

Global Strategies for Localized Trauma Education in Medicine
How can a global organization make education local?
Workplace education for surgeons treating orthopedic trauma cases
Anna Maria Montero1, Alexandra Wentschel1, Kodi E. Kojiwar2, Michael R. Baumgaertner3, Jezeh Reichmuth4, Monica Ghidinelli5
- Education Institute, AO Foundation, Davos, Switzerland
- Instituto de Ortopedia, Hospital das Clínicas, UFMG, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil
- Department of Orthopedics and Rehabilitation, Yale University School of Medicine, USA
- Department of Orthopedics, Prince Mohammed bin Abdulaziz Hospital, Riyadh, Saudi Arabia
- Department of Orthopedics, University of São Paulo, Brazil
Correspondence: Anna Maria Montero, AO Foundation, Davos, Switzerland. Email: [email protected]
OPEN ACCESS
PUBLISHED: 30 June 2025
CITATION:Moreno, A.M., et al., 2025. How can a global organization make education local? Workplace education for surgeons treating orthopedic trauma cases. Medical Research Archives, [online] 13(6).
https://doi.org/10.18103/mra.v13i6.4677
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i6.4677
ISSN 2375-1924
Abstract
Continuing medical education (CME) and continuing professional development (CPD) events are critical to the lifelong learning of healthcare professionals (HCPs). HCPs attend a number of continuing medical education (CME) and continuing professional development (CPD) events every year, provided by medical societies, medical education providers, or hospitals. Such in-person CME/CPD events require participants to travel to a designated location, posing logistical challenges such as time constraints, travel and accommodation costs, and potential disruptions to clinical practice. Workplace-based CME/CPD initiatives offer a viable alternative to address the challenges associated with traditional educational formats. This study aims to evaluate the effectiveness of a workplace-based CME initiative for trauma surgeons in various regions, focusing on participant engagement and knowledge acquisition.
Keywords
Continuing medical education, workplace education, orthopedic trauma, surgeons, knowledge acquisition
Introduction
Continuing medical education (CME) and continuing professional development (CPD) contribute to the lifelong learning of healthcare professionals (HCPs). Thus, HCPs attend a number of continuing medical education (CME) and continuing professional development (CPD) events every year, provided by medical societies, medical education providers, or hospitals¹,². Such in-person CME/CPD events require participants to travel to a designated location, posing logistical challenges such as time constraints, travel and accommodation costs, and potential disruptions to clinical practice and family or personal commitments³. These barriers limit access to education, especially for young HCPs⁴–⁶.Workplace-based CME/CPD initiatives offer a valuable alternative to address the challenges associated with centralized courses and have been shown to offer positive effects on: decision-making skills, self-motivation, development of new perspectives and techniques, alignment with hospital rules and regulations, collaboration within teams and among colleagues, and overall work atmosphere⁷,⁸. Workplace-based CME initiatives are grounded in sociocultural learning theory and the concept of “communities of practice”⁹, emphasizing the dynamic relationship between learners, experts, and the environment. Within this framework, experts guide novices through collaborative learning experiences, enabling participants to contextualize and immediately apply their newly acquired knowledge to their clinical environment.The AO Foundation, a global surgeon-led organization focusing on the treatment of musculoskeletal disorders, has a well-established history of delivering centralized CME courses worldwide¹⁰. Additionally, the AO has experience with decentralized courses, including workplace-based education events on fracture care for older adults¹¹, a course on magnetic resonance imaging of spinal trauma¹², and hospital-based clinical training modules for operating room personnel (ORP). This ORP-specific solution has been implemented in hospitals worldwide since 2015, providing course content (lectures, videos, and clinical cases) exclusively to AO faculty members through an online platform. The faculty run these educational events in their own hospital, adapting the teaching materials to the surgical procedures, local guidelines, and local language.In 2016 AO Trauma decided to build on the experience gained from ORP training modules and address gaps in its educational offerings, particularly for young surgeons, to offer decentralized, flexible, accessible, and locally relevant training modules. The project started under the name AO In-Hospital in 2020 when adequate funding and resources were made available. This article describes the development, implementation, and impact of the In-Hospital trauma modules.
