

Balancing Patient Rights and Medical Training Ethics
How to Balance Patient Rights, Safety and Choice of Provider with the Need to Train Future Doctors
Ben Gray 1
- Associate Professor Dr Ben Gray MBChB MBHL FRNZCGP(Dist) Primary Health Care and General Practice University of Otago Ōtākou Whakaihu Waka Wellington
OPEN ACCESS
PUBLISHED: 30 June 2025
CITATION: Gray, B., 2025. How to Balance Patient Rights, Safety and Choice of Provider with the Need to Train Future Doctors. Medical Research Archives, [online] 13(6). https://doi.org/10.18103/mra.v13i6.6620
COPYRIGHT:© 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i6.6620
ISSN 2375-1924
ABSTRACT
There is significant variation internationally in ethical guidance on teaching and involvement of students in patient care. New Zealand is an outlier in requiring consent for teaching which “includes training” for all medical students and post graduate trainees. There is an ethical tension between the patient’s best interests to receive the best available care and the societal need to train new doctors. This tension is hard to resolve if the patient lacks capacity, and the decision is required to be made solely on the best interest of the patient. If this New Zealand standard is applied rigorously no-one would be able to learn a procedure that is only performed on a person lacking capacity. Requiring consent is not usual in the apprenticeship model which is central to the training of doctors. Any standards relating to managing the risks of teaching, and agreement for involvement in care must apply to all students and qualified doctors. Whilst patients retain the right to refuse treatment the value of having students as part of the team should be emphasised and the social norm should be that patients are involved in teaching. Teaching should be an ethical responsibility of all doctors. Particular guidance is needed for teaching/learning with patients who have limited or impaired capacity. This can be modelled on guidance developed for research on vulnerable patients.
Keywords
- Patient Rights
- Medical Education
- Informed Consent
- Apprenticeship Model
- Vulnerable Patients
Introduction
The concept of Informed consent for clinical practice and research is well developed with consistency across ethical codes from different jurisdictions. The application of Informed Consent to teaching is less developed and ethical codes have significant variation. In New Zealand (NZ), teaching is broadly defined and Informed Consent for teaching is approached in the same way as for clinical care. If the patient is unable to consent, then the patient’s best interest is the guiding principle. This approach fails to address the balance between the patient’s best interest and the societal goal of training doctors. The variation between different codes of practice will be described, followed by a broad description of the structure of medical education. There will be a particular focus on the nature of the apprenticeship model, where consent for involvement of the apprentice is not the norm and there is little scope for choice of doctor. Patient safety is the responsibility of the supervising doctor who gains consent for the whole team. Central to this discussion is whether the learning that occurs during the provision of care by either a student, graduate or fully qualified specialist, should be considered teaching. A narrow definition of teaching will be presented with a discussion as to why inclusion of learning during the provision of care in a definition of teaching is unworkable. The proposed approach will focus on strengthening the role of supervision under the apprenticeship model, emphasising the self-awareness of all practitioners to only provide care within their ability and to seek supervision if they are in doubt and introduce guidance for learning whilst providing care to vulnerable patients (those with limited or no capacity) modelled on the provisions used in conducting research on vulnerable patients.
Methodology
This is an opinion piece based on the training and experience of the author. I have had a career as a specialist general practitioner in a high needs clinic. In that role I taught 4th year students and GP registrars. For the last seventeen years I have convened the course on Professional Practice for undergraduate medical students at Otago University Wellington. I have a detailed knowledge of the regulatory requirements for practice in NZ and have investigated standards from other countries. An important element of my teaching is that for around 150 students a year, I read, and discuss one-on-one, student reflective essays titled “Thought Provoking Episode Report”. Over the years there have been many addressing the question of consent for teaching. Whilst this paper is written from a NZ perspective the issues raised will affect all jurisdictions. When I refer to Students this includes 4-6th yr medical students and graduate doctors in training: Post Graduate Year (PGY) 1,2 and registrars doing their specialty training. Fully qualified doctors I refer to as Senior Medical Officers (SMO’s).
