






Impact of Pre-MET and Digital Code Blue on Cardiac Arrest Outcomes
Impact of implementing pre-Medical Emergency Team tier and digital Code Blue monitoring on cardiac arrest outcomes: A clinical audit at an Indian tertiary care center
Mehul Shah,¹ Gauri Pathare,² Chandrima Pramanik,¹ Ayesha Shaikh,³ Tushar Parmar,¹ Ketan Karigwar,¹ Rahul Pandit,¹ Kapil Joshi,⁴ Binal Mehta,⁴ Jeetendra Parihar⁴
- Department of Critical Care Medicine,
- Sir H. N. Reliance Foundation Hospital and Research Centre, Prarthana Samaj, Girgaon, Mumbai 400004, Maharashtra, India
- Sir H. N. Medical Research Society, Sir H. N. Reliance Foundation Hospital and Research Centre, Prarthana Samaj, Girgaon, Mumbai 400004, Maharashtra, India
- Department of Endocrinology, Sir H. N. Reliance Foundation Hospital and Research Centre, Prarthana Samaj, Girgaon, Mumbai 400004, Maharashtra, India
- Department of Information Technology, Sir H. N. Reliance Foundation Hospital and Research Centre, Prarthana Samaj, Girgaon, Mumbai 400004, Maharashtra, India
OPEN ACCESS
PUBLISHED: 30 November 2025
CITATION: Shah, M., et al., 2025. Impact of implementing pre-Medical Emergency Team tier and digital Code Blue monitoring on cardiac arrest outcomes: A clinical audit at an Indian tertiary care center. Medical Research Archives, [online] 13(11). https://doi.org/10.18103/mra.v13i11.7082
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i11.7082
ISSN 2375-1924
Abstract
Background: In-hospital cardiac arrest contributes significantly to inpatient mortality. Code Blue systems vary globally, and data from India are limited. Recent evidence supports integrating pre-medical emergency team (pre-MET) reduce MET call (activated via early warning scores) and Code Blue events. Our hospital is among the first in India to implement a pre-MET system. Additionally, we developed a digital platform to monitor Code Blue performance that tracks key resuscitation step timings.
Aims: To evaluate impact of pre-MET implementation on MET and Code Blue incidence, and to assess efficacy of our digital tool in enhancing response team performance and patient outcomes.
Methods: This retrospective observational study was conducted between January 2022 and May 2025 at a tertiary hospital in Mumbai, India. All adult patients experiencing Code Blue, MET, and pre-MET calls were included. Data for Code Blue events, including chest compression fraction, were collected using the digital software. Primary outcome was return of spontaneous circulation (ROSC).
Results: We analyzed 1016 Code Blue and 1332 MET/pre-MET events. Post-implementation of pre-MET criteria, pre-MET calls significantly increased with corresponding decrease in MET calls (χ²=10.98, p=0.012). With digital Code Blue monitoring, ROSC rates improved from 37.5% (2022) to 56.5% (2025), with ward-specific rates rising from 63.2% to 85.7%. Chest compression fraction improved over time, indicating enhanced cardiopulmonary resuscitation (CPR) quality.
Conclusion: Implementation of pre-MET tier facilitated early identification of clinical deterioration, reducing MET activations. Real-time digital Code Blue assessment, particularly of chest compression fraction, enhanced CPR quality. Our findings support wider implementation of structured escalation protocols and digital Code Blue monitoring to improve patient outcomes in similar healthcare settings.
Keywords
Code Blue, pre-MET, in-hospital cardiac arrest, CPR quality, chest compression fraction, ROSC, digital monitoring
Introduction
In hospitals, medical emergencies are frequent, requiring immediate and coordinated response. To facilitate quick and effective in-hospital communication, internationally recognized emergency codes, which are color-coded signals, are used to alert relevant teams to take immediate action. Code Blue (CB) is the only color code used for the same emergency case worldwide. Code Blue originated in the 1900s in Bethany Medical Center in Kansas to signal cardiac arrest. Over the years, the CB system has evolved to alert a dedicated emergency response team of in-hospital cardiac arrest (IHCA), prompting resuscitation efforts without disrupting hospital operations. Code Blue protocols often involve a wide range of personnel, including emergency physicians, intensivists, cardiologists, anesthetists, nurses, and support staff. The incidence of IHCA varies globally, ranging 1.2-10 per 1000 admissions. Majority of reports are from the UK, USA, and European nations, while Indian data are limited. Moreover, the immediate success rate of return of spontaneous circulation (ROSC) varies across the globe.
Cardiac arrest, although often perceived as a spontaneous event, is typically preceded by several signs of physiological instability. Early warning systems were introduced to help ward staff determine the need for escalation to specialist. The Modified Early Warning Score (MEWS) was designed to alert the hospital staff of clinical deterioration. Medical emergency teams (METs)/rapid response teams were introduced to respond to patients showing signs of clinical deterioration to prevent potential cardiopulmonary arrest. A MET call is activated when pre-defined physiological criteria are fulfilled or attending clinicians have concerns about a patient’s condition.
