





Rheumatoid Arthritis and Bronchiectasis: Unexplained Link
Rheumatoid Arthritis and HRCT proven Bronchiectasis – a strong association, still unexplained
Introduction
The strong association between rheumatoid arthritis (RA) and diffuse bronchiectasis (dBr) is well established¹. Whether this association holds true for different bronchiectasis (Br) subtypes, e.g. post-infective or mainly childhood onset bronchiectasis, pre- or post-RA onset or possibly an immune-mediated subtype is unclear. Whilst the association between RA and dBr is strong, RA associated bronchiectasis as a subtype amongst all forms of bronchiectasis is uncommon. For example, amongst all bronchiectasis subtypes, RA+dBr was found to account for just 2-4% of all bronchiectasis in a cohort of approximately 17,000 bronchiectasis patients under study in Europe, (EMBARC registry)². In contrast, idiopathic and post-infective dBr together account for about 60% of all subtypes in the EMBARC registry². In this short review, we set out the evidence for an RA and dBr association, discuss insights into this combination of morbidities and explore potential implications and pathways to further understand this association. Recommendations to address unresolved issues and guide future research are also proposed.
Methodology
PATIENTS AND METHODS
Patients who participated in the RA+dBr survival study by Makin et al were recruited sequentially from 1st Jan 2007 and followed until 31st Oct 2018. No other selection criteria were applied. Participants had no knowledge of their MBL status³. They were required to have either RA+dBr or uncomplicated RA as determined by high resolution computed tomography imaging (HRCT) and by the American Rheumatism Association 1987 classification criteria for rheumatoid arthritis respectively⁴. Diffuse bronchiectasis was determined by clinical history and at least one HRCT. All HRCTs were performed in tertiary hospital radiology departments and reported by radiologists with experience in thoracic pathology and radiology.
Patients who participated in the rheumatoid arthritis and serious infection (RA+SI) cohort study had clinically apparent RA for at least 6 months and met the American Rheumatism Association 1987 classification criteria for rheumatoid arthritis⁴˒⁵. Serious infections were those infections resulting in death or requiring either intravenous antibiotics or admission to hospital. RA+SI participants were recruited between 2007 and 2014. Participants were not required to have had antecedent SIs. All SIs were validated by systematic examination of hospital records. MBL concentrations were performed after enrolment and results were not known to participants or the investigators auditing medical records for SIs.
MBL ASSAYS
MBL assay and MBL genotyping methods are described in detail in the RA+SI cohort study⁵. The MBL Oligomer ELISA kit (Bioporto, Hellerup, Denmark) was used to determine the concentration of oligomerized MBL in human serum as per the manufacturer’s specifications⁵. Genotyping was performed by PCR restriction fragment length polymorphism based on the method described by Madsen et al⁶.
Results and Discussion
RA AND DIFFUSE BRONCHIECTASIS – EVIDENCE FOR A STRONG ASSOCIATION AND IMPLICATIONS FOR SURVIVAL
Results from previous studies have been abstracted, subjected to further examination and reviewed in the context of comorbid rheumatoid arthritis and diffuse bronchiectasis.
