





Impact of Rituximab on Non-Hodgkin Lymphoma Outcomes
Accessibility to Rituximab and its impact on treatment outcomes in major Non-Hodgkin Lymphoma subtypes: Insights from a resource-limited setting
Linu Abraham Jacob¹, Animesh Gupta¹, Praveen Khandare², M C Suresh Babu¹, Lokesh K. N.¹, A H Rudresha¹, Rajeev L. K.¹, Smitha C. Saldanha¹
- Department of Medical Oncology, Kidwai Memorial Institute of Oncology, Dr. M. H. Marigowde road, Bengaluru Karnataka India.
- Medical oncologist, Mumbai, Maharashtra, India
OPEN ACCESS
PUBLISHED: 30 September 2024
CITATION: Jacob, L. A., Gupta, A., et al., 2024, Accessibility to Rituximab and its impact on treatment outcomes in major Non-Hodgkin Lymphoma subtypes: Insights from a resource-limited setting, Medical Research Archives, [online] 12(9).
https://doi.org/10.18103/mra.v12i9.5791
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i9.5791
ISSN 2375-1924
ABSTRACT
Objective: Non-Hodgkin’s lymphoma is a relatively uncommon cancer and outcome data in Indian setting is scarce. This study aimed to evaluate the accessibility to rituximab and its impact on treatment outcomes in major non-Hodgkin’s lymphoma (NHL) subtypes at a tertiary care cancer hospital in South India.
Methods: This was a single-centre, hospital-based retrospective study of all newly diagnosed NHL patients between April 2015 and March 2020, at Kidwai Memorial Institute of Oncology, Bengaluru, Karnataka. Case files of the patients were retrieved, relevant data was collected and analysed.
Results: In total, 929 patients were diagnosed with NHL [diffuse large B-cell lymphoma =478(51.4%), follicular lymphoma =82(8.8%), mantle cell lymphoma=65(6.9%), peripheral T-cell lymphoma=50(5.4%), and high-grade B-cell lymphoma=49(5.2%) and rest others). Diffuse large B cell lymphoma patients mostly presented with stage IV disease (n=162(33.5%)). More than one-third (188(39.3%)) of the patients had extra-nodal disease with gastrointestinal tract involvement being the most common. The median progression free survival and overall survival of diffuse large B cell lymphoma patients were 15.2 and 23 months respectively. Only 37% of these patients had access to rituximab, and those who received rituximab-based chemotherapy demonstrated significantly better overall survival (HR=0.64, p=0.001). Follicular lymphoma patients also presented primarily with stage IV (n=40(49%)) disease, with 31(37.8%) and 58(70%) patients showing bone marrow involvement and extra-nodal involvement respectively. The median progression free survival and overall survival for these patients were not reached, however, the 2-year median progression free survival was 75%. Only 58% of the follicular lymphoma patients had access to rituximab. Response rates were higher with rituximab-based therapy, with complete response rates of 62% with rituximab vs 49% without rituximab. The progression free survival of patients who received rituximab was 61 months vs 41 months for those who did not (p=0.012).
Conclusion: There is significant gap in treatment outcomes of NHL patients between richer and poorer countries. There is an urgent need for framing of policies and public health interventions to improve access to newer therapies in resource constrained countries to further enhance cancer treatment outcomes.
Keywords: Chemotherapy, non-Hodgkin’s lymphomas, DLBCL, Follicular lymphoma, Rituximab.
Introduction
Cancer remains the second leading cause of death worldwide, affecting individuals across all age groups. Lymphomas are relatively uncommon types of cancers ranking ninth in incidence worldwide and in India according to recent GLOBOCAN 2022 data. Lymphomas are broadly classified into Hodgkin’s lymphoma (HL) and non-Hodgkin’s lymphoma (NHL), with each category encompassing various subtypes. The incidence of both HL and NHL has been steadily increasing each year, with males showing a higher susceptibility than females. In 2022, there were 553,387 new cases of NHL globally, accounting for 2.8% of all cancer diagnoses, and resulting in 250,679 deaths. In India alone, 39,736 cases were diagnosed, leading to 22,972 deaths. In India, the growing number of NHL cases presents a significant public health challenge, adding pressure to an already overburdened healthcare system. To effectively address this, it is vital to strengthen healthcare infrastructure and improve access to advanced treatments, ensuring better patient outcomes and longer survival rates.
The etiological factors contributing to NHL remain largely unexplained and vary across geographical regions. Immunodeficiency or factors influencing immunity are major risk factors for lymphomas. Other contributing factors include infections such as Helicobacter pylori, Hepatitis C virus, Epstein-Barr virus, and exposure to occupational hazards or environmental chemicals.
NHLs are a heterogeneous group of diseases characterized by distinct morphology, clinical features, natural history, prognosis, and response to treatment. The distribution of various subtypes of NHL varies with geography. In the Western world, the most common subtypes of NHL include diffuse large B-cell lymphoma and small lymphocytic lymphoma (SLL). Studies from India also report DLBCL as the most common subtype of NHL, followed by FL and T-cell NHL.
