





Hybrid Care for Type 1 Diabetes in Older Adults
Hybrid care model: Combining telemedicine and office visits for diabetes management in older adults with type 1 diabetes
Elena Toschi, MD1,2,3; Atif Adam, PHD, MPH, MD1; Nana Frimpong, BA4; Rebecca Hurlbert, BA1; Christine Slyne, BA1; Lori Laffel, MD, MPH1,2,3,5; Medha Munshi, MD1,2,3
- Joslin Diabetes Center
- Beth Israel Deaconess Medical Center
- Harvard Medical School
- Drexel University College of Medicine
- Boston Children’s Hospital
OPEN ACCESS
PUBLISHED: 30 September 2024
CITATION: Toschi, E., Adam, A., et al., 2024. Hybrid care model: Combining telemedicine and office visits for diabetes management in older adults with type 1 diabetes. Medical Research Archives, [online] 12(9). https://doi.org/10.18103/mra.v12i9.5728
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i9.5728
ISSN 2375-1924
ABSTRACT
Aims: To evaluate the use of hybrid (telehealth and in-person) care on visitation and glycaemia in older adults with type 1 diabetes (T1D).
Methods: In this retrospective study, we examined clinical characteristics, number of visits (telehealth and in-person) and continuous glucose monitoring (CGM) metrics for older adults (≥65 years) with T1D from electronic health records during the pre-COVID-19 pandemic (March 1, 2019-March 1, 2020; in-person) and pandemic (September 1, 2020-August 31, 2021; hybrid) periods. Main outcomes were the number of visits and changes in glycaemic control (HbA1c), and in a sub-group of older adults using CGM, changes in CGM metrics between in-person and hybrid care.
Results: We analysed data of 661 older adults with T1D (age 72±5 years). The hybrid care resulted in an increased number of annual diabetes visits (6.3 vs 4.2 visits/person) without change in glycaemic control (HbA1c 7.4% vs 7.2%) compared with in-person care alone. In the sub-group of 299 older adults with T1D using CGM, hybrid care compared with in-person care resulted in an improvement of time-in-range (70-180 mg/dL) (68% to 71%; p<0.001) without increasing hypoglycaemia (<70 mg/dL).
Conclusion: Compared with in-person only visits, hybrid care maintained visit frequency and preserved glycaemic control measured as HbA1c. In a sub-group of older adults with T1D using CGM, time-in-range improved while time in hypoglycaemia did not change. These data suggest that a hybrid care model is efficacious in maintaining visitation and glycaemic control, and, as demonstrated in a sub-group of older adults with T1D using CGM, safe with respect to time in hypoglycaemia.
Keywords
type 1 diabetes, t1d, management, older adults, telehealth, telemedicine, hybrid care, A1C, hypoglycaemia, continuous glucose monitor
Introduction
Older adults (age≥65) with type 1 diabetes (T1D) are a growing population world-wide. Older adults with T1D face unique challenges for their diabetes management, such as increasing concerns related to risk of hypoglycaemia and cognitive decline with aging, and that generally requires intensive insulin replacement therapy. In addition to diabetes management, older adults tend to have multiple comorbidities and other psychosocial barriers to timely care, such as transportation issues and caregiver needs that can make it difficult to maintain in-person clinic visits. However, regular clinical visits are important in this population to maintain glycaemic control and mitigate their risk of hypoglycaemia.
Telemedicine offers an alternative to in-person visits for diabetes management. Telemedicine services carry potential opportunities to expand access to care and reduce costs. However, it also carries limitations due to lack of physical exam and laboratory data, which are instrumental for clinicians to assess health conditions and guide therapy. Older people who are at higher risk of health deterioration may be less proficient in using new technology and/or lack the right equipment (Wi-Fi connection, smart devices) that may impair their ability to use and benefit from telemedicine encounters.
For older adults, in particular, telemedicine holds the potential to expand access to care. Currently, access to specialists for Type 1 Diabetes (T1D) is limited. However, management of T1D requires frequent, uninterrupted follow-up to maintain good glycemic control and reduce the risk of poor diabetes-related outcomes. A few studies have assessed telehealth’s impact on clinical outcomes and economic benefits in T1D, supporting its use. However, there is need for studies to focus on the use of telehealth in older persons with T1D. This age group, which has been growing over the last few decades, is particularly vulnerable to hypoglycemia and its poor consequences, as well as long-term diabetes complications. The use of continuous glucose monitoring (CGM) has been shown to be beneficial in mitigating hypoglycemia in this age group and allows data sharing with the clinicians virtually. Since the COVID-19 pandemic, telemedicine has become a major modality by which to deliver care for older adults with T1D.