Bronchography proven, clinically compatible bronchiectasis has been found to be at least 10 times more frequent in RA than in degenerative joint disease¹. In earlier studies, diffuse Br (dBr) mostly preceded RA onset and was usually symptomatic. In prospective studies, HRCT proven dBr has been found to affect between 5 and 58% of RA participants⁷˒⁸, which is much higher than estimates for degenerative joint disease (0.3%) and appreciably higher than the frequency estimated in the population at large (circa 50 per 100,000 or 0.05%)¹. A meta-analysis of 10 independent studies of coexistent RA and dBr (RA+dBr) found the frequency of HRCT-proven dBr ranged from 3.6% to 62% in observational retrospective studies⁷˒⁸˒⁹. Observational prospective studies showed a range from 12 to 48%¹⁰˒¹¹˒¹². Assuming the true prevalence of coexistent dBr in RA is at the lower end of this wide range at just 3.6%, for example, this estimate equates to approximately 3600 per 100,000, which is still well above estimated prevalences in OA (300 per 100,000) and population controls (circa 50 per 100,000). Asymptomatic post-RA onset, HRCT-proven dBr has been reported in 7% of persons evaluated¹³. Thus, dBr need not be present for RA to develop. Established risk factors for RA+dBr include age, male gender, longer RA duration, genetics (CFTR or cystic fibrosis transmembrane conductance regulator, and HLA or human leukocyte antigen system) and one biomarker, notably undetectable circulating mannose-binding lectin. In addition, anti-CCP (anti-cyclic citrullinated peptide, also referred to as ACPA) antibody status, together with a propensity to increased protein citrullination, both confer increased risk¹⁴.
Higher morbidity and mortality were identified in RA+Br almost three decades ago. Swinson et al reported that RA+Br patients were 7.3 times more likely to die during a five-year follow-up period than the general population, five times more likely to die than those with RA alone and 2.4 times more likely to die than those with Br alone¹⁵. The patients reported in the Swinson et al study may not have had HRCT proven dBr (recruited in 1987, so unlikely to have had an HRCT at that time; Swinson et al report does not mention HRCT confirmation). Accordingly, it may be informative to examine mortality again in the current era of greater diagnostic accuracy for both RA (contribution of more sophisticated imaging and availability of anti-CCP antibodies) and dBr (wider usage of HRCT, better resolution and improved sensitivity and specificity of dBr diagnoses with HRCT). Furthermore, with advances in medical management, there may be improved survival. About a decade ago, Pue’chal et al showed poorer survival in RA+Br with a hazard ratio (HR) of 8.6 (Figure 1, 95% CI, 1.5 to 48.2)¹⁶. De Soyza et al showed statistically poorer survival over a four-year survival period when RA+dBr (Bronchiectasis Overlap Syndrome or BROS) patients were compared with dBr alone (participants drawn from a European cohort of 1716 adults)¹⁷.
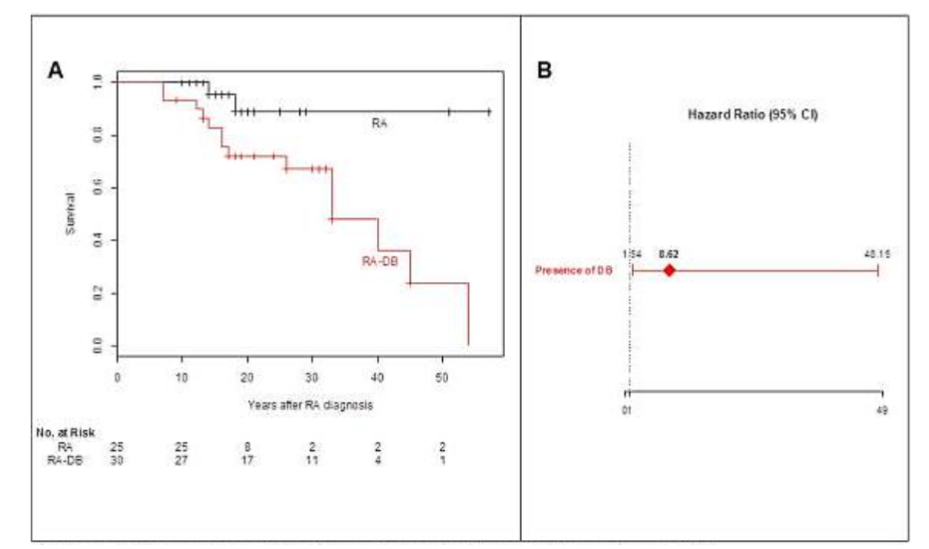
Figure 1. Survival outcomes in the study by Pue’chal et al¹⁶.