The treatment of NHL depends significantly on the specific subtype and how the disease presents in each patient. Rituximab, a type of monoclonal antibody that targets CD20 on B-cell lymphomas, was a major breakthrough in treating B-cell cancers like NHL and chronic lymphocytic leukemia. It is generally better tolerated than chemotherapy, with fewer blood-related side effects. In the Western world, rituximab greatly improved the outlook for people with B-cell NHL. Unfortunately, access to advanced therapies including rituximab remain limited in developing countries due to high costs, inadequate healthcare infrastructure, and unequal access to care. The innovator rituximab has been available in India since the early 2000s, but the higher price made it inaccessible to the majority. The Indian biosimilar rituximab became available in 2007 at a much lower price, and subsequently many other biosimilars were launched significantly reducing the cost. But did this ensure easy and universal accessibility to rituximab over a short span of time? Even though there is sufficient amount of data on the clinical spectrum and histopathological distribution of NHL subtypes from the Indian subcontinent, there is a paucity of information on the access to newer forms of treatment and its impact on clinical outcomes. We conducted this analysis to ascertain the accessibility to rituximab therapy at approximately 2 decades after the initial approval of this drug. Such information is pivotal for effective treatment planning and for framing important health policies.
Materials and Methods:
This single-centre, hospital-based retrospective analysis was conducted at Kidwai Memorial Institute of Oncology, Bengaluru, Karnataka, India from April 2015 to March 2020. The study spanned all adult patients (aged ≥18 years) newly diagnosed with NHL at the inpatient and outpatient services of the Department of Medical Oncology. Medical records of the patients were retrieved, reviewed and relevant data was captured in a case record form. The data collected encompassed demographic details like age and gender; associated comorbidities; history and physical examination.
findings; performance status and reports of relevant investigations like complete blood counts, peripheral smear, renal and liver function tests, serum lactate dehydrogenase, histopathology, immunohistochemistry, contrast-enhanced computed tomography/ fluorodeoxyglucose-positron emission tomography, bone marrow biopsy, cerebrospinal fluid analysis (when performed), two-dimensional echo and 12 lead electro-cardiogram. NHL were classified into subtypes according to the 4th edition of World Health Organization classification system¹¹. Patients were staged according to Cotswold’s modification of the Ann Arbor classification system¹². DLBCL and FL patients were risk stratified according to the International Prognostic Index (IPI) and the Follicular Lymphoma International Prognostic Index (FLIPI) prognostic scores respectively¹³˒¹⁴. The treatment administered, toxicities experienced, and responses attained were meticulously recorded and analysed. The end of treatment response was categorized as complete response, partial response, stable disease, or progressive disease per the Lugano classification for NHL¹⁵. Survival data was analysed for the major NHL subgroups. Response rates (RR), progression-free survival (PFS) and overall survival (OS) of the patients who received rituximab were compared with the non-rituximab groups.
Statistical Analysis:
Data analysis utilized the Statistical Package for Social Sciences (SPSS) software version 23. Qualitative data were reported as numbers (percentages), and quantitative data as mean (standard deviation) and median. The t-test was employed for continuous variables, and the Kaplan–Meier product-limit method was used for estimation of OS and PFS. A P value <0.05 was considered statistically significant.
Results:
A total of 929 patients were diagnosed with NHL during the study period. Major NHL categories observed were diffuse large B cell lymphoma in 478(51.4%) followed by follicular lymphoma in 82(8.8%), mantle cell lymphoma in 65(6.9%), peripheral T cell lymphoma (NOS) in 50 (5.4%), high-grade B-cell lymphoma in 49 (5.2%) of patients and rest others. (Figure 1).
Figure 1: Subtypes of NHL.
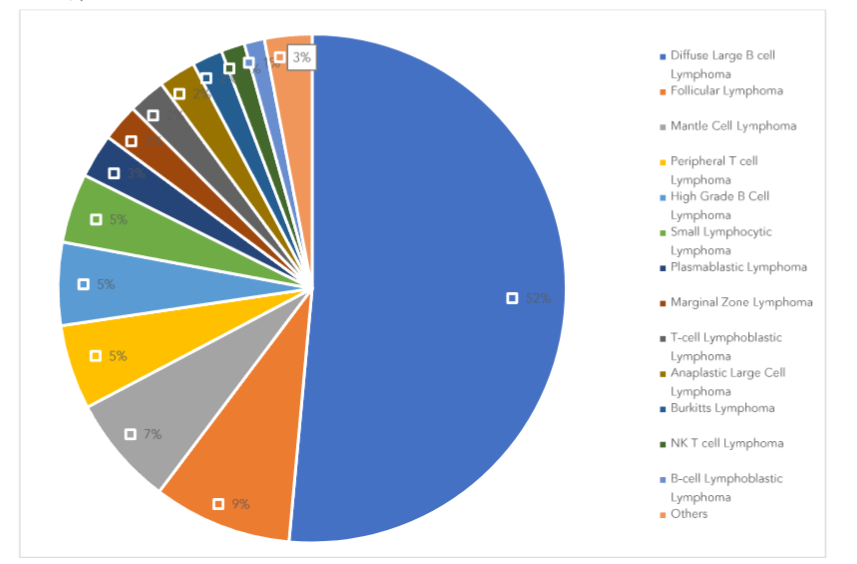
For the DLBCL cohort, the median age of presentation was 54 years with a male preponderance (1.7:1). Majority of the patients were stage IV (33.5%) and stage II (31.4%) at diagnosis. While 60.6% had primary nodal disease, 39.3% presented with extra-nodal disease, with the majority showing gastrointestinal and bone involvement, followed by liver and kidney. (Table 1) Among the 478 DLBCL patients, 429 were available for outcome analysis, and only 160 (37.2%) of them received rituximab-based treatment. The median follow-up period was 18 months. The median PFS and OS were 15.2 months and 23 months respectively. (Table 2)
Table 1. Baseline characteristics of patients with DLBCL
| Patient characteristics | N=478 |
|---|---|
| Sex (men: women) | 1.70:1 |
| Male | 301 (63.0) |
| Female | 177 (37.0) |
| Age (years), mean (range) | 54 (13-90) |
Stage at presentation
| I | 50 (10.4) |
| II | 150 (31.4) |
| III | 116 (24.3) |
| IV | 162 (33.5) |
Nodal disease
| Nodal disease | 290 (60.6) |
| Extra-nodal disease | 188 (39.3) |
Extra-nodal site
| GI Involvement (stomach, small and large intestine) | 54 (11) |
| Bone involvement | 32 (6) |
| Liver | 20 (4) |
| Kidney and suprarenal | 8 (1) |
| Bone Marrow | 7 (1) |
| Others (effusion, CNS, testis, breast, lung) | 67 (14) |
IPI score
| Risk group | |
|---|---|
| Low risk (0,1) | 172 (36.0) |
| Intermediate risk (2,3) | 234 (49.0) |
| High risk (4,5) | 72 (15.1) |
Data shown as n (%), unless otherwise specified.
KCI, Kidwai Cancer Institute; CNS, central nervous system; IPI, Integrated prognostic index.
Table 2: Outcome analysis of patients with DLBCL.
| Patient characteristics | N=429 |
|---|---|
| Patients available for analysis | 429 (89.7) |
| Not taken treatment in KCI | 21 (4.4) |
| Defaulted/ mortality prior to starting therapy | 28 (5.9) |
| Median follow up (months) | 18 |
Treatment regimens received
| Rituximab based | 160 (37.2) |
| Non-rituximab based | 269 (62.7) |
| Patient characteristics | N=429 |
|---|---|
| Not taken treatment | 49 (11.4) |
Treatment response
| Rituximab | Non-rituximab | |
|---|---|---|
| Complete response (CR) | 102 (64.2) | 127 (48.9) |
| Partial response/Stable disease (PR/SD) | 42 (26.3) | 91 (35.2) |
| Progressive disease (PD) | 16 (9.5) | 42 (15.9) |
| Deaths | 219 (51) |
| PFS, median (months) | 15.2 |
| OS, median (months) | 23 |
Data shown as n (%), unless otherwise specified.
KCI, Kidwai Cancer Institute; PFS, progression-free survival; OS, overall survival.
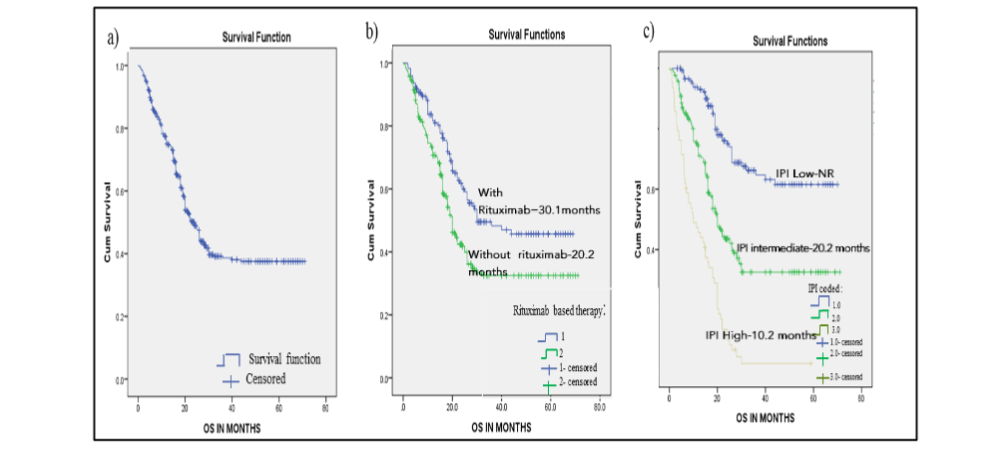
Multivariate analysis demonstrated improved OS with nodal disease vs extra-nodal disease (HR=0.38 (0.76-0.53), p=0.001), rituximab therapy vs non-rituximab therapy (HR=0.64 (95% CI: 0.47-0.87), p=0.001) and low risk IPI vs high risk IPI (HR=0.32 (95% CI:0.17-0.61), p<0.001) and CR vs non-CR (HR=0.19, p=<0.001). The median survival of DLBCL patients who received rituximab-based therapy was 30.1 months, compared to 20.2 months for those who did not receive rituximab. The median survival based on IPI score was 20.2 months and 10.2 months in intermediate and high-risk categories while in low risk IPI median OS was not reached. (Figure 2)