The natural experiment created by the COVID-19 pandemic, that required rapid implementation of telemedicine, offers a unique opportunity to evaluate the impact of the hybrid care model (combined telemedicine and in-person visits) that occurred during the pandemic period, and to compare that model with an in-person only care model before the pandemic. Currently, there are ongoing considerations as to whether and how to continue the use of telemedicine in the future. Data have shown that a hybrid care model was effective in maintaining continuity of care as seen by the maintenance of clinical visit frequency from all adults with T1D, including older adults. However, the impact of hybrid care on glycaemic control and risk of hypoglycaemia in older adults with T1D is not well understood. Such information can help to inform the safety and efficacy of hybrid care in the management of diabetes in older adults with T1D.
We conducted a retrospective analysis in which we examined electronic health records to evaluate the impact of hybrid care on the number of visits and glycaemic control in older adults with T1D. In addition, we examined glycaemic metrics and time spent in hypoglycaemia in a sub-group of older adults with T1D using continuous glucose monitoring (CGM).
Materials and Methods
In this retrospective data analysis, we examined data from electronic health records at the Joslin Diabetes Center, a tertiary diabetes care facility. The local Institutional Review Board approved this study and all data were de-identified. This study was executed in accordance with the Declaration of Helsinki as revised in 2013.
Data covering two time periods, before the pandemic (pre-pandemic: March 1, 2019-March 1, 2020) and during the pandemic (pandemic: September 1, 2020-August 31, 2021), were retrieved. The period from March 1st, 2020 to August 31st, 2020 was excluded due to pandemic lockdown necessitating an urgent need to transition from in-person to telemedicine visits with minimal to no in-person visits and no laboratory access other than for exceptionally urgent clinical needs. Inclusion criteria were a diagnosis of type 1 diabetes (defined by ICD 10 codes E10.XX), duration of diabetes ≥1 year, older age (≥65), and receipt of one or more insulin prescriptions. Exclusion criteria included type 2 diabetes, age <65, dysglycemia codes. In addition, patients selected for this analysis needed to have had at least 1 appointment in pre-pandemic (in-person care): April 1, 2019 – March 1, 2020 and on HbA1c values as well as 1 appointment during pandemic (hybrid care): September 1, 2020 – August 31, 2021 with HbA1c.
Information regarding clinical and sociodemographic characteristics as well as modalities of diabetes treatment and glucose monitoring were collected. Laboratory data for HbA1c and data from CGM were retrieved.
Data were analysed using STATA, version 15.0. Data are reported as means, standard deviations, lower and upper range, and percentages, as appropriate. The analyses included comparisons between the pre-pandemic and pandemic periods with respect to the annualized number of diabetes visits with medical doctors and nurse practitioners, and the laboratory HbA1c measurements for the entire sample. The mean HbA1c was computed as the average of all measurements taken for each patient within the pre-pandemic and pandemic periods and was adjusted for the number of tests conducted. Additional analyses looked at comparisons of CGM metrics from the sub-group with available CGM data in both periods. Comparisons between the attributes utilized paired t-tests for normally distributed continuous variables, non-parametric tests for non-normally distributed variables, and chi-square tests for categorical variables. Time-series bar charts depict group differences graphically. A type 1 error of .05 provided significance in these analyses with no correction for multiple comparisons, as these were a priori hypotheses.
