

EBV-Positive CD8+ T-Cell Lymphoma Post-Transplant Case Study
An autopsy case of EBV-positive CD8+ T cell lymphoma after allogeneic transplantation of peripheral blood stem cells
Abbreviations
PTLD- posttransplant lymphoproliferative disorder
EBV- Epstein-Barr virus
allo-HSCT- allogeneic hematopoietic stem cell transplantation
PBSC- peripheral blood stem cells
DLBCL- diffuse large B cell lymphoma
AITL- angioimmunoblastic T-cell lymphoma
SOS- sinusoidal obstruction syndrome
VOD- veno-occlusive disease
TFH- follicular helper T
Introduction
Posttransplant lymphoproliferative disorder (PTLD) encompasses a broad spectrum of lymphoid and plasmacytic proliferations that occur in immunocompromised patients following transplantation. PTLD is particularly well-documented after allogeneic hematopoietic stem cell transplantation (allo-HSCT). PTLD is most commonly associated with B-cell disorders, frequently linked to Epstein-Barr virus (EBV) infection¹. In contrast, T-cell PTLD is exceptionally rare and has a lower association with EBV².
A case series and systematic review highlighted that T-cell PTLD is more likely to arise from the proliferation of donor-derived T cells and can exhibit various morphologies, including both monomorphic and polymorphic types². Another study emphasized the rarity of T-cell PTLD, noting that it accounted for only 4 cases (0.39%) out of 1015 allo-HSCT patients³. T-cell PTLD generally presents with a later onset and has an unfavorable prognosis compared to its B-cell counterpart⁴. Pathologically, T-cell PTLD displays considerable diversity, encompassing peripheral T-cell lymphoma, not otherwise specified (PTCL, NOS), hepatosplenic T-cell lymphoma, and cutaneous T-cell lymphoma⁴. Unlike B-cell PTLD, T-cell PTLD are less frequently associated with EBV infection, with only about one-third of cases showing EBV positivity. Despite this, in some instances, EBV-positive T-cell PTLD may exhibit monoclonal expansion of EBV-infected cells, complicating the clinical course and outcomes⁵.
In this case report, we present a rare and unique case of EBV-positive CD8+ T-cell PTLD that developed after allo-HSCT. Given the monoclonality of the CD8+ cells, the final diagnosis of “EBV-positive CD8+ T-cell lymphoma” was established in accordance with the WHO Classification of Haematolymphoid Tumours, 5th edition⁶. This case underscores the complexity of T-cell PTLD and highlights the need for further research to elucidate the mechanisms driving its development.
Case report
A 57-year-old man was diagnosed as EBV-positive DLBCL based on a biopsy of an inguinal lymph node. Chemotherapy of R-CHOP 5 courses and CHASER 2 courses were performed, but the disease progressed. The pathological diagnosis was reviewed, and the revised diagnosis was AITL with secondary development of EBV-positive DLBCL.
A year after the first diagnosis, he received an allogeneic PBSCT using a reduced-intensity conditioning regimen with fludarabine/melphalan 140 mg/m² (Flu/Mel140). On day 14 post-PBSCT, dysfunction of the liver and kidneys developed, and sinusoidal obstruction syndrome (SOS)/veno-occlusive disease (VOD) was suspected. The patient was admitted to the intensive care unit. Due to severe diarrhea, a complication of thrombotic microangiopathy (TMA) or graft versus host disease (GVHD) was suspected, and steroid therapy was performed. The liver function was recovered, but the renal dysfunction remained. He underwent dialysis three times a week. After that, his general condition improved, and steroids were gradually tapered off. On day 30, neutrophil engraftment was confirmed, and on day 36, complete engraftment of donor-derived cells was observed with bone marrow examination (complete chimerism). His clinical status was stable for over two months.
However, on day 106, severe liver dysfunction suddenly developed, with a rapid increase in T cell count in the peripheral blood. On day 113, southern blot analysis revealed the presence of the EBV genome in the peripheral blood, and the distinct single DNA fragment indicated monoclonal expansion. Steroid pulse therapy was performed, and rituximab was also administered. However, he passed away on day 114 post-PBSCT.
