





Nutrition Risk in Older Adults: Community Care Strategies
Addressing Nutrition Risk in Older Adults in Community Settings
Megan Macaset¹˒², Rupinder Dhaliwal³and Catherine B. Chan¹˒⁴
- Department of Agricultural, Food and Nutritional Sciences, University of Alberta, Edmonton, Alberta
- Nutrition Services, Alberta Health Services, Edmonton, Alberta
- Canadian Malnutrition Task Force, Canadian Nutrition Society, Ottawa, Ontario
- Department of Physiology, University of Alberta, Edmonton, Alberta
OPEN ACCESS
PUBLISHED: 30 September 2024
CITATION: Macasae, M., Dhaliwal, R., et al., 2024. Addressing Nutrition Risk in Older Adults in Community Settings. Medical Research Archives, [online] 12(9). https://doi.org/10.18103/mra.v12i9.5893
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i9.5893
ISSN 2375-1924
ABSTRACT
Nutrition risk, and subsequent malnutrition, can be common in community-dwelling older adults in Europe and other high-income regions. While a major factor in predicting loss of independence, hospitalization and mortality, they also largely preventable, but older adults often have limited supports to prevent or manage nutrition concerns in communities, compared with hospital settings. Primary care and other community settings are well-situated to provide screening and follow-up, although several barriers may exist when implementing preventative or curative interventions. Indeed, malnutrition prevalence in older adults ranges from less than 1% to almost 20% in high-income countries, which suggests there is disparity in prevention and treatment strategies. This narrative review aims to highlight the prevalence and costs of malnutrition, then focus on recent examples of community-based nutrition risk mitigation to guide the establishment of care pathways for malnutrition management in primary and community care. In particular, care pathways incorporating routine screening, which includes monitoring of dietary intake and weight of patients, with risk-based follow-up are shown to reduce nutrition risk. Likewise, leveraging both medical interventions from dietitians and non-medical interventions such as addressing food insecurity or social isolation are required to mitigate nutrition risk.
Keywords
Nutrition risk, malnutrition, older adults, community settings, healthcare, screening
1. Introduction
Despite its high prevalence and association with other common morbidities of aging, such as frailty and cognitive decline, nutrition risk and malnutrition are largely under-detected and often untreated. Through evidence-based care pathways, screening and intervention, community-based healthcare providers can influence malnutrition-related outcomes. The purpose of this review is to provide an overview of malnutrition, a common condition occurring in older adults living independently in the community. The first objective is to define malnutrition and its risk factors, document its prevalence in a community setting and illuminate the costs of malnutrition to individuals and healthcare systems. The second objective is to provide examples of evidence-based care pathways, screening tools appropriate for primary care, and interventions that can be adapted to a variety of community-based settings. The importance of interdisciplinary teams, including supports outside the healthcare system, is also highlighted.
2. Methods
For this narrative review, a search of the literature was conducted in PubMed using search terms malnutrition, nutrition risk, older adults, community, primary care and synonyms thereof to identify publications describing the prevalence, risk factors, costs and risk mitigation strategies of malnutrition and nutrition risk. Websites of nutrition organizations that support implementation of nutrition risk screening, prevention and treatment were also consulted.
3. Discussion
3.1 DEFINITION OF MALNUTRITION
Malnutrition is a complex condition that presents in various forms in the community. It is defined as a sustained imbalance between nutrient intake and nutrient requirements due to inadequate intake, impaired nutrient absorption and/or increased energy expenditure. This imbalance can lead to muscle and fat loss, weakness, altered immune function, reduced capacity for healing and decreased cognition. In disease-related malnutrition, which is caused by any acute or chronic noncommunicable disease, inflammation is also seen, in addition to reduced food intake and absorption.
Malnutrition is commonly attributed to developing countries and has not garnered attention as an issue of concern in the Western world. Despite this widespread misbelief, malnutrition related to undernutrition or disease is prevalent and continues to go undetected and untreated. The World Health Organization (WHO) – European Region, in partnership with The European Society of Clinical Nutrition and Metabolism (ESPEN), has recently called on policy makers and healthcare professionals to acknowledge the extent of malnutrition in older adults and to take action to educate themselves and adopt practices that will lead to better patient outcomes. Engagement of physicians, including those in primary care, in supporting practices that promote screening and interventions is judged to be sub-optimal. A recent qualitative study found that the principal barriers to addressing malnutrition are incorporating malnutrition-related processes into the workflow, integrating care with specialists in nutrition, i.e. the dietitians, considerations like lack of time, lack of knowledge, lack of resources and food insecurity. On the other hand, solutions like utilizing the multi-disciplinary team, provision of clinical pathways and continuing medical education, demonstrating the efficacy of treatments and the ability to provide adequate financial support to those with food insecurity were suggested by physicians.