Panel A. Kaplan-Meier curves of survival after Rheumatoid arthritis (RA) diagnosis, as a function of the presence or absence of diffuse bronchiectasis (DB).
Panel B. Hazard ratios (95%CI) for death after RA diagnosis associated with the presence of DB.
A mixed effect Cox model was fitted, taking RA diagnosis as the starting point. Individual random effects were assumed to be correlated as a function of the corresponding kinship coefficients. The variance of the random effect was 4×10⁻⁴.
RA: rheumatoid arthritis; DB: diffuse bronchiectasis.
In the study by Makin et al, survival was not reduced compared with uncomplicated RA, but uMBL correlated with poorer survival in RA overall (Figure 2, P = 0.057)³.
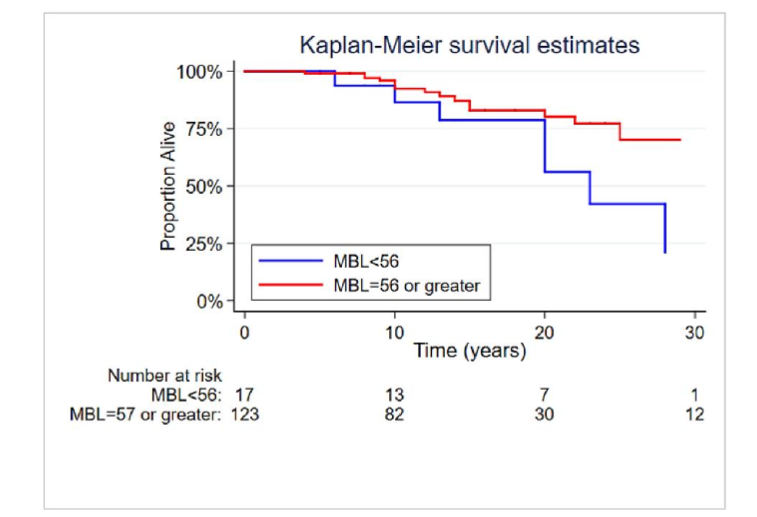
Kaplan-Meier survival according to MBL status
Figure 2. Effect of undetectable MBL on survival in Rheumatoid arthritis³.
Makin et al reported just over a third of patients with RA+dBr had undetectable mannose-binding lectin (uMBL) concentrations, which implies this common form of selective immunodeficiency may not only be a biomarker for the disease association and an indicator of poorer survival, but possibly even a contributor to the development of RA in dBr patients³. Chalmers et al did not detect a difference in MBL concentrations when all cause Br was compared with healthy controls, but did observe higher annual exacerbation frequencies, increased hospital admissions, lower quality of life scores and more severe HRCT determined structural lung damage in Br patients with MBL < 200 ng/ml¹⁹. In the RA and serious infection cohort study reported by Carroll et al, about one in eight RA patients were found to have uMBL, which is about twice the background rate in the population, however still much lower than in the RA+dBr group (37.5%, almost three-fold greater)⁵. In the RA / serious infection cohort of 228 RA patients, 16 participants had HRCT-proven dBr and amongst these 16, seven (44%) had uMBL⁵. Furthermore, in nine of the 16 in whom genotyping studies were performed, all nine (56%) were found to have one or more MBL gene mutations. Thus, the rate of undetectable MBL in RA+dBr is appreciably higher than in RA alone, all cause Br (<19%, by inference, cut-offs at 200 ng/mL, not undetectable) or in the general population³˒¹⁸. Important caveats are the relatively small number of cases and the limited number of gene studies undertaken in RA+dBr. Nevertheless, it is possible uMBL may permit the emergence or hinder the clearance of chronic infection in RA+dBr lungs, thereby allowing an altered pulmonary microbiome to drive inflammation and break tolerance, which in turn, may give rise to auto-immune disease expression, including RA¹⁹.