Pathological findings of inguinal lymph node (biopsy)
Pathological findings of the inguinal lymph node, obtained by biopsy, were intensively described elsewhere (Shishido-Hara et al, Med Res Arch, in press). Normal lymph node architecture was disrupted, and immunohistochemistry (IHC) displayed a diffuse distribution of T cells throughout the lymph nodes. High endothelial venules were apparent, and they were surrounded by relatively homogeneous atypical lymphocytes. The atypical cells displayed distinct expression of CD10 and PD-1, as well as mild-to-moderate expression of Bcl-6, indicating neoplastic follicular helper T (TFH) cells, and the pathological diagnosis of AITL was defined. There were also atypically large cells with distinct nuclei, which were CD20-positive. The cells were also positive for EBER-ISH and were labeled with MIB-1. Thus, the diagnosis of DLBCL was also determined. The DLBCL lesion was focal and was thought to be developed to succeed the AITL lesion.
An autopsy on 114 days post-allogeneic transplantation of stem cells.
The patient died on day 114 after transplantation, and an autopsy was performed. In post-mortem lymph nodes, pathology of either AITL or DLBCL was not observed. Instead, diffuse infiltration of small T-lymphocytes was seen. Most cells in the nodes were CD8-positive T cells, and EBV infection was recognized using EBER-ISH (Fig. 1).
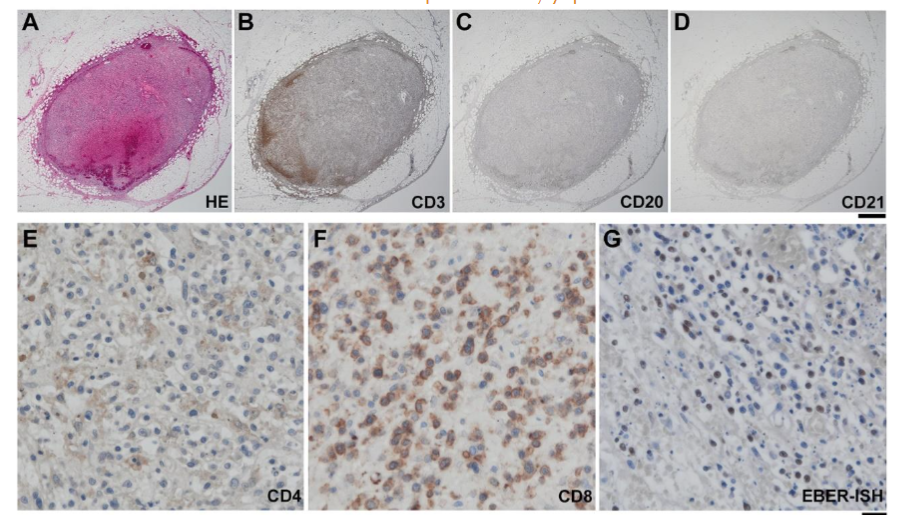
Figure. 1: The post-mortem lymph node with atypical EBV-positive CD8⁺ cells.
In the post-mortem lymph nodes, atypical CD8⁺ cells were present diffusely. They were positive for EBER-ISH. B cells were absent, and FDC meshwork was also not seen. Scale bars: 1 mm for A-D, 20 mm for E-G.
The liver (1908g) was reddish-brown (Fig. 2A), and histologically, hemosiderin deposition was observed around the central vein. Silver impregnation showed obstruction of the central vein and surrounding sinusoids, indicating SOS/VOD (data not shown). Lymphocytes were clustered mainly in the portal vein area and were CD8⁺ T cells (Fig. 2B, C). The spleen (440g) was highly congested (Fig. 2D). Given the findings of SOS/VOD in the liver, portal hypertension was considered a major cause of splenomegaly. Histologically, the white pulp was diminished, and hemosiderin deposition was also apparent (data not shown). Atypical lymphocytes were clustered mainly around the splenic artery, all CD8-positive T cells (Fig. 2E, F).
Intestinal hemorrhage was seen only in the superficial mucosal layer, mainly in the distal ileum and part of the cecum (Fig. 2G). Histologically, hemorrhagic change was not observed in deeper than the submucosal layer. The superficial mucosa was elevated in a papillary fashion, in which narrow vascular stroma (Fig. 2H) and CD8⁺ T cells migrated in lumens of small vessels. The cells were also positive for EBER-ISH (Fig. 2I-K). Similar findings were also found in the stomach and esophagus. TMA and GVHD were clinically suspected, but the pathology did not indicate their likeness.