Methodology
IN-HOSPITAL MODULE DESIGN AND DEVELOPMENT
The design followed a competency-based approach through backward planning and Kern’s 6-step model for curriculum development¹³–¹⁵. The target audience was residents and surgeons with up to 5 years of experience in trauma centers. The identified educational needs covered knowledge, skills, and attitudes in the management of polytrauma, acute compartment syndrome, elbow fractures in children, fracture-related infection, best practices in geriatric hip fractures, limb salvage versus amputation, and open fractures (Table 1).The In-Hospital materials were developed and edited by AO surgeons from different regions, assuring a high-quality standard. The pre-course assessment questions were designed as an interactive learning activity with three key goals: 1. to motivate learners to self-assess and engage in self-directed learning, 2. to identify gaps that require further attention, and 3. to address curricular objectives. At least one assessment question was developed for each learning objective, with four options and a single correct/best answer, followed by feedback rationale explaining the correct and incorrect options. The same questions were asked after completion of the module.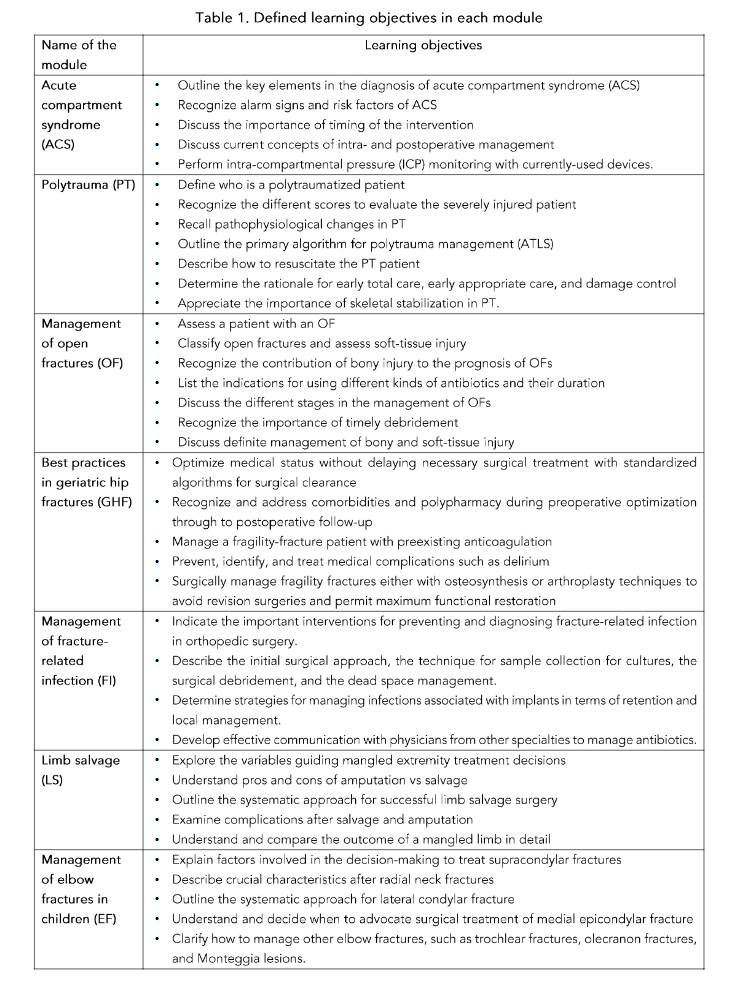
The module was designed to be flexible; a complete module for face-to-face events contains up to 4 hours of teaching material. Faculty can tailor the event duration from 60 minutes to 4 hours to meet the needs of the participants and the hospital. The module packages include a user manual for the course director, a pre- and post-course knowledge assessment based on clinical vignettes, pre-reading material, lecture slide sets, cases for small group discussions, a certificate of attendance, instructions for optional practical exercises, and an event evaluation form. The faculty can select content appropriate for their participants according to their experience level, hospital requirements, available infrastructure, and time availability.
DELIVERY METHOD
An online platform was developed to provide access to educational materials, facilitate faculty members in running the event, and automate communication, and trigger evaluation and assessment processes. The system automatically sends registration confirmations to chairpersons and participants, invitations to participants to complete the pre-event assessment including demographics and practice profile, present and desired levels of expertise for a series of defined competencies, multiple-choice questions (MCQs), certificates of attendance, post-event assessment invitations to participants with event evaluation, present and desired expertise levels after the educational event, same set of MCQs, and feedback form to chairpersons. Automated reminders are sent to participants who have not completed questions to ensure higher response rates. Additionally, chairpersons receive timely information emails that invitations with links to pre- and post-event assessments have been sent to participants.
The chairpersons are asked to complete specific tasks, such as confirming the list of participants and submitting their feedback form. This built-in functionality helps maintain accountability and ensure that deadlines are met. An automated reporting system allows for the timely generation of detailed pre- and post-event reports on participant profiles, present and desired levels of competencies, MCQs, educational impact, knowledge increase, and event feedback.
