

Diminished Finger Creases in Inclusion Body Myositis
Diminished distal dorsal finger crease is associated with handgrip weakness in inclusion body myositis
Matthew N. Prinsen MD1, Ava Yun Lin MD2, Kevin Dooley MD3, Conrad C. Wei MD, PhD4, Leo H. Wang MD, PhD5
- Department of Neurology, University of Washington, Seattle, Washington.
- University of Washington Medical Center, Box 356465, 1959 NE Pacific Street, Seattle, WA 98195-6465
- Department of Pediatrics, University of Michigan
- Cure IBM, Davis, CA
- Department of Neurology, Washington University in St. Louis
OPEN ACCESS
PUBLISHED: 31 July 2025
CITATION: Preston, M.K., et al., 2025. Diminished distal dorsal finger crease is associated with handgrip weakness in inclusion body myositis. Medical Research Archives, [online] 13(7).
https://doi.org/10.18103/mra.v13i7.6773
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i7.6773
ISSN 2375-1924
Abstract
Background: Sporadic inclusion body myositis (IBM) is the most common acquired myopathy in populations over age 45. This disorder causes slowly progressive asymmetric weakness with a predilection for weakness in knee extensions and in finger flexion, particularly in flexor digitorum profundus and flexor pollicis longus in the upper extremities.1 Though this clinical phenotype of IBM is relatively unique, the diagnosis can be missed without a high index of suspicion, or mistaken for amyotrophic lateral sclerosis (ALS), which can also be an asymmetric progressive motor weakness.2 Diagnosis of IBM remains challenging, with an average delay in diagnosis of 5.6 years after symptom onset.3
Methods: We examined distal dorsal finger creases in 32 patients with IBM and 44 controls.
Results: Loss of finger creases and dominant grip strength: Grip strength in patients with IBM showed mean 20th percentile [IQR 12.27] with loss of finger creases (n=32) versus 31st percentile [IQR 24.42] without loss of finger creases (p=0.008).4
Discussion: Our findings show that loss of distal dorsal interphalangeal finger creases is present in many patients with IBM (40%) compared to controls (15%). Additionally, we show that distal finger creases are associated with reduced grip strength (20th percentile vs 31st percentile; p=0.008). We hypothesize that the presence of reduced distal finger creases is helpful in distinguishing between IBM and ALS, which typically does not present with this finding.
Keywords
Inclusion Body Myositis, Handgrip Strength, Distal Dorsal Finger Creases, Muscle Weakness, Diagnosis
Introduction
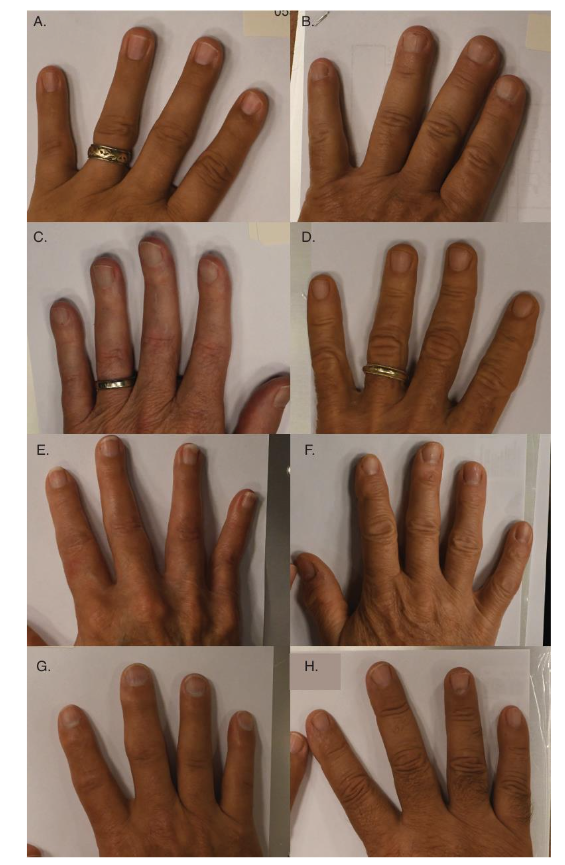
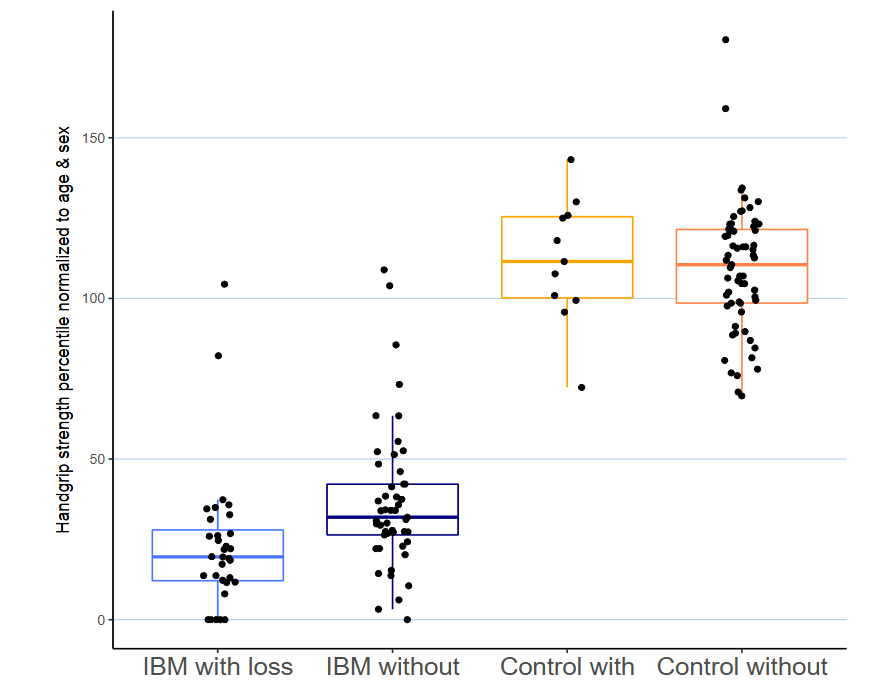
Figure 2: Loss of finger creases and dominant grip strength: Grip strength in patients with IBM showed mean 20th percentile (IQR 12–27) with loss of finger creases (n=32) versus 31st percentile (IQR 24–42) without loss of finger creases (n=49, p value = 0.008). Control patients with or without loss of distal finger creases both showed normal grip in 110–111th percentile. IQR: interquartile range; IBM: inclusion body myositis
Discussion
Our findings show that loss of dorsal distal interphalangeal finger creases is present in more patients with IBM (40%) than control patients (15%). Additionally, we show that the loss of finger creases within the IBM cohort is associated with reduction of grip strength (20th percentile vs 31st percentile; p = 0.008). We also confirm that grip strength testing is a clinically useful and easy measurement in this population in addition to qualitative testing of distal finger flexor strength. Prior studies have demonstrated that grip strength correlates with finger flexor function, supporting this as a helpful component of the exam.¹²,¹³ It should be noted that testing of the deep finger flexors, while remaining essential in an evaluation for the possibility of IBM, requires proper technique including testing all fingers flexed simultaneously due to the quadriga phenomenon of interconnectedness between deep digit flexors, whereas grip testing is more straightforward for clinicians.¹³
