

Evaluation of PresbyMAX for Elderly Presbyopia Treatment
Evaluation of the Outcome of Refractive Error Treatment in Elderly Patients Using the PresbyMAX Method at Sai Gon Can Tho Eye Hospital
Ket V. Tran1, Phap V. Le1, Thanh T. Hoang2
- Sai Gon Can Tho Eye Hospital
- Ha Noi Eye Hospital
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Tran, KV., Le, PV., et al., 2024. Evaluation of the Outcome of Refractive Error Treatment in Elderly Patients Using the PresbyMAX Method at Sai Gon Can Tho Eye Hospital. Medical Research Archives, [online] 12(11). https://doi.org/10.18103/mra.v12i11.6104
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i11.6104
ISSN 2375-1924
ABSTRACT
Purpose: To evaluate the safety, efficacy, and patient satisfaction following PresbyMAX surgery for presbyopia correction.
Methods: A case series study was conducted in a private clinical setting on 25 presbyopic patients (72% females, 28% males; average age: 40.72 ± 3.14 years). The dominant eye underwent standard LASIK for distance correction, while the non-dominant eye received a central PresbyMAX monocular correction. Binocular uncorrected distance visual acuity (BUDVA), near visual acuity (BUNVA), and intermediate visual acuity (BUIVA) were assessed at intervals of 1 week, 1 month, and 3 months post-surgery.
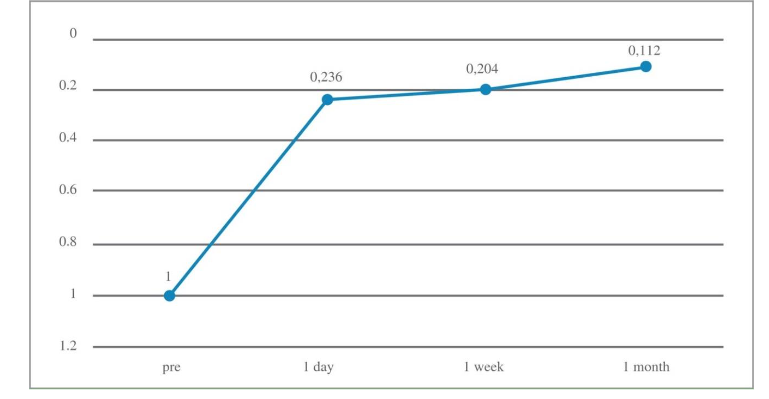
Results: Preoperative spherical equivalent was -3.27 ± 1.16, with an average preoperative visual acuity of 1 ± 0.02. At 1 month postoperatively, mean BUDVA was 0.11 ± 0.09, and BUNVA was 1.96 ± 0.35. BUDVA was at or better than 20/25 and 20/32 in all patients (64% and 96%, respectively). Near vision at J2 or better was achieved by 96% of patients. Post-surgery, 92% expressed satisfaction, although 8% reported mild symptoms such as blurred vision and glare.
Conclusion: The PresbyMAX monocular correction in combination with standard LASIK in the fellow eye offers a safe and effective solution for elderly patients with presbyopia, yielding high patient satisfaction.
Keywords
Presbyopia, LASIK, PresbyMAX, visual acuity, patient satisfaction
Introduction:
Presbyopia is the irreversible loss of the accommodative ability of the eye that occurs due to aging. Accommodation refers to the ability of the eye to increase its refractive power of the crystalline lens in order to focus near objects on the retina. The most significant decrease in accommodative power occurs in between the ages of 20 and 50.
The Global Burden of Disease Study estimated in 2020 that approximately 510 million people worldwide have visual impairment from uncorrected presbyopia (defined as worse than N6 or N8 near acuity at 40 cm when best-corrected distance visual acuity was 6/12 or better). This represented a 6.3% increase over the past three decades (largely in Eastern Europe and Africa) and this is predicted to increase to 866 million in 2050 due to population ageing. In Asia, the prevalence of presbyopia is about 33.9%. Although age is the primary predictive factor in the development of presbyopia, early loss of accommodative ability can be induced by certain systemic disease, medications, and trauma. The onset is earlier in some regions, such as in subcontinental and African populations, but this has been attributed to ethnic variations rather than environmental differences. Other risk factors associated with presbyopia include dry eye disease (even matching for age and sex) and diabetic glycaemic level. One study has also reported associations with cigarette smoking, pregnancy, refractive error, sunglasses use, and alcohol consumption.