3.2 DEFINITION OF NUTRITION RISK
Nutrition or nutritional risk is defined as being at risk of poor nutritional status. It helps identify individuals that need further assessment to prevent or treat malnutrition or to identify populations that need targeted community programs. As people age, their physiology and body composition changes, and many factors contribute to increased nutrition risk. Guidelines for the nutrition of older adults, such as those approved by the National Nutrition Council of Finland, can help identify areas of concern including protein and Vitamin D intake. Several screening tools have also been developed to identify one’s risk of poor nutrition and/or developing malnutrition.
4. Malnutrition and nutrition risk prevalence
A limitation in defining the prevalence of malnutrition and nutrition risk is the lack of an agreed upon gold-standard measurement tool that is specific to the community setting. A systematic review of the prevalence of energy-protein malnutrition in community-dwelling populations, using 3 similar assessment tools, in adults aged 65 years and older reported varying prevalence from regions around the globe. For European countries, some had prevalence less than 1% (Sweden, Netherlands), with others ranging from 2-5% (Denmark, Finland, Poland, Ireland, United Kingdom (UK), Germany, Spain), and some countries greater than 10% (Italy, France, Czech Republic and Austria). Another meta-analysis that included only studies using one specific tool (the Mini Nutritional Assessment (MNA) assessment), reported malnutrition prevalence in Europe of 2.1% overall for community settings. Countries in other high-income regions showed similar variability (Australia 18.1%, Canada and United States of America (USA) 6%). In Canada, up to 1 in 2 adult patients admitted to hospital are malnourished, which means they came from the community in that state. Across countries, people receiving homecare had double the prevalence of malnutrition of those presenting to primary care centres (14.6% vs 7.3%) and the odds ratio for females versus males for malnutrition was 1.45 (95% CI 1.27, 1.46). In addition, those in long-term care homes may similarly be at high risk as, in a study conducted in Canadian long-term care homes, up to 1 in 2 residents were identified as malnourished.
Although malnutrition is highly prevalent in communities, it is also often preceded by a period of nutrition risk, which is similarly pervasive. A Canadian survey found that 1 in 3 adults aged >65 years old are at nutrition risk but other authors find higher risk. Borkent et al. compared nutrition risk in the Netherlands, New Zealand and Canada using the same screening tool for all 3 populations. High nutrition risk was detected in >60% of older adults, ranging from 61% in Netherlands to 70% in Canada. Those who do not attend primary care comprise an at risk population, which underscores the importance of establishing alternative, non-medical sites for screening for nutrition risk. Moreover, 1 in 4 adult patients lose at least 5 pounds of weight within 30 days of being discharged from hospital and 20% are readmitted to hospital. Most of these patients are elderly. This would suggest that better screening for and treatment of nutrition risk in the community is necessary to reduce hospitalizations and improve transitions in care.
5. Risk factors
| Physiological or medical factors | Life and social factors | Psychological factors |
|---|---|---|
| Age | Isolation & loneliness; loss of interest in life | Poor or moderate self-reported health status |
| Excessive polypharmacy and drug interactions | Poverty & food insecurity | Dementias |
| Poor appetite often related to loss of taste and smell | Lack of cooking, shopping skills and nutrition knowledge | Depression |
| Chronic disorders, e.g. affecting respiratory, endocrine & neurological systems; cancer | Inability to shop or prepare food | Bereavement |
| Poor dentition, dysphagia | Eating dependencies | Anxiety |
| Infections | Being institutionalized | Confusion |
| Chronic disorders contributing to frailty and loss of mobility | Acute diseases | Constipation |
6. Consequences and costs of high nutrition risk and malnutrition
Malnutrition can negatively affect a person’s quality of life and increases the risks for complications and mortality. In American older adults, mortality directly attributed to malnutrition using ICD-10 codes compiled by the US Centers for Disease Control and Prevention has been rising since 2013 and was estimated at 25.0 per 100,000 in 2020. While this trend might not be true for all countries, it points to insufficient responses to the challenge of malnutrition. It also does not account for the contribution of malnutrition of death from other causes. Malnutrition in adults aged 55 years or older in Denmark surged from 1999-2008, from <10 per 100,000 to approximately 40 per 100,000, likely as a result of public health policy changes. Significant excess deaths from stroke, Alzheimer’s Disease and schizophrenia were also documented. Other studies also find that malnutrition increases cause-specific mortality as determined by a prospective Swedish study, which found higher hazard ratios for mortality attributed to cancer, mental or behavioral disorders, nervous, circulatory and respiratory causes, among others. Without timely intervention, malnutrition can result in long-lasting effects such as muscle and fat loss resulting in weakness and fatigue, loss of bone mass increasing risk of falls and fractures, pressure injuries, delayed wound healing, weakened immune system leading to poor recovery from illness or surgery, increased risk of chronic diseases, and cognitive and mental health issues. A systematic review of observational and intervention trials reports a 2.85-fold higher risk of poor quality of life in the malnourished compared with well-nourished older adults.
