

Adult Day Center Use in Older Mexican Americans with Dementia
Adult Day Center Use among Older Mexican Americans with Dementia in California and Texas
Jacqueline L. Angel, Ph.D.¹, Sunshine M. Rote, Ph.D.²*
- Wilbur J. Cohen Professor of Health and Social Policy and Professor of Sociology, The University of Texas at Austin, LBJ School of Public Affairs
- Associate Professor and Associate Dean for Research, The University of Louisville, Kent School of Social Work and Family Science
OPEN ACCESS
PUBLISHED: 31 October 2024
CITATION:Angel, JL., Rote, SM., et al., 2024. Adult Day Center Use among Older Mexican Americans with Dementia in California and Texas. Medical Research Archives, [online] 12(10). https://doi.org/10.18103/mra.v12i10.5936
COPYRIGHT:© 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI:https://doi.org/10.18103/mra.v12i10.5936
ISSN 2375-1924
ABSTRACT
Background.
Dementia is one of the most common causes of disability and dependence in the world and is a frequent reason that older people require supportive living arrangements. Providing such arrangements on a broad scale will require a broad public dialogue and insights from social science, especially with respect to the neediest, who suffer from a profound gap in access to care. New and innovative social policy, in line with Recommendation #10 of the European Society of Medicine Policy Framework Reducing the Burden of Neurodegenerative Diseases in Europe and Beyond, is vital. The current study offers insights based on dementia care for Latinos in California and Texas, a population with a high incidence of the disease and few low access to resources.
Objective.
This study investigates how a growing number of Latino families use adult day care services. We focus on California and Texas, the two states with the largest Latino populations of Mexican origin with dual-eligible (Medicare and Medicaid) beneficiaries.
Methods.
We employ the 2016 Hispanic Established Epidemiologic Studies of the Elderly to compare the socioeconomic characteristics of Mexican Americans 85 and over who are day care service users living with and without dementia in both states (n = 406). Logistic regressions are used to determine the likelihood of participation in adult day care programs in both states by insurance status.
Results.
Compared to California, restrictive income eligibility requirements in Texas limit participation in adult day care despite a higher need for care. Multivariate analyses reveal that foreign-born dual-eligibles in Texas are particularly dependent on family to provide dementia caregiving in comparison to the native born; they do not report using adult day health services.
Conclusion.
The paper ends with a discussion of viable policy options for promoting equity in access to affordable and sustainable adult day health centers as well as other community-based long-term care services in Texas and California. A multi-faceted approach is necessary and must involve all levels of government, as well as private and charitable organizations.
Keywords: Alzheimer’s Disease and Dementia, Adult Day Care, Medicare/Medicaid insurance, Mexican Americans, Health Equity.
Introduction
As the population of 78 million baby boomers in the United States ages, the total number of people with dementia will inevitably rise. Nearly 7 million U.S. residents ages 65 or older had dementia in 2023 and this figure is expected to double by 2060 if current demographic trends continue¹. These trends have serious consequences for the family, the community, and governmental agencies at all levels as nations struggle to adapt to the needs of a society while devoting adequate resources that foster economic development and full employment. Due to global shifts in women entering the workforce and the mobility of many households, informal support systems are smaller, more dispersed, and generally are less able to allocate the time and resources necessary to provide all the care an aging parent living with dementia might need than they once were. In the Americas, for example, in the United States, this change is affecting even the Latino communities that have historically been highly “familistic,” the ideal which informs the structures, processes, and interactions of Latino culture².
This study investigates the consequences of rapid population aging and its implications for minority groups, focusing on Latinos in two large states. California and Texas have similar demographic profiles but quite different political cultures, and a significant fraction of low resourced residents. This population suffers disproportionately from lifelong disadvantages in terms of education, occupation, asset accumulation, and retirement security. Consequently, they are at elevated risk of Alzheimer’s disease. This crisis will disproportionately affect individuals with the fewest resources with which to manage the illness.
The United States does not guarantee publicly funded medical care to the entire population. However, those who contribute to Social Security receive Medicare at age 65. Medicare, however, covers only 80% of medical expenditures, nor does it pay for long-term care, aside from a short period of post-acute care. In the absence of supplemental insurance (referred to as Medigap) even middle-class individuals and families can be seriously burdened. For the poorest older individuals long-term care can be paid for by Medicaid. The Medicaid program is a jointly federal state entitlement safety-net program that finances health and long-term care services for low-income populations. Federal and State law determines eligibility. As a result, the extent of coverage varies by each state, as does access to Medicaid services across states.
California and Texas also have a high proportion of dual eligible, a term that refers to recipients of both Medicare and Medicaid, commonly known as duals. Full Duals receive all the services offered, including physician, hospital, nursing home care, and community-based services, such as adult day care, and home health care. Partial duals, low-income Medicare beneficiaries who qualify for Medicaid, do not receive long-term care. Although they do receive coverage for doctor visits and hospitalization, they are responsible for their out-of-pocket expenses (e.g., co-payments and deductibles).
Older adult duals account for one-third of state Medicaid (a public health program for low-income persons) spending in the United States³. This is particularly salient because states have a great deal of discretion in how to structure their Medicaid programs. We employ the 2015 Hispanic Established Epidemiologic Studies of the Elderly (H-EPESE) to examine how socioeconomic characteristics and functional cognitive status predict use of ADCs in both states. The paper ends with a discussion of viable policy options for closing the gap in access to affordable and sustainable adult day care as well as other community-based long-term care services and supports.
LONGER LIVES, GREATER DEMENTIA DEPENDENCY
For the growing population of older Latinos in the United States, of whom Mexican Americans are the largest subgroup, the future is particularly uncertain. Findings from a benchmark study of Mexican Americans show that the population has longer lives than other racial/ethnic groups, especially among immigrants⁴⁵. Examining the Mexican American population by gender and nativity shows that life expectancy at age 65 is highest for foreign-born Mexican-origin women. However, they will spend over 60% of their remaining years in a seriously physically impaired state while their male peers will spend about 50% of their remaining years in such a state⁴⁵. These added years spent with disability are partly explained by lifetime exposure to physically demanding work⁶,⁷.