Figure 2:
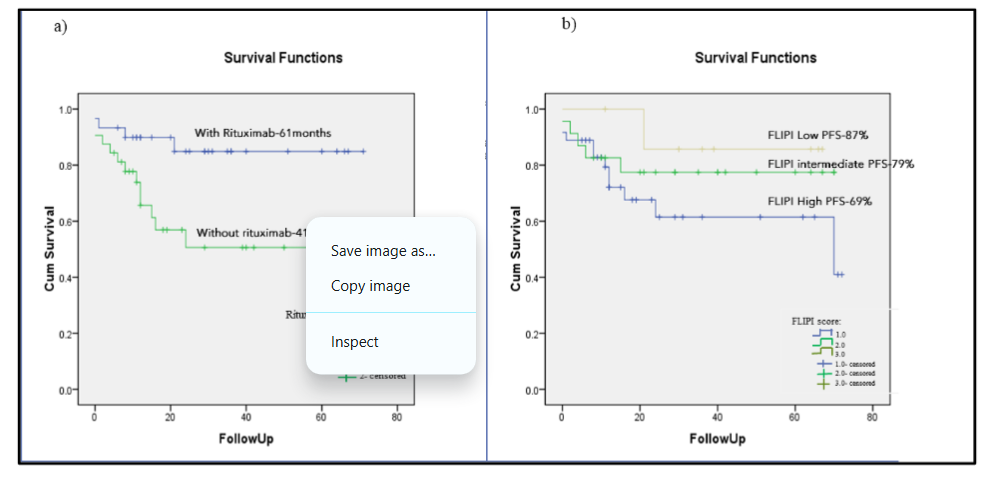
A total of 82 patients were diagnosed with FL, with a median age of 55 years. Patients primarily presented with stage III (n=37,45%) and IV (n=40,49%) disease, with 31(37.8%) showing bone marrow involvement and 58 (70%) showing extra-nodal involvement. (Table 3). Among 82 FL patients, 68 were available for outcome analysis and only 40 (58%) of them received rituximab-based treatment. The median follow-up for the entire cohort was 31 months. The median PFS and OS was not reached in both the subgroups. The 2-year PFS for all patients was found to be 75%. Patients who received rituximab had better rates of CR (62% vs 49%), and PR/SD (25% vs 24%). The PFS of patients who received rituximab was 61 months vs 41 months for those who did not (p=0.012). (Table 4, Figure 3)
Table 3. Baseline characteristics of patients with follicular lymphoma
| Patient characteristics | N=82 |
|---|---|
| Sex (men: women) | 1.27:1 |
| Male | 46 (56) |
| Female | 36 (43) |
| Age (years), mean (range) | 55 (17-81) |
FLIPI scores
| Low (0,1) | 12 (14) |
| Intermediate (2) | 29 (35) |
| High (3 or more) | 41 (51) |
| Extra-nodal involvement | 58 (70) |
| Bone marrow involvement | 31 (37) |
Stage at presentation
| I | – |
| II | 5 (6) |
| III | 37 (45) |
| IV | 40 (49) |
Grade
| I | 24 (29) |
| II | 34 (42) |
| III | 24 (29) |
Data shown as n (%), unless otherwise specified.
FLIPI, Follicular Lymphoma International Prognostic Index;
Table 4: Outcome analysis of patients with follicular lymphoma.
| Patient Outcomes | N=68 |
|---|---|
| Median follow-up | 31 months |
| Rituximab based treatment | 40 (58) |
Treatment response
| Rituximab (40) | Non-rituximab (28) | |
|---|---|---|
| Complete Response (CR) | 25 (62) | 14 (49) |
| Partial Response/Stable disease (PR/SD) | 10 (25) | 6 (24) |
| Progressive Disease (PD) | 5 (12) | 8 (27) |
| Median PFS | NR |
| Median OS | NR |
| 2 years PFS (%), median | 75 |
2 years PFS as per FLIPI score (%)
| FLIPI score | |
|---|---|
| 0-1 | 87 |
| 2 | 79 |
| 3 or more | 69 |
Data shown as n (%), unless otherwise specified.
FLIPI, Follicular Lymphoma International Prognostic Index; PFS, progression-free survival. OS, overall survival.
Figure 3:Progression-free survival in follicular lymphoma based on a) Rituximab treatment. b) Follicular lymphoma International Prognostic Index score.
Among the 929 NHL patients, 13% had T-cell NHL, with PTCL being the most common subtype, comprising 5.4% of all lymphoma cases. Among the 50 patients diagnosed with PTCL, the majority were males (78%) with a median age of 54 years. Among these, 44% were diagnosed at stage IV, and 40% at stage III, with bone marrow and extra-nodal involvement at 32% and 14%, respectively.
Discussion
The present study aimed to investigate the accessibility to rituximab and its impact on treatment outcomes of the major subtypes of NHL in a resource constrained setting. A total of 929 NHL patients diagnosed over a period of 6 years were analysed.
The most common NHL type was DLBCL (51.4%), making up more than half of all diagnosed cases, followed by FL (8.8%), MCL (6.9%), PTCL NOS (5.4%), and others. This contrasts with data from a large dataset from the USA (n=104,506), where DLBCL accounted for 23% and CLL/SLL for 16% of NHL cases. The incidence of SLL was higher in the USA compared to India (16% vs. 5%), while T-NHL was less common in the USA than in India (13% vs. 5.9%). The higher incidence of CLL in the Western world compared to India is attributed to a variety of genetic and environmental factors, but the exact cause remains unknown, warranting further research¹⁷.