DATA COLLECTION
Data were collected from June 2022 to June 2024 utilizing a standardized evaluation and assessment system based on Moore’s framework¹³,¹⁶, in addition to module-specific knowledge-based multiple-choice questions. Participants were invited by email to complete the questions online. 1,829 pre-event and 1,287 post-event responses were collected for analysis. This study utilized data collected to measure the impact of the In-Hospital educational program on participant knowledge and professional practice based on Moore’s educational outcomes¹³.
DATA ANALYSIS
The collected data were analyzed using SPSS version 29.0.2 (SPSS Inc., Chicago, USA). Descriptive statistics were calculated to summarize the participant demographics and survey responses. Paired sample t-tests were conducted to evaluate changes between the pre- and post-test. Cohen’s d was calculated to determine the effect sizes meaning the practical significance of the observed changes in the pre-post-test.
ETHICAL APPROVAL
According to the Ethics Committee of the Canton of Zurich, this study did not require ethical committee approval (Req-2025-00604). In the survey, we included the following statement of purpose, which disclosed our intended use of the data: “The information you provide will be anonymized and made available to the study group in aggregate form. The data will be used for research purposes.”
Results
Between June 2022 and June 2024, 87 AO faculty implemented 169 In-Hospital educational events across 30 countries and enrolled a total of 3,950 attendees. 43% of the faculty delivered two or more events using either the same module multiple times or different modules (range: 1 to 9 educational events per faculty). In 2022, 41 events (24.3% of
(total activities) were recorded, with a substantial increase in 2023, documenting 76 events (45.0%). Through June 2024 (study endpoint), 52 events were implemented, comprising 30.8% of the total occurrences (Table 2).
EVENT DISTRIBUTION AND PARTICIPANT ENGAGEMENT ACROSS MODULES
The initiative exhibited pronounced regional participation in South Asia, the Middle East, and Latin America. India demonstrated the highest implementation, with 33 events, followed by Pakistan (20 events), Egypt (17 events), and Mexico (12 events) (Fig. 1).
Table 3 illustrates the frequency distribution and participant involvement in the seven educational modules.
Table 2: Number of In-Hospital events
| Year | Number of Events | Percentage of Total |
|---|---|---|
| 2022 | 41 | 24.30% |
| 2023 | 76 | 45.00% |
| 2024* | 52 | 30.8% |
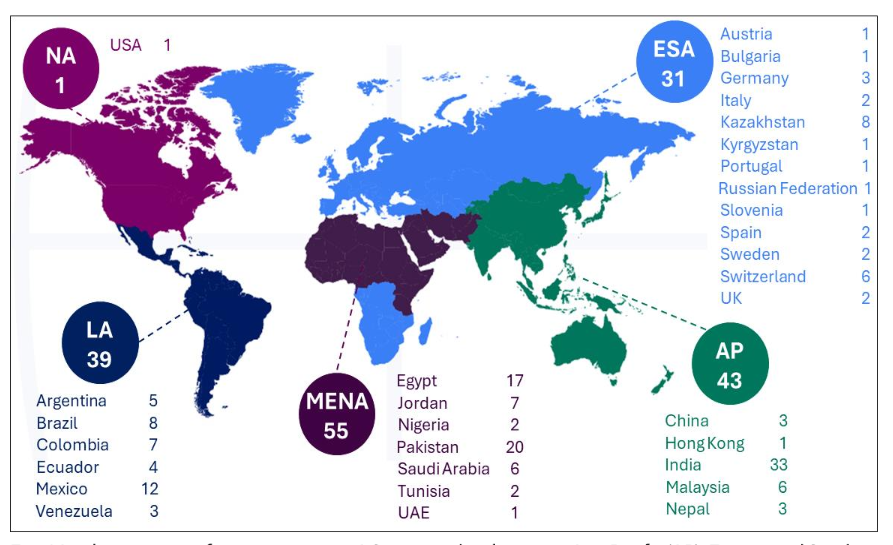
Fig. 1 Implementation of events at various AO geographical regions. Asia Pacific (AP), Europe and Southern Africa (ESA), Latin America (LA), Middle East and Northern Africa (MENA), North America (NA)
Table 3: Number of events per module and number of participants
| Module name | Number of events | Participants | Percentage (%) |
|---|---|---|---|
| Polytrauma (PT) | 45 | 1,206 | 30.5 |
| Open Fractures (OF) | 43 | 1,053 | 26.7 |
| Fracture Infection (FI) | 24 | 548 | 13.9 |
| Geriatric Hip Fractures (GHF) | 22 | 445 | 11.3 |
| Acute Compartment Syndrome (ACS) | 22 | 341 | 8.6 |
| Elbow Fractures (EF) in Children | 7 | 210 | 5.3 |
| Limb Salvage (LS) | 6 | 147 | 3.7 |
The polytrauma module demonstrated predominant engagement, comprising 45 educational sessions and attracting 1,206 participants (30.5% of the total attendance). The open fractures module had 43 sessions and 1,053 participants (26.7%). Fracture infections and geriatric hip fractures maintained intermediate participation levels, with 24 (548 participants, 13.9%) and 22 (445 participants, 11.3%) sessions, respectively. Acute compartment syndrome was delivered 22 times, involving 341 participants (8.6%). Specialized modules demonstrated more focused participation patterns: elbow fractures in pediatric cases encompassed 7 sessions with 210 participants (5.3%), and limb salvage procedures included 6 sessions engaging 147 participants (3.7%).