As a result of longer lives, there is a growing incidence of dementia in the Mexican-American population. Compared to non-Latino whites, Latinos are more likely to develop mild cognitive impairment and Alzheimer’s disease⁸. Dementia affects 5% of Mexican Americans 60 and over⁹,¹⁰ and 8.8%–12.2% of Latino groups aged 65 and over in the United States¹¹,¹². Estimates for Latinos indicate approximately 200,000 cases of U.S. Latinos living with dementia in 2000 will have ballooned to 11.3 million in 2050¹³. Comparing the two states, age-adjusted death rates due to dementia are much higher in Texas than California.
In both states, an increased number of years characterized by poor health and dependency poses potentially serious economic and social problems for Latino groups given fragile social support, little wealth, and low levels of education, health insurance, and income². In California, there are 1.4 million dementia caregivers who can contribute over $44 million in unpaid care. In Texas, there are 1 million dementia caregivers who provide an economic contribution of $24 million in unpaid care. As age and disabling health conditions force families to make decisions about long-term care, they may have limited options. Employed people cannot provide the level of care an incapacitated older family member requires, and in most U.S. Latino families all working-age family members have jobs¹⁴. Latino families also tend to lack the financial resources to pay for in-home care or other community-based services¹⁵. Even when Medicaid would pay for nursing home care, Latinos, especially those of Mexican heritage, have traditionally been highly resistant to this option¹⁶,¹⁷. ADCs are thus potentially a vital solution for this population if they are affordable and accessible.
ADULT DAY CARE
Long-term care services and supports provide health or personal care needs for individuals unable to perform everyday activities on their own¹⁸. Settings range in the level of care depending on an individual’s physical, mental, and social care needs. Although unpaid family caregivers such as spouses, extended family, and neighbors provide most dementia care¹⁹, increasingly long-term care is offered in third places such as ADCs²⁰. Licensed adult day care in these settings offer services such as meals, exercise, social activities, personal care, and transportation from home. Depending on eligibility or for a fee. Adult day care can promote long-term health care equity for the neediest older adults.
Research shows that in most cases families provide extensive informal care for an individual with dementia, but the demands of this task can cause tremendous strain due to the nature and progression of the disease. As the cognitive abilities of older adults with dementia decrease, the loss of autonomy increases the reliance on caregivers for assistance in self-care and instrumental activities of daily living (IADLs) and with the management of medication²¹. Many families in this situation decide to utilize adult day care to help cope with these challenges. ADCs provide many support services without the steep cost of nursing homes²² and allow care receivers to remain in the community (see Table 1). Advanced stages of dementia seriously undermine the capacity of caregivers and render alternative sources of respite necessary if they are to live in the community. Dementia care recipients are incapable of self-care and need 24/7 supervision, which creates challenges for Latino caregivers²³.of all assistance options available, ADCs are often the most feasible sources of caregiver respite during daytime hours²⁴.
A short-term respite care stay in an ADC is frequently utilized for sporadic support or to promote healthful aging for a parent after hospital discharge or because they cannot be safely left alone. As Table 1 shows, an ADC program provides a range of community-based long-term care services that can include transportation, social activities (e.g., pet therapy, gardening) plus assistance with eating, taking medicines, toileting, and/or walking, mental stimulation, exercise programs, and health monitoring (e.g., blood pressure and food or liquid intake); as well as nursing and medication administration. Caregivers receive respite support consisting of education and counseling as needs change for assistance. Adult day care participants receive care for 10 hours a day in a safe environment.
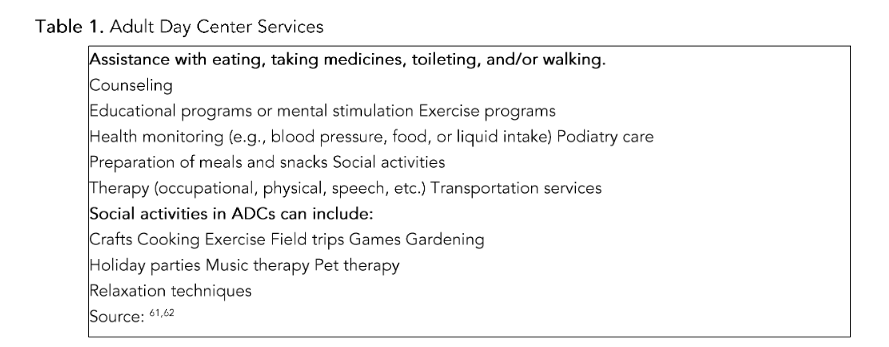
Table 1: Adult Day Center ServicesMedicaid’s Coverage of Home and Community-Based Care began with 1965 amendments to Title 19 of the Social Security Act. Home health care services were one of the optional services under state Medicaid plans. Amendments instituted in 1968 and effective in 1970 required states to provide home health care services to persons entitled to skilled nursing facility care under state Medicaid plans; 1981 amendments created the Medicaid waiver option for home and community-based services under Section 1915(c). Today, 15 state Medicaid programs offer ADCs to needy participants with few financial resources who need skilled nursing care²⁹. These programs are funded by a combination of federal and state dollars and are administered at the state level but subject to federal government standards³⁰.All 50 states and Washington, DC offer assistance for adult day care in one form or another through their Medicaid programs²⁵. A study by MetLife Mature Market Institute and The Ohio State University surveyed over 47,000 people receiving services at 557 ADCs. Findings indicated that 46% went to the center every weekday and 80% attended for a full day when they were present²⁶. This enables family caregivers to continue supporting a care recipient while also holding a job. Most ADCs in the United States are private nonprofits operating in 1,000–5,000 square foot spaces²⁵, and exceptions, for-profit enterprises, have dementia patients as a smaller portion of their care recipient populations than nonprofit facilities²⁷. According to the biennial National Study of Long-Term Care Providers, 28% of people receiving services at ADCs have Alzheimer’s disease and other dementias²⁸.the monthly income limit for eligibility is considerably lower than the limit for Medicaid community-based service waivers. To a lesser extent “regular Medicaid” or Medicaid State Plans offer adult day care as a benefit.