Results
We identified 661 unique older adults with T1D. The demographic and clinical characteristics appear in Table 1. Fifty-five percent of the older adults were female gender. In the pre-pandemic period, the mean (SD) age of the older adults identified was 72±12 years, diabetes duration was 41±17 years. Glucose control as HbA1c (%) was 7.4±0.9 in the in-person (pre-pandemic period) and 7.2±1.1 in telemedicine (pandemic period) (P=0.18), In the pre-pandemic period CGM users were 382 (58%) and pump users were 477(72%); while during the pandemic period CGM users 477(72%) and pump users were 279(42%). Visits in the pre-pandemic period were almost all in-person, averaging 4.2 annualized visits/person (CI 3.9-4.4), of which <2% were performed as phone visits. During the pandemic hybrid care, the annualized mean number of visits was significantly greater than in the pre-pandemic period, at 6.3 visits/person (CI 5.7-6.9) (p<0.01); represented by 30% in-office visits, 38% by video telehealth visits, and 32% by phone visits.
| In-person care Pre-pandemic | Hybrid care Pandemic | |
|---|---|---|
| N | N=661 | N=661 |
| Age (years) | 72±5 | 73±5 |
| Female (n,%) | 360 (55) | 360(55) |
| Duration of diabetes (years) | 40±17 | 41±17 |
| HbA1c (%) | 7.4±0.9 | 7.2±1.1 |
| CGM users n (%) | 382 (58) | 477(72) |
| Pump users n(%) | 248 (38) | 279(42) |
All 661 older adults with T1D included in the analysis had at least one HbA1c measurement in both the pre-pandemic in-person period (mean average 2.5±1.0) and the pandemic hybrid period (mean average 1.4±1.1) (Table 1). Mean HbA1c values were not statistically different between the two periods (in-person care: 7.4±0.9% vs hybrid care: 7.2±1.1%; p= 0.18). To better assess change in the distribution of HbA1c between the study periods, we compared the proportions of older adults with HbA1c values <7%, 7-8%, >8% in the pre-pandemic in-person period and the pandemic hybrid period. There was a favourable, but not significant, leftward shift in the latter period (in-person care period 34%, 40%, and 26%, respectively; and hybrid care 44%, 35%, and 21%, respectively; p<.0.058)
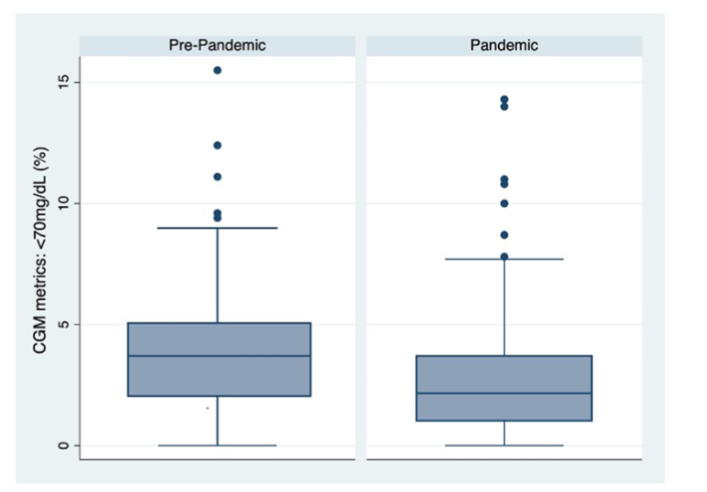
Next, we examined the sub-group of older adults with T1D using CGM. During in-person care, 382 (59%) older adults with T1D used CGM, which increased to 477 (72%) during the hybrid care. For 299 (78%) older adults with T1D using CGM during the pre-pandemic in-person care period, the electronic health records provided CGM data for both periods. Demographic characteristics of this sub-group were similar to the entire cohort with a mean age of 72±4 years and similar gender proportions with 53% female. However, in the CGM sub-group, there was a greater proportion of older adults receiving insulin pump therapy compared with the entire cohort (51% vs 37%, respectively; p<0.01). In this sub-sample, CGM metrics did not change. Mean glucose levels during the pre-pandemic in-person period versus the pandemic hybrid period were 170±31 mg/dL and 171±34 mg/dL, respectively; (p=0.77). The percent glucose time-in-range (70-180 mg/dL) was significantly different from the in-person care period versus the hybrid care period [68% (17 h/d) vs 71% (17.75 h/d)], respectively; (p=0.0001) (Table 2). Time spent in hyperglycemia (time-above-target with glucose levels >180 mg/dL) was not significantly different from the in-person care period to the hybrid care period [29 (~7.25 hr/d) to 26% (6.5 hr/d) (p=0.89)]. The mean time-below-range (time <70 mg/dL) did not differ significantly from the in-person care period to the hybrid care period [2.6 (IQ1-IQ3: 2.2 – 3) vs. 2.8 (IQ1-IQ3: 2.3 – 3.2); p= 0.42] (Figure 1). Glucose management indicator (GMI) (7.4% vs 7.4% p=0.42), and coefficient of variation (CV) (36% vs 35%; p=0.71) were not significantly different between the pre-pandemic in-person care period to the pandemic hybrid care period. Laboratory HbA1c were not significantly different between the pre-pandemic in-person care period to the pandemic hybrid care period (7.5±0.9% and 7.3±1.1%, respectively p=0.06) (Table 2).
