





Graves’ Disease Presenting as Spontaneous Intracranial Hypotension
Spontaneous Intracranial Hypotension Can be the Presenting Manifestation of Grave’s Disease: A Case Report
1Pournamy Sarathchandran, 2 Ajithkumar BV, 3 Muna Lootah, 3 Hamdan Al Zarooni, 4 Shaikh Syed Iqbal
- Department of Endocrinology, Al Qassimi hospital, Sharjah
- Department of Neurology, Rashid Hospital, Dubai
- Department of Radiology, Rashid hospital
OPEN ACCESS
PUBLISHED:31 March 2025
CITATION Sarathchandran, P., BV, Ajithkumar., et al., 2025. Spontaneous Intracranial Hypotension Can be the Presenting Manifestation of Grave’s Disease: A Case Report. Medical Research Archives, [online] 13(3). https://doi.org/10.18103/mra.v13i3.6378
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i3.6378
ISSN 2375-1924
ABSTRACT
Introduction: Autoimmune thyroid disorders are known to cause various neurological manifestations; however spontaneous intracranial hypotension (SIH) is an extremely rare association and to the best of our knowledge this is the first report describing SIH to be presenting manifestation of Graves’ disease.
Case presentation: We report the case of a middle-aged lady who presented with spontaneous intracranial hypotension secondary to Graves’ disease. A 43-year-old Arab lady presented with subacute onset orthostatic headache, vomiting and dizziness followed by blurring of vision and diplopia.
Investigations and outcome: Brain and spine imaging was suggestive of spontaneous intracranial hypotension. Lab investigations revealed hyperthyroidism with elevated anti TSH (thyroid stimulating hormone) receptor antibodies confirming diagnosis of Graves’ disease. She was managed conservatively for the orthostatic headache and was started on anti-thyroid medications. She was asymptomatic at 3 months follow up.
Conclusion: Thyroid disorders should be looked for in patients presenting with intracranial hypotension since correcting the underlying thyroid dysfunction may help correcting the intracranial pressure changes thus preventing recurrence of headache.
Keywords:
- Graves’ disease
- orthostatic headache
- Spontaneous intracranial hypotension
- antithyroid medications
Introduction
Spontaneous intracranial hypotension (SIH) usually presents with orthostatic headache due to low CSF pressure and is usually attributed to spinal cerebrospinal fluid (CSF) leaks. It is clinically characterized by an acute or gradual onset of severe orthostatic headache, which is relieved with supine position. It can be associated with diplopia, tinnitus, photophobia, nausea, vomiting, vertigo, neck stiffness, local back pain, facial numbness or weakness. Rare clinical features include poor memory, parkinsonism, chorea, cerebellar ataxia, change in personality, and galactorrhoea.
Thyroid hormones have a crucial role in many aspects of nervous system activities including cognitive development. The mechanisms of actions postulated are direct interaction with intrinsic regulatory circuits or indirectly by systemic effects exerted on the circulatory system or metabolic pathways. Hence, disturbances of thyrometabolic state results in a spectrum of neurological signs and symptoms including mood and cognitive disorders, headache, ophthalmoplegia, tremor and other movement disorders, muscle weakness etc. Both hyper- and hypothyroidism may cause psychiatric symptoms like depressive or anxiety disorder, memory deficits, executive inability and even psychosis.
Hyperthyroidism and hypothyroidism had been linked to intracranial pressure changes. although the exact mechanism is not known Auto immune thyroid diseases including Grave’s disease and Hashimoto’s thyroiditis has been reported to be associated with Idiopathic intracranial hypertension. Extra thyroidal manifestations of Graves’ disease include thyroid ophthalmopathy, dermopathy and acropachy. In addition, it is known to cause a myriad of neurological symptoms including tremor, proximal myopathy, and axonal neuropathy causing sensory abnormalities. Seizures, hyperkinetic disorders, dementia, and encephalopathy may occur rarely. Spontaneous intracranial hypotension has been reported in a patient with Grave’s disease. Monosymptomatic presentation of Graves’ disease as Spontaneous intracranial hypotension (SIH) is not known.