Chinese data indicated a higher incidence of extranodal NK/T cell lymphoma (17% vs. 1%), making it the second most common lymphoma in their series¹⁸. Studies have shown that environmental factors such as excessive exposure to insecticides and pesticides, along with EBV exposure, are strongly associated with this disease, but further research is needed¹⁹.
Our results were comparable to most Indian studies, except for those conducted in Mumbai and Jodhpur, which showed a lower incidence of DLBCL (35.2-36.5%)²⁰˒⁸. The variation in frequencies across studies can be attributed to differences in geographic, demographic, genetic, etiologic, ethnic, socioeconomic, and environmental factors. Mondal et al. reported a higher proportion of T-NHL compared to the rest of India, likely due to the small sample size and single-centre data (Table 5)²¹. The high incidence of B-cell lymphomas in India underscores the critical role that therapies like Rituximab can play in patient treatment. Improved availability of this therapy could significantly enhance patient outcomes.
Table 5: Studies comparing distribution of common subtypes of NHL.
| Naresh et al.²⁰ | Devi et al.³² | Mondal et al²¹ | Sharma et al³³ | Arora et al.³⁴ | Gogia et al³⁵ | Patel et al⁸ | Yang et al.¹⁸ | Morton et al¹⁶ | Present study | |
|---|---|---|---|---|---|---|---|---|---|---|
| Region | Mumbai Maharashtra | Imphal, Manipur | Kolkata W. Bengal | Guwahati Assam | Vellore Tamil Nadu | New Delhi | Jodhpur Rajasthan | China | USA | Bangalore Karnataka |
| Year | 2000 | 2017 | 2014 | 2019 | 2013 | 2018 | 2022 | 2011 | 2022 | 2024 |
| Patients | 2773 | 100 | 347 | 130 | 4026 | 390 | 178 | 5549 | 104506 | 929 |
| B-NHL(%) | 79 | 66 | 74 | 74 | 78 | 89 | 75 | 62 | 83 | 87 |
Percentage of all NHL cases (%)
| Subtype | Naresh | Devi | Mondal | Sharma | Arora | Gogia | Patel | Yang | Morton | Present study |
|---|---|---|---|---|---|---|---|---|---|---|
| DLBCL | 34 | 45 | 35.2 | 60.8 | 46.9 | 68.5 | 36.5 | 41 | 23 | 52 |
| FL | 12 | 5 | 19.3 | 4.8 | 10.5 | 9 | 6.7 | 5 | 10.2 | 8.8 |
| BL | 1.8 | 6 | 5.8 | 0.8 | 3.4 | 1.3 | 3.9 | 1.9 | 1 | 1.9 |
| MCL | 3.4 | 5 | 2.6 | 3.2 | 1.6 | 5 | 8.4 | 3.1 | 9 | 7 |
| SLL | 5.7 | – | 5.5 | 3.2 | 4 | 1.3 | 2.2 | 4.6 | 16 | 5 |
| MZL | 2.1 | 1 | – | 0.8 | 0.3 | 2.3 | 1.1 | – | 3 | 2 |
| MALT | 6.1 | 1 | 2 | – | 2.17 | – | 2.2 | 6.3 | – | – |
| T-NHL | 16.2 | 23 | 25.9 | 24 | 20.2 | 11 | 24.7 | 30.2 | 5.9 | 13 |
| T-LBL | 6 | – | 8.6 | 4 | 0.4 | 1.8 | 3.9 | – | 0.8 | 2 |
| ALCL | 4.3 | 15 | 12.1 | 4 | 5 | 2.3 | 4.5 | 3.5 | 0.8 | 2 |
| PTCL | 2.9 | – | 1.7 | 15.2 | 5.9 | 3.9 | 10.7 | 4 | 0.9 | 5 |
| NK-T | – | – | – | – | – | – | – | 17.1 | – | – |
| AITL | 1 | 5 | 1.4 | – | 1.4 | 0.8 | 1.1 | 3.3 | 0.1 | – |
Diffuse large B cell lymphoma patients demonstrated PFS and OS of 15 months and 23 months, respectively, which is lower than what is reported in other Indian and Western studies (Table 6). Only 37% of DLBCL patients received rituximab-based chemotherapy, primarily due to the low socioeconomic status of the patients at our centre and lower availability of biosimilars during the study period. This probably explains the poorer responses observed in our cohort. As expected, our analysis showed that survival was better for patients who received rituximab-based treatments which was consistent with multiple Western trials²²˒²³. Patients with higher IPI scores exhibited worse survival, consistent with multiple trials conducted elsewhere²⁴.