| In-person care Pre-pandemic | Hybrid care Pandemic | p-value | |
|---|---|---|---|
| N | 299 | 299 | |
| mean glucose (mg/dL) | 170 ±31 | 171±34 | 0.77 |
| TIR (%) | 68 ±12 | 71 ± 16 | 0.0001 |
| <70mg/dL (%) | 2.6 (2.2 – 3) | 2.8 (2.3 – 3.2) | 0.43 |
| >180 mg/dL (%) | 29 ± 9 | 26 ±12 | 0.89 |
| GMI (%) | 7.4 ± 0.8 | 7.4 ± 0.8 | 0.42 |
| CV (%) | 36 ±6 | 35 ± 6 | 0.71 |
Discussion
Our data from a large cohort of over 650 older adults with T1D showed that the use of a hybrid care model was equally effective as an in-person care model in maintaining annual visit frequency and glycaemic control. In the sub-group of older adults with T1D using CGM, CGM metrics showed an improvement in time-in-range without an increase of time spent in hypoglycaemia during hybrid care compared to in-person care. This is suggestive that hybrid care can be as efficacious and safe as in-person care in older adults with T1D. To our knowledge, this is the first real-world report of clinical outcomes in association with a hybrid care model in a large cohort of older adults with T1D.
Older adults with T1D are a heterogeneous population with unique challenges related to their management of diabetes with intensive insulin therapy. The requisite needs for consistent follow-up visits with the use of intensive insulin therapy may be counter to several age-specific barriers, such as physical and cognitive decline along with frequent dependence upon family members for help with transportation to in-person visits. A hybrid care model that includes telehealth visits can help overcome many of these challenges. Our data supporting the efficacy of the hybrid care model are consistent with recent publications where hybrid care maintained patient-clinician encounters in a large group of patients with diabetes who were seen in primary care as well as in adults and older adults with type 1 diabetes seen in a tertiary diabetes-only clinic.
Older adults with T1D interviewed during the COVID-19 lockdown voiced that the use of telehealth was beneficial for maintaining continuity of care, connecting with the medical team, and reducing isolation. However, they also voiced concerns about telehealth related drawbacks such as lack of physical exams and laboratory assessments for diabetes and overall care. This suggests that hybrid care might be the preferred model of care moving forward.
Interestingly, the use of CGM during the pandemic period increased significantly from 58% to 72% in older adults with T1D. This suggests that the use of a hybrid care model did not negatively impact initiation of new diabetes technology in this sample of patients. Our findings are consistent with a recent report where initiation of CGM using a virtual endocrinology clinic was feasible and efficacious in adults with type 1 or type 2 diabetes. Moreover, the penetration of telehealth in these older adults with T1D highlights their ability to adapt to using remote communication technologies to connect by video and/or audio conferencing.
Maintaining visit frequency with CGM use may help mitigate the risk of hypoglycaemia and its adverse consequences in older adults with T1D. In the sub-group of older adults with T1D using CGM, the time spent in range improved during the pandemic period to a similar degree to what has been described in children and adolescents with T1D during the pandemic lockdown. The improvement in time spent in range could be due to changes in dietary habits and/or physical activity, as reported by older adults with T1D when interviewed during the COVID-19 lockdown period. In addition, when older adults with T1D were interviewed during the COVID-19 lockdown, they reported that use of CGM was key to their diabetes management and they feared not having CGM devices due to their reliance upon them. More importantly, the time spent in hypoglycaemia did not increase between the two time periods; this is consistent with an observation in a much smaller cohort.
These findings highlight that the use of hybrid care in older adults with T1D is not only effective in delivering care and maintaining glycaemic control as HbA1c but is also safe in people using CGM.