Case presentation
A 43-year-old Arab lady presented emergency department with history of acute onset headache, vomiting and dizziness of 1 week duration. She had consulted a neurologist from a private clinic and was evaluated by MRI brain, which showed bilateral subdural collections and hence was referred to the emergency for a neurosurgical evaluation. At presentation, she complained of severe headache, which had worsened after sitting for about 30 minutes associated with neck pain and improves on lying down. She also complained of left eye drooping and diplopia. She also complained of excessive sleepiness since past few weeks. There was no history of early morning headache. There was no history of palpitation, weight loss or menstrual irregularities. She denied any history of trauma, recent surgeries, fever, or any recent intake of medications other than paracetamol. She denied any strenuous exercise, sneezing, weight bearing or straining.
At presentation she was afebrile, the pulse rate was 100/min, blood pressure was 110/70mm Hg and respiratory rate was 13/min. Thyroid examination revealed mild diffuse enlargement. Chest and cardiovascular examinations were normal. Abdominal examination did not reveal any organomegaly. On neurological examination, she was conscious and oriented to time place and person. Cranial nerve examination revealed mild non-fatiguable left eye ptosis, mild right abduction restriction with horizontal diplopia on lateral gaze and mild up gaze restriction, and bilateral gaze evoked nystagmus. Pupils were bilaterally equally reactive and optic fundi were normal. There was no facial asymmetry, facial sensory loss, or any bulbar weakness. Motor system examination revealed normal tone and power with brisk reflexes and down going plantar response. There was no sensory loss and the coordination testing was normal.
Investigations
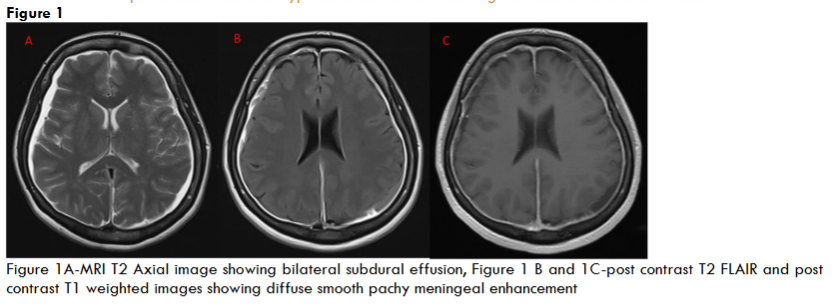
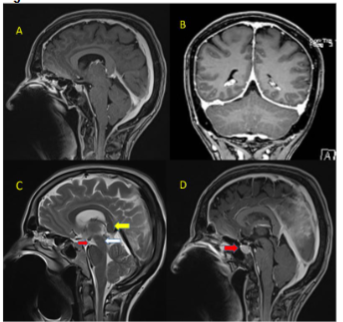
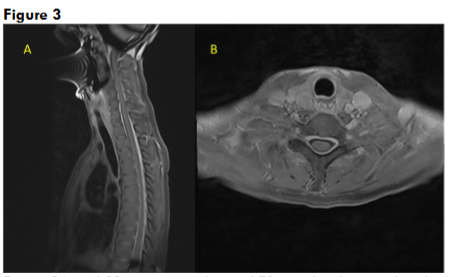
Her routine blood investigations including blood counts, liver and renal function tests were normal. Serum vitamin D and vitamin B12 levels were normal. CT brain and CT cerebral angiography was done in emergency to rule out any pituitary apoplexy, subarachnoid hemorrhage, vascular aneurysm, or vascular malformation, which was normal. Gadolinium-enhanced magnetic resonance imaging (MRI) showed bilateral subdural effusion, with diffuse smooth pachymeningeal enhancement (Figure 1). There was drooping of splenium of corpus callosum, sagging of the midbrain, reduced mammillo-pontine distance, and pituitary hyperaemia. MRI of the spine showed smooth dural enhancement of the cervical and thoracic region. No CSF leak was noted in the contrast images. MR venogram showed engorgement of the venous sinuses. The imaging findings were in countenance with SIH (Figure 2). Ultrasound of the thyroid showed mild diffuse thyroid enlargement, with mild increase in vascularity.
