





Fascial Dextrose Injections for Referred Back Pain Treatment
Treatment of Referred Back Pain using Fascial Dextrose 5% Injections: A Case Report
J Kersschot LF Marques A Hajji R Baalbaki
OPEN ACCESS
PUBLISHED: 31 May 2025
CITATION: KERSSCHOT, J et al. Treatment of Referred Back Pain using Fascial Dextrose 5% Injections: A Case Report. Medical Research Archives, [S.l.], v. 13, n. 5, may 2025.Available at: <https://esmed.org/MRA/mra/article/view/6560>.
DOI: https://doi.org/10.18103/mra.v13i5.6560
ISSN 2375-1924.
Abstract
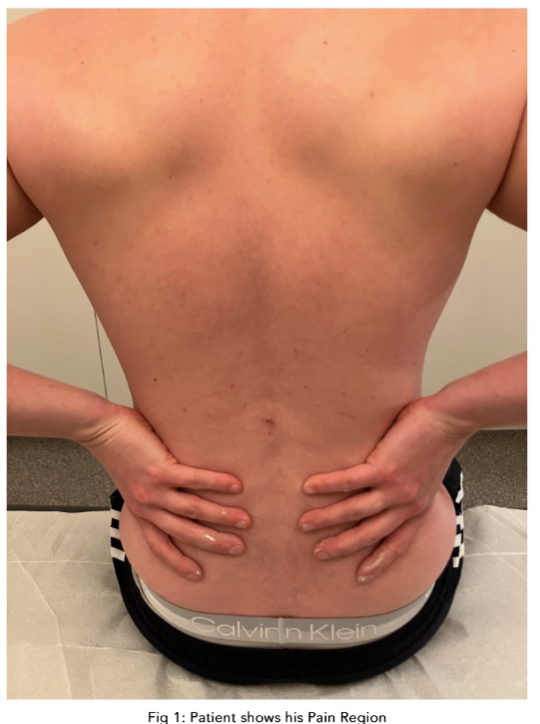
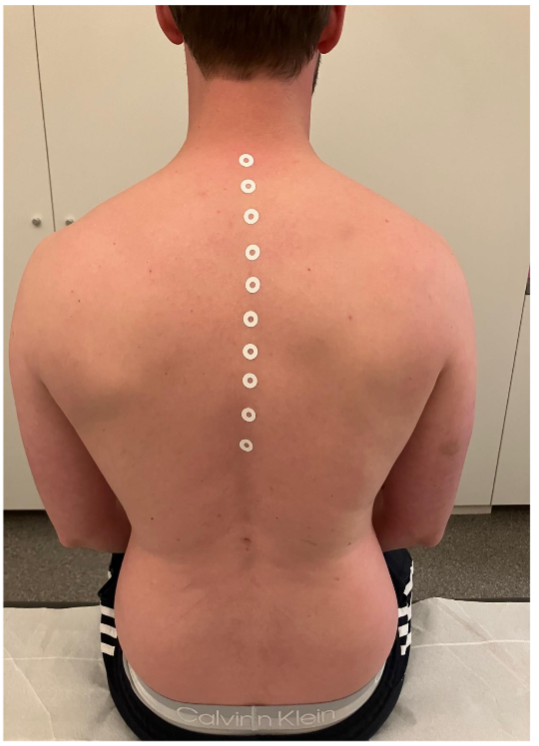
The fascial system (FS) is a complex network of connective tissue throughout the human body, encompassing both superficial and deep layers. Regional fascial dysfunctions can lead to pain, trauma, stress and other issues. Fascial dysfunction has been associated with both diminished range of motion as well as regional pain. Unfortunately, such injuries are often misdiagnosed, leading to ineffective treatment. This case report describes the use of 5% dextrose injections to treat referred back pain originating from the subcutaneous fascia. The patient, a 30-year-old female, presented with pain in her right lower back that radiated to her right hip. It was hypothesized that her pain might be referred from the subcutaneous fascia. She received a total of 10 injections. To test this hypothesis, a follow-up was conducted 6 months after the injections. The patient reported a significant decrease in pain levels and improved mobility. This case report highlights the potential benefits of using fascial injections in treating referred pain.