While to our knowledge, this is the first large, longitudinal study focused solely on older adults with T1D and the impact of hybrid care compared with in-person care on process and glycaemic outcomes, there are limitations to these analyses. First, this study involves a retrospective, electronic chart review performed at a single tertiary diabetes centre from the Northeastern United States. Second, the participants consisted of a predominantly white, English-speaking, non-Hispanic sample. Next, access to technology and the internet may be greater in this region than in other areas of the country. Moreover, the use of CGM might be higher in our cohort than in the general U.S. older adult population with T1D, given the highly specialized nature of our diabetes centre. We did not have information on episodes of severe hypoglycaemia, emergency room visits, nor hospitalizations. Therefore, our ability to assess more robust clinical outcomes with the different care models was reduced. Lastly, we did not have consistent nor complete information on race, ethnicity, nor insurance due to the recognized inaccuracies of such data in the electronic health record. Future research can help fill these gaps.
Conclusion
In summary, compared with mainly in-person diabetes visits, hybrid care, combining telemedicine and in-person visits, allowed for an increase in visit frequency with preserved glycaemic control assessed as HbA1c without worsening hypoglycaemia in a large cohort of older adults with T1D.
These data are encouraging with respect to the likely value of continuing to use a hybrid care model for older adults with T1D. In addition, these data can inform health care systems, both private and public payers, and policy makers on the impact of telemedicine on quality of care in older adults with T1D. These data findings can also help with decision making regarding the continued use of telehealth for chronic disease management in older adults moving forward.
Further studies to comprehensively understand how to best use a hybrid-care model in the management of older adults with chronic disease beyond retrospective analyses should be performed.
Conflict of Interest
Elena Toschi is a consultant for Vertex and Sequel. Lori Laffel is a consultant for Boehringer Ingelheim Pharmaceutical, Eli Lilly and Company, NovoNordisk, Janssen Pharmaceuticals, Dexcom, Medtronic, Sanofi, Provention, Mannkind, and Vertex. Medha Munshi is a consultant for Sanofi and Abbott. No other authors have duality of interest.
Acknowledgments
Part of this research was funded by NIH DP3 Grant 1DP3DK112214-01 along with from the Beatson foundation.
References
- Sinclair AJ, Dunning T, Dhatariya K, an International Group of E. Clinical guidelines for type 1 diabetes mellitus with an emphasis on older adults: an Executive Summary. Diabet Med. Jan 2020;37(1):53-70. doi:10.1111/dme.14135
- ElSayed NA, Aleppo G, Aroda VR, et al. 13. Older Adults: Standards of Care in Diabetes-2023. Diabetes Care. Jan 1 2023;46(Suppl 1):S216-S229. doi:10.2337/dc23-S013
- Schutt M, Fach EM, Seufert J, et al. Multiple complications and frequent severe hypoglycaemia in ‘elderly’ and ‘old’ patients with Type 1 diabetes. Diabet Med. Aug 2012;29(8):e176-9. doi:10.1111/j.1464-5491.2012.03681.x
- Fisher L, Hessler D, Polonsky W, Strycker L, Masharani U, Peters A. Diabetes distress in adults with type 1 diabetes: Prevalence, incidence and change over time. J Diabetes Complications. Aug 2016;30(6):1123-8. doi:10.1016/j.jdiacomp.2016.03.032
- Mehrotra A, Bhatia RS, Snoswell CL. Paying for Telemedicine After the Pandemic. JAMA. Feb 2 2021;325(5):431-432. doi:10.1001/jama.2020.25706