Implementation of MET has been associated with decreased incidence of cardiac arrests outside the intensive care unit (ICU) for both adult and pediatric cases. In recent years, several hospitals across the globe have adopted a pre-MET tier of rapid response system, which includes criteria that detect signs of clinical deterioration earlier than MET criteria. Depending on the degree of clinical deterioration (which is based on key parameters such as respiratory rate, oxygen saturation, blood pressure, neurological symptoms), medical emergencies can be divided into MET calls (red zone) pre-MET calls (yellow zone). Attending clinicians and nurses play a key role in identifying signs of pre-MET criteria, potentially preventing further decline in patient condition and the need for a MET call. While Australia has been an early adopter of the three-tier rapid response system (CB, MET call, pre-MET call), rapid response systems vary with institutions and countries. Moreover, the design, clinical thresholds, implementation, and impact of the pre-MET tier remain poorly characterized in published literature, particularly in Indian healthcare settings. Our hospital is one of the first few to implement the pre-MET tier (yellow zone) of rapid response in India. The pre-MET criteria empower nurses to escalate care for at-risk patients to primary physicians or MET.
Our tertiary hospital has developed and implemented an in-house digital platform to enhance the performance of rapid responders. It provides a real-time guidance during CB events and records turnaround times (TATs) for rescue steps, including initiation of cardiopulmonary resuscitation (CPR; <1 min), identification of rhythm (<3 min), first dose of adrenaline (3-5 min), and chest compression fraction (CCF; >80%). High quality chest compressions, with minimal pauses (both frequency and duration), are integral to successful resuscitation. The American Heart Association (AHA) recommends a compression rate of 100-200/min, depth of 5-6 cm, and CCF (total duration of chest compressions/total duration of Code) >80% for adults. A key feature of our software is CCF tracking during CB event, indicating the proportion of time spent performing chest compressions. This feature provides real-time CPR quality data, allowing rescuers to assess and improve performance.
The present study performed a clinical audit of CB, MET, and pre-MET calls at a tertiary hospital in India to assess rapid response team performance, determine trends, and identify areas of improvement, with the goal of improving patient outcomes. Further, it evaluated the impact of pre-MET tier implementation on the incidence of CB and MET call events. Finally, it assessed the efficacy of our digital platform in improving response team performance and patient outcomes.
Materials and Methods
STUDY DESIGN
This retrospective observational study was conducted in a tertiary healthcare hospital in Mumbai, India between January 2022 and May 2025. The primary endpoint was sustained ROSC. This study was conducted in accordance with the principles of Helsinki Declaration and Good Clinical Practice and was approved by the Institutional ethics committee (HNH/IEC/2024/OCS/CCM/154). The need for informed consent was waived considering the observational nature of the study.
STUDY DESIGN AND POPULATION
This study included all adult patients (age > 18 years) who experienced a pre-MET call, MET call, or CB event during the study duration. End-of-life patients were excluded from the study.
COMPOSITION OF MEDICAL EMERGENCY/ CODE BLUE TEAM
The hospital maintains a specialized Code Stroke MET Call team that operates continuously, ensuring round the clock availability. The team comprises three physicians with designated roles, including one member who assumes the leadership role during emergencies; two nurses who are responsible for administering medication, supervising the process, and documenting the event; and a patient care attendant who provides support by performing physical chest compressions when required. All physicians are Advanced Cardiac Life Support (ACLS) certified, while clinical hospital staff are trained in Basic Life Support (BLS) and non-clinical personnel are taught by-stander CPR.
INITIATING PRE-MET (PRE-MEDICAL EMERGENCY TEAM) AND MET (MEDICAL EMERGENCY TEAM) CALLS
Yellow-zone criteria to initiate a pre-MET call were implemented in our hospital since 2022. The nursing staff were trained to recognize signs, differentiate between pre-MET and MET calls, and initiate the calls when the respective criteria were met (Table 1). To ensure patient safety, nursing staff monitor the vital signs of all admitted patients at four-five hourly intervals throughout the day. Upon detecting deviations from expected parameters, the nurse either escalates care to primary/attending physician or on call team (yellow zone) or activates a MET (red zone), which dispatches the ICU team as appropriate. Upon activation, the MET promptly responds to the situation and performs necessary therapeutic interventions.
DATA COLLECTION
Data for all CB, MET call, and pre-MET call events were collected using the in-house digital software. All relevant staff were trained in operation of the digital software. Key variables collected included the clinical indication for the call, patient diagnosis, specific interventions administered, the patient’s disposition, TATs of the response team, including CCF, and final patient outcome. The digital platform automatically tracks the CCF in real time, enabling review of CPR quality and facilitating performance feedback.
STATISTICAL ANALYSIS
Descriptive statistics were used to summarize patient demographics, clinical outcomes, and other variables. Numerical data are presented as mean ± standard deviation (SD) or frequency and percentage. Normality of continuous data was assessed using the Shapiro Wilk test. For non-normally distributed data such as chest compression fraction (CCF), comparison of variables across years were performed using the Chi-square test or Kruskal’s test. Odds ratios (OR) with 95% confidence intervals (CI) were calculated to compare survival between sub-groups. P-value < 0.05 was considered statistically significant. All analyses were performed using the SPSS statistical software (version 29.0, IBM Corp. NY, USA).