Table 6: Comparison of treatment outcomes of DLBCL
| Prakash et al.²⁶ | Gogia et al.³⁶ | Nair S. et al.³⁷ | Pavlovsky et al.³⁸ | Present study | |
|---|---|---|---|---|---|
| Patient No. | 185 | 775 | 224 | 1457 | 478 |
| Year | 2012 | 2020 | 2022 | 2022 | 2024 |
| Percentage of patients receiving rituximab (%) | 18 | 62.8 | 73 | 97.5 | 37 |
| RR (%) | 73 | 82 | 76 | – | 79.7 |
| mPFS | 4 year EFS 54% | 3 year EFS 78% | 3 year PFS 65% | 5 year PFS 45-56% | 15.2 months |
| mOS | 4 year OS 64% | 3 year OS 88% | 2 year OS 82% | 5 year OS -69% | 23 months |
RR, Response Rate; PFS, Progression Free survival; OS, Overall Survival
In Western countries patients have near 100% accessibility to rituximab, which contributes to their better survival data for DLBCL. However, financial constraints in resource-limited countries like India limit access to newer treatments. Rituximab has been available in India since 2000 as an innovator molecule, and was initially very expensive. By 2007, biosimilars entered the Indian market, significantly reducing the cost²⁵. The use of rituximab in adult aggressive B-NHL patients as per a study reported by Prakash et al²⁶ from a centre in Delhi, India was about 18% during the period 2007-2009. The same centre reported (Gogia et al) an increase in rituximab usage in DLBCL patients to approximately 62% during the period 2014-2018³⁶, which also led to an improvement in outcomes for these patients. Similarly, Ganeshan et al reported that only 26% of DLBCL patients received rituximab during the period 2000-2013 at a study conducted in South India²⁷. A 2022 report on real world outcomes of lymphoma by the Onco-collect Lymphoma registry with data of over 9000 lymphoma patients from India pegged rituximab usage at 83.7% of DLBCL patients²⁸. All these reports clearly demonstrate that even though access to rituximab has increased over the years with availability of biosimilars and reducing costs, accessibility rates remain abysmally low even more than two decades after its approval. Although using rituximab initially increases financial strain on patients, it results in cost savings over time. A trial in the Middle East and Africa found that including rituximab in government health programs could save up to $50 million in the long run²⁹.
We found that patients with follicular lymphoma had a median age of 55 years, which is younger compared to Western data³⁰. Approximately 90% of the patients presented with advanced disease, a significantly higher percentage than reported by the SEER program in the USA³⁰. This discrepancy may be attributed to delayed hospital visits by patients and the indolent nature of the disease. The use of rituximab in our study was lower than in Western data (58% vs. 81%). Patients treated with rituximab experienced better progression-free survival (PFS) rates than those who did not receive the treatment. Western studies with higher rituximab usage, such as the one by Pavlovsky et al. in the USA, reported a 5-year PFS rate of 65% and an overall survival rate of 87%. Our analysis observed a PFS rate of 75% after 2 years (Table 7).
Table 7: Comparison of treatment outcomes of follicular lymphoma.
| Gogia et al.³⁹ | Pavlovsky et al.³⁸ | Present study | |
|---|---|---|---|
| Patients No. | 181 | 578 | 82 |
| Year | 2017 | 2022 | 2024 |
| Percentage of patients receiving rituximab (%) | 18 | 81 | 58 |
| RR (%) | 70 | – | 74 |
| mPFS | 2.5 years | 5 year PFS-65% | 2 year PFS-75% |
| mOS | 5.5 years | 5 year OS -87% | NR |
RR, Response Rate; PFS, Progression Free survival; OS, Overall Survival
Our study aimed to provide an epidemiological overview of NHL subtypes at a hospital in South India and the pattern of rituximab usage in B-NHLs. The data indicate that even 2 decades after its approval, rituximab access could not reach 100% of patients thereby compromising outcomes. It also highlights the fact that availability of biosimilars alone does not automatically guarantee 100% access. The same holds good for newer therapies like immunotherapies and CAR-T cell therapies that are approved for patients with difficult-to-treat NHL. They are likely to remain largely out of reach for most patients in India for the next decade or so.
vedotin, a novel CD79b-directed antibody-drug conjugate was incorporated into the first-line therapy of DLBCL.³¹ Similar to rituximab in its initial stages, this molecule is expensive and will likely remain inaccessible for the majority in India, until generics and biosimilars reach clinical practice a decade or so later. It is therefore imperative for the governments to take up urgent steps to address the disparities in cancer care globally and crank up regulatory and financing mechanisms to support cancer care systems. Additionally, as the majority of patients present at an advanced stage, more efforts should be directed to educate the general public so that patients present to cancer hospitals at an earlier stage, thereby improving prognosis.
Limitations of our study include its single-centre design, which may introduce selection bias, the lack of division into various DLBCL subtypes, and the absence of markers like C-MYC and BCL2/BCL6, which have prognostic implications. Additionally, PET scans were performed in only a minority of patients, despite being the investigation of choice in many high-grade lymphomas. Furthermore, bone marrow transplants, a standard treatment for relapsed lymphomas, were not performed for these patients.
Conclusion
Diffuse large B cell lymphoma and follicular lymphoma patients with access to rituximab had better outcomes than those who did not. Access to rituximab has increased over the years with availability of biosimilars and reducing costs. Public health interventions and framing of policies to improve access to monoclonal antibodies and newer therapies are the need of the hour to further improve cancer treatment outcomes in resource constrained countries like India.
Conflict of Interest:
No conflict of interests.
Funding Statement:
This study did not receive any funding.
Acknowledgements:
None.
