

Multifaceted Pilonidal Disease: Clinical Insights and Treatments
The Multifaceted Pilonidal Disease: A Review of this Dermatological Machiavellian!
Dr. Uwais Riaz Ul Hasan, M.Med 1; Dr. Khathija Hasan, M.Med 2; Dr. Shehla Riaz Ul Hasan, Phd 3; Dr. Shehab Yousef Buhulaigah 4, Dr. Abdul Rahman Al Gannam 4; Dr. Ammar AlSulaiman 4; Dr. Aissa Saidi 5; Dr. Amith Ibrahim 5; Dr. Ridha Essa Ali Alali 4; Zainab Essa Alhasawi 6; Raid Allowaymi 6; Waleed AlAbood 6; Jaffer Ali AlOthman 6; Ali Abdullah Mohammed AlShagag 6; Fatimah Naji NafaAlshakus 6; Maryam Mohammed AlMutawa 6; Omnia Ahmed Alturaifi 6; Hiba Abdullah AlSaleh 6
- Consultant General Surgeon Al Omran General hospital Al Hasa
- Anesthetist RIPAS Hospital Brunei Darussalam
- Al Omran General Hospital
- Surgeon Al Omran General Hospital
- Anesthetist Al Omran General Hospital
- Anesthesia Al Omran General Hospital
- Anesthetist, Department of Anesthesia, R.I.P.A.S Hospital, Bandar Seri Begawan B.A/T/2, Ministry of Health, Brunei. Formerly USM, Malaysia.
[email protected]
Correspondence:
[email protected]
OPEN ACCESS
PUBLISHED: 30 September 2025
CITATION: Ul Hasan, UR., Hasan, K., et al., 2025. The Multifaceted Pilonidal Disease: A Review of this Dermatological Machiavellian! Medical Research Archives, [online] 13(9). https://doi.org/10.18103/mra.v13i9.6768
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i9.6768
ISSN 2375-1924
Abstract
Chronic Skin lesions are characterized by signs of inflammation the nature and duration of these illness affects the disease outcome. Pilonidal Disease (PD) is a chronic dermatological disorder Characterized by formation of regional follicles abscesses that progress to fistulas & Scars over the period of years. The Clinically myriad features of Pilonidal Disease (PD) presentation depends upon the site and the anatomical location of the disease process. The Clinical features of Axillary pilonidal disease is different from the Mammary pilonidal disease. The spectral clinical presentation for the groin, genitals & Umbilical pilonidal disease is even more diverse. Hence the patients end up to different specialities like medicine, dermatology, gynaecology, surgery, cosmetic surgery even under infection control mislabelled as tuberculosis and actinomycosis. The disease takes a toll on subjects with chronic Pain & foul-smelling discharge as they continue to live life bondaged to dressings. Over time the individual develops a negative impact on their psyche socially it affects their relationships even takes a toll on their caregivers. The differential diagnosis associated with Pilonidal disease is momentous this dermatological condition has a multifaceted presentation all depending on the stage & the anatomical zone of presentation. It is easily passed off initially as an epidermoid cyst or an abscess, furuncle, carbuncles, Staphylococcal skin infections as pyoderma, Bartholin cysts Ano Cutaneous Crohn disease even as Hidradenitis suppurativa (HS). The controversies that were associated with its origins may have been resolved but optimal treatment modalities that reduce recurrences continue to be debatable.
Keywords
Sacrococcygeal pilonidal sinus, abscess, recurrent pilonidal disease, Limberg flap, dermatological Machiavellian.