Discussion
GUIDANCE ON CONSENT FOR TEACHING AND CHOICE OF DOCTOR
If every person wanting a cataract removed were able to choose the best doctor available and decline a trainee, we would end up with no surgeons. Surgeons can only gain experience by doing something for the first time. Atul Gawande addressed this conundrum in “Educating the knife”: this is an uncomfortable truth about teaching. By traditional ethics and public insistence (not to mention court rulings), a patient’s right to best possible care must trump the objective of training novices. We want perfection without practice. Yet everyone is harmed if no one is trained for the future. So learning is hidden behind drapes and anaesthesia and the elisions of language. 1(p24).
In the USA in 2002 he avoided this issue by not talking with patients about his level of expertise, getting surgical experience with poor people who had no other choice and ignoring the issues of training in fully qualified doctors. This opaque approach is not congruent with valuing transparency and patient rights. Since then, regulations have been developed in many jurisdictions covering teaching during the provision of care. There is broad agreement on ethical guidance in relation to informed consent for research and clinical care 2-7. By comparison there is significant variation in recommendations on consent for teaching. Table 1 summarises guidance from a range of countries with different approaches.
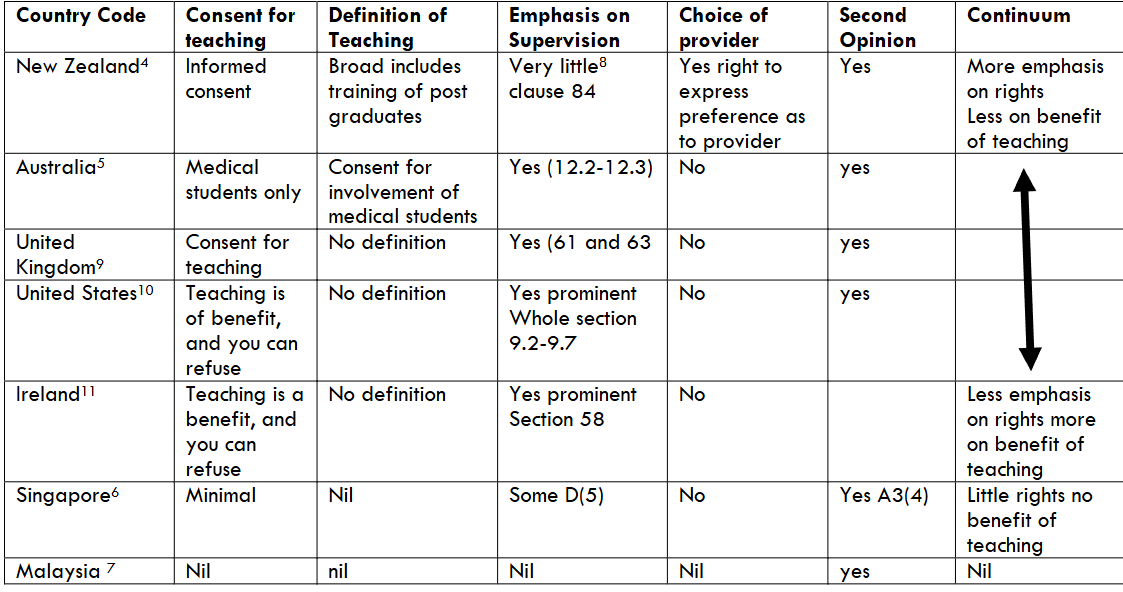
There is a continuum of guidance. At one end in NZ there is more focus on patient rights and little or no focus on the benefits of teaching and the apprenticeship model. In the middle is Australia where the rights focus is limited to medical students and there is moderate reference to supervision, and the UK that merely requires consent for teaching without any elaboration and has some guidance on supervision. Further along is the USA and Ireland with less focus on rights and more focus on the value of teaching and the apprenticeship model. The USA and Ireland both emphasise the value that involvement with teaching has for patients, whilst emphasising the importance of good supervision, and acknowledging a right to decline involvement. Ireland even includes a clause regarding school students observing practice 11 (section 59) At the far end Singapore does not provide any ethical guidance on teaching as it affects patients and implies that none is required. When talking of third parties in attendance they say, “Unless the third parties are an obvious part of the healthcare team, you must explain to patients who the third parties are…”. Only in relation to patient information does it mention the right for patients to decline participation in teaching 6.