Authors Contribution:
Dr. Linu Jacob-Conceptualization and methodology, writing-original draft, writing-review, editing and data curation; Dr. Animesh Gupta- Formal analysis, writing-original draft, writing-review, editing and data curation; Dr. Praveen Khandare- resources, methodology Dr. M C Suresh Babu, Dr. Rudresha, Dr. Lokesh, Dr Rajiv, Dr. Smitha- resources, supervision.
References
1. Dattani S. Causes of Death. Our world in data. 2023. Accessed 2024. https://ourworldindata.org/causes-of-death .
2. Bray F, Laversanne M, Sung H, et al. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. Ca (Print). 2024;74(3). doi: https://doi.org/10.3322/caac.21834
3. Morton LM, Zheng T, Holford TR, et al. Alcohol consumption and risk of non-Hodgkin lymphoma: a pooled analysis. Lancet Oncology. 2005;6(7):469-476. doi:https://doi.org/10.1016/s1470-2045(05)70214-x
4. Boffetta P. I. Epidemiology of adult non-Hodgkin lymphoma. Annals of Oncology. 2011;22: iv27-iv31. doi:https://doi.org/10.1093/annonc/mdr167
5. Chiu BCH ., Weisenburger DD. An Update of the Epidemiology of Non-Hodgkin’s Lymphoma. Clinical Lymphoma. 2003;4(3):161-168. doi: https://doi.org/10.3816/clm.2003.n.025
6. What is Non-Hodgkin lymphoma?: Types of non-hodgkin lymphoma. Types of Non-Hodgkin Lymphoma | American Cancer Society. Accessed August 11, 2024. https://www.cancer.org/cancer/types/non-hodgkin-lymphoma/about/what-is-non-hodgkin-lymphoma.html .
7. Bhutani M, Vora A, Kumar L, Kochupillai V. Lympho-hemopoietic Malignancies in India. Medical Oncology. 2002;19(3):141-152. doi: https://doi.org/10.1385/mo:19:3:141
8. Patel GR. Clinical spectrum and subtype distribution of Non Hodgkin’s Lymphoma based on the World Health Organization classification of tumors of lymphoid tissues (2017): an analysis from a tertiary care center in Western India. World cancer research journal. Published online 2023. doi:10.32113/wcrj_20235_2551
9. Sarma S, Mehta J. Spectrum of lymphomas in India. International journal of molecular and immuno oncology. 2024;9:16-24. doi: https://doi.org/10.25259/ijmio_18_2023
10. Plosker GL, Figgitt DP. Rituximab. Drugs. 2003;63(8):803-843. doi: https://doi.org/10.2165/00003495-200363080-00005
11. Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127(20):2375-2390. doi: https://doi.org/10.1182/blood-2016-01-643569
12. Olweny CL. Cotswolds modification of the Ann Arbor staging system for Hodgkin’s disease. J Clin Oncol. 1990;8(9):1598.
13. A Predictive Model for Aggressive Non-Hodgkin’s Lymphoma. New England Journal of Medicine. 1993;329(14):987-994. doi: https://doi.org/10.1056/nejm199309303291402
14. Solal-Celigny P. Follicular Lymphoma International Prognostic Index. Blood. 2004;104(5):1258-1265. doi: https://doi.org/10.1182/blood-2003-12-4434
15. Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. Journal of Clinical Oncology. 2014;32(27):3059-3067. doi: https://doi.org/10.1200/jco.2013.54.8800
16. Morton LM. Lymphoma incidence patterns by WHO subtype in the United States, 1992-2001. Blood. 2006;107(1):265-276. doi: https://doi.org/10.1182/blood-2005-06-2508
17. Ruchlemer R, Polliack A. Geography, ethnicity and “roots” in chronic lymphocytic leukemia. Leukemia & Lymphoma. 2012;54(6):1142-1150. doi: https://doi.org/10.3109/10428194.2012.740670
18. Yang QP, Zhang WY, Yu JB, et al. Subtype distribution of lymphomas in Southwest China: Analysis of 6,382 cases using WHO classification in a single institution. Diagnostic Pathology. 2011;6 (1). doi: https://doi.org/10.1186/1746-1596-6-77
19. Xu J, Yoshihiko Hoshida, Yang W, et al. Life‐style and environmental factors in the development of nasal NK/T‐cell lymphoma: A case–control study in East Asia. International journal of cancer. 2006;120(2):406-410. doi: https://doi.org/10.1002/ijc.22313
20. Naresh KN, Srinivas V, Soman CS. Distribution of various subtypes of non-Hodgkin’s lymphoma in India: A study of 2773 lymphomas using R.E.A.L. and who classifications. Annals of Oncology. 2000;11. doi:10.1093/annonc/11.suppl_1.s63
21. Mondal S, Mandal P, Roy S, Chattopadhyay S, Roy S, Biswas P. Malignant lymphoma in Eastern India: A retrospective analysis of 455 cases according to World Health Organisation classification. Journal of Cancer Research and Therapeutics. 2014;10(2):354. doi: https://doi.org/10.4103/0973-1482.136639