Atypical EBV-positive, CD8⁺ T cells were found systemically in the lumen of all the blood vessels. In bilateral lungs (left 579g, right 637g), atypical EBV-positive CD8⁺ T cells were densely invading beneath the bronchial epithelium and migrating prominently in the capillaries of all the alveolar septa. They were also positive for EBER-ISH (Fig. 2L-O).
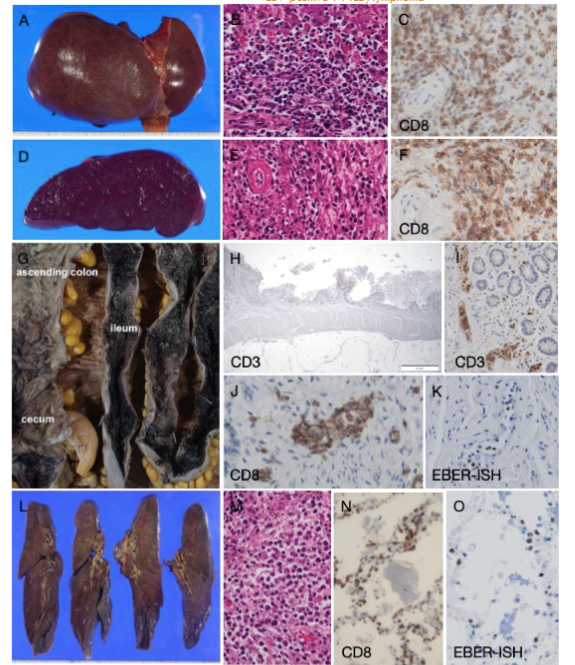
Figure. 2: Pathology of the liver, spleen, small and large intestines, and lungs.
A-C: Liver, weighed 1908g. Atypical CD8⁺ T cells were clustered in portal areas.
D-F: Spleen, weighted 440g. The spleen was markedly congested, and atypical CD8⁺ T cells were clustered around splenic arteries.
G-K: Small and large intestines. Surface mucosa was hemorrhagic in the ileum and partially in the cecum. Intestinal mucosa was elevated in a papillary fashion, where EBV-positive CD8⁺ T cells migrate in blood vessel lumens.
L-O: Lungs, weighted left 579g, right 637g. Atypical CD8⁺ T-cells were observed everywhere in the capillary lumen. They were also EBV-positive.
One day before his death, EBV DNA was examined in peripheral blood cells using southern blot analysis (Fig. 3). On electrophoresis, the positive control of chronic active EBV infection (lane 1 in Fig. 3) was developed into multiple bands, while this case showed a distinct single band of the EBV DNA genome, indicating monoclonality (lane 3). The data simultaneously revealed the monoclonal expansion of EBV-infected T cells, indicating EBV-related CD8⁺ T cell lymphoma, NOS.
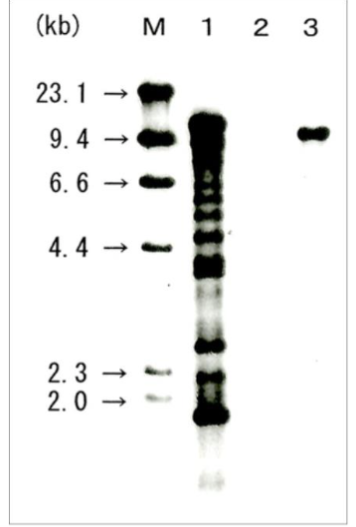
Figure. 3: Southern blot analysis of EBV-DNA in peripheral blood cells.
Detection of monoclonal EBV DNA genome indicated monoclonal expansion of EBV-infected cells. Lane 1 (PC): positive control (chronic active EBV infection), Lane 2 (NC): negative control, Lane 3: the present case.
Discussion
This study presents a rare instance of EBV-positive CD8⁺ T-cell lymphoma that developed after allo-HSCT. The patient, who initially suffered from AITL with secondary EBV-positive DLBCL, experienced a monoclonal expansion of EBV-infected CD8⁺ T cells. Systemic infiltration of EBV-positive CD8⁺ T cells was observed in multiple organs, including the liver, spleen, gastrointestinal tract, and lungs, leading to the final diagnosis of EBV-positive CD8⁺ T-cell lymphoma. The progression of this disorder illustrates the challenges in managing PTLD, especially those involving T cells, which are less commonly associated with EBV infection and often exhibit aggressive clinical behavior.