OPTIONS IN CALIFORNIA AND TEXAS
ADC Services
Both California and Texas have statewide Medicaid (Medi-Cal in California) adult day care services included in a state Medicaid plan. Community-based waiver programs exist as an alternative to nursing homes in both states. A requirement of the waiver program is that states can choose how many waivers they would like and must demonstrate that the waiver service is cost neutral. What follows is a discussion of state differences in the implementation of adult day care services in terms of limits in eligibility, specific geographic areas, and funding models.
In California, adult day care is offered under several programs. One such program under the California Bridge to Health Care Reform waiver known as Community-Based Adult Services (CBAS), older adults with dementia receive services in the community at licensed ADCs as well as at other specialized care centers³¹. Under the 1115 demonstration waiver program, states can experiment with community-based options for individuals 18 and older who are eligible for nursing homes. The program’s chief aim is reducing placement of medically needy persons in nursing homes³². Under the CBAS program, Medicaid capitated (pre-paid) private, managed care organizations at designated centers around the state provide care, including adult day care services.³³ The California Department of Aging maintains contact information on approximately 295 licensed ADCs throughout the state³².
A second program is the Medi-Cal Multipurpose Senior Services Program 1915(c) waiver, which is designed to help California adults 65 and older who are at risk of nursing facility placement to continue living in their homes or elsewhere in the community*. Enrollment is capped at 11,370³⁵. Based on fee-for-service, this program achieves this objective by arranging assistance and managing a broad set of services, including adult day care, home modifications, and care management services. Participation eligibility depends on county of residents; 46 of the state’s 58 counties participate, although some counties have waitlists³⁶.
In Texas, Medicaid Day Activity and Health Services (DAHS, formerly known as Adult Day Care Centers) is an entitlement program for Supplemental Security beneficiaries. Services are guaranteed for medically eligible Medicaid participants 18 years and over and DAHS services residents statewide. In 45 [out of 245] Texas counties³⁷, waiting “interest” lists exist partly because many adult day care centers operate at full capacity³⁸. Adult day services are also available statewide under the State of Texas Access Reform Plus (STAR+PLUS HCBS) program, an 1115 managed care waiver program that offers long-term services and supports (LTSS)³⁹. Low-income Medicare beneficiaries with partial dual eligibility do not qualify for the full array of Medicaid medical benefits from their state, including this LTSS program⁴⁰.
Both California and Texas provide adult day care services through the Program of All-Inclusive Care for the Elderly (PACE), a federally funded, state managed care program, although California’s PACE program is far more expansive than the Texas program. PACE is for people 55 or older who participate simultaneously in Medicare and Medicaid who are eligible for nursing home care. It allows them to receive all their benefits through a single organization rather than navigating separate Medicare and Medicaid coverage. PACE uses a comprehensive care approach, providing an array of services that costs less than comparable nursing home care⁴¹. In addition to adult day and other services, the program provides other health-related services, including inpatient and outpatient medical care, specialty services like dentistry and podiatry, social services, in-home care, meals, and transportation.
transportation. California PACE has over 20,000 participants in 26 counties⁴². Texas PACE operates in three cities: Amarillo, El Paso, and Lubbock⁴³. Our previous research on licensed Medicaid adult day centers in Texas and California shows place-based disparities among older adults living along the Texas-Mexico border⁴⁴. The Rio Grande Valley, a metropolitan area located along the U.S./Mexico border on the southernmost tip of Texas, is home to a 98.4 percent Hispanic population and one of the poorest counties in the United States⁴⁵. The ADC landscape is vastly different along the California-Mexico border, as a small fraction of the 257 centers are located along the border region⁴⁶. ADCs located in Southern California account for almost 80% of those in existence, and among these 60% are in Los Angeles County, 21% in Orange, 6% in Riverside, and 6% in San Bernadina. We also estimated household income by county. In Texas, all 20 border counties fall below statewide median household income. California median income is far higher than in Texas, which may explain border differences in the allocation of Medicaid community-based long-term care services⁴⁴. The dual-eligible population—the sickest, the frailest, and the costliest group—is associated with stark disparities in border aging and access to care⁴⁷.
The results also suggest a border paradox in which supply of adult day care may exceed the demand. Unlike California, Texas has a state Medicaid plan that entitles participants to adult day care⁴⁸. A higher proportion of the poor reside in Texas and particularly along the Texas/Mexico border and qualify for full Medicaid benefits despite restrictive participation rules based on income and assets eligibility⁴⁵. Texas also has an extensive Medicaid community-based managed care waiver program, which may increase participation in ADCs⁴⁰. At the same time, Texas partial “duals” (43%) have no long-term care option—either in the community or in a nursing home.
Material and Methods
To investigate state differences in Medicaid-funded dementia ADC use, we employ the 2016 Hispanic-EPESE, a representative sample of community-dwelling of the Mexican-origin population in the United States. Our objective is to compare the socioeconomic characteristics of caregivers of elderly parents with dementia in two states, Texas and California. The Hispanic EPESE provides data on risk factors (age, gender, income, marital status, insurance coverage, and place of residence for mortality and morbidity) in older Mexican Americans to contrast how these factors operate differently than in non-Hispanic whites, African Americans, and other major ethnic groups. Wave 9 is based on the original cohort followed every 2 years since 1993–1994 in five southwestern states: Arizona, California, Colorado, New Mexico, and Texas⁴⁹ and includes the oldest cohort at highest risk of living with dementia. The large sample of Mexican Americans 85 and older (n = 406) allows comparisons to gauge the extent of state-based disparities associated with ADC use across states.