Frailty is commonly associated with nutrition risk. A Netherlands study reports that 68% of individuals with malnutrition are frail although the converse relationship was weaker, with less than 10% of the frail population also being malnourished. Nevertheless, in practices caring for older adults, pairing nutrition risk and frailty screening could be a viable strategy because there is overlap in some of the assessment criteria, such as weight loss, decreased functional capacity and weakness. It is proposed that adding measures of walk speed and handgrip strength to a nutrition risk screening could be an approach to assessing both frailty and malnutrition in a clinical setting.
Nutrition risk is associated with poorer health outcomes, including a 50% higher risk for hospitalization for high risk community-dwelling older adults and a 54% greater risk of mortality even for those with moderate risk. According to European data summarized in a systematic review, malnutrition translates to higher healthcare utilization and cost, including primary care physician visits that can be avoided through appropriate and timely interventions. Overall, the annual cost of healthcare for a malnourished patient is about triple that of a well-nourished individual, according to UK data.
Although this review focuses on community-dwelling older adults, it is important point out that the higher risk of hospitalization translates to higher in-patient expenditures. In hospitalized patients, malnutrition is associated with an increased risk of mortality, hospital stay, and readmission. In 2016 (pre-COVID 19), costs associated with hospital malnutrition resulted in an additional annual spending of $2 billion (extra 2-3 day stay in hospital) in the Canadian healthcare system. Higher hospital charges were also reported in a US study of 400 inpatients with nutritional decline.
7. Mitigating nutrition risk
The WHO – European Region and ESPEN have issued a call to policy makers and healthcare professionals to decrease the burden of disease-related malnutrition. The main recommendations are 3-fold:
- Recognize disease-related malnutrition as a priority health issue;
- Implement nutritional care in primary care and all outpatient and inpatient care settings;
- Provide enhanced nutrition education for healthcare professionals.
In the next sections, actions that address these recommendations with respect to implementing nutritional care in a variety of community-based settings are discussed.
7.1 NUTRITION RISK PATHWAYS TO GUIDE CARE
Developing a pathway or algorithm to guide care for older adults at nutrition risk is an essential first step in providing consistent, evidence-based support. Care pathways have been developed by ESPEN, the UK, USA, Canada and Australia. An overview of the Canadian pathway is provided here, with additional detail on screening and risk mitigation strategies in sections 7.2 and 7.3.
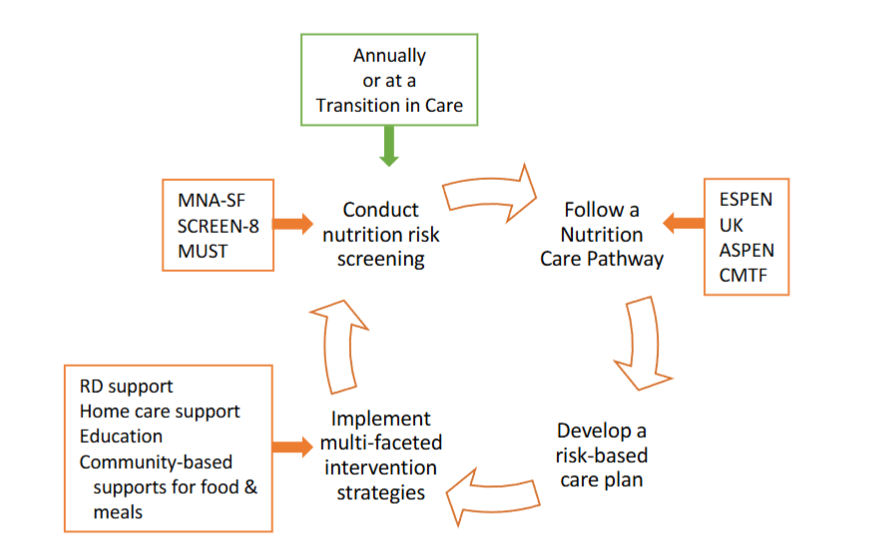
The Canadian Malnutrition Task Force (CMTF) has developed two important pathways, one for providing nutrition care to older adults in the community and the other to guide nutrition care during transitions from hospital to community in at-risk and malnourished patients. In the Primary Care Nutrition Pathway for Adults Aged 65+ developed by the CMTF, the focus is the medical home, which is defined as a team-based healthcare delivery model led by the individual’s most responsible primary healthcare provider. While this may be a dietitian, it is more likely to be a physician, nurse, social worker or other provider and the pathway has been designed to be accessible to all frontline team members. Nurses are often the first point of contact for older adults visiting their medical home or as homecare nurses caring for individuals in the community. They are well-placed to provide the initial screening and etiological assessment of nutrition risk, as well as coordination of care. The dietitian may be integral to the team or an external resource, for example in public health or private practice. Using a care pathway to help prioritize high nutrition risk patients to the specialized care of a dietitian can help with resource allocation. In the primary care setting, dietetic interventions for patients with chronic diseases and malnutrition is cost effective, with a recent review indicating that 1 dollar spent saves 5.5-100 dollars in healthcare.