Treatment
She was advised strict bed rest. She was given intravenous saline for hydration. Inj. Paracetamol 1g QID was started for her headache. By next day morning her headache was significantly better and could sit upright for more than thirty minutes during her mealtimes. Thyroid function test results came in the morning. Thyroid function tests revealed hyperthyroidism, the values were as follows: serum free T3 >32.2 ng/dL (Normal-0.80-4.60 ng/dL), free T4 >7.74 ng/dL (0.93-1.70 ng/dL), thyroid-stimulating hormone <0.01 μIU/mL (0.27-4.20 μIU/mL), TSH receptor antibody 219.94 U/L (14-100 U/L), anti-thyroid microsomal antibody 600 IU/mL (≤34 IU/mL) and thyroglobulin antibody 193.1 IU/mL (≤115 IU/mL). Her case was discussed with the endocrinologist. She was initiated on Carbimazole 5mg thrice daily. In view of her persisting headache, we started her on oral Methylprednisolone 16 mg/day for five days. Her headache subsided gradually, her diplopia, drooping of lids and excessive daytime somnolence improved over time. She did not require to take any analgesic medication for more than a month. She was asymptomatic at 3 months follow up and examination revealed no focal neurological deficits. Repeat thyroid function tests after 3 months showed a TSH value of 0.3 μIU/mL.
Discussion
Spontaneous Intracranial hypotension may occur primarily are due to CSF leaks after trauma or surgery. The exact reason for primary SIH is not known but presents similarly as in cases with CSF leak. The postulated mechanisms include sagging of the brain, dilation of intracranial veins, and activation of adenosine receptors. The clinical presentation is characterized by orthostatic headache probably due to downward traction on the richly innervated dura by the sagging brain. Orthostatic headache in primary SIH usually develops gradually and ranges from mild to excruciating in severity. Orthostatic headache is a type of headache that is aggravated by standing or sitting up and disappears within a few minutes when the patient lays down. Our patient had a rather acute onset of typical orthostatic headache which was very severe, with evolution of other neurological signs including neck pain, extraocular movement palsy with right eye abduction restriction, up gaze restriction and left ptosis, gaze evoked nystagmus and hypersomnolence. These symptoms are likely related to the traction of the hypothalamus, brain stem and the cranial nerves.
Previous reports have mentioned symptoms including visual blurring, tinnitus, changes in the sense of taste, limb paresthesias, poor memory, parkinsonism, chorea, cerebellar ataxia, change in personality, and galactorrhea due to traction of hypothalamus-pituitary system and brain stem. The MRI of our patient did not show any focal lesions in the brainstem, but it showed midbrain sagging and vertically oval distortion in shape of the midbrain. Bed rest and hydration improved the neurological signs. Our patient’s lab profile showed very low TSH with raised T3 and T4. She had positive anti TSH antibodies in very high titres along with raised anti TPO and antithyroglobulin antibodies. Anti-TSH Receptor antibodies are highly specific for Grave’s disease (GD) occurring in around in 90% of affected patients. It can be present in up to 20% Hashimoto’s thyroiditis (HT), and 10–75% of atrophic thyroiditis patients. Anti TPO antibodies are detected in 90–95% of patients with auto immune thyroid disease and can be positive in up to 80% of patients with GD. Thyroglobulin antibodies are relatively nonspecific and it can be present in up to 60–80% of HT and in 50–60% of GD patients. HT is usually associated with thyroid swelling and mostly presents with hypothyroidism. The presence of Anti-TSH Receptor antibodies and hyperthyroidism confirms the diagnosis of GD in our patient.
Recommended treatment for SIH includes strict bed rest, a generous intake of liquid, caffeine, analgesia, theophylline, abdominal binding, epidural injections (including fibrin glue or homologous blood epidural blood patches) and rarely surgery. She was initiated on Methyl prednisolone 16mg TDS (gradual tapering over 2 weeks) along with Neomercazole(carbimazole) 5mg TDS and Paracetamol. The headache subsided completely over few weeks. All the associated neurological signs also recovered completely. Hyperthyroidism per se can produce ophthalmopathy but is associated with exophthalmos and not ptosis. Also, the worsening of the signs on prolonged upright posture suggested its aetiology to be SIH. Hyperthyroidism and hypothyroidism had been linked to intracranial pressure changes, although the exact mechanism is not known. Thyroxine can alter CSF dynamics as it is an important regulator of sodium transport and can affect the cerebral blood flow. This probably influences the CSF production and reabsorption. Several cases have been reported with Intracranial hypertension occurring in patients with Grave’s disease. However, the association of Graves with SIH has been reported previously in a single case only, where the authors reported SIH in a patient known to have GD for 2 years. She had achieved remission eight months back but had biochemical hyperthyroidism when she presented with features of SIH. She also had symptomatic improvement with steroids and antithyroid medications. Our patient was not known to have thyroid disease and her initial presentation was with SIH. She had orthostatic hypotension in addition to cranial nerve deficits due to the traction effect on to the midbrain by the sagging brain. Contrast enhanced MRI brain showed features suggestive of SIH and no CSF leak could be found. Strict bed rest and use of epidural blood patch to seal the CSF leakage is recommended in patients with SIH. Corticosteroid treatment and epidural saline infusion has shown to improve outcome in some. Despite the severity of symptoms, our patient had a rapid improvement with medications, and she had complete improvement with resolution of all clinical signs over few weeks. She continued carbimazole for her hyperthyroidism and she did not have any recurrence of symptoms.