MeasuresDependent Variable.We measure cognitive impairment and likely independent variable section using the Mini Mental Status Examination (MMSE), a brief, standardized method used to grade cognitive status. The MMSE assesses memory and reasoning abilities and encompasses indicators of orientation, attention, immediate and short-term memory recall, language, and the ability to follow simple verbal and written commands. The Spanish-language version, which was used in the household interview for those who preferred it to the English-language version, includes formal translation, back-translation, and agreement on the final content⁵⁰. Prior research finds that overall scores on the English and Spanish language versions are similar⁵¹. The MMSE ranges from 0 to 30⁵², with a score of 24 or greater considered “normal” cognition and with a score less than 20 indicating “likely dementia.” In Wave 9, 103 participants had missing information on the MMSE from a proxy or proxy-assisted interview. In this study, we classified a participant as having dementia if they had an MMSE score of less than 18, a report of Alzheimer’s disease, or a proxy report of dementia and the need for assistance with at least one IADL. If a respondent did not complete the MMSE and relied on a proxy due to being mentally or cognitively incapacitated by Alzheimer’s disease or dementia, they were assigned a “0” on the MMSE in the H-EPESE.Based on an exhaustive review of MMSE validity and reliability and these latter thresholds⁵³, we categorize the sample into two groups: Likely dementia meaning cognitive impairment measured under 18 with or without a need for assistance with an IADL or MMSE score under 18 with at least one IADL disability, a report of Alzheimer’s disease, or proxy report of dementia vs. Not (the reference category as normal, no dementia).
Independent variables.Background characteristics of caregiver recipient are based on self-reports of Age (in years), Gender (1 = female; 0 = otherwise); Nativity (1 = Mexico born; 0 = U.S. born); Marital Status (1 = widowed, separated, or divorced; 0 = married); Number of Children (ranged from 0 to 13); Medicaid Recipient (dual eligible = 1; 0 = no); Coresidence (live with caregiver = 1, 0 otherwise); and Caregiver Type (1 = adult child; 0 = other).
ANALYSISThe analysis begins with a description of the demographic profile of care recipients stratified by California and Texas (Table 2). These states represent the highest fraction of Mexican Americans, a highly vulnerable population. Then, we present logistic regressions of caregiver recipient use of adult day care services by dementia status, state, and sociodemographic factors (Table 3). In the final step, we estimate the demographic profile of ADC users in both states (Table 4). All analyses were performed using STATA18.
ResultsTable 2 presents the demographic characteristics of older Mexican Americans residing in California and Texas. Overall, 12% of older adults residing in Texas used an ADC in the past year compared with 9% of older adults residing in California. There are significantly more older adults with likely dementia in the HEPSE living in Texas than in California (Pearson chi2(1) = 10.2571 Pr = 0.001). The mean age of the sample was 90 years old in both states and the majority are women. There are significant differences in nativity status with more U.S.-born older adults residing in Texas (Pearson chi2(1) = 15.9152; Pr = 0.001). While more Mexican Americans residing in Texas compared to California are unmarried and dual eligible, these differences are not statistically significant. The mean number of children is five and most older Mexican Americans rely on an adult child for most of their care needs and a little over half reside with their caregiver.
MULTIVARIATE ANALYSISTo evaluate whether the best predictors of the likelihood of adult day care utilization differ by state, we ran a logistic regression model that accounts for dementia status and nativity and other key covariates identified in Table 3.
For older Mexican Americans residing in Texas, there were significant differences in ADC usage with significantly fewer women (vs. men) and U.S.-born adults (vs. Mexico-born) utilizing these services. Additionally, married older adults were less likely and dual-eligible older adults were more likely to use an ADC though these results were only marginally significant (p=.06, p=.07).For older adults residing in California, number of kids was statistically significant with ADC usage with each additional child associated with 29% lower odds of using ADCs
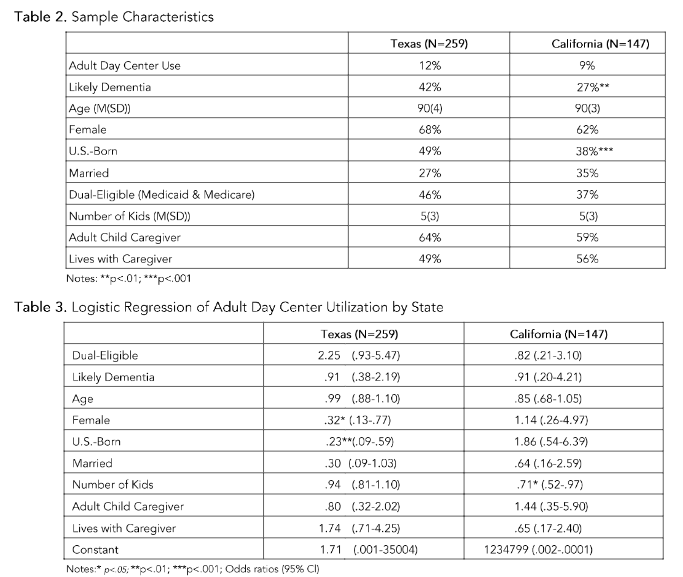
Table 2: Sample Characteristics
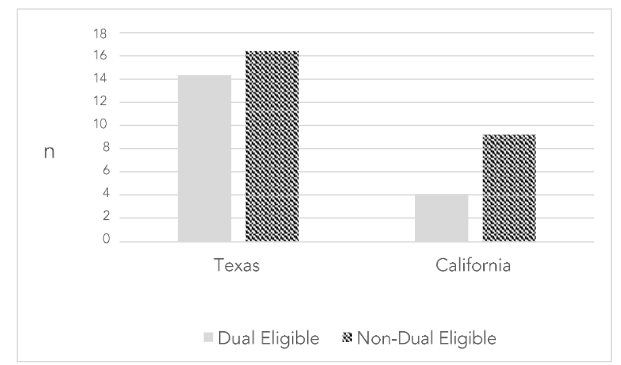
Table 4 provides descriptive statistics for ADC users in Texas and California. From these results, we see that half of the older Mexican American adults residing in Texas who use ADCs have likely dementia compared with 23% of older adults who use ADCs residing in California. ADC users are older than the overall sample with a mean age of 90. More ADC users in California are women, U.S. born, and currently married than in Texas. There are significant differences among ADC users with more duals using ADCs in Texas (46%) compared with California (31%)
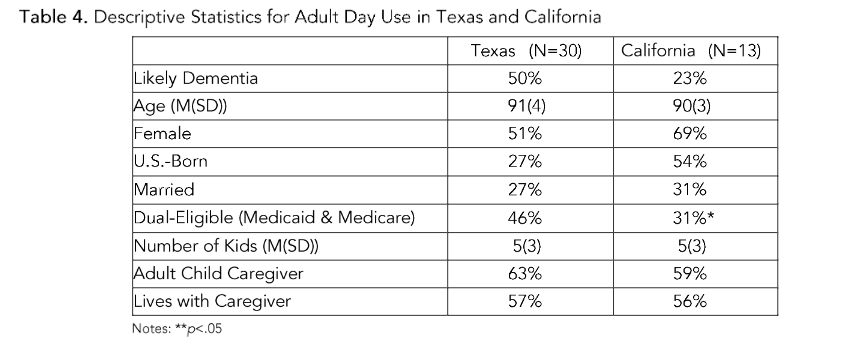