The mechanistic significance of the RA and dBr association calls for further consideration. Where dBr is plain at the time of diagnosis in RA, it is appropriate to consider the possibility the intrinsic lung infection and, in turn, perturbed pulmonary microbiome may function as a trigger or ongoing stimulus for auto-immune disease. It may not matter how the Br is classified; what might be important is the potential for chronic infection in perhaps a genetically susceptible host to persistently modify immune function and eventually break tolerance and contribute to the genesis of RA. Since dBr cannot be permanently cured, except by lung transplantation, such a trigger may have a sustained reinforcing effect, perpetuating the auto-immune disease thus initiated. How the number and severity of infective exacerbations in RA+dBr may contribute to the outcomes for both diseases is poorly understood. Moreover, the exact relationship between flares of dBr (infective exacerbations) and flares of RA is not well documented. It has been proposed that all cause dBr is an autoinflammatory disorder²⁰. Rapamycin derivatives can interrupt the autoinflammatory cascade via NLRP inhibition. Accordingly, azithromycin and similar agents may be useful for inflammation regulation with attenuation of the chronic infection / inflammation in dBr and in turn the autoinflammatory responses they incite²¹.
Lung transplantation for end-stage lung failure in severe bronchiectasis may inform our understanding of the RA and dBr association and help chart ways forward in disease management. Even though the need to maintain lengthy immunosuppression post-transplant confounds assessment of coexistent RA, the observation of “reduced RA disease activity” post-transplant suggests that removal of the chronic infective stimulus may promote RA remission, temporarily or perhaps even indefinitely. If indeed, long-term studies show the rate of RA remission post-transplant is high and sustained with minimal maintenance immunosuppression over time, these findings would at least partially support a perpetuating role for chronic infection in RA+dBr. Furthermore, this might focus efforts to more effectively suppress chronic dBr-related lung infection with a view to achieving improvements in bronchiectasis symptomatology as well as RA disease activity. Germane to this goal is the development of Brensocatib, a dipeptidyl proteinase -1 (DPP-1) inhibitor²² which has already shown capacity to reduce Br exacerbations in phase 2 clinical trials²³. In the RA+dBr subset, which may, in time, come to treatment with this agent, note should be taken of the secondary effects of Brensocatib on exacerbations of RA. It may also be informative to examine the effects of Brensocatib on structural progression and disease outcomes in dBr on the one hand and the RA component of RA+dBr on the other.
PULMONARY INFECTION IN RA WITH AND WITHOUT ASSOCIATED DIFFUSE BRONCHIECTASIS
Pulmonary infections, including serious infections (SIs) and non-serious infections, are common in RA, particularly in those patients who require prolonged corticosteroid therapy and aggressive anti-synovitis Disease Modifying Anti-Rheumatic Drug (DMARD) therapy, such as with biologic DMARDs (bDMARDs)⁵˒²⁴˒²⁵˒²⁶. In contrast, conventional synthetic DMARD (csDMARD) treatment alone and in the absence of corticosteroids, carries variable, but modest SI risk²⁶. Rates of SIs are higher in bDMARD recipients with an OR of up to 8.7²⁷, although long-term prospective follow-up studies are scarce. Rigorous studies in which RA patients with equivalent disease activity are randomised to csDMARD or bDMARD therapy, blinded to treatment and followed for several years or more, do not exist and are believed to be both impractical and unethical. Thus, the true extent to which bDMARDs themselves add to infection risk is uncertain and may be overestimated.