Introduction
Pilonidal disease was first reported by Herbert Mayo a British Surgeon (1833) 1, as a congenital condition with sinus containing hair follicles located in the sacrococcygeal region of a female subject. The term pilonidal was coined by Richard Hodges as derived from the Latin pilus referring to hair and nidus nest. Hodges was a proponent of the congenital theory for pilonidal sinus disease. His belief was three factors were essential for the development of sacral Pilonidal disease, the congenital coccygeal dimple, the presence of abundant hair, and poor hygiene. The term pilonidal cysts by itself is a misnomer the cyst wall is not lined with squamous epithelium but is comprised of vascular pyogenic granulation tissue. The work of Patey and Scarff in 1946 has demonstrated that this granulomatous tract is secondary to free hair follicle penetration, thereby validating the acquired nature theory of pilonidal disease and hence it is the most widely held view today. The controversies related to its origin may have been resolved as of today, but the condition continues to be shrouded in controversies as for instance there is no universally accepted modality of treatment stage wise that reduces recurrences among Surgeons worldwide. Even more fascinating myriad spectrum of clinical of clinical presentation in diagnosing this disease condition as depending on stage of presentation & the anatomical region of body involved the clinical features vary. The result is a multifaceted clinical spectrum of differential diagnosis, the consequences, a delay in surgical consultation leading to an upgrading of the Clinical disease as it progresses to chronic fistula formation with extensive scarring. This review was undertaken as an attempt to revisit the controversies that has historically plagued Pilonidal Disease and to highlight the importance of an accurate early clinical diagnosis with early involvement of the surgical team to optimize outcome.
Clinical Presentation
Pilonidal disease is seen in healthy obese adolescents and adults. It rarely begins before puberty. The onset is gradual, the earliest regional sign being erythema followed by pain. The commonest region affected is the axilla, the groin including genitals, the umbilicus, sacrococcygeal region, the mammary folds, and the intertriginous digits of the hands.


The diagnosis is primarily clinical with three Cardinal features to conclude a primary diagnosis of Pilonidal disease.
- Typical lesions pits, Sinuses, fistulas
- Characteristic distribution &
- Recurrence & or Scars.
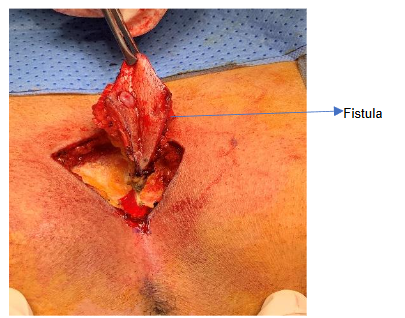
Typical lesions include a Painful and tender erythematous papule, nodules or abscesses smaller or larger than 1 cm in diameter with discharging dermal sinuses or scars. Distribution: Axilla, genitofemoral area, perineum, umbilicus, hands gluteal area and inframammary region even genitals. Depending upon the duration of the illness the abscesses lead to sinuses & fistula that are either dormant or actively discharging malodorous pus. The term Chronic pilonidal disease is used for patients that have undergone at least one pilonidal abscess drainage procedure and continue to have a residual pilonidal sinus tract clinically seen as discharging pus. Recurrent disease is referred to disease process occurring after a period of healing & is characterised by new pit formation. It is not unusual to see patients living with this condition for five to ten years. The cost of annual dressing per subject as per a Swedish study to be EUR 6222 per patient with a recurrence rate of 32% at 5 years2.
The Clinical Scoring systems for Pilonidal Disease are of two types traditional and Modern classification.
Tezel Classification
- Type I-Asymptomatic Sinus
- Type II-Acute Abscess
- Type III-Chronic Symptomatic Disease (Navicular Area)
- Type IV-Chronic Symptomatic Disease (Above Navicular Area)
- Type V-Recurrent Disease
Navicular area: If the buttocks are pushed together, the outer lines of contact represent the lateral edges of the natal cleft. The inferior extent is the posterior border of the anal triangle, which has its tip at the apex of the coccyx and its base between the ischial tuberosities.
Guner Classification
- Stage I-Solitary Midline Pit
- Stage II-Multiple Midline Pits
- IIa < 3 Pits
- IIb > 3 Pits
- Stage III-Midline Pit Lateral Extension (Unilateral Direction)
- Stage IV-Midline Pit Lateral Extension (Multi Directional)
- (Stage R: Recurrent PSD)
Lapsekili Anatomical Classification
Primarily Pits that lie within 1cm of Intergluteal line. Atypical Pits lie Outside this Intergluteal line (inactive disease process). Complex Pits Lie along an imaginary line extending from anal canal to coccyx.