In our IBM cohort, we hypothesize that the worsened grip strength and the loss of dorsal distal finger creases are caused by the same mechanism, which is weakness in the flexor digitorum profundus muscles, and reduced motion at the distal interphalangeal joint. Loss of finger creases has been suspected to be seen as a consequence of weakness at the affected joint, primarily reported in development of flexion
creases and especially in congenital weakness.¹⁴ However, little data is available for loss of finger creases in acquired/degenerative muscle disease, and especially in the dorsal finger creases. Notably, disorders such as ALS which frequently cause distal hand weakness but not finger flexor weakness,¹⁵ do not have this finding in our observations in clinical practice. We expect several factors may be involved in this difference, including the relative sparing of deep finger flexors and the rapidity of symptoms in ALS compared to the slowly progressive weakness often seen in patients with IBM at time of their presentation. The presence of finger creases in 60% of our IBM cohort is suspected to be related to the relative preservation of function in these patients as indicated by the increased grip strength.
The source of absent finger creases in the control cohort is likely different from those with IBM, given the absence of grip weakness. Normal aging expects an increase in distal dorsal finger wrinkles over time.¹⁶ However, reduced mobility even in setting of normal muscle function may occur. Presence of arthritis, primary skin diseases such as scleroderma, or other hereditary sources such as nail-patella syndrome, as well as diabetes (with its association with limited joint mobility) is also associated with reduced wrinkling.¹⁷–¹⁹ These healthy controls should not be easily mistaken for IBM due to lack of motor weakness on exam or by history.
This study has several limitations: Firstly, subjects are self-identified with IBM which raises our possibility of false positives in the IBM group. Secondly, we have only a single observer rating finger creases which raises a question on interobserver validity. The presence of dorsal finger creases in some patients with IBM shows that this test is not highly sensitive. Though finger flexor weakness can help differentiate between those abnormal findings in the control group, they may not be as helpful in setting of other myopathies with finger flexor weakness such as myotonic dystrophies.²⁰
Given the simplicity of examining for this diminishment in dorsal distal finger creases, it can be a helpful complement to a full evaluation for IBM. The presence of reduced distal finger creases is helpful in consideration of potential mimics of IBM such as ALS which more often spares the deep finger flexors and progresses much more quickly so would not be expected to cause this finding.¹⁵,²¹ Additionally, this finding can be a helpful clue to further examine a patient’s grip and finger flexor strength when upper extremity weakness is not apparent on a routine physical exam that may not include finger flexors.