In 2022, the WHO Classification of Haematolymphoid Tumours, 5th Edition (WHO-HAEM5), introduced changes to categorizing immunodeficiency-associated lymphoid proliferations and lymphomas⁶. The previous edition (WHO-HAEM4R) classified these based on the cause of immunodeficiency, but WHO-HAEM5 now emphasizes a three-part nomenclature that includes histopathological features, viral infection, and the cause of immunodeficiency. This case, therefore, is diagnosed as “CD8⁺ T-cell lymphoma, EBV-positive, post-allogenic [transplantation of PBSC]” under the new classification (Figure 3).

Figure. 3: Three-part nomenclature for lymphoid proliferations and lymphomas arising in immune deficiency/dysregulation.
The cause of PTLDs is not fully understood, but a strong association between Epstein-Barr virus (EBV) infection and the pathophysiology of these disorders, particularly in B cells, is suggested⁷⁻⁹. A recent study, in vitro, has reported that EBV can induce the expression of the inosine-5′-monophosphate dehydrogenase 2 (IMPDH2) gene of cells, which is the rate-limiting enzyme for de novo GTP synthesis. This process is crucial for the transformation and proliferation of B cells within the context of PTLDs¹⁰, where EBV-positive B cells or plasma cells are frequently observed to undergo malignant growth. On the other hand, T-cell PTLD is exceedingly rare³, and the role of EBV in its pathogenesis remains less clearly defined. While molecular and genomic alterations in T/NK-cell PTLDs have been found to resemble those seen in peripheral T-cell lymphomas in immunocompetent individuals¹¹, the specific involvement of EBV is not well elucidated. It has been reported, however, that EBV type 2 can latently infect T cells, utilizing glycoprotein gp350 and CD21 as receptors for viral entry¹²˒¹³. This viral infection may potentially enhance IMPDH activity, thereby promoting T-cell proliferation¹⁴. The pathological diagnosis of T-cell PTLDs is highly variable, encompassing a spectrum that ranges from benign lymphocytic hyperplasia to aggressive high-grade lymphomas⁵˒¹⁵. In this particular case, however, the findings strongly suggest a connection between EBV infection and the development of a rare T-cell PTLD, as evidenced by the monoclonal expansion of CD8⁺ T cells, culminating in a distinct CD8⁺ T-cell lymphoma.
Conclusion
In conclusion, this autopsy case represents a rare instance of monoclonal proliferation of EBER-positive CD8⁺ T cells following allo-HSCT. Although the pathological diagnosis, based on a biopsy of an inguinal lymph node, identified AITL with secondary EBV-positive DLBCL, post-mortem analysis revealed the absence of neoplastic CD4⁺ T cells or EBV-positive atypical B cells. Despite the complete engraftment of donor-derived cells in the bone marrow (complete chimerism) on day 36 post-transplantation, the proliferation of EBER-positive CD8⁺ T cells by day 106 was observed. Continued documentation and analysis of similar cases will advance our understanding of T-cell PTLD and potentially unveil new pathways and therapeutic strategies.
Acknowledgments
The authors thank Toshifumi Kawamura and Takashi Okuda for excellent technical assistance.
COI
JK received support or honoraria from Kyowa Kirin, Mochida Pharmaceutical, Sanofi, Chugai Pharmaceutical, Bristol Myers Squibb (BMS), Takeda Pharmaceutical, Ono Pharmaceutical, and Janssen Pharmaceutical, and consulting fees from Janssen Pharmaceutical and BMS.