Malaysia 7 makes no mention of either teaching the value of education or supervision. New Zealand is the only jurisdiction that provides for expressing preference of provider, but all include a right to a second opinion.
Medical Education
At Otago University there are three years of pre-clinical education covering the theoretical grounding for the practice of medicine, followed by three years of advanced learning where theoretical learning is combined with clinical exposure. There are three main modalities of clinical teaching: simulation-based training, teaching on patients and apprenticeship learning.
SIMULATION BASED TRAINING
Simulation Based Training (SBT) has had a significant impact on medical training 12. We routinely utilise actors as simulated patients for teaching and assessing consultation skills. We employ volunteer teaching associates who are willing to have students learn to perform a genital examination on them. We have mannequins for teaching cardiopulmonary resuscitation and genital examination. SBT has been promoted as an important way to avoid the conundrum of risk to patient safety when training doctors. However, it has major limitations of cost and failing to fully capture the complexity and unpredictability of clinical practice. Work is required to develop the simulation scenarios and time is needed to train staff in using simulation. It is most used in some wealthy American medical schools 12. In the current constrained health funding environment, it is only a small adjunct to the training of doctors in NZ. To learn the skills of a doctor Students must be involved with real patients.
TEACHING ON PATIENTS
Teaching on patients occurs where the patient, a doctor teacher and a Student or Students are present, the interaction is for the purpose of teaching, and there is no clinical benefit for the patient. This particularly applies to medical students performing their first vaginal examination on anaesthetised women 13, which in NZ was the index case that led to the requirement for consent for teaching 14. Rowland et al did a literature review of what they described as the disparate body of literature on patient involvement in teaching, and came up with three interpretations of patient involvement in health professional education; patients as teachers, real patients as standardized patients, and bedside learning 15.
Gaining consent for student involvement in this teaching is essential and it would be unacceptable to involve a patient who lacked capacity (who had not consented whilst able as in the example in theatre) as the subject of such teaching. As care is not provided these episodes would not be covered by the ethical guidance on providing care.
APPRENTICESHIP LEARNING
Doctors learn in the apprenticeship model 16,17. Apprenticeship learning is common in many settings. Lave and Wegner analysed apprenticeships of midwives, tailors, quartermasters and butchers to develop their theoretical model 18.
Healthcare is a team activity. Interprofessional practice has become the norm 19(Chapter 2). Doctors do their job by having a web of colleagues, medically trained and from other professions, to consult when they feel a patient needs more than the skills they have to offer. There is significant overlap in skill between professions, Obstetricians and midwives, General Practitioners and Nurse Practitioners being good examples. The Student is learning within this wider community. This aligns well with Lave and Wenger’s ‘Community of Practice’, their apprenticeship model fits medicine well 20.
Novices or apprentices are given small tasks with limited responsibility, then tasks of increasing complexity and responsibility until they become full members of the ‘community of practice’. They are developing into a master in the context of the community.
The medical care provided in a teaching hospital is not provided by individual doctors but by the medical team 21. The SMO decides in discussion with their Student whether the Student is capable of elements of the task and provide supervision varying according to the Student’s level of accomplishment. For each task, the SMO is best suited to judge the Student’s capability, based on understanding the task’s requirements and the Student’s abilities. For example the task of inserting a central line 1. The risk of this procedure is hard to quantify. It may be the first time the Student has inserted a central line, but what other similar procedures have they done? How good is their knowledge of anatomy? Are they particularly dextrous or are they ham fisted? A knowledge of the status of the learner is a poor guide to their ability to perform a particular task, which is more related to what specific experience they have had. The SMO in discussion with the Student decides whether the task should be done under close supervision, crucial for the first insertion of a central line, or under no direct supervision after having inserted lines successfully. For more routine tasks within their ability Students will practice independently. Patient accountability is held by the SMO, based on developing the trust of the patient, or if the patient lacks capacity with their surrogate decision makers. The SMO may ask Students not to be present for the care of particularly anxious patients, or patients who have limited trust in doctors 22. Our public hospitals depend on this model to function 23.