Conclusion
Thyroid disorders should be looked for in patients presenting with intracranial pressure changes including Idiopathic intracranial hypertension and spontaneous intracranial hypotension. Correcting the underlying thyroid dysfunction may help correcting the intracranial pressure changes thus improving clinical symptoms and preventing recurrence of headache.
Take home messages
- Thyroid disorders should be considered in all patients presenting with orthostatic headache
- Short course oral steroids may help in rapidly alleviating in symptoms related to SIH associated with Grave’s disease and may help to avoid epidural blood patch injection or saline infusion
- Treatment of hyperthyroidism can result in complete resolution of symptoms and signs of SIH.
References
- Schievink WI, Meyer FB, Atkinson JL, Mokri B. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. J Neurosurg 1996;84:598-605.
- Headache Classification Subcommittee of the International Headache Society. Headache Classification Committee of the International Headache Society. The international classification of headache disorders, 3rd edition (beta version). Cephalalgia 2013;33:629–808.
- Mokri B. Spontaneous intracranial hypotension. Continuum (Minneap Minn) 2015;21:1086–108.
- Stasiolek: Neurological symptoms and signs in thyroid disease. Thyroid Research 2015 8(Suppl 1):A25.
- Merkenschlager A, Ehrt O, Muller-Felber W, et al. Reversible benign intracranial hypertension in a child with hyperthyroidism. J Pediatr Endocrinol Metab 2008;21:1099–101.
- Nickel SN, Frame B: Neurologic manifestations of myxedema. Neurology 1958;8:511517.
- Prendes JL, McLean WT Jr: Pseudotumor cerebri during treatment for hypothyroidism. South Med J 1977;71:977.
- Gutch M, Bhattacharjee A, Kumar S, Pushkar D. Graves’ disease and idiopathic intracranial hypertension. Med J DY Patil Univ 2017;10:290-2
- Press OW, Ladenson PW. Pseudotumor Cerebri and Hypothyroidism. Arch Intern Med. 1983;143(1):167–168.
- Iwasaki Y, Kinoshita M, Ikeda K, Takamiya K, Shiojima T. Thyroid function in patients with chronic headache. Int J Neurosci. 1991;57:263-267.
- Liang H, Xu C, Liu T, Huang S, Hu S. Spontaneous intracranial hypotension in Hashimoto’s thyroiditis: A case report. Medicine (Baltimore). 2019;98(18)
- Cansu GB, Dora B, Karaali K, Sari R. Spontaneous intracranial hypotension in Graves’ disease. Euro Res J 2016;2:236–9.
- de Carvalho G, Perez C, Ward L. The clinical use of thyroid function tests. Arq Bras Endocrinol Metabol (2013) 57:193–204
- Braverman LE, Utiger RD, DeLong GR, Adams RD. The neuromuscular system and brain in hypothyroidism. The thyroid, eds Braverman LE, Utiger RD. Lippincott: New York; 1991. p. 1027‐39.
- Sokoloff L, Wechsler RL, Mangold R, Balls K, Kety SS. Cerebral blood flow and oxygen consumption in hyperthyroidism before and after treatment. J Clin Invest 1953; 32:202-8
- Coutinho E, Silva AM, Freitas C, Santos E. Graves’ disease presenting as pseudotumor cerebri: A case report. J Med Case Rep 2011;5:68.
- Dickman MS, Somasundaram M, Brzozowski L. Pseudotumor cerebri and hyperthyroidism. N Y State J Med 1980;80(7 Pt 1):1118-20.
- Mokri B. Spontaneous intracranial hypotension. Continuum (Minneap Minn) 2015;21:1086–108.
- Roos RA, van der Blij JF. Pseudotumor cerebri associated with hypovitaminosis A and hyperthyroidism. Dev Med Child Neurol 1985;27:246-8.