PARTICIPANTS EXPERIENCE LEVEL ACROSS IN-HOSPITAL MODULES
Among the 3,950 attendees, 1,829 submitted pre-event evaluations, 1,287 provided post-event feedback, and 528 completed both assessments. This substantial response rate demonstrates robust engagement levels and provides comprehensive data for programme analysis. Fig. 2 illustrates the years of experience of medical practitioners across trauma modules, analyzed by their post-graduation duration.
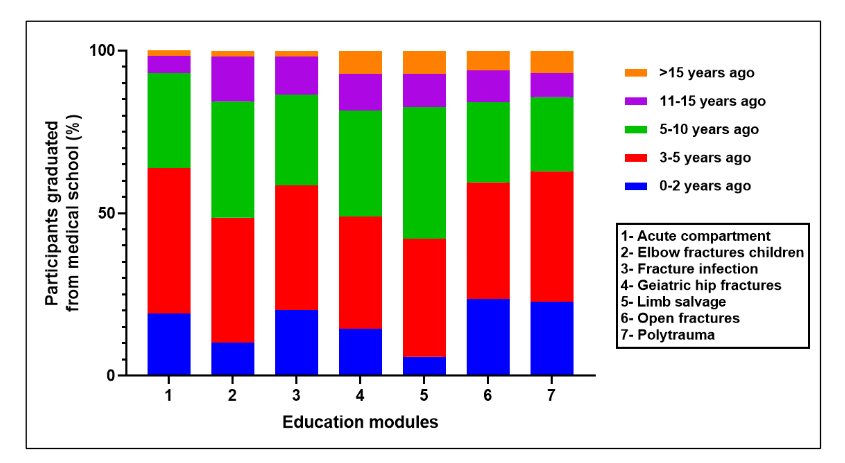
Fig. 2 Distribution of participants’ graduation timeline across modules
As expected, the data indicated predominant participation of young practitioners who had completed medical school 3–5 years prior (peaking at 44.68% in the acute compartment module), followed by those with 5–10 years of clinical experience (reaching 40.58% in limb salvage). Within 0–2 years post-qualification, recent graduates constitute a notable minority, with their highest representation (23.57%) observed in the open fractures module.
EDUCATIONAL OUTCOMES
To evaluate the educational outcomes of the modules, we employed Moore’s framework¹³,¹⁴. For satisfaction (Moore’s level 2), we analyzed the participants’ evaluation of module usefulness in their clinical practice (Fig. 3).
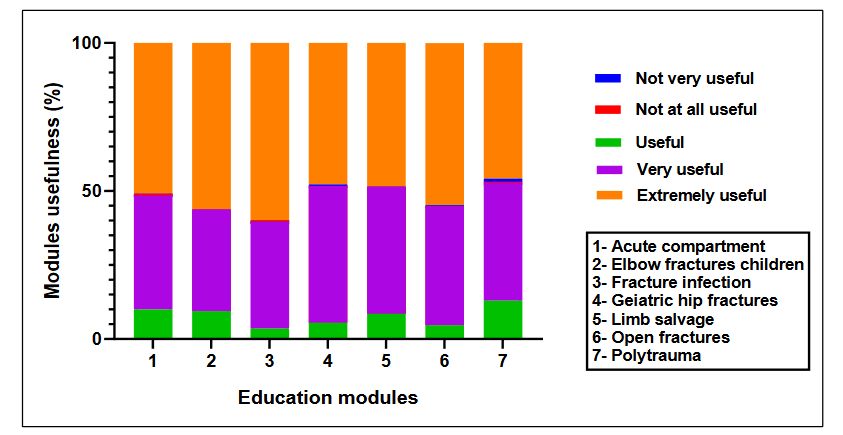
Figure 3. Participants responses on module usefulness post-event.