The safest and least invasive management of presbyopia consists of corrective glasses lenses either as a separate set of reading glasses, contact lenses, bifocals, or progressive lenses. There are, however, a growing number of presbyopic patients who desire to remain independent of glasses, and thus, many surgical methods of compensating for near vision deficits in presbyopes have become available. Some methods such as IOL implant surgery or various forms of refractive corneal surgery. Corneal-based procedures offer the advantage of reversibility, they include Monovision LASIK, PRK, PresbyLASIK. PresbyMAX belongs to a subgroup of PresbyLASIK. PresbyMAX® is a module available on SCHWIND AMARIS (SCHWIND eye-tech-solutions GmbH, Kleinostheim, Germany) platform, works on the principle of central presbyLASIK by the creation of a bi-aspheric profile. This is a technique where cornea is ablated using multifocal ablation profiles to correct ametropia and presbyopia.
At Saigon Can Tho Eye Hospital, we have applied the PresbyMAX method on 25 patients. This study reviews the application of PresbyMAX at Saigon Can Tho Eye Hospital, evaluating its efficacy, safety, and patient satisfaction.
Patient Information:
Patients seeking presbyopia correction at Sai Gon Can Tho Eye Hospital were screened. The patients satisfying following criteria were enrolled and followed up throughout to 1 month after surgery. Inclusion criteria were as follows: age > 35 years, spherical refraction error of -10 to +7 dioptres (D); astigmatism of up to -3D; stable refraction for 2 years; no use of contact lens within the previous 2 weeks; strong willing of getting rid of glasses. The exclusion criteria were the following: intolerance to the preoperative anisometropic test (> 0.75D), any eye disease except for refraction errors, a history of ocular surgery or trauma.
Clinical Findings and Diagnostic Assessment:
Regular preoperative examinations were performed, including subjective refraction, intraocular pressure, visual acuity, corneal topography, ophthalmoscope, and slit lamp examination. Visual acuity was tested using a Snellen chart (at 4 m and 0.33 m, respectively, for distance and near visual acuity) including corrected distance visual acuity (CDVA), binocular uncorrected distance visual acuity (BUDVA), binocular uncorrected near visual acuity (BUNVA), and binocular distance corrected near visual acuity (BDCNVA). All visual acuities are expressed in logMAR units. Determine the exact refraction after 3 times of accommodation paralysis with Mydrin-P.
Therapeutic Intervention:
All surgeries were performed by the same operator (Dr. Ket). The surgery consisted of two steps: flap creation using Visumax femtosecond laser (Carl Zeiss Meditec AG, Jena, Germany) and stromal ablation using the Schwind AMARIS 1050RS excimer laser platform with Smart Pulse Technology (Schwind eye-tech-solutions GmbH, Kleinostheim, Germany). The intended flap thickness was 110 µm, with a diameter of 8.0 mm. The patients were then transferred to the Schwind AMARIS platform. A normal aspheric femtosecond-assisted LASIK (FS-LASIK) ablation profile was performed on the dominant eye and a bi-aspheric PresbyMAX ablation profile was performed on the non-dominant eye with the optical zone at 6.2 – 6.8 mm. After the ablation, the central 3 mm cornea zone of the non-dominant eye was reshaped to a hyper-positive area for near correction, which is influenced by the amount of presbyopia addition. The addition was planned and selected within the range of +1.25 to +2.50 D for non-dominant eyes.
Follow-up and Outcomes:
Patients are instructed to wear protective eyewear. 0.5% Levofloxacin, artificial tears, and 0.1 fluorometholone eye drops for 1 week. Patients were reviewed at 1 day, 1 week, and 1 month, 3 months, and 1 year after surgery. Evaluation index includes: binocular uncorrected distance visual acuity (BUDVA), binocular uncorrected near visual acuity (BUNVA), safety index (postoperative CDVA/preoperative CDVA), which reflects the surgery’s safety on visual acuity, was calculated.