Keywords: fascial system, referred pain, dextrose injections, case report, back pain
Introduction
The fascial system (FS) is a complex network of connective tissue surrounding muscles and organs; it is in fact a three-dimensional network connecting dermis, muscles, vessels and organs into one integrative system. Fascia contains a lot of nociceptors as well and as a result it is hypothesized that the FS may lead to musculoskeletal pain which does not match the diagnosis based on MRI or ultrasound. Dealing with such musculoskeletal pain syndromes can be challenging for both primary physicians and pain specialists.
The Potential Role of the Interstitium
More recently a “new organ” was described, the so-called interstitium. This interstitium contains the ECM but is much larger and wider than the ECM. The interstitium is sometimes described as an underground network of fluid-filled channels. This space between cells and fibrous tissues is tissue filled with both interstitial fluid and ECM. This interstitial space is found in the dermis and fibrous connective tissues throughout the entire body. It does not matter if the injectate can “penetrate” to adjacent regions. More research is definitely required to clarify the potential role of interstitial DSW injections at a cellular level.
Difference Between Glucocupuncture and Perineural Injection Therapy
Difference between glucocupuncture and perineural injection therapy (PITT) involves landmark-based injections of dextrose 5% along superficial peripheral nerves. These injections are all administered subcutaneously, which allows deeper structures, such as joints. In contrast to PITT, GP is also applied for chronic functional problems outside the field of MSK pain by injecting in the subcutaneous fascia in the pain region. PITT is directed to Lyboty typically applied buffered dextrose (pH 7.2) by adding bicarbonate to the DSW. The latter is not used to the injectate in GP.
Difference Between Glucocupuncture and Neuraltherapy
Neuraltherapy (NT) is a therapeutic technique which involves landmark-based injections of procaine 1% along peripheral nerves and autonomic ganglia. The main goal of NT is to regulate the autonomic nervous system (e.g., stellate ganglion). One also injects into the region of complaints (segmental therapy), into joint cavities and into interference fields (e.g., scars). GP typically injects locally for regional pain modulation, while NT is considered as an holistic treatment because it takes into account the whole system.
Conclusion
In the last decade, physicians came to see that the fascia is a system that connects different parts of the body like an invisible three-dimensional web. As such, it is hypothesized that chronic low back pain can be referred from one region to another. Recently, it has been postulated that acupuncture can regulate pain originating from subcutaneous fascia lesions. This technique may be important in patients with regional pain who show no pathological signs on MRI or ultrasound. The superficial fascia may also explain referred pain which does not correspond with myofascial trigger points, bulging discs, fast joint degeneration nor peripheral nerve patterns. It is still not completely clear how pain is transmitted through the fascia and there are still a lot of unanswered questions regarding this system and interstitium. We realize that there are still a lot of unanswered questions regarding this system and interstitium.
Statement of Informed Consent:
Informed consent was obtained from the participant included in this case study.
References
- Stecco C, Macchi V, Porzionato A, De Caro F, De Caro R. The fascia: the forgotten structure. Ital J Anat Embryol. 2011;116(3):127-38.
- Exeter D, Connell DA. Skeletal muscle: functional anatomy and pathophysiology. Semin Musculoskelet Radiol. 2010 Jun;14(2):107-15.
- Pandey N, Nayak P, Gahoiya A. A Randomized Control Trial on Efficacy of Aqueous Effect of 5% Dextrose Caudal Epidural Injection for Non-specific Low Back Pain. International Journal of Scientific Research, 2020, 9 (1): 11-13.
- Smigel LV, Reeves KD, Lyfotgt J, Rabago DP. Perineural Injection Therapy: A Systematic Review and Meta-Analysis. Dovepress. 2017;11:1837.
- Karsdorp P, van der Windt DA, Faber R, Faleh B, Azami A. Neurofascial Dextrose Prolotherapy for Managing Chronic Ankle Ligament Injury. Anesth Pain Med. 2022 Jan;32(1):e18137.
- Kim H, Kim H, Jung YH, Do W, Kim EU. The effect of perineural injection therapy on neuropathic pain: a retrospective study. J Dent Anesth Pain Med. 2024 Feb;24(1):45-62. doi: 10.17245/jdap.2024.24.1.45.
“`