Conclusion
This study provides further confirmation that loss of distal finger creases is associated with IBM and associated with reduced grip strength. This is a helpful feature to identify patients who may have IBM and is best interpreted in combination with an appropriate history and will guide an expanded examination for other clinical features associated with IBM.
References
1. Lloyd TE, Mammen AL, Amato AA, et al. Evaluation and construction of diagnostic criteria for inclusion body myositis. Neurology. 2014 Jul 29;83(5):426-33.
2. Badrising UA, Maat-Schieman ML, van Houwelingen JC, et al. Inclusion body myositis. Clinical features and clinical course of the disease in 64 patients. J Neurol. 2005 Dec;252(12):1448-54.
3. Felice KJ, Relva GM, Conway SR. Further observations on forearm flexor weakness in inclusion body myositis. Muscle Nerve. 1998 May;21(5):659-61.
4. Phillips BA, Cala LA, Thickbroom GW, et al. Patterns of muscle involvement in inclusion body myositis: clinical and magnetic resonance imaging study. Muscle Nerve. 2001 Nov;24(11):1526-34.
5. Abdelnaby R, Mohamed KA, Elgenidy A, et al. Muscle Sonography in Inclusion Body Myositis: A Systematic Review and Meta-Analysis of 944 Measurements. Cells. 2022 Feb 9;11(4).
6. Simon NG, Lomen-Hoerth C, Kiernan MC. Patterns of clinical and electrodiagnostic abnormalities in early amyotrophic lateral sclerosis. Muscle Nerve. 2014 Dec;50(6):894-9.
7. Molberg O, Dobloug C. Epidemiology of sporadic inclusion body myositis. Curr Opin Rheumatol. 2016 Nov;28(6):657-60.
8. Fried K, Mundel G. Absence of distal interphalangeal creases of fingers with flexion limitation. J Med Genet. 1976 Apr;13(2):127-30.
9. Lin AY, Koo B, Wang LH. Diminished distal dorsal finger wrinkling in patients with sporadic inclusion body myositis. Journal of Clinical Images and Medical Case Reports. 2021;2.
10. Lin AY, Clapp M, Karanja E, et al. A cross-sectional study of hand function in inclusion body myositis: Implications for functional rating scale. Neuromuscul Disord. 2020 Mar;30(3):200-6.
11. Wang YC, Bohannon RW, Li X, et al. Hand-Grip Strength: Normative Reference Values and Equations for Individuals 18 to 85 Years of Age Residing in the United States. J Orthop Sports Phys Ther. 2018 Sep;48(9):685-93.
12. Horton TC, Sauerland S, Davis TR. The effect of flexor digitorum profundus quadriga on grip strength. J Hand Surg Eur Vol. 2007 Apr;32(2):130-4.
13. Schreuders TA. The quadriga phenomenon: a review and clinical relevance. J Hand Surg Eur Vol. 2012 Jul;37(6):513-22.
14. Stevens CA, Carey JC, Shah M, et al. Development of human palmar and digital flexion creases. J Pediatr. 1988 Jul;113(1 Pt 1):128-32.
15. Shemesh A, Arkadir D, Gotkine M. Relative preservation of finger flexion in amyotrophic lateral sclerosis. J Neurol Sci. 2016 Feb 15;361:128-30.
16. Jakubietz RG, Kloss DF, Gruenert JG, et al. The ageing hand. A study to evaluate the chronological ageing process of the hand. J Plast Reconstr Aesthet Surg. 2008 Jun;61(6):681-6.
17. Banno Y, Ikemiyagi M, Hamada R, et al. Nail-patella syndrome with nephropathy in a de novo LMX1B mutation: triangular lunula of the thumb and lack of finger creases as clues. Pediatr Nephrol. 2024 Sep;39(9):2627-31.
18. Itin PH, Eich G, Fistarol SK. Missing creases of distal finger joints as a diagnostic clue of nail-patella syndrome. Dermatology. 2006;213(2):153-5.
19. Rosenbloom AL. Limitation of finger joint mobility in diabetes mellitus. J Diabet Complications. 1989 Apr-Jun;3(2):77-87.
20. Nicolau S, Liewluck T, Milone M. Myopathies with finger flexor weakness: Not only inclusion-body myositis. Muscle Nerve. 2020 Oct;62(4):445-54.
21. Menon P, Bae JS, Mioshi E, et al. Split-hand plus sign in ALS: differential involvement of the flexor pollicis longus and intrinsic hand muscles. Amyotroph Lateral Scler Frontotemporal Degener. 2013 May;14(4):315-8.