22. Pfreundschuh M, Kuhnt E, Trümper L, et al. CHOP-like chemotherapy with or without rituximab in young patients with good-prognosis diffuse large-B-cell lymphoma: 6-year results of an open-label randomised study of the MabThera International Trial (MInT) Group. The Lancet Oncology. 2011;12(11):1013-1022. doi: https://doi.org/10.1016/s1470-2045(11)70235-2
23. Habermann TM, Weller EA, Morrison VA, et al. Rituximab-CHOP Versus CHOP Alone or With Maintenance Rituximab in Older Patients With Diffuse Large B-Cell Lymphoma. Journal of Clinical Oncology. 2006;24(19):3121-3127. doi: https://doi.org/10.1200/jco.2005.05.1003
24. A Predictive Model for Aggressive Non-Hodgkin’s Lymphoma. New England Journal of Medicine. 1993;329(14):987-994. doi: https://doi.org/10.1056/nejm199309303291402
25. Sathyanarayanan V, Flowers CR, Iyer SP. Comparison of Access to Novel Drugs for Lymphoma and Chronic Lymphocytic Leukemia Between India and the United States. JCO Global Oncology. 2020;(6):1124-1133. doi: https://doi.org/10.1200/go.20.00012
26. Prakash G, Sharma A, Raina V, Kumar L, Mehar Chand Sharma, Bidhu Kalyan Mohanti. B cell non-Hodgkin’s lymphoma: experience from a tertiary care cancer center. Annals of Hematology. 2012;91(10):1603-1611. doi: https://doi.org/10.1007/s00277-012-1491-5
27. Ganesan P, Sagar TG, Kannan K, et al. Long-term outcome of diffuse large B-cell lymphoma: Impact of biosimilar rituximab and radiation. Indian J Cancer. 2017;54(2):430-435. doi:10.4103/ijc.IJC_241_17
28. Kumar L, Kn N, Gujral S, Kulkarni P, Stockler MR, Nair R. Editorial: Real World Outcomes of Lymphoma From India. Front Oncol. 2022;12:9223 70. Published 2022 Jul 19. doi:10.3389/fonc.2022. 922370
29. Ammar Almaaytah. Budget Impact Analysis of Switching to Rituximab’s Biosimilar in Rheumatology and Cancer in 13 Countries Within the Middle East and North Africa. ClinicoEconomics and outcomes research. 2020;Volume 12:527-534. doi: https://doi.org/10.2147/ceor.s265041
30. Seer incidence data – Seer Data & Software. SEER. Accessed August 11, 2024. https://seer.cancer.gov/data/ .
31. Tilly H, Morschhauser F, Sehn LH, et al. Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. New England Journal of Medicine. 2022;386(4):351-363. doi: https://doi.org/10.1056/nejmoa2115304
32. Adhikarimayum Ambika Devi, Takhenchangbam Dhaneshor Sharma, Yengkhom Indibor Singh, Sonia H. Clinicopathological profile of patients with non-hodgkin’s lymphoma at a regional cancer center in Northeast India. Journal of the scientific society. 2017;44(3):140-140. doi: https://doi.org/10.4103/jss.jss_42_17
33. Mahanta D, Sharma J, Sarma A, Ahmed S, Kakoti L, Kataki A. Pattern of non-hodgkin lymphoma in a tertiary care center in Northeast India using morphology and immunohistochemistry. Indian Journal of Medical and Paediatric Oncology. 2019;40(4):595. doi: https://doi.org/10.4103/ijmpo.ijmpo_129_18
34. Arora N, Manipadam MT, Nair S. Frequency and distribution of lymphoma types in a tertiary care hospital in South India: analysis of 5115 cases using the World Health Organization 2008 classification and comparison with world literature. Leukemia & Lymphoma. 2012;54(5):1004-1011. doi:https://doi.org/10.3109/10428194.2012.729056
35. Gogia A, Das CK, Kumar L, Sharma A, Sharma MC, Mallick S. Profile of non-Hodgkin lymphoma: An Indian perspective. South Asian Journal of Cancer. 2018;07(03):162-170. doi: https://doi.org/10.4103/sajc.sajc_60_18
36. Ajay Gogia, Nair S, Sharma A, et al. Non-Hodgkin lymphoma: The Indian scene. Journal of clinical oncology. 2020;38(15_suppl):e20063-e20063. doi:https://doi.org/10.1200/jco.2020.38.15_suppl.e20063 .
37. Nair S, Gogia A, Arora S, et al. Clinicopathologic features and outcomes of diffuse large B-cell lymphoma with extranodal involvement: A retrospective analysis. Cancer research, statistics, and treatment/Cancer research, statistics and treatment. 2022;5(1):67-67. doi: https://doi.org/10.4103/crst.crst_204_21
38. Pavlovsky M, Cubero D, Agreda-Vásquez GP, et al. Clinical Outcomes of Patients With B-Cell Non-Hodgkin Lymphoma in Real-World Settings: Findings From the Hemato-Oncology Latin America Observational Registry Study. JCO Global Oncology. 2022;(8). doi: https://doi.org/10.1200/go.21.00265
39. Gogia A, Raina V, Kumar L, Sharma A, Sharma MC, Mallick SR. Follicular lymphoma: an Institutional Analysis. Asian Pacific Journal of Cancer Prevention: APJCP. 2017;18(3):681-685. doi:https://doi.org/10.22034/APJCP.2017.18.3.681