The data demonstrate predominant “Very Useful” and “Extremely Useful” ratings across all modules, with “Extremely Useful” consistently representing the highest percentage. Notable peaks in the “Extremely Useful” ratings were observed for modules covering acute compartment syndrome, fracture infections, and polytrauma management, highlighting their perceived significance. In addition, 99% of participants answered yes to the question “Would you recommend this educational event?” (range 97% to 100% in the different modules), and 92.4% rated the faculty performance in education delivery as either “extremely effective” (n = 757) or “very effective” (n = 432) (Table 4). A negligible fraction indicated ratings of “not very effective” (n = 3) or “not at all effective” (n = 3), validating the faculty’s instrumental contribution to educational excellence. These results suggest high participant satisfaction with the clinical relevance and pedagogical value of the educational material.
Table 4: Faculty effectiveness
| How effective were all faculty in the role they played? | No. of participants (n) |
|---|---|
| Extremely effective | 757 |
| Very effective | 432 |
| Effective | 92 |
| Not very effective | 3 |
| Not at all effective | 3 |
| Total | 1287 |
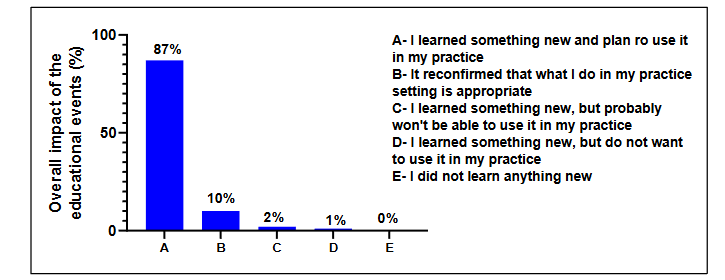
Fig. 4 Overall impact of educational events
Competence (Moore’s level 4) was measured by pre-test vs. post-test analysis of case-based assessment questions. The analysis demonstrated notable enhancements in comprehension across all modules post-course (Table 5). The limb salvage versus amputation module displayed the most substantial progress, with a remarkable 33% improvement, whereas the fracture infection module had the smallest improvement (13%). These findings substantiate that the educational interventions effectively enhanced participants’ comprehension across all trauma-related modules (Table 5).
Table 5: Knowledge assessment during pre- and post-event modules
| Modules | Pre knowledge questions | Post Knowledge Questions | Pre–Post difference (%) | ||||
|---|---|---|---|---|---|---|---|
| Correct answers (n) | Total no. of answers (N) | (%) | Correct answers (n) | Total no. of answers (N) | (%) | ||
| Acute compartment syndrome | 1976 | 3465 | 57 | 2191 | 3095 | 71 | 14 |
| Elbow fractures in children | 711 | 1740 | 41 | 297 | 465 | 64 | 23 |
| Fracture infection | 3201 | 6026 | 53 | 2261 | 3431 | 66 | 13 |
| Geriatric hip fractures | 2520 | 4917 | 51 | 2036 | 3084 | 66 | 15 |
| Limb salvage | 370 | 753 | 49 | 339 | 414 | 82 | 33 |
| Open fractures | 2285 | 5343 | 43 | 2529 | 4358 | 58 | 15 |
| Polytrauma | 1367 | 4314 | 32 | 1389 | 3105 | 45 | 13 |
Additionally, statistical analysis using a paired samples t-test demonstrated an enhancement in participants’ knowledge metrics following the In-Hospital educational events. The knowledge assessment scores increased from a mean of 7.33 (SD = 3.806) pre-intervention to 9.64 (SD = 4.173) post-intervention, demonstrating substantial improvement in their clinical competencies. Statistical validation through paired samples t-test corroborated this advancement, yielding a mean difference of −2.305 (SD = 3.209), with a statistically significant t-value of −16.506 and p-value <0.001. The mean difference confidence interval spanned from −2.579 to −2.031, validating the statistical reliability of these findings (Table 6A). The intervention’s impact magnitude, quantified by Cohen’s d, was −0.714 (95% CI: −0.814 to −0.622), suggesting a substantial effect on knowledge enhancement (Table 6B). These findings substantiate the efficacy of the educational intervention in significantly improving participant competencies.