The Primary Care Nutrition Pathway takes a risk-based approach and depends upon initial screening. According to the pathway, individuals found to be at low nutrition risk can be encouraged to continue their healthy eating habits and refer to provided resources (handouts, websites, etc.). Individuals at high risk or diagnosed with malnutrition should be referred to a dietitian, who can provide a complete nutritional assessment, develop an individualized treatment and nutrition care plan, coordinate care with other members of the team, and periodically reassess nutrition status. Even in the absence of a dietitian, team members can investigate the etiology of the nutrition problem, initiate diagnostics and a care plan and, at minimum, monitor weight and appetite at follow-up appointments. The healthcare team should also initiate actions to prevent malnutrition in individuals at moderate risk. In addition to investigations of etiology, providing a basic care plan, resources and community services, then following up with regular weighing and appetite monitoring can reduce progression of nutrition risk. The pathway, detailed guidance document and a basic nutrition care plan are available at the CMTF website.
Transitions in care are a critical time for intervening on nutrition risk status. If patients are diagnosed with malnutrition or high nutrition risk during a hospital stay, a transition care plan enables the community-based healthcare team to follow up appropriately with the older adult. A specific pathway has been developed for transitions from hospital to community, in which discharge from hospital is followed up by the medical home team to reassess the patient, initiate the discharge nutrition care plan, provide further investigation of etiology, provide resources and education, monitor weight and appetite and follow uptake of community services. A community dietitian may be involved in these processes. Additional research with longer follow-up is necessary to fully establish the efficacy of pathways for transitions because one study that found little benefit at 3 months reported significantly higher MNA score and lower mortality than the control group at 6 months.
Involvement of community-based organizations (CBOs) is integral to nutrition care pathways for older adults. Such organizations can support the medical home healthcare team by participating in screening as well as providing resources essential to improving nutrition, such as meal delivery and social programs. Some screening tools have been developed so that they can be administered by non-medical staff. A pilot project in Canada found that a partnership between a CBO and the local primary care organization facilitated access to screening and was feasible for the organization because they already routinely assessed clients’ needs for a variety of services. By providing the pathway and guidance from the healthcare partner, the organizations’ personnel were able to appropriately support older adults with nutrition risk. In other settings, forming a steering committee that included the voluntary sector, homecare and other stakeholders was essential in the successful spread of a nutrition and hydration programme in the UK. Volunteers from these organizations were trained in the use of the screening tool and appropriate follow-up. Such partnerships allow for a holistic approach to malnutrition, which as discussed earlier has many contributing etiologies, including financial and social risk factors.
7.2 NUTRITION RISK SCREENING
Nutrition risk screening is globally recognized by many professional bodies as an imperative step to detect and address malnutrition within all healthcare settings and is recommended to be undertaken annually. This is important because older adults are unlikely to bring ‘malnutrition’ as a primary complaint. They are conditioned to think that weight loss is beneficial and that snacking is unhealthy, not recognizing that malnutrition can co-exist with obesity. Despite this, older adults do appreciate their healthcare team addressing nutrition issues, indicating that screening could be a “wake-up” to remind people to follow healthy eating guidelines. In addition, primary healthcare teams may disregard unintended weight loss as a serious condition once life-limiting diseases have been ruled out, particularly in those with more moderate risk. Also, due to lack of training, they may not know how to help patients address their nutrition risk, highlighting the importance of providing clear guidance through a pathway.
In older adults, screening can help reduce hospital admission rates, lengths of stay, and improve functional capacity. While nutrition screening in hospitals is a robust and well-practiced method to identify malnutrition, some literature suggests that models based purely on hospital-based screening may be insufficient to address the rising magnitude of malnutrition in communities. Therefore, community-based nutrition screening in primary care and other stakeholder organizations has become an emerging avenue for detecting and preventing address malnutrition where it begins, in the community. To manage malnutrition in the community, practitioners must first develop an awareness of the validated screening tools for community-dwelling older adults, and the following paragraphs highlight examples of successful implementation of community-based screening.
7.2.1 Mini Nutritional Assessment
One screening tool validated for older adults and ambulatory care is the MNA-Short Form (MNA-SF), an abbreviated version of its predecessor MNA. The MNA and MNA-SF are recommended by ESPEN for use in older adults. One American study used the MNA-SF in multiple homecare sites to address malnutrition in community-dwelling veterans. Each program used an interdisciplinary healthcare team with physicians, nurses, nurse practitioners, dietitians, with screening largely conducted by nurses or dietitians. Screening on initial assessment was highly feasible and all programs subsequently adopted the MNA-SF into their regular visits, demonstrating the relative sustainability of this model. Some noted advantages of MNA-SF included a completion time of 5 minutes or less, minimal training or professional background requirements for use, high (94%) specificity, and high (98%) sensitivity. Several articles document that nurse-led screening and follow-up effectively reduced nutrition risk in diverse settings including rural primary care and in nurse-led nutrition classes for caregivers of community-living older adults compared to standard home care. These 2 studies demonstrate that empowering practitioners to implement screening and subsequent nutritional interventions is efficacious to reduce the prevalence and severity of malnutrition in communities, but it is unclear whether patients accessed any other healthcare professionals. For greater capacity to sustain screening, expert groups recommend the division of roles when screening and addressing malnutrition, due to the multi-factorial nature of nutrition risk. Specifically, those delivering care may benefit from using dietitian-created nutrition education materials, as accessibility to quality nutritional information is a significant determining factor in sustaining screening. Interdisciplinary collaboration may also help ease the burden of one discipline alone to manage all aspects of screening and implementation of care.