The model is dependent on two important features. Firstly, there must be supervision available when needed. Secondly every doctor, not just Students, need an awareness of their own abilities, not attempt tasks that they are not sure they can safely complete and have a good relationship with their supervisor and other colleagues to seek help when needed.
Gaining consent for the involvement of apprentices is not a usual part of the model. The builder, lawyer or architect has the relationship with the client and the client has no say as to exactly who does the work. Medicine is different because the care is provided in person. Patients have a right to refuse treatment. For patients with capacity, every Student and SMO must introduce themselves with their role, who they work with and their level of training to establish that the patient agrees to that person’s involvement in their care.
In theory a patient could refuse care from a junior and insist on seeing the SMO. In practice this rarely happens due to the practical barriers. Choice of carer within a community of practice is limited.
DEFINITION OF TEACHING, IS LEARNING TEACHING?
Defining clinical care is straight forward. It is the service that a health provider [doctor] provides 4. The definition of teaching involving patients is more complex. As discussed above teaching on patients can be clearly defined. More difficult is defining whether learning that occurs during the provision of care should be considered teaching that requires consent.
Many clinical interactions result in learning, whether involving a Student or SMO. The distinction between when a learner is gaining experience and when they are competent in a task is variable and complex. Being able to insert an intravenous line in an adult with slim arms does not mean an ability to insert a line in a distressed child. It might also be a skill that wanes if not regularly practiced. Implicit in trying to define teaching/learning is the idea that there are doctors who are now competent (and no longer learning). This is only true in a narrow sense. It is true for a proceduralist. It is true for hospital specialists within their area of specialty, but patients never present as just an eye. There is usually a need for knowledge and skills outside of the specialty and the PGY may well be better reading an ECG than the Eye Surgeon. It is not true of a General Practitioner (GP) who cannot possibly be competent in all of medicine.
A recent decision of The NZ Health and Disability Commission (HDC) discussed consent for teaching in relation to Gynaecology procedures in theatre 23. The HDC argued that it was the presence of a supervisor that defined teaching for graduate doctors. Where doctors who are not certified in the procedure are performing that procedure under the direction and supervision of the doctors who are certified in the procedure, and who are available as a safety net and to impart their knowledge, experience, and instruction along the way, this represents teaching, and consequently Rights 6(1)(d) and Right 9 apply 23.
In this example if the same registrar with the same level of experience performed the procedure without the SMO in the room, it would not be teaching. However, they are still under supervision and if they ran into difficulties would call the SMO in.
The premise for requiring consent for teaching is that there is patient risk in receiving care from a doctor not competent in providing that form of care. This could apply to the narrow range of care (procedures and narrow specialist knowledge) for which competence could be defined and measured. For real complex patient problems, it is unworkable. Competence in managing a wound for a distressed child in a rural clinic, depends on interpersonal skills with parents and children, skill with the use of local anaesthetic and skill with suturing. Importantly the nature of the wound can vary from minor (needing a dressing only) through to something requiring complex plastic surgical procedure. It could be that a “good enough” job by the rural GP would be better than travelling 6 hours to the nearest tertiary centre to see a plastic surgeon. The GP needs to judge if the care is within their competence in this particular instance. A generic description of competence in suturing could not cover all the variables.
If you cannot define competence, you cannot define when, during the provision of care, teaching/learning is occurring, and when there is no teaching/learning.
The risks and benefits of teaching
It seems intuitively true that receiving care from a fully trained person is better than having the same care from a lesser trained person. There are clear risks for procedures performed by Students that require the skill of an individual practitioner. Many people would prefer to have only one provider for sensitive consultations or procedures, out of concern for privacy and dignity. Care may take longer if provided by a supervised novice. This could result in a greater degree of pain or discomfort.