Dolls Classification
- Type 1: Characterized by only midline pits or sinuses.
- Type 2: Involves midline disease with secondary sinuses/abscess/scars.
- Type 3: Any midline or secondary disease extending below the tip of the coccyx.
- Type 4: Any disease after treatment with definitive intent (recurrence).
Karkas Classification
- Type 1.Intergluteal midline Sulcus
- Type 2. Gluteal Region.
- Type 3.Lumbar Region /Perianal Region.
Chavoin Anatomical type classification
Pits or sinuses that are midline or lateral to natal cleft.
- Type 1. Primarily Midline & or Lateral sinuses
- Type 2. Recurrent Disease process.
Irkörücü Anatomical type classification
- Type I pits along the natal cleft,
- Type II pits either one side of natal cleft,
- Type III pits on both sides,
- Type IV Multiple pits on/either side the natal cleft Complex disease
- Type V Recurrent disease.
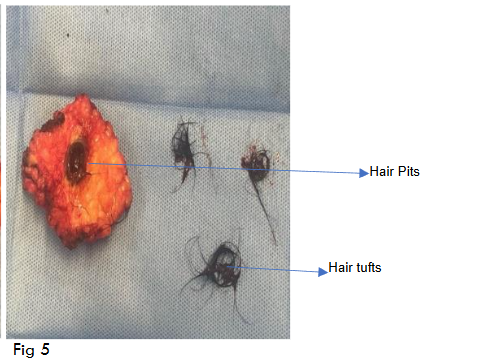
Hair Pits Hair tufts
Awad Scoring Criteria
Awad Scoring Criteria utilizes demographic and local disease characteristics.
- Sex
- Weight
- Hirsute (hairiness)
- Sinus characteristics (number, site, size, recurrence, and duration of disease)
Treatment Decision based on total score that is Assigned into A, B, or C category.
- Group A: (scores 8-10) local excision/primary closure.
- Group B: (scores 11-13) local excision/primary closure.
- Group C: (scores 14-16) flap procedure.
Modern scoring is the PITSTOP Scoring system that is practical & has gained popularity. This PITSTOP Study refers to Pilonidal Sinus Treatment Studying the Options, A prospective cohort study proposed International Pilonidal Sinus Society (IPS) Berlin 2017 classification.
- Type 1: Midline pit or sinuses
- Type 2: Midline disease with secondary sinuses or abscess or scars
- Type 3: Midline disease with secondary extension below the tip of the coccyx
- Type 4: Previous disease treated with definitive intent.
It is clearly evident the Clinical spectrum, Differential Diagnosis, even Scoring Systems are myriad when dealing with Pilonidal Disease.