7.2.2 Other nutrition risk screening tools
The MNA and MNA-SF may have limited practicality in some settings due to lack of trained personnel to complete nutritional screening. Such clinics may benefit from the use of the Self-MNA instead, a self-administered version of the aforementioned screens with demonstrated high sensitivity and validity. Other alternatives include the Seniors in the Community: Risk Evaluation for Eating and Nutrition (SCREEN) series, a set of validated nutrition risk screens for community-dwelling older adults. The SCREEN tools are self-administered questionnaires of varied lengths designed to identify nutrition risk based on the presence of contributing factors including weight loss, low appetite, chewing/swallowing difficulties, and more. The various SCREEN versions have widespread use throughout Canada, where they were originally developed.
For instance, one study evaluated the feasibility of using SCREEN-8 in primary care networks and one CBO. The team surveyed social workers, nurses, outreach workers and members of CBOs to determine their experience and perceived barriers with screening. The majority of workers found SCREEN-8 to be acceptable and feasible, concurring that minimal training was required to administer the screen and follow its pre-determined care pathway. While some barriers to nutrition risk screening were underscored, such as limited community resources in rural communities, undefined future funding, and limited membership and personnel in CBOs, practitioners in this study endorsed that more organizations should get involved in screening. This study also demonstrates that self-administered screening tools hold particular advantages in primary care due to their ease of use and minimal training requirements.
Another nutrition risk screening tool with high acceptability among older adults is the Malnutrition Universal Screening Tool (MUST). MUST is one of the most popular nutrition screens in the UK, where it was developed, and the tool appears to primarily have criterion validity in community-based settings and some predictive validity for general practitioner visits and hospitalizations. Unlike SCREEN, one noted disadvantage is that MUST is traditionally practitioner administered but it has some potential for self-administration, as results have been shown to be highly similar to practitioner administered screens. Further research may still be necessary to verify the self-administrative capacities of MUST, though some literature has demonstrated that this screening tool can be successfully implemented in the community. A study in the UK used MUST to screen older adults at 5 clinics. Using a standardized care pathway, those screened at high or moderate nutrition risk were given nutrition counselling by a dietitian, but only those at high risk were provided additional oral nutrition supplement prescriptions. After 6 months, hospital admission rates and length of stay were reduced by nearly 50% from baseline in those with malnutrition. Nutrition risk screening also led to lower healthcare costs in the high (£997 reduction per patient) and moderate (£400 reduction per patient) nutrition risk categories. Therefore, at both the individual and institutional level, screening in primary care settings has many notable benefits.
7.2.3. Limitations and barriers to nutrition risk screening
Implementing screening processes as highlighted above must first consider the limitations and barriers of community-based screening. For instance, lack of infrastructure to train staff, initial training costs, and limited awareness of referral pathways for patients at malnutrition risk can greatly impact the success of screening programs. Other studies have highlighted that choosing a screening tool, the need for awareness building about the importance of nutrition screening in the general population, and workload capacities may also need to be considered. Individual clinics or organizations will also need to consider their unique capacity to implement screening before selecting the most appropriate tool for the population that they serve. Although there are perceived barriers to community-based nutrition screening, such practices can become a powerful pre-emptive strategy to address a growing public health problem in the aging population. As highlighted above, regular nutrition risk screening outside of hospital settings remains a future-forward step to identify and treat malnutrition.
7.3 INTERVENTION STRATEGIES
A recent scoping review of 15 intervention studies to address poor nutrition in older adults, divided them into telehealth approaches, micro-level or targeted interventions, and multi-faceted interventions. In the 2 studies that used telehealth approaches, when telephone check-ins with patients were combined with a service such as meal delivery, the outcomes were deemed more beneficial than those found in the 1 study of monitoring alone. It may be that the older clientele are less receptive to telehealth interventions than other populations. It is also possible that the efficacy of remotely administered care could be improved using strategies developed during the COVID-19 pandemic. It has been reported that screeners find the remote approach less acceptable and harder to evaluate, even when using screening tools validated for telephone administration. In addition, providing education about food-based resources and social supports available during the pandemic via telephone and web links did not improve nutrition risk scores after 3 months. The following discussion of strategies therefore focuses on traditional, face-to-face programs.