The benefits of teaching are not always apparent to patients. In its statement on medical student involvement in patient care the American Medical Association (AMA) says: Much to the benefit of patients and medical education, medical students are participating in patient care from the start of their medical education. Initially, students may be mere observers, but soon they assume more responsibilities, such as monitoring the condition of patients and even becoming involved directly in treatment. Patients and the public benefit from the integrated care that is provided by health care teams that include medical students and other trainees. Students’ limited experience is counter-balanced by the supervisory structure of medical teams and patient care generally is enhanced by the involvement of medical students 10.
Historically, teaching hospitals were seen as more prestigious, and it was expected that trainees would be involved in care. Outcomes have been shown to be better in teaching hospitals compared to non-teaching hospitals 24. Teachers also learn from the process of teaching 25,26. An essential role of the Student is to ask why. As a clinician I have benefited from the extra rigour required when consulting with a Student present, of needing to justify my decisions. Overall, Student involvement in care is a benefit to patients. In limited settings there are more significant risks that can be mitigated but not removed by good supervision.
Objections to requiring consent for apprenticeship learning
The apprenticeship model is central to medical education. It has been modified particularly for patients with capacity, by requiring doctors to introduce themselves with their role, who they work with and their level of training to establish that the patient agrees to that person’s involvement in their care. There remain several important objections to requiring consent for teaching in all settings.
- THERE IS A SOCIAL OBLIGATION TO PARTICIPATE IN DOCTOR TRAINING
It has been argued that there is a social obligation to participate in research 27,28. If individuals want to benefit from the findings of research, then there is some obligation to be available to participate. It is argued that those who decline to participate in research are “freeloading” on those prepared to accept the risk and inconvenience of participating. Like research, but to a much greater extent, there is a social obligation for patients to participate in training doctors. This is part of the social contract 29. If individuals want to benefit from trained doctors, then there is some obligation to participate in their training. Giving patients the right to decline involvement in training undermines this obligation. - If informed consent is required for medical students, then it is necessary for all other health students. It also applies to all the other nonprofessional staff involved in patient care, including those in training. In 2022 in NZ (population 5 million), over 290,000 weeks of placements were needed to train pre-registration health students 30. International medical graduates (IMGs) who come to the country have received their training by clinicians and on patients in their home countries. Last year 70% of new medical registrations in New Zealand were IMG’s 31. Overall in NZ 43% of registered doctors are IMGs, the highest proportion in the developed world 31. The comparable figures are; for the United Kingdom (30%) 32, Australia (10%) 33, USA (23%) 34. In effect, to the extent to which countries rely on IMGs, they are free loading on the patients and clinician teachers of the home countries. Just 28.7% of overseas-trained doctors remain in NZ after five years, compared to 84.9% of locally trained doctors 31. We need to train more doctors so we will need more places in medical schools, PGY1 and training registrars and will need more people willing to be involved in training them.
- There is no post graduate training in the NZ private specialist sector 35. The bulk of care in this sector is elective surgery. Private health insurance is held by 35% of New Zealand adults 36. These people are therefore able to “choose” not to be involved in training.
- New Zealand needs more training positions. If being involved with teaching is a burden for patients, then it is fairest for that burden to be shared by all rather than just those who cannot afford to avoid it.
2. IT PREVENTS LEARNING TO CARE FOR PATIENTS WITH LIMITED OR NO CAPACITY
A significant amount of clinical work involves patients with either no capacity; babies, unconscious people, people with severe dementia, or people with impaired capacity; those in pain or distress, intellectual handicap and children. These people cannot consent for teaching. In NZ if the involvement in provision of care is by a qualified doctor, then this can proceed either with consent of an available surrogate decision maker or based on the best interests of the patient. Care can only involve teaching of Students if it is in the best interests of the patient. Walker et al 37 have provided a detailed interpretation of the requirement for informed consent included in the NZ Code for undergraduate medical student involvement in patient care. This paper was a consensus statement from both the Auckland and Otago Medical Schools after consultation with key stake holders including the HDC. They advised that:
- In almost all circumstances, students should only undertake an examination, provide treatment or perform a procedure when the patient consented to this.
- The exceptions to this are very limited, e.g., time-critical situations where a patient is unconscious, and the student’s involvement is urgently needed to provide or contribute to life saving treatment.
- The role of medical students in ICU should usually be restricted to observation.