Table 1. Criteria for MET/pre-MET call activation.
| Criteria | Temperature | RR (breaths/min) | OS (%) | SBP (mmHg) | Heart rate (bpm) | Neurology | Blood glucose (mg/dL) | Additional criteria (if applicable) |
|---|---|---|---|---|---|---|---|---|
| Yellow Zone | <35 ºC or 95 ºF | 6-10 or 25-30 | <95% on room air | <92% on 4 L O2 | 90-100 or 180-200 | 40-50 or 120-140 | Responds to voice only | <70 or >250 with no decrease in consciousness |
| Red Zone | >38.5 ºC or 101.3 ºF | <6 or >30 | <90% on room air | <92% on 5 L O2 | <90 or >200 | <40 or >140 | Responds to pain only | <60 or >300 with decrease in consciousness |
Adapted from the MEWS. MET, medical emergency team; RR, respiratory rate; OS, oxygen saturation; SBP, systolic blood pressure; GCS, Glasgow Coma Scale; U/O, urine output. Pre-MET or MET call is initiated if any one of the criteria in yellow zone or red zone, respectively, are met.
Results
PATIENT DEMOGRAPHICS
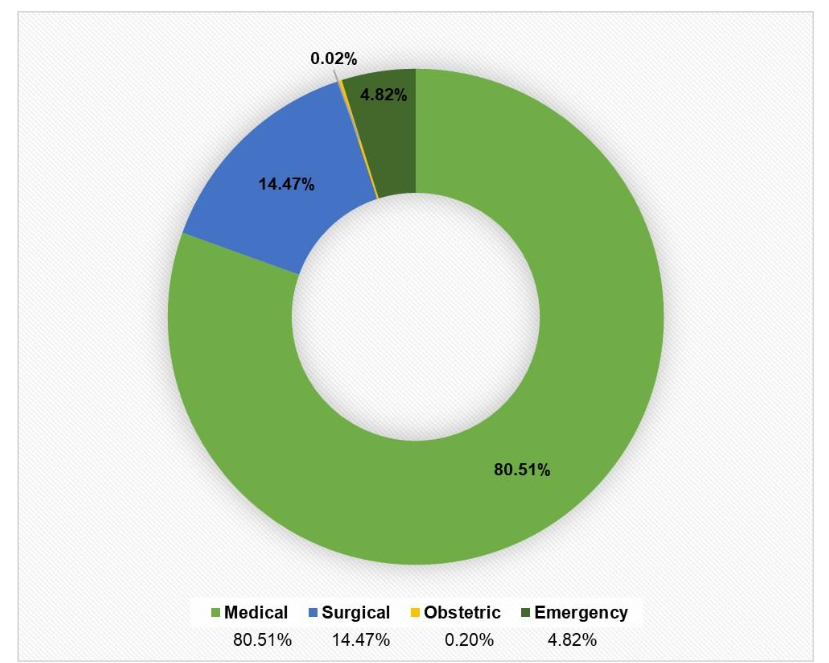
The study included at a total of 1016 CB, 855 MET, and 477 pre-MET call events. The mean age of the CB cohort was 63.9±15.4 years (minimum age, 18 years; maximum age, 99 years). Approximately 64% of the CB cohort comprised males. The age and sex trends remained the same for patients experiencing CB and MET/pre-MET call events (Table 2). Most of the patients suffering a cardiorespiratory event were medical admissions (80.51%), while 14.74% were surgical patients and only 4.82% were emergency admissions (Figure 1). Code Blue was activated in the ICU (60.13%), emergency department (ED; 20.18%), wards (7.09%), and periphery (locations other than ward, ICU, ED, operating theatre; 12.6%). MET/pre-MET calls were activated only in the wards.
INITIAL RHYTHM
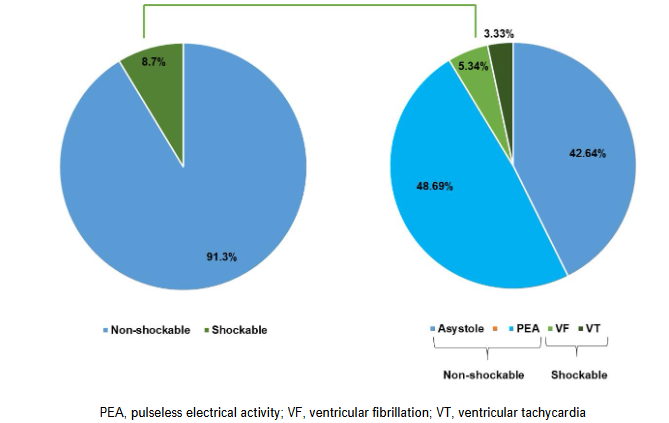
Of the 1016 patients in CB cohort, initial rhythm was accessible in 992 patients. This may be attributed to missing data owing to human error during the initial phase post-introduction of the software. Of these, initial rhythm was non-shockable in majority of the cases (91.33%). Further, asystole and pulseless electrical activity (PEA) was detected in 423 (42.64%) and 483 (48.69%) patients, respectively. The shockable rhythms ventricular fibrillation (VF) and ventricular tachycardia (VT) were detected in 53 (5.34%) and 33 (3.33%) patients, respectively (Figure 2).