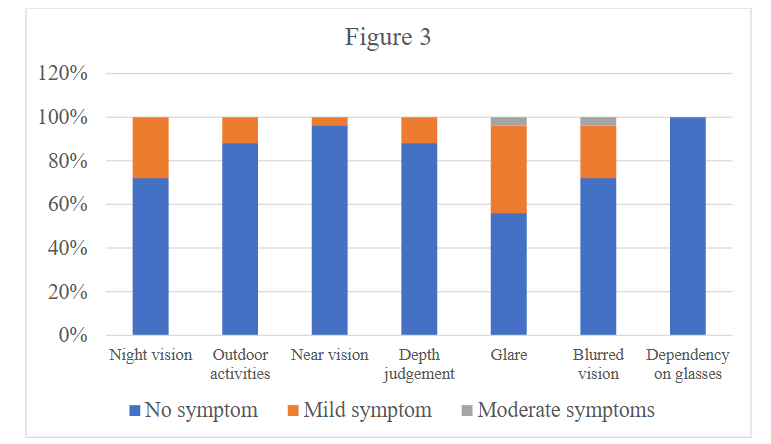
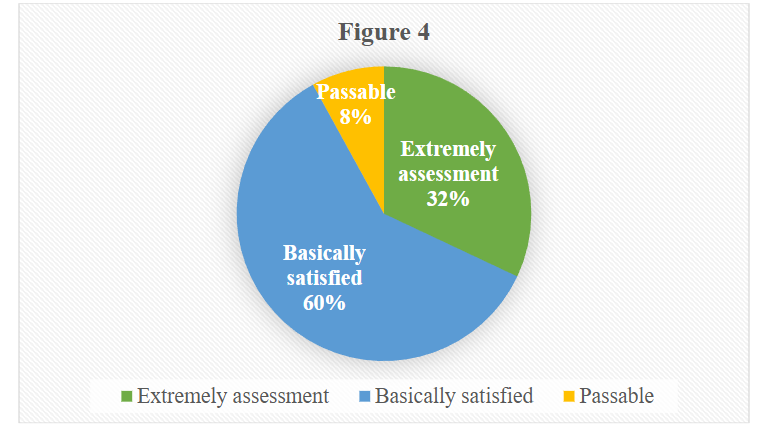
Satisfaction was subjectively assessed preoperative at 1 month. The questionnaire covered several aspects including: Night vision, outdoor activities, near vision, depth judgement, glare, blurred vision, subjective satisfaction. Each symptom was assessed according to four levels: 1 – No symptom, 2 – Mild symptom, 3 – Moderate symptoms, 4 – Severe symptoms. For satisfaction assessment: 1 – Extremely satisfied, 2 – Basically satisfied, 3 – Passable, 4 – Not satisfied.
Results:
In total, 50 eyes of 25 patients were included, all patients had myopia and or associated astigmatism. Basic demographic information of patients is summarized in Table 1.
| Variables | Age | Sex | The mean Preoperative spherical equivalent | The mean Preoperative visual acuity |
|---|---|---|---|---|
| Mean (SD) | 40.72 (3.14) | Male 7, Female 18 | -3.27 (1.16) | 1 (0.02) |
EFFICACY
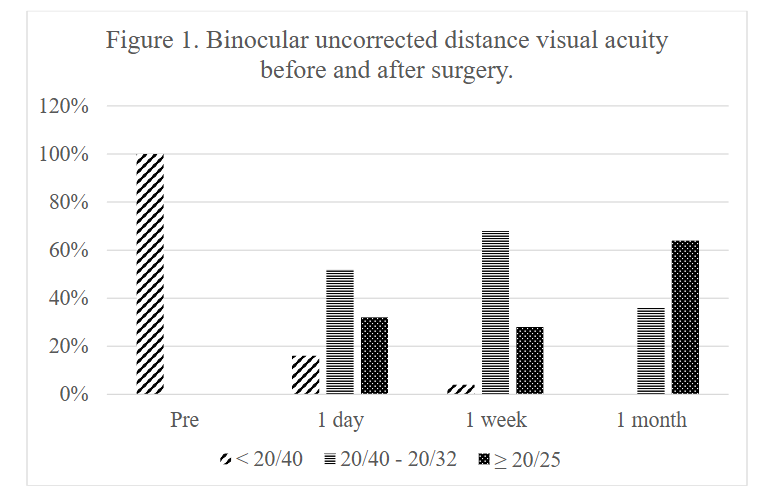
At the follow-up one month after surgery, BUDVA was equal or better than 20/25 and 20/32 in all patients, 64% and 96%, respectively. The BUDVA at 1 month postoperatively was 0.11 ± 0.09, the BUNVA was 1.96 ± 0.35.
The BUNVA after 1 month of surgery is shown in Table 2.
| J1 | J2 | J3 | |
|---|---|---|---|
| 1 month | 8% | 88% | 4% |
SAFETY INDEX
All surgeries went smoothly, without any complications during surgery or after surgery. The safety index was 1.04 ± 0.11.
STABILITY
UDVA and BUDVA improved significantly after surgery (p < 0.01). There was no significant difference in BUDVA between 1 day and 1 week postoperatively, but BUDVA improved since 1 month after surgery (post 1 month vs. post 1 day, P < 0.01).
SATISFACTION ANALYSIS
The patient satisfaction questionnaire showed: 92% were satisfied with the surgical results, 8% were temporary. Patients complain mainly of symptoms of night vision, glare, and blurred vision. No patient was dependent on glasses after surgery.
Discussion:
Presbyopia is one of the problems that frequently occurs in people over 40 years old. Refractive surgery on this subject has been proven to be highly effective in terms of economy and quality of life. Previous studies have reported the efficacy and safety of surgical correction for presbyopia.
Our results demonstrate that PresbyMAX is a safe technique, with a safety index of 1.04 ± 0.11. Similar results have been reported in previous conventional LASIK procedures. D. Fu acquired a short-term safety index of 1.03 ± 0.14.
