(4):713-21. doi:10.1089/neu.2006.0193
- Krakenes J, Kaale BR. Magnetic resonance imaging assessment of craniovertebral ligaments and membranes after whiplash trauma. Spine. Nov 15 2006;31(24):2820-6. doi:10.1097/01.brs.0000245871.15696.1f
- Vetti N, Kråkenes J, Damsgaard E, Rørvik J, Gilhus NE, Espeland A. Magnetic resonance imaging of the alar and transverse ligaments in acute whiplash-associated disorders 1 and 2: a cross-sectional controlled study. Spine. Mar 15 2011;36(6):E434-40. doi:10.1097/BRS.0b013e3181da21a9