The risk factors for the development of superadded infections in dBr in general and SIs in particular are poorly defined. Conventional immunodeficiency syndromes such as diverse forms of neutropenia, lymphopenia, hypocomplementaemia and hypogammaglobulinaemia do not appear to be important contributors, except perhaps in a very small minority of Br patients. Risk factors for SIs in HRCT-proven dBr include i) pre-bDMARD treatment colonisation with any bacteria in the sputum of bDMARD recipients, and ii) bDMARD exposure²⁷. Serious respiratory infections of all kinds were the most frequent organ- or system-based infections complicating the RA and serious infection cohort study⁵. Of the 56 patient-infection events attributable to pulmonary SIs, 26 (46%) were associated with uMBL. The rate of uMBL in the entire RA cohort was 13%. The frequency of uMBL or genotypes compatible therewith in an ethnically comparable geographically similar population was estimated to be 7-8%²⁸. In a small sample of all cause “idiopathic” Br, the rate of detection of uMBL was four amongst 30 participants (unpublished data, 13%, like the frequency found in the RA cohort study)⁵. Thus, amongst the treated RA participants with pulmonary SIs, those who had uMBL were over-represented. In their assessment of 470 mixed cause dBr patients, Chalmers et al found that those with MBL concentrations < 200 ng/ml accounted for 19% of participants and was like that in healthy controls¹⁸. Survival was poorer in those with low-expressing MBL genotypes (85% at 4 years)¹⁸.
Taking these findings into account, perhaps the most likely explanation for the RA and dBr association is the high propensity for infections in RA, especially pulmonary infections, due to RA associated immunodeficiency, including uMBL on the one hand and continuous long-term therapeutic immunosuppression on the other hand.
Future studies should incorporate serum MBL determination and perhaps MBL genotyping in RA+dBr patients, RA without dBr and in Br controls, with stratification according to treatment categories and preferably incorporating at least a four-year or longer period of observation to assess longitudinal infection rates and risk factors for SIs in these cohorts. Data forthcoming may help determine whether uMBL constitutes an additional risk factor for SIs in RA+dBr. It may also be informative to compare SI rates in low and high corticosteroid users in these subgroups.
Conclusions and Recommendations
Lung infection in untreated and treated persons with autoimmune diseases should be a major concern for physicians in general and rheumatologists, pulmonologists, infectious disease physicians and immunologists, in particular. Chronic infections associated with bronchiectasis may trigger and drive auto-immune disease, contribute to RA exacerbations and complicate therapy. Even in patients with no known pulmonary pathology, lung infections are common and sometimes serious, especially in the context of corticosteroid use and probably to a moderate extent, with the use of biologic DMARD therapy. Amongst well recognised and newly emerging risk factors for lung infection in RA+dBr, undetectable MBL warrants further examination, both to confirm and more clearly define its role in the pathogenesis of infection and to explore scope for MBL repletion, with a view to preventing infection and improving survival.
With reference to the body of evidence discussed, we make the following recommendations:
- Classification criteria for Br in general should be extended to RA-associated dBr to allow differentiation of the dBr associated with RA from other forms of dBr, including potentially that which manifests after the diagnosis of RA. Importantly, dBr pre-dating the diagnosis of RA will need to be compared with post-RA onset dBr, since the former may be predominantly post-infective, and the latter may represent a potential extra-articular complication of RA or an immune-mediated disease sequel. Contributions from RA treatment to dBr development cannot be discounted but are considered improbable.
- New classification criteria could also be developed to re-evaluate the increased morbidity and mortality associated with RA+dBr with a view to figuring out which dBr subsets confer the greatest risks and in turn, which subtypes may have potentially modifiable risk factors. In addition to the potential use of Brensocatib, use of aggressive antibiotic regimens for infective exacerbations, as well as IVIG (where deficiency can be shown) or perhaps fresh frozen plasma for short term MBL supplementation, should be considered. Recombinant human MBL is not yet available.
- The association between different forms of dBr and uMBL should be investigated further. Whether pre-RA dBr or post-RA dBr are associated with MBL deficiency to the same extent requires scrutiny. Furthermore, the relative risk of SIs related to pulmonary infection should be decided afresh for recipients of i) csDMARDs in RA, ii) csDMARDs in combination with corticosteroids, and iii) bDMARDs alone or in combination with corticosteroids.