Figure 1 presents cognitive status and health characteristics of ADC users. Low-income Medicare beneficiaries who qualify for Medical (Medi-Cal in California) versus traditional coverage are known as dual eligible). The data reveal that more older adults residing in Texas, especially dual eligible, utilize ADCs than older adults residing in California.
Figure 1. Dual status of ADC Usage by State
Discussion
Access to adult day services and other community-based long-term care services will become increasingly important in public discourse as the populations of both California and Texas rapidly age. The growing number of individuals living with dementia magnifies that need. All states offer Medicaid benefits at some level to older adults who are dual eligible, but states pursue very different routes depending on political culture, population trends, and the imperative for cost containment. This paper highlights significant differences between these two states. The results provide insights into the structural circumstances, giving rise to greater ADC service use. Particularly, it reveals the role of smaller family size in ADC usage in California and the role of gender and migration history in ADC usage in Texas.
As was briefly noted at the beginning of this article, California and Texas are rapidly aging and resemble each other in terms of population characteristics including race, Hispanic ethnicity, immigration, and geographic variation, and rural areas. The U.S. Census Bureau estimated a total of 55 million older Americans in 2020 with California and Texas making up the lion’s share of the oldest populations 65 and over in the Southwestern United States, 6.2 million in California and 3.9 million in Texas. Florida ranks second⁵⁴. Both states are becoming Latinized. In 2020, California and Texas had the highest number of older Hispanics, respectively, as well as Mexican immigrants of any U.S. state or the District of Columbia⁵⁵. California and Texas lead the country in rural areas and agricultural industry, which is a major economic engine. California’s technology sector is a major source of revenue. These population aging trends signal the need for an expanded role of federal and state support at all levels.
Politically, Texas has no state income tax and has a limit on social spending in its constitution. California does not have limits. Texas expects citizens to be self-sufficient. From this viewpoint, Texans take responsibility to take care of themselves and their family, and do not turn to the state for assistance. Texas lawmakers and public officials see a higher cost for social services, possible labor shortages, and higher costs for pensions, and health care as probable outcomes of having a larger older population. In 2023, the 88th Texas state legislature passed legislation to better prepare aging Texas.
Interagency Aging Services Coordinating Council (IASCC) to develop a five-year strategic statewide approach for implementing aging programs and services⁵⁶. The 2024–2029 IASCC Report is expected to develop a strategic plan for meeting the need for aging services, an updated inventory of state-funded interagency aging programs and services, and ways of fostering collaboration for the effective expenditure of available federal and state money for interagency aging services in this state. All this strategic planning for the next five years requires a deeper understanding of the future growth in the aging of the Hispanic population, which will occur at a time when fiscal strains on the state and municipal budgets will be increasing. Older Texans with few resources will place new demands on publicly funded health and long-term care programs, as well as other social service services. The demand for programs like adult day care as fewer families will provide informal care and as the number of older individuals with dementia grows. Caregivers will be forced to find multiple ways of dealing with the burden and government will be required to develop programs that support their efforts.
Under California’s Master Plan for Aging (MPA), a 10-year blueprint to prepare the state for an aging population, a 2023–24 report cited major progress toward 132 initiatives that were the focus of the first two years of MPA implementation in 2022, including achievements in Community Care Expansion, and have awarded adequate funding of projects for dementia care awareness⁵⁷. The Department of Health Care Services (DHCS) launched the nation’s first Dementia Care Aware program. Through this $23 million investment, DHCS, in partnership with UC San Francisco, is leading a statewide program for primary care providers, including trainings, tools, and resources needed to administer cognitive health assessments in a culturally responsive manner and determine the appropriate next steps for patients. More than 660 beds or units will be created with these funds.
California also launched the MPA Initiatives Tracker, an interactive website that provides on-demand public access to initiative progress updates. The state’s MPA recognizes that the next generation of older Californians will be significantly more diverse, will live longer, and will frequently face challenges in adaptation to a new culture that can be accompanied by health, social, and economic disparities that must be addressed.