Table 2. Patient demographics
| Demographic | Code Blue N=1016 | MET/pre-MET call N=1332 |
|---|---|---|
| Mean ± SD / Frequency (%) | Mean ± SD / Frequency (%) | Mean ± SD / Frequency (%) |
| Age (years) | 63.94 ± 15.38 | 62.38 ± 15.01 |
| Sex | Male 649 (63.88%) | Male 787 (59.08%) |
| Female 367 (36.12%) | Female 545 (40.92%) |
IMPROVEMENT IN CHEST COMPRESSION FRACTION (CCF)
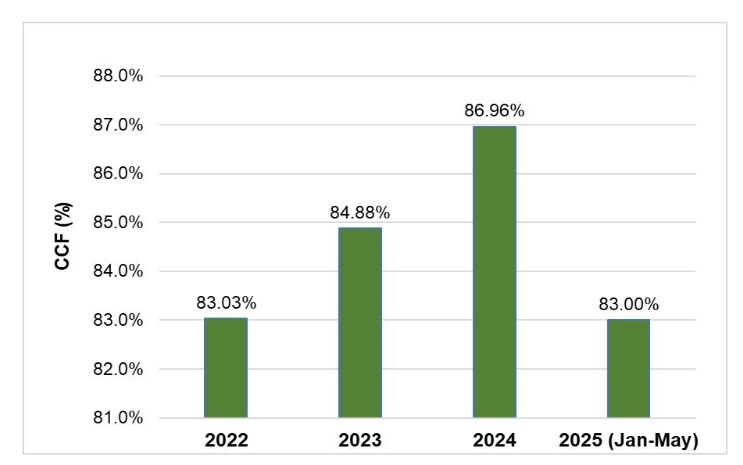
Over the study period, we observed a steady improvement in the CCF, with values increasing from 83±17% in 2022 to 87±13% in 2024 (Figure 3). This improvement corresponded with increased ROSC rates and reflects enhanced CPR quality over time. However, the difference was not statistically significant (Kruskal-Wallis test).
OUTCOMES
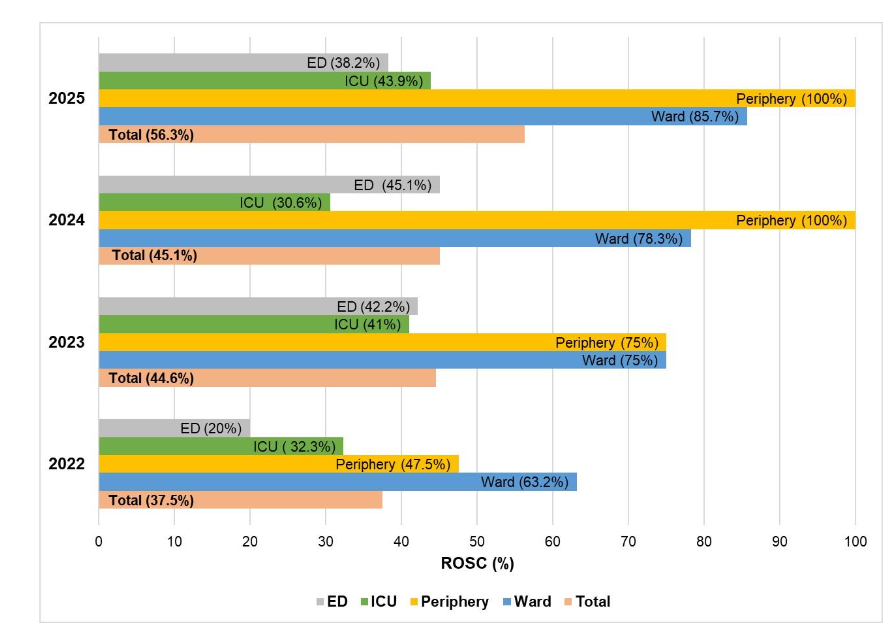
We observed an overall survival rate of 44.59% (453/1016) in our cohort. The survival rate was 58.02% (235/405) when cases from ICU were excluded and 74% (148/200) when ICU and ER cases were excluded. Considering that ICU and ER admit severe cases and that the survival in these locations may be skewed owing to other factors, we calculated ROSC rates for all locations reporting CB events. The distribution of ROSC rates over the study period is given in Figure 4. The overall ROSC rate improved from 37.5% in 2022 to 56.53% in 2025. When considering only ward cases, ROSC rates increased from 63.16% in 2022 to 75% in 2023, 78.26% in 2024, and 85.71% in 2025. Moreover, there was a statistically significant difference in survival rates across the years from 2022 to 2025 (χ²=14.68, p-0.002). We observed a high ROSC rate for CB events in the periphery, which includes outpatient department (OPD) and remote unmonitored locations such as radiology, oncology/nuclear medicine. Any emergencies in these locations are escalated as CB as per hospital policy to avoid untoward incidence, and may therefore not represent true CB events.