- The medical student role in caring for babies should be limited to observation.
- When there is no practical opportunity to obtain consent from a legal representative, the treating doctor should determine what, if any, student involvement is in the patient’s best interests.
If we limit undergraduate students in this way, it delays the acquisition of skills and presents a serious risk that as a new graduate, they are called on to do a task that they may not have attempted or observed before.
Walker et al argued there was a distinction in the consent requirement for undergraduate medical students compared to post graduate trainees because they are not registered health professionals. This distinction is not present in the NZ Code and the Commissioner has explicitly affirmed that the requirement for consent for teaching applies to PGY1-2 and Registrars 23.
The point has been made in relation to research, that if research is not allowed on people who lack capacity to consent, then there is an absence of good evidence to guide the care of these people. The same argument applies to teaching for example in the care of people with intellectual impairments. If they lack decision making capacity then no doctor will learn how to care for this group of patients.
3. THERE IS INCREASED PATIENT RISK FROM EXCLUDING STUDENTS FROM PROVISION OF CARE.
In many settings teaching/learning/training is interwoven with service. Health New Zealand estimated in relation to postgraduate trainees that “70% of the ‘training’ is actually experiential learning gained while undertaking the specific clinical work for which they are employed 23”. There is a continuum. At one end (for example a medical student observing a procedure) it is almost all learning and no provision of care. At the other end (for example a senior registrar performing a routine operation) it may be almost all provision of care and little learning. It is difficult in advance of the procedure to predict exactly where on the continuum it may lie. The routine procedure being observed and performed may turn into a resuscitation beyond the skill of the registrar, requiring the summoning of the SMO and active assistance from the student. In the HDC case discussed above Health NZ said, “It is impossible to define a boundary at which point experiential ‘learning through service’ ends and formal ‘teaching’ starts when an RMO is a member of the team undertaking a procedure” 23.
A rigid rule requiring consent for all student interactions has the potential to cause harm; see Box 1.

In this setting, it was impractical to gain consent for teaching. There was urgency, the woman was in the middle of labour and arguably had limited capacity for this decision based on pain and distress. Had the student not participated due to a lack of consent the risk to the baby was higher. This case was of a 5th year student but if it had been the PGY1 who had had no experience of this procedure the need for consent would have been the same. An important problem with this requirement for consent is the uncertainty of when it applies. If the PGY1 had attended alone, despite their lack of experience, they were not being supervised and therefore this would not be considered “teaching”. Alternately if the baby was born severely distressed the neonatal SMO would have been called. Walker et al allowed for student involvement in “time-critical situations where a patient is unconscious, and the student’s involvement is urgently needed to provide or contribute to life saving treatment” but this is not simple to decide. As in this case it could be that the student involvement prevented a need for life saving treatment by assisting earlier on.
Because of the complex nature of medical practice we often cannot know in advance what role a Student may play, and what mixture of service provision and teaching will occur.
4. INFORMED CONSENT IS CULTURALLY UNSAFE
Informed consent is a culture bound concept from the dominant “Western” culture based on placing a high value on individual autonomy and rational decision making 38. In NZ it is not a good fit with the collective cultures of Māori and Pacific peoples, who operate more on relationship and trust 39(Chapter 5). The cultural norm in Malaysia is that there is no requirement for consent for teaching 7. Informed Consent as a concept has received significant critique when applied to research 40 and described as incoherent as applied to clinical care 41. There has been little work done on how to address informed consent in relation to teaching other than adopting the same mechanisms as for clinical care. A rigid enforcement of informed consent for teaching of all people denies cultural variability.
Mrs Jones had a spontaneous rupture of membranes and was delivering a preterm baby of 33+6 weeks at 10.00 pm. The PGY1 was busy with another patient, so the Neonatal registrar asked the 5th year student to attend the birth and help with any required resuscitation. The registrar quickly explained the help that they would need. When they arrived, Mrs Jones was in the final stages of labour. The registrar did not explain to Mrs Jones that they were a trainee or that their assistant was a student and did not ask the woman to consent to the student assisting in the care of her baby. The baby was delivered and successfully resuscitated by the registrar and medical student. On reflection the student was distressed at not having gained consent from Mrs Jones.