7.3.1. Interventions in primary care settings
In general, increasing protein intake of older adults is recommended to maintain muscle mass. According to the care pathway, supports recommended by the care team could include protein and calorie-dense foods, oral nutrition supplements or even enteral nutrition. Clinical actions can cost-effectively improve outcomes like physical function. A recent 3-arm randomized controlled trial of 276 Dutch community-dwelling older adults provided nutrition advice to consume protein within 30 minutes of usual physical activity compared with advice to simply increase protein (recommended at 1.2 g/kg body weight in total) versus usual intake controls (selected to consume <1.0 kg protein/kg body weight). After 6 months, both groups consuming protein-rich foods had faster 400-m walk time than controls, and greater leg extension strength. Advice to consume protein-rich foods was cost-effective relative to controls.
Additional approaches should consider the broader etiologies of malnutrition. A trial providing personalized interventions based on an algorithm that considered 9 potential modifiable risks (including use of certain pharmacotherapies, cognition, hearing and vision, mobility issues, social risks). There was no improvement in the primary outcome, nutrition risk assessed by MNA after 2 years of follow-up in the population, but those at higher risk did exhibit a trend to improved nutritional status. Moreover, cognitive decline predicted worsening nutrition risk, underscoring the importance of considering multiple risk factors.
Poor vision and dentition issues can impact nutrition status. Medical practitioners can support their older adult patients by recommending regular check-ups with their optometrists and dentists.
7.3.2. Interventions in home care settings
In the Netherlands, one-third of community dwelling older adults receiving home care were classified as undernourished. Some of the risk factors were related to poor mobility, physical symptoms like nausea, disease status and depression. In Canada, newly-referred homecare clients have a high rate of malnutrition, estimated at 21% and for those within 30 days of a hospitalization, a high risk of readmission (2.7-fold compared with well-nourished clients). Older adults already receiving home care in Finland have less prevalent malnutrition (3%) but nearly half still have nutrition risk.
In a Spanish study, caregivers of individuals receiving home care received education on nutrition interventions from a nurse. Caregivers then administered MNA screens at baseline, 6 months, and 12 months following regularly scheduled homecare follow-ups. The intervention group saw significantly greater improvements in nutritional risk scores, with increased consumption of protein-rich foods like eggs and total protein and less prevalence of malnutrition than the control group. In Israel, a dietitian-led intensive nutrition intervention was compared with physician-led usual medical care (with provision of a nutrition education booklet) in individuals ≥75 years old for 6 months. The nutrition intervention yielded improvements in dietary intake, cognition, and depressive symptoms. Lower cost associated with reduced physician visits were also documented. In a randomized study conducted in the Netherlands, customized advice from a dietitian to increase protein intake to 1.2g/kg/day and provision of protein-rich and protein-enriched foods led to significant increases in protein intake compared with controls at 6 months.
A scoping review of the effectiveness of post-hospitalization transitions in care interventions to address malnutrition with up to 3 months follow-up reports mixed results, with 6 of 9 included studies identifying at least one statistically significant benefit, with energy intake most consistently improved. Two-four home visits or telephone calls by a dietitian to provide nutrition counseling, motivation, education and weight monitoring, along with provision of oral nutritional supplements, improves energy intake and weight gain, according to Danish data. However, other studies included in the scoping review using similar inventions report no benefits on outcomes such as weight, physical function or quality of life.
7.3.3. Community-based food and meal supports
The risks for malnutrition include factors like mobility and social support that are not easily addressed by the healthcare system. The Academy of Nutrition and Dietetics and the Society for Nutrition Education and Behaviour have issued a position statement that clearly supports integration of the healthcare system with community players in order to ensure that older adults have safe access to appropriate nutrition. Involvement of community groups and social agencies is important to provide holistic interventions. Several examples appear in the literature, although there is a dearth of evaluation focused on malnutrition and nutrition risk outcomes. The available data do suggest that such programs are fundamental to care of older adults with respect to providing nutrition support.
A systematic review found 48 studies addressing nutritional status and/or nutrient intake of older adults living at home and provided with a home-delivered meal service. Although providing such meals did elicit improvements in the nutrition outcomes, recipients generally still had gaps in nutrient intake. Providing nutrition counselling or enriched or supplemented foods improved the overall nutrition.
The Greater Manchester Nutrition and Hydration Programme (GMNHP) was instigated in 2017 after a successful pilot undertaken with support from the UK Malnutrition Task Force in 2015. Success of GMNHP delivery depends on 5 key principles: 1) raising awareness; 2) identifying screening and intervention protocols and providing training to personnel; 3) partnerships and breaking down boundaries; 4) individualized care; 5) monitoring outcomes. A key part of the GMNHP is a one-stop navigation point that directs people to non-medical supports. The publication describes governance and workforce development within the GMNHP, such that there is now a plan to spread the approach to other locations and organizations. However, health-related outcomes of patients receiving screening and intervention have not yet been reported.