In this study, BUDVA was equal or better than 20/25 and 20/32 in all patients, 64% and 96%. UNVA > J3 in 96%. Baudu et al. studied 358 presbyopic patients with myopia and hyperopia using PresbyMAX. At 6 months, in the myopic and hyperopic groups, they found binocular UDVA >20/25 in 70% and 74%, respectively, and UNVA > J3 in 94% and 87%, respectively. They also reported a retreatment of 19% in both the groups. In the study of Tommy et al. Eighty-seven percent of patients achieved UDVA of 20/25 or better and 90% had UNVA of J3 or better.
At 1 month after surgery, the overall satisfaction was 92% (23/25). Baudu et al. found that ~83% of patients achieved objectively successful outcomes because some patients asked for retreatment to improve distance or near vision.
There were 2 patients who felt passable with the surgical results. These patients mostly present with symptoms of difficulty with night vision and glare. One limitation of the present study is the relatively small sample size.
Conclusion:
The PresbyMAX technique provides a safe, efficient solution for presbyopic patients desiring independence from corrective lenses. Further studies with larger samples and longer follow-up are recommended to substantiate these findings.
References:
- American Optometric Association. (2010). Care of the Patient with Presbyopia. St. Louis, MO.
- Bourne, R., Steinmetz, J. D., Flaxman, S., Briant, P. S., Taylor, H. R., Resnikoff, S., … & Tareque, M. I. (2021). Trends in prevalence of blindness and distance and near vision impairment over 30 years: an analysis for the Global Burden of Disease Study. The Lancet global health, 9(2), e130-e143.
- He, M., Abdou, A., Ellwein, L. B., Naidoo, K. S., Sapkota, Y. D., Thulasiraj, R. D., … & Congdon, N. G. (2014). Age-related prevalence and met need for correctable and uncorrectable near vision impairment in a multi-country study. Ophthalmology, 121(1), 417-422.
- Mai, E. L., Lin, C. C., Lian, I., Liao, R., Chen, M., & Chang, C. (2019). Population-based study on the epidemiology of dry eye disease and its association with presbyopia and other risk factors. International Ophthalmology, 39, 2731-2739.
- Kaido, M., Kawashima, M., Shigeno, Y., Yamada, Y., & Tsubota, K. (2017). Relation of accommodative microfluctuation with dry eye symptoms in short tear break-up time dry eye. PLoS One, 12(9), e0184296.
- Ayaki, M., & Negishi, K. (2022). Short tear breakup time could exacerbate the progression of presbyopia in women. BioMed Research International, 2022(1), 8159669.
- Srinivasan, R., Paramasivan, G., Sharma, A., Surya, J., Sharma, T., & Raman, R. (2021). Prevalence, risk factors and association with glycemic levels of presbyopia in South Indian population. Indian Journal of Ophthalmology, 69(11), 3173-3178.
- Andualem, H. B., Assefa, N. L., Weldemichael, D. Z., & Tefera, T. K. (2017). Prevalence and associated factors of presbyopia among school teachers in Gondar city, Northwest Ethiopia, 2016. Clinical optometry, 85-90.
- Yildirim, Y., Olcucu, O., Alagoz, C., Basci, A., Agca, A., Yasa, D., … & Demirok, A. (2016). Visual and refractive outcomes of photorefractive keratectomy and small incision lenticule extraction (SMILE) for myopia. Journal of Refractive Surgery, 32(9), 604-610.
- Fu, D., Aruma, A., Xu, Y., Han, T., Xia, F., & Zhou, X. T. (2022). Refractive outcomes and optical quality of PRESBYOND laser-blended vision for presbyopia correction. International Journal of Ophthalmology, 15(10), 1671.
- Fu, D., Zhao, J., Zeng, L., & Zhou, X. (2020). One year outcome and satisfaction of presbyopia correction using the PresbyMAX® monocular ablation profile. Frontiers in Medicine, 7, 589275.
- Baudu, P., Penin, F., & Mosquera, S. A. (2013). Uncorrected binocular performance after biaspheric ablation profile for presbyopic corneal treatment using AMARIS with the PresbyMAX module. American journal of ophthalmology, 155(4), 636-647.
- Chan, T. C., Kwok, P. S., Jhanji, V., Woo, V. C., & Ng, A. L. (2017). Presbyopic correction using monocular bi-aspheric ablation profile (PresbyMAX) in hyperopic eyes: 1-year outcomes. Journal of Refractive Surgery, 33(1), 37-43.
- Baudu, P., Penin, F., & Mosquera, S. A. (2013). Uncorrected binocular performance after biaspheric ablation profile for presbyopic corneal treatment using AMARIS with the PresbyMAX module. American journal of ophthalmology, 155(4), 636-647.