Is there an ethical responsibility for doctors to teach?
Whilst there is variation in current ethical codes, historically teaching has been viewed as an ethical responsibility. The whole of the second paragraph of the Hippocratic Oath is concerned with passing on the knowledge of the profession 42. The now obsolete New Zealand Medical Association Code of Ethics 43 retained this emphasis: Clinical teaching is the basis on which sound clinical practice is based. It is the duty of doctors to share information and promote education within the profession and the wider healthcare team. Education of colleagues and medical students should be regarded as an ethical responsibility for all doctors. Current guidance in NZ much weaker. The Medical Council of New Zealand describes teaching as a “professional responsibility” 8. The Oath taken by Otago medical students on graduation makes no mention of teaching.
Teaching is less valued partly because of requiring patient consent, but also because of the separation of teaching budgets from budgets for providing care, and the pressure on the health budget. Teaching is seen in several settings as being discretionary. During the Covid pandemic, clinical teaching of medical students all but stopped 44,45. The private specialist sector rarely has Students to the detriment of the training of surgical registrars 35. It is seen as an optional choice in General Practice, such that academic general practice departments have trouble recruiting sufficient placements 46. This year 24 of the graduating doctors were not offered jobs during the matching process 47. There were insufficient training posts for PGY1’s to accommodate all the graduating students.
As noted above we need to train more doctors, so will need more doctors to do the training. We need to change expectations such that the norm is that all doctors participate in teaching.
How to balance patient rights safety and choice of provider with the need to train future doctors.
The exact balance will depend on the culture of the country. As noted, Malaysia has not included patient rights at all. New Zealand currently puts little emphasis on the need to train future doctors and I have argued that the current situation is not tenable. Any policy should include some emphasis on the following.
- STANDARDS RELATING TO MANAGING THE RISKS OF TEACHING SHOULD APPLY TO ALL STUDENTS AND SMO’S
There is no logic to limiting standards on teaching to undergraduates. If there are risks for a patient being involved in teaching those risks are present whenever a Student or SMO is learning something. Arguably the risks of an SMO learning a new procedure (perhaps robotic surgery) are the same as if that procedure were being learned by a registrar. The risk of performing the first lumbar puncture is the same if performed by a 6th year medical student as by a PGY1. - AGREEMENT FOR INVOLVEMENT IN CARE SHOULD BE SOUGHT FOR EVERY INTERACTION WHERE POSSIBLE.
Every interaction whether Student or SMO, with patients who have capacity, should start with an introduction of their name, their role, who they work with and their level of training, to establish that the patient agrees to that person’s involvement in their care. - PATIENTS HAVE A RIGHT TO REFUSE CARE FROM ANY STUDENT OR SMO.
There is a fundamental right to be able to refuse treatment. If a patient refuses care, then the doctor responsible must continue to negotiate to find an agreed management plan. There will be settings where this will be straightforward; for example, in most settings a woman who requires a vaginal examination will be able to insist on a female doctor. In many public hospital settings, a patient choice as to who provides care is not feasible. - THE SOCIAL NORM SHOULD BE THAT PATIENTS ARE INVOLVED IN TEACHING.
The clause from the AMA 10 is a good expression of this norm. It highlights the value of teaching. There is no justification for the norm to be that the risks of teaching are only borne by those who cannot afford private care. - TEACHING SHOULD BE AN ETHICAL OBLIGATION OF ALL DOCTORS.
All specialist colleges set standards and requirements for continuing registration and could require all doctors to demonstrate involvement in teaching to maintain registration. There is a large overlap between teaching of doctors and teaching of patients. An ability to teach is an essential professional skill. In NZ currently, surgical trainees have little exposure to procedures that are only performed in the private sector. Arguably being involved in teaching is an important part of professional development and therefore should be required of all doctors. If teaching is a burden, then it should be shared across the profession. - PRINCIPLES FOR LEARNING WHILST PROVIDING CARE TO PATIENTS WITH IMPAIRED CAPACITY.