Because most of our cohort comprised medical admissions, we performed subgroup analysis for medical and surgical admissions. However, we did not observe a major difference in the overall survival rate between medical subgroup (45.6%) and surgical subgroup (40.14%). A comparison of survival outcomes using odds ratio analysis did not reveal a significant difference (OR=1.25, 95% CI: 0.88-1.79).
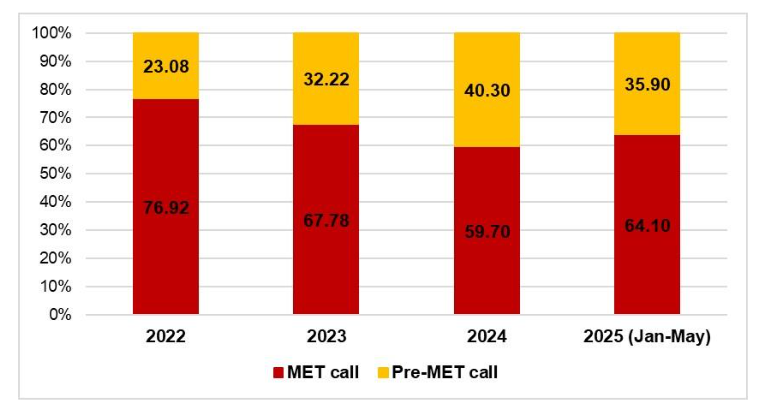
TRENDS IN MET (MEDICAL EMERGENCY TEAM) AND PRE-MET (PRE-MEDICAL EMERGENCY TEAM) CALL TRENDS
Post-implementation of Yellow-zone criteria, we observed a steady decrease in MET calls and a corresponding increase in pre-MET calls (Figure 5). The trend in the distribution of MET and pre-MET calls over the years showed a statistically significant shift (χ²=10.98, p=0.012). Interestingly, the survival to discharge in wards showed an increasing trend, with 69.23% in 2022, 76.72% in 2023, 85.55% in 2024, and 89.01% in 2025.
Discussion
In-hospital cardiac arrest (IHCA) is a major contributor to inpatient mortality worldwide. The incidence of IHCA varies among institutions and countries, ranging from 1.6 to 10 per 1000 admissions. Data on ICHA incidence in India is limited, and the incidence rate may be underreported due to lack of standardized reporting systems. A systematic review and meta-analysis of studies on IHCA, predominantly conducted in North America and Western Europe, found a pooled survival-at-discharge and 1-year survival rates of 17.6% and 13.4%, respectively. Although information on the long-term prognosis of IHCA survivors is limited, available literature suggests a poor overall prognosis with higher mortality rate, physical or neurological impairment, and poor quality of life. Therefore, management of IHCA is crucial, and healthcare institutions across the globe have implemented CB systems to rescue such patients. However, recent evidence underscores the importance of early recognition and intervention to prevent cardiac arrest. Such a proactive approach through implementation of pre-MET systems rather than a reactive approach (CB activations) can reduce the incidence of CB events, eventually improving hospital mortality and morbidity.
Code blue is a widely recognized emergency code used to signal a cardiorespiratory arrest in hospitals and is managed in accordance with international guidelines. Adherence to the American Heart Association ACLS guidelines improves ROSC rates and thereby outcomes. Although prompt activation of CB helps rescue patients suffering from IHCA by restoring spontaneous circulation, recent evidence highlights the importance of early recognition of clinical deterioration and intervention to prevent cardiac arrest. Several healthcare settings recommend the use of pre-MET call (yellow zone) criteria that empower the bedside ward nurses to escalate care for at-risk patients to primary/attending physicians or team & activate a pre-MET. Timely review and effective management of pre-MET cases may avert the escalation to a subsequent MET call. Therefore, we implemented the pre-MET call criteria in our tertiary hospital and conducted a clinical audit of CB and MET calls to evaluate its influence. A clinical audit of CB and MET calls involves systematically evaluating the effectiveness and quality of emergency responses in healthcare settings with the aim of assessing processes, identifying gaps, and strategizing improvements to ensure better patient outcomes during critical events.
We found that implementation of pre-MET call criteria led to a corresponding decrease in MET calls, indicating earlier identification and intervention for likely deteriorating patients. This trend further suggests enhanced early warning system performance and greater staff responsiveness to pre-MET (yellow zone) criteria. Moreover, we observed an increasing trend in the survival-to-discharge rate among these patients (69.23% in 2022 to 89.01% in 2025). This can be attributed to early detection of at-risk patients due to vigilance through the pre-MET (yellow zone) criteria.