In previous work, Angel and colleagues found significant differences in benefits by state. California had more full duals than partial duals⁴⁷. This pattern persists. In 2021, 98% of dual Medicare and Medicaid recipients were eligible for full benefits in California compared to 48% in Texas³. In California, Hispanic dual eligibles are also more likely than in Texas to be full beneficiaries than partials⁵⁸. California’s program provides all Medi-Cal services to individuals with no share of cost, including acute care, long-term nursing⁴°. In the current study, our multivariate analyses reveal that Mexico-born dual recipients in Texas are particularly dependent on family and informal networks to provide dementia care compared to U.S.-born dual recipients. They do not report using adult day health services to the same degree. These findings suggest that while ADCs are a valuable resource for Mexican Americans, administrative barriers may hinder use, increasing family caregiver burden that is often reported when Latino caregivers have limited or no family support⁵⁹. The majority of caregivers are women, and family caregiving responsibilities are frequently cited as the main reason of exiting the workforce⁶⁰.
What is more, addressing the impediments to support family caregivers will require strengthening the Caregiver Respite Program (CRP), which allocates funds to support states, like California and Texas⁶¹. The CRP program trains caregivers to provide self-care, wellness, and relaxation therapies. Access to these interventions is available at home, in adult day care centers, and overnight residential facilities and increasing outreach efforts and awareness of them is essential. Respite services offered at adult day centers are a critical source of necessary information to lessen burden on all family members, including keeping women in the workforce⁶².
Finally, both states use federally funded Medicaid/Medi-Cal waiver programs. Texas relies more on managed care organizations (MCOs) and statewide implementation of these programs to contain costs of dual eligibles. California uses a combination of federal, state, and local resources to address the diverse needs of the aging population, focusing more on specialized programs and federal funding to provide services. A question remains as to whether adult day care and community-long term care in a MCO model are cost-effective and equitable. Additionally, the COVID-19 global pandemic had a significant effect on older Mexican Americans living in Texas and California, which may have magnified disparities in both dementia and access to care. In response to these critical questions, future research issues merit attention in order to understand how best to support these populations.
Conflict of Interest Statement:
None declared.
Funding Statement:
This study was funded by the National Institute on Aging (R03/AG063183-02).
Acknowledgements:
None.
Both authors have reviewed and approved the final version submitted for publication.
References
1. Alzheimer’s Association. 2023 Alzheimer’s disease facts and figures. Alzheimer’s & Dementia. 2023;19(4):1598-1695.
2. Angel RJ, Angel JL. Latinos in an Aging World: Social, Psychological, and Economic Perspectives. New York: Routledge; 2015.
3. MEDPAC. Data Book: Beneficiaries Dually Eligible for Medicare and Medicaid. Retrieved 7/21/24 from https://www.macpac.gov/wpcontent/uploads/2024/01/Jan24MedPACMACPACDualsDataBook-508.pdf. ln:2024.
4. Angel RJ, Angel JL, Hill TD. Longer Lives, Sicker Lives? Increased Longevity and Extended Disability Among Mexican-Origin Elders. The Journals of Gerontology Series 8: Psychological Sciences and Social Sciences. 2015;70(4):639-649.
5. Garcia MA, Downer B, Chiu CT, SaenzJL, Rote S, Wong R. Racial/Ethnic and Nativity Differences in Cognitive Life Expectancies Among Older Adults in the United States. The Gerontologist. 2017;59 (2):281-289.
6. Boen CE, Hummer RA. Longer-but Harder Lives?: The Hispanic Health Paradox and the Social Determinants of Racial, Ethnic, and Immigrant Native Health Disparities from Midlife through Late Life. Journal of Health and Social Behavior. 2019; 60(4):434-452.
7. Montez JK, Angel JL, Angel RJ. Employment, Marriage, and Inequality in Health Insurance for Mexican-Origin Women. Journal of Health and Social Behavior. 2009;50(2):132-148.
8. Office of the Assistant Secretary for Planning and Evaluation. Racial and Ethnic Disparities in Alzheimer’s Disease: A Literature Review. Retrieved 3/1/2020 from https://aspe.hhs.gov/report/racialand-ethnic-disparities-alzheimers-disease-1iterature-review. 2014.
9. Haan MN, Mungas DM, Gonzalez HM, Ortiz TO, Jagust WJ. Prevalence of Dementia in Older Mexican Americans: Influence of Stroke, Diabetes and Genetic Factors. Journal of the American Geriatric Society. 2003.
10. Mejia-Arango S, Aguila E, Lopez-Ortega M, et al. Health and social correlates of dementia in oldest-old Mexican-origin populations. Alzheimer’s Disease and Dementia: Translational Research and Clinical Interventions. 2020.
11. Langa KM, Larson EB, Crimmins EM, et al. A Comparison of the Prevalence of Dementia in the United States in 2000 and 2012. JAMA Internal Medicine. 2017;177(1):51-58.
12. Matthews KA, Xu W, Gaglioti AH, et al. Racial and ethnic estimates of Alzheimer’s disease and related dementias in the United States (2015& #x2013;2060) in adults aged ≥65 years. Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association. 2019;15(1):17-24.
13. Alzheimer’s Disease Research and Resource Foundation. Dementia Statistics. Retrieved 3/1/2020 from https://ararf.org/dementia-statistics/. 2019.
14. Brown HS, Herrera AP, Angel JL. Opportunity Costs Associated with Caring for Older Mexican Americans. 2013;28:375-389.
15. Herrera AP, George R, Angel JL, Markides K, Torres-Gil F. Variation in Older Americans Act Caregiver Service Use, Unmet Hours of Care, and Independence Among Hispanics, African Americans, and Whites. Home Health Care Services Quarterly. 2013;32(1):35-56.
16. Angel JL, Angel RJ, Aranda MP, Miles TP. Can the Family Still Cope? Social Support and Health as Determinants of Nursing Home Use in the Older Mexican-origin Population. Journal of Aging and Health. 2004;16:338-354.