Table 6 A: Improvement in knowledge scores during pre-and-post educational events
| Measure | N | Mean ± SD | Mean difference ± Standard deviation (SD) | t | df | p-value | 95% Confidence interval (CI) (lower) | 95% Confidence interval (CI) (upper) |
|---|---|---|---|---|---|---|---|---|
| Pre-Test | 528 | 7.33 ± 3.806 | −2.305 ± 3.209 | −16.506 | 527 | <0.001 | −2.579 | −2.031 |
| Post-Test | 528 | 9.64 ± 4.173 |
B: Estimation of effect size (Cohen’s d effect)
| Measure | Cohen’s d | 95% CI (lower) | 95% CI (upper) |
|---|---|---|---|
| Pre_Test – Post_Test | −0.714 | −0.814 | −0.622 |
Discussion
The current study highlights the development, implementation, and global impact of the AO In-Hospital educational program, designed to address barriers to centralized CME/CPD events and to meet the educational needs of young trauma surgeons. The findings revealed significant success in decentralizing medical education, improving accessibility, and enhancing participants’ competencies.
The AO In-Hospital program demonstrated robust adoption, with 169 events across 30 countries and nearly 4,000 participants in two years. The program’s geographic distribution, particularly in South Asia, the Middle East, and Latin America, underscores its adaptability and relevance to these settings. Countries such as India, Pakistan, and Egypt demonstrated particularly strong engagement, suggesting that the program effectively addressed unmet educational needs, possibly due to limited access to traditional in-person CME/CPD. The polytrauma and open fractures modules received the highest engagement, demonstrating the critical need for education on complex trauma cases in regions with high trauma burdens. This aligns with prior research from low-resource settings, where trauma-focused CME interventions significantly improved healthcare professionals’ competencies and were associated with better patient outcomes¹⁷,¹⁸. The presence of early career practitioners, particularly in these modules, highlights the importance of providing advanced-level competencies to those who will encounter the most critical trauma cases in their clinical practice.
settings. By addressing these high-priority areas, the modules may contribute directly to reducing trauma-related morbidity and mortality, as supported in similar settings where trauma education has led to improvements in clinical care and patient outcomes¹⁹,²⁰.
In our study, the pre-post test showed a significant increase in competencies, and 87.18% of participants reported acquiring new knowledge with the intention to implement it in their practice. This underscores the potential of workplace-based CME to catalyze immediate improvements in clinical competence. This mirrors the success of other international initiatives that aim to enhance trauma care in resource-limited settings. For instance, the Trauma Support Practitioner project has leveraged technology-enhanced learning across various regions, including India and Africa, demonstrating that such interventions are crucial for improving trauma training and ultimately patient care²¹. These international efforts, combined with our findings, suggest that flexible, context-specific CME models, such as the AO In-Hospital modules, hold great promise for addressing urgent needs in global trauma education.
The AO In-Hospital trauma modules are deeply rooted in situated learning theory and the concept of “communities of practice”⁹. This framework emphasizes that learning is most effective when it occurs in a social context. The module design allows faculty and participants to contextualize knowledge in the clinical setting and adapt it to local guidelines. The high level of engagement, coupled with the ability to tailor the learning experience to local needs, makes these modules particularly effective in fostering continuous learning and competence development. This approach not only enhances knowledge but also helps create communities of practice where medical professionals can share expertise and collaborate, a dynamic known to facilitate deeper learning and long-term knowledge retention¹⁷. The modules promoted reflection on experiences, especially during the small group discussions, allowing participants to confirm or modify pre-existing concepts, leveraging the principle of experiential learning²².
While our study primarily focused on knowledge acquisition and competence through pre- and post-assessments, the literature supports the assertion that these improvements are likely to translate into enhanced skills and ultimately better patient care²³,²⁴. In a similar study, O’Brien et al.²⁰ found that a train-the-trainer module for healthcare professionals in Bangladesh resulted in significant improvements in trauma management skills, which directly impacted patient care in the region. Similarly, the significant improvements in knowledge observed in our study, particularly in areas such as polytrauma, open fractures, and fracture infections, suggest that these modules have the potential to lead to improved clinical outcomes through better-informed decision-making in trauma management.
The enhancement of clinical competencies among young practitioners is of particular significance because these learners, as they gain more clinical experience, will be in a position to apply the knowledge gained through the In-Hospital modules in more complex clinical situations. Thus, the program not only addresses immediate educational needs but may also contribute to the longer-term professional development of healthcare professionals, ensuring sustained improvement in clinical practice²³.