Discussion
The estimated incidence is 26 per 1,00,000 people in US. In the acute stage it presents as an infected cyst or abscess with discharging active tracts. In the later stages it appears as dormant midline natal pit openings in case of sacral pilonidal disease or as sinus and fistulas at other anatomical regions over the body. Initial presentation as a painful condition seen among those aged 15-30 years. The male-to-female ratio is 3:1. This disease process is considered a chronic inflammatory state characterized by a foreign body reaction secondary to repeated micro trauma & hair penetration. The maceration of the skin promotes infection in an anaerobic environment. The result is a sinus formation with hair studded pits aligned along the midline. These pits in sacral pilonidal disease are stretched out epidermal hair follicles that measure 1-3mm in size. The pits contain the loose hair sans the follicle component that act like ba. The pits contain the loose hair sans the follicle component that act like barbs that are drilled, propelled & finally driven into the subcutaneous tissues along tracts and find their final resting place in pits. The entry is ‘one way’ tip first thereby preventing them from expulsion this has been confirmed using light microscopy. It is this orientation of the hair that motivates them to be steered deeper into the subcutaneous tissue. The mechanism proposed is vacuum forces created secondary to a deep anatomical natal cleft. This suction draws hair and debris into the midline pits. During standing and subsequent sitting the bones lift away initially pulling away from soft tissues creating a vacuum effect. Thus a subcutaneous vacuum is formed both during repeated standing and sitting position. In sitting, the pilonidal openings are pushed to close and the cavity is compressed, creating pressure that drives contents through fat to eventually rupture through sacral skin as secondary openings. The final resting place of these barbed hair are in pits. The entry is ‘one way’ tip first thereby preventing expulsion; this has been confirmed using light microscopy. It is this orientation of the hair that motivates them to be steered deeper into the subcutaneous tissue. The mechanism has been proposed is vacuum force created along with a negative suction created by a deep natal cleft. This suction draws hair and debris into the midline pits. During standing and subsequent sitting the bones lift away initially pulling away from soft tissues creating a vacuum effect. This subcutaneous vacuum is formed both during repeated standing and sitting position. In sitting, the pilonidal opening is pushed closed and the cavity is compressed, creating pressure that drives contents through fat to eventually rupture through sacral skin as secondary openings.
The race, ethnicity, coarseness, and the morphological pattern of the hair type (straight curled or kinked) including the medullation are important factors influencing both the development and persistence of chronic pilonidal disease. The Caucasians therefore are more susceptible to development of this disease when compared to other races as the volume of sweat and the number of sweat glands are more in the former than those of African or Asian descent. The Pilosebaceous unit is an apocrine apparatus. The cystic hair pit inflammation entraps commensal microbes subsequent to inflammation that progresses over time to rupture into the dermal skin. This inflammation at times triggers an exaggerated response of the cutaneous innate immune system. Whether this auto inflammatory response is predominantly an immune-mediated disease or a primary infectious disease continues to be debatable. A multitude of Complex factors such as Obesity, the hair type & pattern distribution, genetics, family history, innate immune response to inflammation are decisive in the final outcome of this disease condition. Primary canals are formed as extensions of these hair pit cavities and are lined by squamous cells that begin from the sinus orifice in the skin. Posterior to these primary canals are secondary canals that arise as side extensions. The secondary canals are lined by granulating tissue. The abscess formation takes place in secondary canals. Analysis of the nature & type of the hair have revealed that hair from the upper torso and scalp can be found as components in these hair pits! It is repeated suction from an anatomical deep natal cleft that has been proposed as the cause for vacuum forces with negative suction that draws hair and debris into the midline pits. The reason for the chronicity of this clinical disease is the colonization of the primary and secondary canals with anaerobic bacteria. In a hypoxic environment collagen synthesis is triggered and it is this excess collagen accumulation that retards healing. The end result of this relapsing inflammation is formation of sinuses & fistulas with chronic scarring. Abscesses with Loose hairs are the primary components of the primary canal and secondary canals along with Keratin flakes & hemosiderin-stained macrophages. These loose hairs accumulate in time to form tufts of hair. The final result of this relapsing inflammation is formation of chronic sinuse & fistulas culminating in chronic scarring.
Interestingly the direction of growth of the hair follicle serves as a predictor of sinus tract direction in 90% of times. Hence the sinus tracts are located cephalad in direction indicating tracking follicle ought to lie 5-8 cm from the anus. Rarely should the sinus be located caudally, the tracking follicle will in such cases lie 4-5 cm from the anal verge. If pilonidal sinus tracts encroach onto the coccyx bone, coccygeal osteomyelitis develops as a complication. The longer the duration of the disease the larger the accumulated hair in the canals. A sacral coccygectomy with Musculo cutaneous flap closure is the procedure of choice cases with osteomyelitisure of choice cases with osteomyelitis.