To enhance the performance of rescue responders and improve patient outcomes, our hospital developed a digital platform that provides real-time aid during CB events and records TATs for the steps involved during rescue. The software, operated by the scribe nurse during a rescue event, provides invaluable assistance by indicating intervention times and tracking TATs. Moreover, the unique feature of CCF measurement optimizes CPR performance. Review of CCF data along with monthly meetings with the nursing scribers who are trained CPR coaches helped improve team dynamic as well as minimized the duration between consequent chest compressions. This eventually led to a measurable improvement in CCF values over time. To the best of our knowledge, this is the first report on the use of a digital platform to review key factors/steps during MET call/CB events in India. Review of TATs using business intelligence (BI) reports generated by the software helps assess and improve team performance, ultimately improving ROSC rates and patient outcomes. Indeed, we observed an increasing trend in CCF over the years, suggesting the usefulness of the digital platform in improving CPR performance. This was supported by an increase in overall ROSC rates from 37.5% in 2022 to 56.3% in 2025. The low overall ROSC rates can be attributed to events in ICU and ED, where the patient condition is severe and outcome is poor. In these locations, patient condition rather than the performance of the CB team is the major factor influencing ROSC. In our cohort, the ROSC rates in the wards (excluding CB events in these two locations) increased from 63.16% in 2022 to 85.71% in 2025. Furthermore, ROSC rates vary globally, with low-income countries such as Kenya and Uganda reporting only 29.2% and 7.4 %, respectively, while middle and high-income countries reporting comparatively higher rates. The overall ROSC rates in the present study were comparable to those reported in urban tertiary hospitals in Indonesia (38-46%), Turkey (45.5%), UAE (40%), as well as a previous study from India (44.1%). Notably, Thailand (67.3%) and USA (61.7%) reported higher ROSC rates.
Beyond the technological innovation, the success of such systems depends heavily on team culture, training, and workflow integration. A realist review of early warning and rapid response systems found that desired outcomes are more likely when ward staff have appropriate escalation protocols and multidisciplinary, competency-based education. In our setting, the integration of a digital platform, combined with quarterly mock drills and trained scribe-nurses, may have strengthened team responsiveness and empowered frontline staff. Integrating this digital workflow with the electronic health record systems of hospitals could further augment scalability, automating escalation triggers and providing real-time feedback to relevant teams.
Another factor that influences ROSC rates is the initial rhythm during cardiac arrest. Several studies report a positive association between initial shockable rhythm and increased survival compared to an initial non-shockable rhythm. A systemic review found the most common initial rhythms in IHCA to be asystole and PEA. Another study in the USA reported that PEA and asystole together account for 81% of initial rhythms. Consistently, the majority of our CB cohort had non-shockable rhythm (91.33%). We observed asystole in 42.64% of our cohort, followed by PEA in 48.69%; shockable rhythms were observed in only 8.67% of the cohort.
In addition to clinical outcomes, proactive surveillance and escalation systems have economic implications. For example, a cost effectiveness study of a rapid response system in a tertiary care hospital in Barcelona found that implementation of the RRS was less costly and more effective compared with standard care, resulting in incremental cost saving over a period of five years. This highlights how early intervention strategies (such as pre-MET implementation) not only potentially improve patient outcomes but may reduce resource utilization by averting cardiac arrests, ICU transfers and prolonged hospitalization. Given the high costs associated with IHCAs (owing to intensive interventions, morbidity, and prolonged length of stay), implementing a pre-MET tier could offer significant resource and cost savings, making it a valuable investment for hospitals while also alleviating the potential financial burden on patients.
Global consensus suggests a higher risk of IHCA with age. A recent study in Asian population found patients 65 years to be at a higher risk of IHCA. A study in Indian population reported mean age of such patients to be 56 years, while another reported a majority of their cohort to be over 60 years of age. Consistent with these trends, our study cohort had a mean age of approximately 64 years, with the majority being males. There are discrepancies in reported literature on the influence of sex on IHCA. While several studies report a higher incidence in males, few report a higher incidence in females. Another study reported female sex to be independently associated with approximately two-fold higher in-hospital mortality rate. However, the influence of sex on IHCA remains unclear and warrants further investigation.
A major strength of our tertiary care center is that all rescue responders are trained in ACLS protocols, with refresher courses conducted annually and mock drills conducted quarterly. Further, all medical as well as non-medical staff are trained in BLS. This significantly improves the success rate of resuscitation as rescue operations can be commenced immediately upon detection of a cardiac event, even before the arrival of the MET/CB team.
A limitation of the study is its single-center design, which may limit the generalizability of the findings. We propose implementation of yellow zone criteria in healthcare institutions across the nation. Such multi-center studies will help validate our findings. Further, although the use of digital software facilitated real-time monitoring of CPR quality, reliance on manual input may have introduced the risk of human error in data entry.
The introduction of a digital platform in our setting has proven to be a pivotal step in enhancing operational efficiency and patient care. The successful integration of this platform reflects not only the potential for technological advancement but also the importance of seamless workflow adaptation. Future directions of this initiative involve the broader implementation of this digital platform across various hospitals throughout India. Such multi-center expansion will provide an opportunity to assess the platform’s effectiveness in diverse clinical environments, enabling a comprehensive evaluation of its impact on patient outcomes, workflow efficiency, and overall healthcare delivery. Moreover, evaluating its scalability, user acceptance, and clinical utility, will provide critical insights that will drive further refinement of the platform. The goal is to establish the digital platform as a standardized tool across hospitals, optimizing both clinical practice and patient care.