- The development of a register of RA+dBr patients who come to lung transplantation should be encouraged with a view to evaluating outcomes and especially RA remission frequency and longevity. To what extent these remissions are sustained with minimal immunosuppression over time could further inform the dBr/chronic infection/RA pathogenesis hypothesis.
- Assuming no unforeseen developments obstruct the impending usage of Brensocatib for treatment of dBr, including RA+dBr, it is reasonable to expect new opportunities to evaluate the contribution of this and potentially other DPP-1 inhibitors to pre-RA and post-RA forms of RA+dBr. The frequency with which RA develops in Brensocatib-treated dBr may also inform the debate about dBr-associated infection and inflammation acting as an RA trigger. The scope for Brensocatib to bring about fewer dBr-infective exacerbations and the possibility that this, in turn, may translate into improved survival also calls for examination. How these outcomes may vary according to MBL status might also prove to be illuminating.
Conflict of Interest Statement:
None
Acknowledgements:
None
References
1. Walker W. Pulmonary Infections and Rheumatoid arthritis. Quarterly Journal of Medicine. 1967; 142:239–51.
2. Chalmers JD, Polverino E, Crichton ML, Ringshausen FC, De Soyza A et al. Bronchiectasis in Europe: data on disease characteristics from the European Bronchiectasis registry (EMBARC). The Lancet Respiratory Medicine 2023; 11:637-649.
3. Makin K, Easter T, Kemp M, Kendall P, Bulsara M, Coleman S et al. Undetectable mannose binding lectin is associated with HRCT proven bronchiectasis in rheumatoid arthritis (RA). 2019: PLOS ONE;
https://doi.org/10.1371/journal.pone.0215051
4. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988: 315-324. doi: 10.1002/art.1780310302
5. Carroll GJ, Makin K, Garnsey M, Bulsara M, Carroll BV, Curtin SM, et al. Undetectable Mannose Binding Lectin and Corticosteroids Increase Serious Infection Risk in Rheumatoid Arthritis. The Journal of Allergy and Clinical Immunology: In Practice. 2017; 5(6):1609–1616
6. Madsen HO, Garred P, Kurtzhals JA, Lamm LU, Ryder LP, Thiel S et al. A new frequent allele is the missing link in the structural polymorphism of the human mannan-binding protein. Immunogenetics 1994; 40:37-44.
7. Hassan WU, Keaney NP, Holland CD and Kelly CA. High resolution computed tomography of the lung in lifelong non-smoking patients with rheumatoid arthritis. Ann Rheum Dis: 1995; 54:308-310.
8. Metafratzi ZM, Georgiadis AN, Ioannidou CV, Alamanos Y, Vassiliou MP, Zikou AK et al. Pulmonary involvement in patients with early rheumatoid arthritis. Scand J Rheum 2009; 36:338-344.
9. Zou YQ, Li YS, Ding XN, Ying ZH. The clinical significance of HRCT in evaluation of patients with rheumatoid arthritis-associated interstitial lung disease: a report from China. Rheumatol Int 2012; 32(3):669-673.
10. Terasaki H, Fujimoto K, Hayabuchi N, Ogoh Y, Fukuda T, Muller NL. Respiratory symptoms in rheumatoid arthritis: relation between high resolution CT findings and functional impairment. Radiat Med 2004; 22(3):179-185.
11. Wilczynska MM, Condliffe AM and McKeown DJ. Coexistence of Bronchiectasis and Rheumatoid Arthritis: Revisited. Respir Care 2013; 58:694-701.
12. Bilgici A, Ulusoy H, Kuru O, Celenk C, Unsal M, Danaci M. Pulmonary involvement in rheumatoid arthritis. Rheumatol Int 2005; 25(6):429-435.
13. Attar SM, Alamoudi OS, Aldabbag AA. Prevalence and risk factors of asymptomatic bronchiectasis in patients with rheumatoid arthritis at a tertiary care centre in Saudi Arabia. Ann Thor Med 2015; 10:176-180.