17. Thomeer MB, Mudrazija S, Angel JL. How Do Race and Hispanic Ethnicity Affect Nursing Home Admission? Evidence From the Health and Retirement Study. The Journals of Gerontology Series 8: Psychological Sciences and Social Sciences. 2015;70(4):628-638.
18. National Institute on Aging. What is Long- term Care? Retrieved 7/20/20 from https://www.nia.nih.gov/health/what-long-term care. ln:2017.
19. Callahan CM, Sachs GA, Lamantia MA, Unroe KT, Arling G, Boustani MA. Redesigning systems of care for older adults with Alzheimer’s disease. Health affairs (Project Hope). 2014;33(4): 626-632.
20. Torres S, Cao X. Improving Care for Elders Who Prefer Informal Spaces to Age-Separated Institutions and Health Care Settings. lnnov Aging. 2019;3(3):igz019.
21. Angel JL, Lopez-Ortega M, Chiu CT, et al. Loss of Autonomy: Likely Dementia and Living Arrangement Transitions among Mexicans and Mexican Americans. Gerontologist. 2023.
22. National Adult Day Services Association. Adult Day ServicesThe Most Cost-Effective Option in Long-Term Care Today Retrieved 3/1/2020 from https://www.nadsa.org/wp- content/uploads/2017/05/Updated-NADSA Public-Policy-Day-2017-Documents.pdf. 2017.
23. Rote SM, Angel JL, Moon H, Markides K. Caregiving Across Diverse Populations: New Evidence From the National Study of Caregiving and Hispanic EPESE. Innovation in aging. 2019;3(2):igz033 .
24. Alzheimer’s and Dementia Caregiver Center. Adult Day Centers Retrived on 12/5/2016 from http://www.alz.org/care/alzheimersdementia-adult-day-centers.asp#ixzz4S02HPOWA ln:2016.
25. National Adult Day Service Association. Overview: About Day Services. Retrieved 6/23/24 from https://www.nadsa.org/research/overview/#:-:text=With%20more%20than%207%2C500%20ADS,source%20of%20Iong%2Dterm%20care.ln:2024.
26. Metlife Mature Market Institute. The 2011 MetLife Market Survey of Nursing Home, Assisted Living, Adult Day Services, and Home Care Costs Retrieved 12/13/19 from https://www.aarp.org/content/dam/aarp/livablecommunities/old-learn/health/the-metlife-marketsurvey-of-nursing-home-assisted-living-adult-dayservices-and-home-care-costs-2011-aarp.pdf. ln:2011.
27. Lendon JP, Rome V. Variation in Adult Day Services Center Participant Characteristics, by Center Ownership: United States, 2016. Retrieved 6/23/24 from https://www.cdc.gov/nchs/data/databriefs/db296.Qili.2018.
28. Lendon JP, Singh P. Adult Day Services Center Participant Characteristics: United States, 2018. Retrieved 6/23/22 from https://www.cdc.gov/nchs/data/databriefs/db411.Qili.2021.
29. Paying for Senior Care. Medicaid & Adult Day Care: State by State Benefits & Eligibility. Retrieved 7/8/24 from https://www.payingforseniorcare.com/medicaidwaivers/aduIt-day-care. 2024.
30. Norouzi N, Angel JL. Intergenerational Day Centers: A New Wave in Adult and Child Day Care. International Journal of Environmental Research and Public Health. 2023;20(1):809.
31. California Department of Aging. CBAS Providers. Retrieved 3/15/2020 from https://www.aging.ca.gov/ProvidersandPartners/Community-BasedAdultServices/CBASProviders/. 2020.
32. California Department of Health Services. CalAIM 1115 Demonstration & 1915(6) Waiver. Retrieved 6/21/24 from https://www.dhcs.ca.gov/provgovpart/Pages/CalA IM-1115-and-19156-Waiver-Renewals.aspx. ln:2024.
33. Medicaid Waiver.org. California Medicaid Waiver Disability Services & Waivers Retrieved 2/11/2018 from http://medicaidwaiver.org/state/california.htmI.ln:2018.
34. California Department of Aging. Multipurpose Senior Services Program Narrative. Retrieved 6/22/24 from https://aging.ca.gov/download.ashx?IE0rcNUV0zZa7b30odaOzg%3d%3d.ln:2022.
35. California Department of Aging Medi-Cal Service Branch. Multipurpose Senior Services Program. Retrieved 6/22/24 from https://mcweb.apps.prd.cammis.medical.ca.gov/assets/871A7A2D-4BC7-4FA2-AC5E-B42E75935A0B/multisen.pdf?accesstoken=6UyVkRRfByXTZEWlh8j8OaYylPyP5ULO. ln:2020.
36. American Council on Aging. California Medicaid (Medi-Cal) Multipurpose Senior Services Program: Benefits, Eligibility & How to Apply. Retrieved 6/22/24 from https://www.medicaidplanningassistance.org/medi-cal-m ultipurpose-senior-services/. In:2024.
37. Texas Health and Human Services. Texas Health and Human Services Commission, Directory of Traditional DAHS and DAHS with Individualized Skills and Socialization Facilities with an Active License. Retrieved 7/8/24 from https://www.google.com/url?sa=i&url=https%3A%2F%2Fapps.hhs.texas.gov%2Fproviders%2Fdire ctories%2FDAHS.xlsx&psig=AOvVaw1MpCZmNJpxZZnRjxFlakhm&ust=1720547305676000&sourc e=images&opi=89978449. ln:2024.
38. Texas Health and Human Services. Interest List Reduction.Retrieved 7/8/2024 from https://www.hhs.texas.gov/about/recordsstatistics/interest-list-reduction. In:2024.
39. Texas Health and Human Services. STAR+ PLUS. Retrieved 7/8/24 from https://www.hhs.texas.gov/services/health/medica id-chip/medicaid-chip-members/starplus ln:2024.