Conclusion
The present study revealed that structured escalation protocols and staff training improved the performance of rescue responders and enhanced patient outcomes. The introduction of yellow zone criteria facilitated earlier identification of at-risk patients, allowing timely intervention and potentially preventing the need for CB and MET calls. The successful implementation of yellow zone criteria in our study underscores the importance of proactive, continuous monitoring and prompt response. The use of a digital CB platform assists rescue by providing real-time guidance, thereby enhancing the efficiency and effectiveness of CB and MET responses. Moreover, it facilitates accurate documentation of events, which can be reviewed through the business intelligence report, providing valuable insights for continuous improvement.
Conflict of interests:
The authors have no conflicts of interest to declare.
Authorship:
Mehul Shah: Conceptualization, Methodology, Validation, Investigation, Writing – Review & Editing, Supervision, Project administration; Gauri Pathare: Formal analysis, Writing – Original Draft, Writing – Review & Editing, Visualization; Chandrima Pramanik: Validation, Investigation, Data Curation, Writing – Review & Editing; Ayesha Shaikh: Validation, Investigation, Data Curation, Writing – Review & Editing; Tushar Parmar: Methodology, Validation, Investigation, Writing – Review & Editing; Ketan Kargirwar: Methodology, Validation, Investigation, Writing – Review & Editing; Rahul Pandit: Methodology, Validation, Writing – Review & Editing, Supervision; Kapil Joshi: Methodology, Software, Writing – Review & Editing; Binal Mehta: Methodology, Software, Writing – Review & Editing; Jeetendra Parihar: Methodology, Software, Writing – Review & Editing.
References:
- Sahin KE, Ozdinc OZ, Yoldas S, Goktay A, Dorak S. Code Blue evaluation in children’s hospital. World J Emerg Med 2016;7:208 12. doi:10.5847/wjem.j.1920-8642.2016.03.008.
- Penketh, J., Nolan, J.P. In-hospital cardiac arrest: the state of the art. Crit Care 2022;26: 376. https://doi.org/10.1186/s13054-022-04247-y.
- Chan PS, Tang Y; American Heart Association’s Get With the Guidelines®‐Resuscitation Investigators. Risk-Standardizing Rates of Return of Spontaneous Circulation for In-Hospital Cardiac Arrest to Facilitate Hospital Comparisons. J Am Heart Assoc 2020;9: e014837. doi:10.1161/JAHA.119.014837
- Jones DA, DeVita MA, Bellomo R. Rapid-response teams. N Engl J Med 2011;365:139 46.
- Devita MA, Bellomo R, Hillman K, et al. Findings of the first consensus conference on medical emergency teams. Crit Care Med 2006;34:2463 78.
- Audit Commission. Critical to success: the place of efficient and effective critical care services within the acute hospital. London, UK; 1999.
- Gardner-Thorpe J, Love N, Wrightson J, Walsh S, Keeling N. The value of Modified Early Warning Score (MEWS) in surgical in-patients: a prospective observational study. Ann R Coll Surg Engl 2006;88: 571 5. doi:10.1308/003588406X130615
- Sprogis SK, Currey J, Jones D, Considine J. Use of the pre-medical emergency team tier of rapid response systems: A scoping Review. Intensive Crit Care Nurs 2021;65:103041. doi:10.1016/j.iccn.2021.103041
- Chan PS, Jain R, Nallmothu BK, Berg RA, Sasson C. Rapid response teams: a systemic review and meta-analysis. Arch Intern Med 2010;170:18 26.
- De Jong A, Jung B, Daurat A, et al. Effect of rapid response systems on hospital mortality: a systemic review and meta-analysis. Intensive Care Med 2016;42:615 7.
- Maharaj R, Raffaele I, Wendon J. Rapid response systems: a systemic review and meta-analysis. Crit Care 2015;19:254.
- Subbe CP, Kruger M, Rutherford P, Gemmel L. Validation of a modified Early Warning Score in medical admissions. QJM 2011;10:521 6.
- Jones D, Orosz J, Psirides A, Pilcher D. Potential metrics for rapid response systems in Australia and New Zealand. Crit Care Resusc 2023;25:116-7. doi:10.1016/j.ccrj.2023.06.006
- American Heart Association. High-quality CPR performance metrics [Internet]. American Heart Association; [cited 2025 Jun 17]. Available from: https://cpr.heart.org/en/resuscitation-science/high-quality-cpr
- Schluep M, Gravesteijn BY, Stolker RJ, Endeman H, Hoeks SE. One-year survival after in-hospital cardiac arrest: A systematic review and meta-analysis. Resuscitation 2018;132:90 100. doi:10.1016/j.resuscitation.2018.09.001
- Ocen D, Kalungi S, Ejoku J, et al. Prevalence, outcomes and factors associated with adult in hospital cardiac arrests in a low-income country tertiary hospital: a prospective observational study. BMC Emerg Med 2015;15:23. doi:10.1186/s12873-015-0047-0
- Nallamothu BK, Greif R, Anderson T, et al. Ten steps toward improving in-hospital cardiac arrest quality of care and outcomes. Circ Cardiovasc Qual Outcomes 2023;16:e010491. doi:10.1161/CIRCOUTCOMES.123.010491
- Spearpoint KG, Gruber PC, Brew SJ. Impact of the immediate life support course on the incidence and outcome of in-hospital cardiac arrest calls: An observational study over 6 years. Resuscitation 2009;80:638 43.