References
1. Al Hamed R, Bazarbachi AH, Mohty M. Epstein-Barr virus-related post-transplant lymphoproliferative disease (EBV-PTLD) in the setting of allogeneic stem cell transplantation: a comprehensive review from pathogenesis to forthcoming treatment modalities. Bone Marrow Transplant. Jan 2020;55(1):25-39. doi:10.1038/s41409-019-0548-7
2. Jiang C, Huang J, Shao J, et al. T-Cell Posttransplant Lymphoproliferative Disorders After Allogeneic Hematopoietic Stem Cell Transplantation: Case Series and Systemic Review. Cell Transplant. Jan-Dec 2024;33:9636897241259722. doi:10.1177/09636897241259722
3. Kuno M, Ito A, Maeshima AM, et al. T-cell posttransplant lymphoproliferative disorders after allogeneic hematopoietic cell transplantation. Int J Hematol. Aug 2020;112(2):193-199. doi:10.1007/s12185-020-02890-1
4. Tiede C, Maecker-Kolhoff B, Klein C, Kreipe H, Hussein K. Risk factors and prognosis in T-cell posttransplantation lymphoproliferative diseases: reevaluation of 163 cases. Transplantation. Feb 15 2013;95(3):479-88. doi:10.1097/TP.0b013e3182762e07
5. Quintanilla-Martinez L, Swerdlow SH, Tousseyn T, Barrionuevo C, Nakamura S, Jaffe ES. New concepts in EBV-associated B, T, and NK cell lymphoproliferative disorders. Virchows Arch. Jan 2023;482(1):227-244. doi:10.1007/s00428-022-03414-4
6. Alaggio R, Amador C, Anagnostopoulos I, et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia. Jul 2022;36(7):1720-1748. doi:10.1038/s41375-022-01620-2
7. Morscio J, Tousseyn T. Recent insights in the pathogenesis of post-transplantation lymphoproliferative disorders. World J Transplant. Sep 24 2016;6(3):505-16. doi:10.5500/wjt.v6.i3.505
8. Styczynski J, van der Velden W, Fox CP, et al. Management of Epstein-Barr Virus infections and post-transplant lymphoproliferative disorders in patients after allogeneic hematopoietic stem cell transplantation: Sixth European Conference on Infections in Leukemia (ECIL-6) guidelines. Haematologica. Jul 2016;101(7):803-11. doi:10.3324/haematol.2016.144428
9. Dojcinov SD, Quintanilla-Martinez L. How I Diagnose EBV-Positive B- and T-Cell Lymphoproliferative Disorders. Am J Clin Pathol. Jan 4 2023;159(1):14-33. doi:10.1093/ajcp/aqac105
10. Sugimoto A, Watanabe T, Matsuoka K, et al. Growth Transformation of B Cells by Epstein-Barr Virus Requires IMPDH2 Induction and Nucleolar Hypertrophy. Microbiol Spectr. Aug 17 2023;11(4):e0044023. doi:10.1128/spectrum.00440-23
11. Margolskee E, Jobanputra V, Jain P, et al. Genetic landscape of T- and NK-cell post-transplant lymphoproliferative disorders. Oncotarget. Jun 21 2016;7(25):37636-37648. doi:10.18632/oncotarget.9400
12. Coleman CB, Wohlford EM, Smith NA, et al. Epstein-Barr virus type 2 latently infects T cells, inducing an atypical activation characterized by expression of lymphotactic cytokines. J Virol. Feb 2015;89(4):2301-12. doi:10.1128/JVI.03001-14
13. Smith NA, Coleman CB, Gewurz BE, Rochford R. CD21 (Complement Receptor 2) Is the Receptor for Epstein-Barr Virus Entry into T Cells. J Virol. May 18 2020;94(11)doi:10.1128/JVI.00428-20
14. Dayton JS, Lindsten T, Thompson CB, Mitchell BS. Effects of human T lymphocyte activation on inosine monophosphate dehydrogenase expression. J Immunol. Feb 1 1994;152(3):984-91.
15. Clerico M, Dogliotti I, Aroldi A, et al. Post-Transplant Lymphoproliferative Disease (PTLD) after Allogeneic Hematopoietic Stem Cell Transplantation: Biology and Treatment Options. J Clin Med. Dec 19 2022;11(24)doi:10.3390/jcm11247542
Most read articles by the same author(s)
- Yukiko Shishido-Hara, Aya Miyagawa-Hayashino, Junya Kuroda, B-cell maturation in angioimmunoblastic T cell lymphoma (AITL): Development of secondary diffuse large B cell lymphoma (DLBCL) is likely associated with Attygalle patterns II and III , Medical Research Archives: Vol 12 No 9 (2024): Vol 12 No 9 (2024): September ISSUE, Issue 9, VOl.12