Prevention by Hygiene & Shaving
The Armstrong and Barcia hypothesis (1994) Habitual Wide, meticulous shaving is superior & equal to surgical therapy. Especially in at risk individuals such as the morbid obese, hirsute and those with poor personal hygiene. There is however no consensus on the timing and frequency of shaving whether weekly or monthly. The role of hygiene in sacral pilonidal disease is imperative not only as a preventive measure but in the post operative period as it continues to be a decisive risk factor affecting outcome thereby reducing recurrences. Especially in at risk individuals such as the morbid obese, hirsute and those with poor personal hygiene, there is however no consensus on the timing and frequency of shaving whether weekly or monthly. The role of hygiene in sacral pilonidal disease is imperative not only as a preventive measure but in the post operative period as it continues to be a decisive risk factor by affecting outcome and reducing recurrences.
Role of Surgery
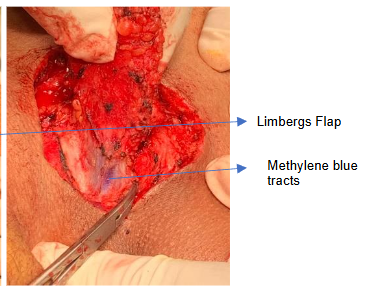
The Surgical option is most valuable for chronic recalcitrant & recurrent Pilonidal disease albeit there is no single universally accepted surgical procedure stage wise worldwide with zero recurrences. The Principle for surgical closure option techniques is based on the “Reconstruction Ladder” principle viz The use of simple procedure to be considered first followed by an increasing complex procedure in a step ladder fashion meaning the initial choice for closure of defect is skin graft, followed by a local transpositional or rotational flap followed by increasing complex procedures like a free flap & finally a composite Allografts for closure of wound. The current accepted surgical procedures in the management of pilonidal disease include simple drainage, deroofing of skin tissue, curettage of the pilonidal sinus disease, healing by secondary intension, sinusectomy, reconstructive procedures like karyadakis flap, limbergs flap, Bascom I & II procedure. Overall, the recurrences are reduced with flap procedures especially if intraoperative methylene dye is utilized to localize tracts during surgery. With radical excision and flap covers, the disease recurrence is reported to be 33%. A metaanalysis of RCT comparing different techniques for closure among flaps Karydakis/Bascom versus Limberg found No difference in recurrence or wound complications rate but concluded midline primary closure ought to be abandoned and off line line closures are the preferred approaches. Today Minimally invasive options like endoscopic sinus treatment and video assisted ablation are in fashion. Other Modern minimally invasive options include the use of Platelet-rich plasma derived from centrifuged autologous blood it contains a high concentration of platelets and growth factors. These procedures appear promising but the long term recurrence rates with these MIS procedures awaits to be seen.
Minimally Invasive Surgery (MIS) & LASER
MIS Endoscopic pilonidal sinus treatment (EPSiT) by Meinero in 2014 along with Video Assisted Ablation of Pilonidal Sinus (VAAPS) by Milone are minimally invasive techniques that are new in the management of pilonidal sinus disease, the rate of recurrences and long term evidence based studies are awaited & will determine the outcome of these MIS procedures. Laser treatment using Nd:YAG for hair removal has been suggested as an alternative to shaving. Laser epilation has been used in pilonidal disease with mixed results. The overall recurrence rate for 60 patients treated with laser therapy as an adjunct to surgery was found to be 13.3%. Disadvantages included Pain, Cost, multiple treatment sessions and rashes that were seen in up to 40% of patients. New modifications include the SiLaC procedure Sinus Laser assisted Closure and SMILE procedure Sinus Pilonidal Minimally Invasive Laser Excision.
Chronic Neglected Pilonidal Disease
There is a risk for Malignant transformation in Chronic discharging pilonidal disease if neglected and left untreated for a prolonged period of time can transform into malignancy. The first reported case was by Wolff H in 1900. The most frequent histiological tumor type is squamous cell carcinoma. The treatment following the development of malignancy is challenging and requires MDT involvement for optimal outcomes. The single most effective surgical procedure that can be universally accepted for the management pilonidal disease does not exist! And incites debates worldwide. The long term outcome of newer Centrifuged Autologus Platelet-rich plasma that contains a high concentration of platelets and growth factors are eagerly awaited.