- Jones D. The medical emergency team – current status and future directions: a perspective for acute care physicians. Intern Med J 2023;53:888 91.
- Abu-Jeyyab M, Al-Jafari M, El Din Moawad MH, et al. The role of clinical audits in advancing quality and safety in healthcare services: A multiproject analysis from a Jordanian hospital. Cureus 2024;16: e54764.
- Ngunga LM, Yonga G, Wachira B, Ezekowitz JA. Initial rhythm and resuscitation outcomes for patients developing cardiac arrest in hospital: Data from low-middle income country. Glob Heart 2018;13:255 60. doi:10.1016/j.gheart.2018.07.001
- Leona DF. Prevalence and determinants of return of spontaneous circulation (ROSC) in in-hospital cardiac arrest patients in Indonesia: A systematic review. International Journal of Research Publication and Reviews 2024;5:2354 8.
- Topeli A, Cakir B. Evaluation of the blue code system established in the health campus of a university hospital. Turk J Emerg Med 2020;21:149. doi:10.4103/2452-2473.301912.
- Alao DO, Mohammed NA, Hukan YO, et al. The epidemiology and outcomes of adult in-hospital cardiac arrest in a high-income developing country. Resusc Plus 2022;10:100220. doi:10.1016/j.resplu.2022.100220.
- Hazra D, Nekkanti AC, Jindal A, et al. Code blue: Predictors of survival. J Anaesthesiol Clin Pharmacol 2022;38:208 14. doi:10.4103/joacp.JOACP_327_20.
- Rattananon P, Tienpratarn W, Yuksen C, et al. Associated factors of cardiopulmonary resuscitation outcomes; a cohort study on an adult in-hospital cardiac arrest registry. Arch Acad Emerg Med 2024;12:e30. doi:10.22037/aaem.v12i1.2227.
- Cagino LM, Moskowitz A, Nallamothu BK, McSparron J, Iwashyna TJ; American Heart Association’s Get With The Guidelines-Resuscitation Investigators. Trends in return of spontaneous circulation and survival to hospital discharge for in-intensive care unit cardiac arrests. Ann Am Thorac Soc 2023;20:1012 9. doi:10.1513/AnnalsATS.202205-393OC.
- McGaughey J, O’Halloran P, Porter S, Blackwood B. Early warning systems and rapid response to the deteriorating patient in hospital: A systematic realist review. J Adv Nurs 2017;73:2877 91. doi:10.1111/jan.13398.
- Han Y, Hu H, Shao Y, et al. The link between initial cardiac rhythm and survival outcomes in in-hospital cardiac arrest using propensity score matching, adjustment, and weighting. Sci Rep 2024;14:7621. doi:10.1038/s41598-024-58468-y.
- Grunau B, Reynolds JC, Scheuermeyer FX, et al. Comparing the prognosis of those with initial shockable and non-shockable rhythms with increasing durations of CPR: Informing minimum durations of resuscitation. Resuscitation 2016;101:50 6. doi:10.1016/j.resuscitation.2016.01.021.
- Allencherril J, Lee PYK, Khan K, Loya A, Pally A. Etiologies of In-hospital cardiac arrest: A systematic review and meta-analysis. Resuscitation 2022;175:88 95. doi:10.1016/j.resuscitation.2022.03.005.
- Andersen LW, Holmberg MJ, Berg KM, Donnino MW, Granfeldt A. In-hospital cardiac arrest: A review. JAMA 2019;321:1200 10.
- Muñoz-Rojas G, García-Lorenzo B, Esteve D, et al. Implementing a Rapid Response System in a tertiary-care hospital. A cost-effectiveness study. J Clin Monit Comput 2022;36:1263 9. doi:10.1007/s10877-022-00859-5.
- Chang FC, Hsieh MJ, Yeh JK et al. Longitudinal analysis of in-hospital cardiac arrest: trends in the incidence, mortality, and long-term survival of a nationwide cohort. Crit Care 2025;29:41 doi:10.1186/s13054-025-05274-1.
- Monangi S, Setlur R, Ramanathan R, Bhasin S, Dhar M. Analysis of functioning and efficiency of a code blue system in a tertiary care hospital. Saudi J Anaesth 2018;12:245 9.
- Jayasingh IA, Margos RA, Philip S. A clinical audit to assess the adherence of the Code Blue team to advanced cardiac life support protocol and its effect on the patient outcome in a tertiary care hospital in Kochi, Kerala. Indian J Respir Care 2018;7:46 9.
- Al-Dury N, Rawshani A, Israelsson J, et al. Characteristics and outcome among 14,933 adult cases of in-hospital cardiac arrest: A nationwide study with the emphasis on gender and age. Am J Emerg Med 2017;35:1839 44. doi:10.1016/j.ajem.2017.06.012.