Since 1972, the United States has had the Older Americans Act Nutrition Program with a mandate to provide meals in the community, plus nutrition education and counseling, and access to social services in order to reduce hunger and improve food security, increase opportunities for socialization and generally promote health and well-being in older adults. Its current day activities include provision of meals in congregate settings, meal home delivery, and nutrition education, counseling, screening and assessment. Meals are required to be nutritious, appealing and individualized to address chronic disease, religious and cultural/ethnic needs and preferences. Participant satisfaction with both the congregate and home-delivery models is high, with ≥95% indicating they would recommend them to a friend. Although nutrition risk is not a criterion for enrolment, a significant proportion of the home-delivery program, in particular, have challenges with activities such as grocery shopping or meal preparation, and more than 60% have ≥6 chronic health conditions.
Independent evaluation of the program benefits includes reduced hospitalizations, keeping people in their homes and reducing food insecurity.
A survey of older adults receiving home delivery of meals found that only 20-30% of meal recipients met nutritional recommendations for energy and macronutrients, with the best outcomes in people receiving 2 or 3 meals per day. Other studies have tried to identify ways of enhancing outcomes. For example, a U.S.-based pilot study assessed nutrition risk and dietary intake pre-post initiation of a meal delivery service by self-report. Significant improvements in these outcomes as well as food security, less loneliness and better social well-being were observed. Similarly, providing 3 meals/day to a group of older adults in their homes decreased nutrition risk and increased physical functioning. However, another attempt produced unintended consequences, with participants allowed to choose their own meals selecting foods lower in protein, fat, and calories. The authors suggest that providing nutritional counselling before allowing participants to choose may result in better outcomes.
Providing meals during hospital to community transitions has also been studied. In the COMEAT trial, older patients with low socioeconomic status were randomized to receive a delivered dinner meal vs no support. The intervention improved survival at 6 months by 20% and those in the intervention had a higher Hospital Anxiety and Depression Scale but nutrition-related outcomes were not directly assessed. A pilot randomized controlled trial provided 10 days of home meal delivery and nutrition education vs usual care and nutrition education. Feasibility and client satisfaction criteria were met, with 87% of participants retained for follow-up. The meal delivery increased participants’ energy intake but the duration of the program was quite short. Conversely, in an analysis of real-world practices, in patients ≥65 years discharged from hospital after screening as high nutrition risk, there was less than 2-point improvement in the MNA score, which was likely attributable to less than 20% of those discharged receiving a post-discharge nutrition review by a dietitian and/or nutrition supports at home. Thus, while meal delivery services may improve outcomes, the intensity, duration and feasibility of such interventions is not well-studied.
8. Conclusion
Nutrition risk is highly prevalent but under-recognized among community dwelling older adults living in high income countries. Nutrition risk screening and appropriate interventions in primary care and community settings can cost-effectively alleviate the burden of malnutrition. The involvement of multi-disciplinary teams and community organizations, not just dietitians, can increase capacity.
References
- McKinlay AW. Malnutrition: the spectre at the feast. J R Coll Physicians Edinb. 2008;38:317-321.
- Cederholm T, R B, Austin P, et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin Nutr. 2017;36:49-64. doi:10.1016/j.clnu.2016.09.004
- World Health Organisation – European Region. Disease-related malnutrition: a time for action. 2023.
- Veldhuijzen van Zanten D, Vantomme E, Ford K, et al. Physician perspectives on malnutrition screening, diagnosis, and management: A qualitative analysis. Nutrients. 2024;16:2215. doi:10.3390/nu16142215
- Ramage-Morin PL, Gilmour H, Rotermann M. Nutritional risk, hospitalization and mortality among community-dwelling Canadians aged 65 or older. vol 82-003-X. Statistics Canada; 2017.
- Keller HH, Haresign H, Brockest B. Process evaluation of Bringing Nutrition Screening to Seniors in Canada (BNSS). Can J Diet Pract Res. 2007;68:86-91. doi:10.3148/68.2.2007.86
- Suominen MH, Jyvakorpi SK, Pitkala KH, et al. Nutritional guidelines for older people in Finland. J Nutr Health Aging. 2014;18(10):861-867. doi:10.1007/s12603-014-0509-1
- Seron-Arbeola C, Labarta-Monzon L, Puzo-Foncillas J, Mallor-Bonet T, Lafita-Lopez A, Bueno-Vid. Nutrition screening tools: an analysis of the evidence. J Parenter Enteral Nutr. 2012;36(3):292-8. doi:10.3390/nu14122392
- Crichton M, Craven D, Mackay H, Marx W, de van der Schueren M, Marshall S. A systematic review, meta-analysis and meta-regression of the prevalence of protein-energy malnutrition: associations with geographical region and sex. Age Ageing. Jan 1 2019;48(1):38-48. doi:10.1093/ageing/afy144
- Cereda E, Pedrolli C, Klersy C, et al. Nutritional status in older persons according to healthcare setting: A systematic review and meta-analysis of prevalence data using MNA. Clin Nutr. 2016;35:1282-1290. doi:10.1016/j.clnu.2016.03.008
- Allard JP, Keller H, Teterina A, et al. Factors associated with nutritional decline in hospitalised medical and surgical patients admitted for 7 d or more: a prospective cohort study. Br J Nutr. 2015;114(10):1612-1622.