Conclusion
The challenges facing the clinician arise from not only arriving at a definite diagnosis of Pilonidal disease amid a multitude of mimic differential list as well as in the choice of an appropriate surgical technique that reduces recurrences. The Surgical fraternity worldwide continues to be in debate as regards the optimal Universal Surgical modality, stage wise as it continues to be shrouded in controversies! The aim of any modality of therapy should not only be a resolution of disease with cure but ensuring a dressing free Quality of life. This Multifaceted Machiavellian will continue to be a formidable ally among clinicians worldwide.
Reconnaissance
Concept & Design
Supervision Approval of Manuscript
Data Acquisition
Data Analysis with Interpretation
Critical Review
Administrative Technical Editor
Sourire en Signe de Reconnaissance to Dr Khathija Hasan for review & final editing this manuscript.
Orchid 1 Https://orchid.org/0000-0003-1195-9383
Orchid 2 Https://orchid.org/0000-0003-3420-20413
References
-
- Buie LA. Jeep disease. South Med J. 1944;37:103–109.
- Khodakaram, K., Stark, J., Höglund, et al, (2017). Minimal excision and primary suture is a cost-efficient definitive treatment for pilonidal disease with low morbidity: a population-based interventional and a cross-sectional cohort study. World journal of surgery, 41, 1295-1302.
- Tezel E (2007) A new classification according to navicular area concept for sacrococcygeal pilonidal disease. Colorectal Dis [Internet]. 9(6):575–6.
- Guner A, Cekic AB, Boz A, et al. A proposed staging system for chronic symptomatic pilonidal sinus disease and results in patients treated with stage-based approach. BMC Surg. 2016 Apr 16;16:18.
- Lapsekill E, Coskun M, Oztas M, et al (2013) A classification proposal for the sacrococcygeal pilonidal sinus disease (SPSD). Eur Surg Res [Internet]. 50(SUPPL.1):144.
- Doll D, Vassiliu P (2018) Another pilonidal classification—PLLATIN. Pilonidal Sinus J [Internet]. 4(1):1–3.
- Karakaş DÖ, Yılmaz İ, Hazer B, et al (2017) Congress of Turkish colon and rectal surgery on 19–23. Color Dis [Internet]. 27:65–6.
- Chavoin JP, Quinodoz PD, Chilcott M, et al Surgical treatment of sacrococcygeal pilonidal sinus disease by excision and skin flaps: the Toulouse experience. Eur J Surg. 1999 Nov;165(11):1061-5.
- Irkörücü O. Management for pilonidal disease: Before you compare, use a classification system. Asian J Surg. 2016 Oct;39(4):260-1.
- Awad MM, Elbaset AA, Ebraheem S, et al. A scoring system as a method to evaluate pilonidal sinus disease to make an easy decision for its management. Indian J Plast Surg. 2009 Jan-Jun;42(1):43-8.
- Steven RBrown, Daniel Hind, Emily Strong et al Real world practice and outcomes in pilonidal surgery: Pilonidal Sinus Treatment Studying The Options (PITSTOP) cohort, BJS, Volume 111, Issue 3, March 2024, znae009, https://doi.org/10.1093/bjs/znae009
- Spivak H, Brooks VL, Nussbaum et al. Treatment of chronic pilonidal disease. Dis Colon Rectum. 1996 Oct. 39 (10):1136-9.
- Shanmugathas N, Yassin M, Ross C et al. Pilonidal Sinus Disease of the Penis: A Case Report and Review of the Literature. Andrologia. 2021;53(1):e13837. doi:10.1111/and.13837.
- Topgül K, Ozdemir E, Kilic K, et al(2003) Long-term results of Limberg procedure for treatment of pilonidal sinus: a report of 200 cases. Dis Colon Rectum 46:1545–1548
- Bascom J. Pilonidal disease. Origin from follicles of hairs and results of follicle removal as treatment. Surgery 1980;87:567–72.