40. Texas Health and Human Services. Dual Eligible Individuals Enrolled in Medicaid Managed Care. Retrieved 7/8/24 from https://www.hhs.texas.gov/sites/default/files/documents/dually-eligible-individuals-enrolledmedicaid-managed-care.pdf. ln:2022.
41. CalPace. PACE Cost-effectiveness. Retrieved 6/22/24 from https://www.calpace.org/wp content/uploads/2017/12/PACE-Cost-Effective-FactSheet.pdf#:-:text=Based%20on%20analysis%20of%20recent%20data%2C%20PACE%20costs,and%20out%20of%20expensive%20hospitals%20and%20nurs ing%20homes. 2019.
42. CalPACE. Cal PACE. Retrieved 6/22/2024 from https://calpace.org/0,000. 2024.
43. National PACE Association. PACE in the States. Retrieved 6/22/24 from https://www.npaonIine.org/docs/defauItsource/public-files/publicpaceinthestates5.1.24.pdf?sfvrsn=7041002c 1.2024.
44. Angel JL, Rote SM. Dementia Support among Older Mexican Americans: Is Adult Day Care a Viable Alternative? In: Angel JL, ed. Understanding the Context of Cognitive Aging: Mexico and the United States. Vol 5. Cham Switzerland: Springer Nature; 2021:227-245.
45. U.S. Census Bureau. OuickFacts: Rio Grande City, Texas Retrievec 3/15/2020 from https://www.census.gov/quickfacts/fact/table/riograndecitycitytexas/RHl725218#RHl725218.ln:2019.
46. California Department of Social Services. The Regions of California: Recommended Grouping of the Counties for Regional Studies. Retrieved 3/15/2020 from https://www.cdss.ca.gov/research/res/pdf/muItire ports/RegionsofCalifornia.pdf. ln:2002.
47. Angel JL, Angel RJ, Cantu P. Medicaid Use among Older Low-Income Medicare Enrollees in California and Texas: A Tale of Two States. Journal of health politics, policy and law. 2019;44(6):885- 910.
48. Texas Aging Services Council. Aging Texas Well Strategic Plan: 2020-2021. Retrieved 8/24/24 from https://www.hhs.texas.gov/sites/default/files/documents/laws-regulations/reports-presentations/2019/ag ing-tx-well-strat-plan-2020- 21-sept-2019.pdf. 2019.
49. National Archive of Computerized Data on Aging. Hispanic Established Populations for the Epidemiologic Study of the Elderly (HEPESE) Wave 9, 2016 [Arizona, California, Colorado, New Mexico, and Texas] (ICPSR 39038). Retrieved 6/23/24 from https://www.icpsr.umich.edu/web/NACDA/studie s/39038. ln:2024.
50. Hill T, Angel J, Balistreri K, Herrera A. Immigration Status and Cognitive Functioning in Late Life: An Examination of Gender Variations in the Healthy Immigrant Effect. Social Science & Medicine. 2012;75:2076-2084.
51. Morales LS, Flowers C, Gutierrez P, Kleinman M, Teresi JA. Item and scale differential functioning of the Mini-Mental State Exam assessed using the Differential Item and Test Functioning (DFIT) Framework. Med Care. 2006;44(11 Suppl 3):S143- 151.
52. Folstein MF, Folstein SE, McHugh PR. “Mini mental state”: a practical method for grading the cognitive state of patients for the clinician. Journal of psychiatric research. 1975;12(3):189-198.
53. Tombaugh TN, McIntyre NJ. The Mini Mental State Examination: A Comprehensive Review. Journal of the American Geriatrics Society. 1992;40(9):922-935.
54. U.S. Census Bureau. Exploring Age Groups in the 2020 Census. Retrieve 7/17 /24 from https://www.census.gov/library/visualizations/interactive/exploring-age-groups-in-the-2020-census.htm I. ln:2023.
55. U.S. Admininistration for Community Living. 2020 Profile: Hispanic Americans Age 65 and Older. Retrieved 7/7 /24 from https://acl.gov/sites/default/files/Profile%20of%20OA/HispanicProfileReport2021.pdf ln:2021.
56. Texas Legislature Online. H.B. No. 728 An act relating to the statewide interagency aging services coordinating. Retrieved 7/21 /24 from https://capitol.texas.gov/tlodocs/88R/billtext/html/HB00728E.htm. ln:2023.
57. California Department of Aging. Master Plan for Aging. Retrieved 7/21 /24 from https://www.aging.ca.gov/download.ashx?IEOrcN UV0zYXf9JtT7jkAg%3D%3D Master Plan for Aging: Third MPA Annual Report (ca.gov). ln:2021.
58. California Department of Health Care Services. Dual Eligible Special Needs Plan (D-SNP) Performance Monitoring Dashboard Report – Quarter Two 2023. Retrieved 6/24/24 from https://www.dhcs.ca.gov/services/Documents/MCOMD/D-SNP-Dashboard-O2-with-narrative.pdf. ln:2024.
59. Rote S, Angel J, Hinton L. Characteristics and Consequences of Family Support in Latino Dementia Care. Journal of Cross-Cultural Gerontology. 2019;34(4):337-354.
60. U.S. Department of Labor Women’s Bureau. Issue Brief: Older Women and Unpaid Caregiving in the United States. Retrieved 8/27/24 from https://www.dol.gov/sites/dolgov/files/WB/WB1ss ueBrief-OlderWomenAndUnpaidCaregiving.pdf. 2023.
61. National Adult Day Service Association. Choosing a Center Retrieved 7/8/24 from https://www.nadsa.org/for-caregivers/choosing-a center/. ln:2024.
62. Alzheimer’s Association. Adult Day Centers, Retrieved 7/8/24 from https://www.alz.org/helpsupport/caregiving/care-options/aduIt-daycenters. 2024.