- Keller H, Vucea V, Slaughter SE, et al. Prevalence of malnutrition or risk in residents in long term care: Comparison of four tools. J Nutr Gerontol Geriatr. Oct-Dec 2019;38(4):329-344. doi:10.1080/21551197.2019.1640165
- Borkent JW, Keller H, Wham C, Wijers F, de van der Schueren MAE. Cross-country differences and similarities in undernutrition prevalence and risk as measured by SCREEN II in community-dwelling older adults. Healthcare. 2020;8:151. doi:10.3390/healthcare8020151
- Klemenc-Ketis Z, Ruzic Gorenjec N, Blagus R, Blaz Kovac M, Poplas Susic A. Risk for malnutrition in family practice non-attenders living in the community: A cross-sectional study from Slovenia. Nutrition. Apr 2020;72:110657. doi:10.1016/j.nut.2019.110657
- Allard JP, Keller H, Jeejeebhoy KN, et al. Malnutrition at hospital admission-contributors and effect on length of stay: A prospective cohort study from the Canadian Malnutrition Task Force. JPEN J Parenter Enteral Nutr. 2016;40(4):487-497.
- Keller H, Laporte M, Payette H, et al. Prevalence and predictors of weight change post discharge from hospital: a study of the Canadian Malnutrition Task Force. Eur J Clin Nutr. 2017;71(6):766-772.
- Hickson M. Malnutrition and aging. Postgrad Med J. 2006;82(963):2-8. doi:10.1136/pgmj.2005.037564
- Favaro-Moreira NC, Krausch-Hofmann S, Matthys C, et al. Risk factors for malnutrition in older adults: A systematic review of the literature based on longitudinal data. Adv Nutr. May 2016;7(3):507-22. doi:10.3945/an.115.011254
- Mostafa N, Sayed A, Rashad O, Baqal O. Malnutrition-related mortality trends in older adults in the United States from 1999 to 2020. BMC Med. 2023;21:421. doi:10.1186/s12916-023-03143-8
- Sparre-Sorensen M, Kristensen GN. Malnutrition related deaths. Clin Nutr. 2016;15:63068. doi:10.1016/j.clnesp.2016.06.001
- Soderstrom L, Rosenblad A, Adolfsson T, Bergkvist L. Malnutrition is associated with increased mortality in older adults regardless of the cause of death Br J Nutr. 2017;117(4):532-540. doi:10.1017/S0007114517000435
- Norman K, Hass U, Pirlich M. Malnutrition in older adults–recent advances and remaining challenges Nutrients. 2021;13(8):2764. doi:10.3390/nu13082764
- Rasheed S, Woods RT. Malnutrition and quality of life in older people: a systematic review and meta-analysis. Aging Res Rev. 2013;12(2):561-566. doi:10.1016/j.arr.2012.11.003
- Verlaan S, Ligthart-Melis GC, Wijers SLJ, Cederholm T, Maier AB, de van der Schueren MAE. High prevalence of physical frailty among community-dwelling malnourished older adults-A systematic review and meta-analysis. J Am Med Dir Assoc. May 1 2017;18(5):374-382. doi:10.1016/j.jamda.2016.12.074
- Laur CV, McNicholl R, Valaitis R, Keller HH. Malnutrition or frailty? Overlap and evidence gaps in the diagnosis and treatment of frailty and malnutrition. Appl Physiol Nutr Metab. 2017;42(5):449-458.
- Buys DR, Roth DL, Ritchie CS, et al. Nutritional risk and body mass index predict hospitalization, nursing home admissions, and mortality in community-dwelling older adults: results from the UAB Study of Aging with 8.5 years of follow-up. J Gerontol A Biol Sci Med Sci. Sep 2014;69(9):1146-53. doi:10.1093/gerona/glu024
- Abizanda P, Sinclair A, Barcons N, Lizan L, Rodriguez-Manas L. Costs of malnutrition in institutionalized and community-dwelling older adults: A systematic review. J Am Med Dir Assoc. Jan 2016;17(1):17-23. doi:10.1016/j.jamda.2015.07.005
- Curtis LJ, Bernier P, Jeejeebhoy K, et al. Costs of hospital malnutrition. Clin Nutr. 2017;36(5):1391-1396. doi:10.1016/j.clnu.2016.09.009
- Agarwal E, Ferguson M, Banks M, et al. Malnutrition and poor food intake are associated with prolonged hospital stay, frequent readmissions, and greater in-hospital mortality: results from the Nutrition Care Day Survey 2010. Clin Nutr. Oct 2013;32(5):737-45. doi:10.1016/j.clnu.2012.11.021