14. Martin LW, Prisco LC, Huang W, McDermott G, Shadick NA, Doyle TJ et al. Prevalence and risk factors of bronchiectasis in rheumatoid arthritis: a systematic review and meta-analysis. Seminars in arthritis and rheumatism. 2021; 1067-1080.
15. Swinson DR, Symmons D, Suresh U, Jones M, Booth J. Decreased survival in patients with co-existent rheumatoid arthritis and bronchiectasis. Br J Rheumatol 1997; 36(6):689-691.
16. Pue´chal X, Ge´nin E, Bienvenu T, Le Jeunne C, Dusser DJ. Poor Survival in Rheumatoid Arthritis Associated with Bronchiectasis: A Family-Based Cohort Study. PLOS ONE. 2014; 9(10): e110066.
17. De Soyza A, McDonnell MJ, Goeminne PC, Aliberti S, Lonni S, Davison J, et al. Bronchiectasis Rheumatoid Overlap Syndrome is an Independent Risk Factor for Mortality in Patients with Bronchiectasis: A Multicenter Cohort Study. Chest 2017;1247- 1254.
18. Chalmers JD, McHugh BJ, Doherty C et al., “Mannose-binding lectin deficiency and disease severity in non-cystic fibrosis bronchiectasis: a prospective study,” The Lancet Respiratory Medicine 2013; 1: 224–232.
19. Quirke A-M, Perry E, Cartwright A, Kelly C, De Soyza A, Eggleton P et al. Bronchiectasis is a model of chronic bacterial infection inducing autoimmunity in rheumatoid arthritis. Arthritis Rheum 2015; 67:2335-2342.
20. Scambler T, Holbrook J, Savic S, McDermott M and Peckham D. Autoinflammatory disease in the lung. Immunology 2018; 154: 563–573.
21. Lendermon EA, Coon TA, Bednash JS, Weathington NM, McDyer JF, Mallampalli RK. Azithromycin decreases NALP3 mRNA stability in monocytes to limit inflammasome-dependent inflammation. Respir Res 2017; 18:131
22. Cipolla D, Zhang J, Korkmaz B, Chalmers JD, Basso J, Fernandes C et al. Dipeptidyl peptidase-1 inhibition with Brensocatib reduces the activity of all major neutrophil serine proteases in patients with bronchiectasis: results from the WILLOW trial. Resp Res 2023;24: https://doi.org/10.1186/s12931-023-02444-z.
23. Chalmers JD, Haworth CS, Metersky ML et al. Phase 2 trial of the DPP-1 inhibitor brensocatib in bronchiectasis. N Engl J Med 2020; 383:2127–2137. doi:10.1056/NEJMoa2021713
24. Listing J, Strangfeld A, Kary S, Rau R, von Hinueber U, Stoyanover–Scholz M et al. Infections in patients with rheumatoid arthritis treated with biologic agents. Arthritis Rheum 2005: 52;3403-3412.
25. Bechman K, Halai K, Yates M, Norton S, Cope AP, Hyrich KL and Galloway JB. Non-serious infections in patients with rheumatoid arthritis: results from the British Society for Rheumatology biologics register for rheumatoid arthritis. Arthritis Rheumatol 2021; 73;1800-1809.
26. Doran MF, Crowson CS, Pond GR, O’Fallon WM and Gabriel SE. Predictors of infection in rheumatoid arthritis. Arthritis Rheum 2002; 46:2294 -2300.
27. Guillame G, Dadoun S, Bui T, Del Castillo P, Patternotte S and Dougados M. Risk of infections in bronchiectasis during disease-modifying treatment and biologics for rheumatic diseases. BMC Infectious Diseases. 2011: 304; https://doi.org/10.1186/1471-2334-11-304.
28. Minchinton RM, Dean MM, Clark TR, Heatley S, Mullighan CG. Analysis of the relationship between mannose-binding lectin (MBL) genotype, MBL levels and function in an Australian blood donor population. Scand J Immunol 2002: 56; 630-641.