The positive outcomes from the AO In-Hospital modules also underscore the value of evidence-based modular approaches to CME. The flexibility inherent in modular design allows for the customization of learning content to meet the specific needs of both learners and institutions, making it an attractive option for diverse healthcare environments. This modular structure enables a targeted approach to addressing the most pressing clinical needs of different healthcare settings, thereby maximizing the potential impact on patient care²⁵.
This initiative demonstrates the potential of workplace-based education to enhance clinical skills,
particularly for young surgeons and practitioners in resource-constrained settings. By leveraging context-specific, flexible learning methods, the In-Hospital program contributes to bridging educational inequities and advancing global healthcare quality.
Limitations
Despite these promising results, several limitations must be acknowledged. While we observed substantial improvements in participants’ competence, the study did not include a long-term follow-up to assess whether these changes translated into sustained improvements in patient care. Furthermore, the study primarily relied on self-reported data from participants, which, although helpful for gauging satisfaction and perceived knowledge gain, may not fully capture the long-term impact on clinical practice or on patient outcomes. In addition, we have no information regarding the number of events that were associated with practical exercises in the theoretical part.
Conclusion
In conclusion, the study revealed the significant influence of in-hospital training on enhancing surgeons understanding of trauma care. By following the principles of situated learning and communities of practice, the program ensures that learners engage with real-world clinical scenarios, making the knowledge gained immediately applicable to patient care. The positive results, including high satisfaction levels and substantial improvements in competence, suggest that such workplace-based initiatives are a viable alternative to centralized CME programs and can meaningfully contribute to improving trauma care, particularly in regions with limited access to centralized education. By refining and expanding the AO In-Hospital modules, future initiatives can further advance CME accessibility and efficacy, supporting the lifelong learning of healthcare professionals worldwide. Additionally, integrating longitudinal follow-ups to assess the program’s sustained impact on clinical practice and patient outcomes would provide valuable insights.
Conflicts of Interest Statement:
The authors declare no conflict of interest.
Funding Statement:
No specific funding was obtained for this study.
Acknowledgments:
We thank all the course chairpersons and questionnaire respondents.
References
1. Coudane H, Danan JL, Martrille L, et al. Postgraduate training in surgery: From theory to practice. J Visc Surg [Internet]. 2020;157(3):S137–40. Available from: http://dx.doi.org/10.1016/j.jviscsurg.2020.03.004
2. Walton M, Harrison R, Burgess A, et al. Workplace training for senior trainees: a systematic review and narrative synthesis of current approaches to promote patient safety. Postgrad Med J [Internet]. 2015;91(1080):579–87. Available from: http://dx.doi.org/10.1136/postgradmedj-2014-133130
3. O’Brien Pott M, Blanshan AS, Huneke KM, et al. Barriers to identifying and obtaining CME: a national survey of physicians, nurse practitioners and physician assistants. BMC Med Educ [Internet]. 2021 Mar 19;21(1):168. Available from: https://pubmed.ncbi.nlm.nih.gov/33740962
4. Alsaleem SA, Almoalwi NM, Siddiqui AF, et al. Current Practices and Existing Gaps of Continuing Medical Education among Resident Physicians in Abha City, Saudi Arabia. Int J Environ Res Public Health [Internet]. 2020 Nov 16;17(22):8483. Available from: https://pubmed.ncbi.nlm.nih.gov/33207729
5. Minor S, Poenaru D. The in-house education of clinical clerks in surgery and the role of housestaff. The American Journal of Surgery [Internet]. 2002; 184(5):471–5. Available from:
http://dx.doi.org/10.1016/s0002-9610(02)01001-2
6. Stefanescu MC, Sterz J, Hoefer SH, et al. Young surgeons’ challenges at the start of their clinical residency: a semi-qualitative study. Innov Surg Sci [Internet]. 2018 Jun 4;3(4):235–43. Available from: https://pubmed.ncbi.nlm.nih.gov/31579787
7. King R, Taylor B, Talpur A, et al. Factors that optimise the impact of continuing professional development in nursing: A rapid evidence review. Nurse Educ Today [Internet]. 2021;98:104652. Available from:
http://dx.doi.org/10.1016/j.nedt.2020.104652
8. Filipe HP, Silva ED, Stulting AA, et al. Continuing professional development: best practices. Middle East Afr J Ophthalmol [Internet]. 2014;21(2):134–41. Available from: https://pubmed.ncbi.nlm.nih.gov/24791104
9. Lave J, Wenger E. Situated Learning [Internet]. Cambridge University Press; 1991. Available from: http://dx.doi.org/10.1017/cbo9780511815355
10. Joeris A, Höglinger M, Meier F, et al. The impact of the AO Foundation on fracture care: An evaluation of 60 years AO Foundation. Injury [Internet]. 2019; 50(11):1868–75. Available from:
http://dx.doi.org/10.1016/j.injury.2019.07.016
11. Gosch M, Kammerlander C, Fantin E, et al. Design and Evaluation of a Hospital-Based Educational Event on Fracture Care for Older Adult. Geriatr Orthop Surg Rehabil [Internet]. 2021 Mar 31;12:21514593211003856–21514593211003856. Available from: https://pubmed.ncbi.nlm.nih.gov/33868767
12. Kraus MD, Mueller M, Schmitz B, et al. Development of a Performance Improvement Program: A Workplace-Based Educational Intervention on Magnetic Resonance Imaging in Spinal Trauma. J Surg Educ [Internet]. 2016;73(3):416–21. Available from: http://dx.doi.org/10.1016/j.jsurg.2015.12.005
13. Moore DE, Green JS, Gallis HA. Achieving desired results and improved outcomes: Integrating planning and assessment throughout learning activities. Journal of Continuing Education in the Health Professions [Internet]. 2009;29(1):1–15. Available from: http://dx.doi.org/10.1002/chp.20001
14. Moore DE, Chappell K, Sherman L, et al. A conceptual framework for planning and assessing learning in continuing education activities designed for clinicians in one profession and/or clinical teams. Med Teach [Internet]. 2018;40(9):904–13. Available from: http://dx.doi.org/10.1080/0142159x.2018.1483578
15. Kern D, Thomas P, Hughes M, et al. Curriculum Development for Medical Education: A Six-step Approach. Baltimore, MD: The John’s Hopkins University Press; 2009
16. Ghidinelli M, Cunningham M, Uhlmann M, et al. Designing and implementing a harmonized evaluation and assessment system for educational events worldwide. J Orthop Trauma. 2021;35 (suppl 2):S5–S10. available from:
https://journals.lww.com/jorthotrauma/Documents/Learning%20in%20the%20AO_Looking%20Back%20and%20Moving%20Forward.pdf
17. Mock CN, Quansah R, Addae-Mensah L, et al. The development of continuing education for trauma care in an African nation. Injury [Internet]. 2005;36(6):725–32. Available from:
http://dx.doi.org/10.1016/j.injury.2004.12.044
18. Tchorz KM, Thomas N, Jesudassan S, et al. Teaching Trauma Care in India: An Educational Pilot Study From Bangalore. Journal of Surgical Research [Internet]. 2007;142(2):373–7. Available from: http://dx.doi.org/10.1016/j.jss.2006.07.010
19. Petroze RT, Byiringiro JC, Ntakiyiruta G, et al. Can focused trauma education initiatives reduce mortality or improve resource utilization in a low-resource setting? World J Surg [Internet]. 2015 Apr;39(4):926–33. Available from: https://pubmed.ncbi.nlm.nih.gov/25479817
20. O’Brien L, Broom L, Ullah MM. Outcomes and Participant Experience of an Online Train-the-Trainer Program for Bangladeshi Health Professionals: A Case Study Evaluation. Journal of Continuing Education in the Health Professions. 2015; 35(1), 46–56. doi:10.1002/chp.21262
21. Thies KC, Bergmans E, Billington A, et al. The European Trauma Course: Transforming systems through training. Resusc Plus [Internet]. 2024 Mar 15;18:100599. Available from:
https://pubmed.ncbi.nlm.nih.gov/38515443
22. Kolb AY, Kolb DA. Experiential Learning Theory: A Dynamic, Holistic Approach to Management Learning, Education and Development [Internet]. The SAGE Handbook of Management Learning, Education and Development. SAGE Publications Ltd; 2009. p. 42–68. Available from: http://dx.doi.org/10.4135/9780857021038.n3
23. Michael Nnaemeka Ajemba, Chinweike Ikwe, Judith Chioma Iroanya. Effectiveness of simulation-based training in medical education: Assessing the impact of simulation-based training on clinical skills acquisition and retention: A systematic review. World Journal of Advanced Research and Reviews. 2024;21(1).
24. Kanneganti A, Sia CH, Ashokka B, et al. Continuing medical education during a pandemic: an academic institution’s experience. Postgrad Med J. 2020;96(1137).
25. Hancock K. Modular Online Learning Design: A Flexible Approach for Diverse Learning Needs (book review). Journal of the Canadian Health Libraries Association / Journal de l’Association des bibliothèques de la santé du Canada. 2021;42(1).