- Sotomayor F, Hernandez R, Malek R, Parimi N, Spanakis EK. The Effect of Telemedicine in Glycemic Control in Adult Patients with Diabetes during the COVID-19 Era-A Systematic Review. J Clin Med. Aug 31 2023;12(17) doi:10.3390/jcm12175673
- Jaana M, Pare G. Comparison of Mobile Health Technology Use for Self-Tracking Between Older Adults and the General Adult Population in Canada: Cross-Sectional Survey. JMIR Mhealth Uhealth. Nov 27 2020;8(11):e24718. doi:10.2196/24718
- Lam K, Lu AD, Shi Y, Covinsky KE. Assessing Telemedicine Unreadiness Among Older Adults in the United States During the COVID-19 Pandemic. JAMA Intern Med. Oct 1 2020;180(10):1389-1391. doi:10.1001/jamainternmed.2020.2671
- Vigersky RA, Fish L, Hogan P, et al. The clinical endocrinology workforce: current status and future projections of supply and demand. J Clin Endocrinol Metab. Sep 2014;99(9):3112-21. doi:10.1210/jc.2014-2257
- Lee JY, Lee SWH. Telemedicine Cost-Effectiveness for Diabetes Management: A Systematic Review. Diabetes Technol Ther. Jul 2018;20(7):492-500. doi:10.1089/dia.2018.0098
- Bonora BM, Morieri ML, Avogaro A, Fadini GP. The Toll of Lockdown Against COVID-19 on Diabetes Outpatient Care: Analysis From an Outbreak Area in Northeast Italy. Diabetes Care. Jan 2021;44(1):e18-e21. doi:10.2337/dc20-1872
- Bertuzzi F, Stefani I, Rivolta B, et al. Teleconsultation in type 1 diabetes mellitus (TELEDIABE). Acta Diabetol. Feb 2018;55(2):185-192. doi:10.1007/s00592-017-1084-9
- Pratley RE, Kanapka LG, Rickels MR, et al. Effect of Continuous Glucose Monitoring on Hypoglycemia in Older Adults With Type 1 Diabetes: A Randomized Clinical Trial. JAMA. Jun 16 2020;323(23):2397-2406. doi:10.1001/jama.2020.6928
- Xu T, Pujara S, Sutton S, Rhee M. Telemedicine in the Management of Type 1 Diabetes. Prev Chronic Dis. Jan 25 2018;15:E13. doi:10.5888/pcd15.170168
- Kaushal T, Ambler-Osborn L, Turcotte C, Quinn H, Laffel L. Rapid Adoption of Telemedicine Along with Emergent Use of Continuous Glucose Monitors in the Ambulatory Care of Young Persons with New-Onset Type 1 Diabetes in the Time of COVID-19: A Case Series. Telemed J E Health. Jan 2022;28(1):107-114. doi:10.1089/tmj.2020.0554
- Kaushal T, Tinsley L, Volkening LK, Ambler-Osborn L, Laffel L. Improvement in Mean CGM Glucose in Young People with Type 1 Diabetes During 1 Year of the COVID-19 Pandemic. Diabetes Technol Ther. Feb 2022;24(2):136-139. doi:10.1089/dia.2021.0258
- Kaushal T, Tinsley LJ, Volkening LK, Turcotte C, Laffel LM. Improved CGM Glucometrics and More Visits for Pediatric Type 1 Diabetes Using Telemedicine During 1 Year of COVID-19. J Clin Endocrinol Metab. Sep 28 2022;107(10):e4197-e4202. doi:10.1210/clinem/dgac476
- Toschi E, Adam A, Atakov-Castillo A, Slyne C, Laffel L, Munshi M. Use of Telemedicine in Adults with Type 1 Diabetes: Do Age and Use of Diabetes-Related Technology Matter? Telemed J E Health. Jan 24 2023; doi:10.1089/tmj.2022.0397
- Nouri S, Lyles CR, Sherwin EB, et al. Visit and Between-Visit Interaction Frequency Before and After COVID-19 Telehealth Implementation. JAMA Netw Open. Sep 5 2023;6(9):e2333944. doi:10.1001/jamanetworkopen.2023.33944
- Toschi E, Slyne C, Weinger K, et al. Use of Telecommunication and Diabetes-Related Technologies in Older Adults With Type 1 Diabetes During a Time of Sudden Isolation: Mixed Methods Study. JMIR Diabetes. Nov 18 2022;7(4):e38869. doi:10.2196/38869
- Aleppo G, Gal RL, Raghinaru D, et al. Comprehensive Telehealth Model to Support Diabetes Self-Management. JAMA Netw Open. Oct 2 2023;6(10):e2336876. doi:10.1001/jamanetworkopen.2023.36876
- Munshi M, Slyne C, Weinger K, et al. Self-care barriers and facilitators in older adults with T1D during a time of sudden isolation. Sci Rep. Apr 29 2023;13(1):7026. doi:10.1038/s41598-023-33746-3