- Stelzner F. Causes of pilonidal sinus and pyoderma fistulans sinifica Langenbecks Arch Chir. 1984;362(2):105-18.
- Dahl HD, Henrich MH Light and scanning electron microscopy study of the pathogenesis of pilonidal sinus and anal fistula]. Langenbecks Arch Chir. 1992;377(2):118-24.
- Gosselink MP, Jenkins L, Toh JWT et al Scanning electron microscope imaging of pilonidal disease. Tech Coloproctol. 2017 Nov;21(11):905-906.
- Plewig G, Kligman AM. Berlin Springer-Verlag: 1975. Acne Morphogenesis and treatment; pp. 192–193. Acne Morphogenesis and treatment; pp. 192–193.
- Hunt, TkConolly, WBAronsonGoldstein et al P Anaerobic metabolism and wound healing: a hypothesis for the initiation and cessation of collagen synthesis in wounds. Am J Surg. 1978;135328-332 Am J Surg. 1978;135328-332
- Allen DB Maguire JJ Mahdavien M et al. Wound hypoxia and acidosis limit neutrophil bacterial killing mechanisms. Arch Surg. 1997;132991-996. Arch Surg. 1997;132991-996.
- Lord PH Millar DM Pilonidal sinus: a simple treatment. Br J Surg. 1965;52298-300. Br J Surg. 1965;52298-300.
- Coccygeal osteomyelitis managed with wide excision, coccygectomy and perineal musculature reconstruction, with Limberg flap for defect closure. Mugdha Kowli, Pranav Mandovra et al World journal of colorectal surgery 2019:8;1;27-29.
- Dill DB, Yousef MK, Goldman A et al. Volume and composition of hand sweat of White and Black men and women in desert walks. Am J Phys Anthropol. 1983 May;61(1):67-73. doi: 10.1002/ajpa.1330610107. PMID: 6869514.
- Armstrong JH, Barcia PJ. Pilonidal sinus disease. The conservative approach. Arch Surg. 1994 Sep;129(9):914-7; 917-9.
- Alikhan A, Lynch PJ, Eisen DB. Hidradenitis suppurativa: A comprehensive review. J Am Acad Dermatol. 2009 Apr. 60 (4):539-61; quiz 562-3.
- Rompel R, Petres J. Long-term results of wide surgical excision in 106 patients with hidradenitis suppurativa. Dermatol Surg. 2000 Jul. 26(7):638-43.
- Kimball AB, Jemec GB, Yang M, et al. Assessing the validity, responsiveness and meaningfulness of the Hidradenitis Suppurativa Clinical Response (HiSCR) as the clinical endpoint for hidradenitis suppurativa treatment. Br J Dermatol. 2014 Dec. 171 (6):1434-42.
- Blok JL, Spoo JR, Leeman FW et al. Skin-Tissue-sparing Excision with Electrosurgical Peeling (STEEP): a surgical treatment option for severe hidradenitis suppurativa Hurley stage II/III. J Eur Acad Dermatol Venereol. 2015 Feb. 29 (2):379-82.
- Jemec GB. What’s new in hidradenitis suppurativa? J Eur Acad Dermatol Venereol. 2000 Sep. 14 (5):340-1.
- Bohn J, Svensson H. Surgical treatment of hidradenitis suppurativa. Scand J Plast Reconstr Surg Hand Surg. 2001 Sep. 35 (3):305-9.
- Enriquez-Navascues J., Emparanza J., Alkorta M et al. Meta-analysis of randomized controlled trials comparing different techniques with primary closure for chronic pilonidal sinus. Tech. Coloproctol. 2014;18[10]:863.
- Meinero P., Mori L., Gasloli G. et al. Endoscopic pilonidal sinus treatment (E.P.Si.T) Tech. Coloproctol. 2014;18:389–392.