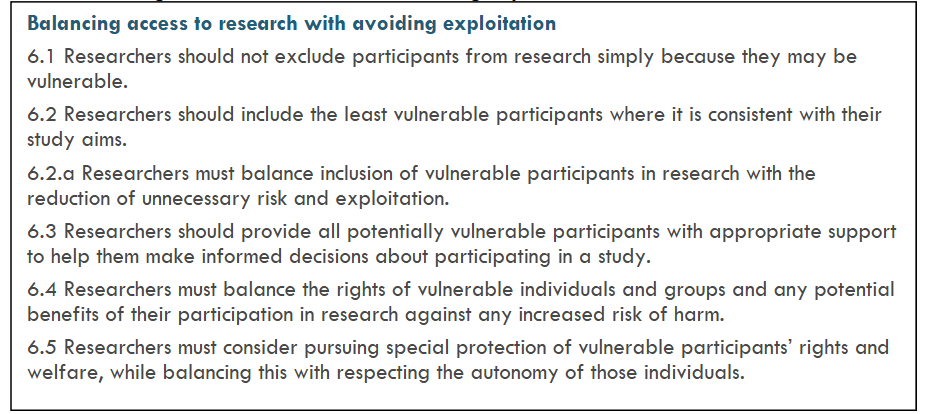
Patients with impaired or absent capacity are by definition vulnerable patients. The principles developed for research on vulnerable people provide some useful guidance 48. (see box 2)
Conclusion
Consent for teaching is required where the sole purpose of the interaction is teaching. When clinical teaching is interwoven with provision of care, it is not possible to clearly delineate a boundary between the two. A balance needs to be found between the best interests of the patients and the benefits to society of training clinicians. Informed consent as a process has limitations applied to research and clinical care, that are even more problematic when applied to teaching. Overall, care provided by a team that includes trainees is superior, but there are inevitably circumstances of risk to the patient. For patients who have capacity every doctor whether Student or SMO. needs to introduce themselves describing their role, who they work with, and their expertise and gain patient agreement to be involved in their care. If consent is given for provision of care, then additional consent for teaching is not required. For patients with limited or no capacity using the standard of the patient’s best interests to permit teaching severely constrains learning on procedures only carried out on patients who lack capacity. In this setting the apprenticeship model is the best option available to balance the risk to the patient against the benefits of training. This requires good supervision, good awareness in the doctor of the limits of their ability, and clear guidance on avoiding exploitation of vulnerability. If the society wishes to train doctors, there is a social obligation for patients to be available to assist in training, and an ethical responsibility on doctors to provide training.
Acknowledgements
Dr Janine Winters provided significant input into the development of this paper.
Conflict of Interest
I have no conflicts of interest
References
- Gawande A. Complications: a surgeon’s notes on an imperfect science. 1st ed. ed. Metropolitan Books; 2002:x, 269.
- United Nations Educational Scientific and Cultural Organization. Universal Declaration on Bioethics and Human Rights. UNESCO. 2021. https://en.unesco.org/themes/ethics-science-and-technology/bioethics-and-human-rights
- Parsa-Parsi RW. The International Code of Medical Ethics of the World Medical Association. JAMA. 2022;doi:10.1001/jama.2022.19697
- The Code of Health and Disability Services Consumers’ Rights, (1996). http://www.hdc.org.nz/theact/theact-thecode
- Medical Board AHPRA. Good medical practice: a code of conduct for doctors in Australia. https://www.medicalboard.gov.au/Codes-Guidelines-Policies/Code-of-conduct.aspx
- Singapore Medical Council. Ethical Code and Ethical Guidelines. 2025. https://isomer-user-content.by.gov.sg/77/775548fb-11df-4393-89c5-33717769ccf6/2016-smc-ethical-code-and-ethical-guidelines—(13sep16).pdf
- Malaysian Medical Association. Code of Medical Ethics. 2025. https://www.mma.org.my/images/pdfs/Link-CodeOfEthics/MMA_ethicscode.pdf
- Medical Council of New Zealand. Good Medical Practice. 2022. https://www.mcnz.org.nz/our-standards/current-standards/good-medical-practice-2/
- General Medical Council. Good Medical Practice. General Medical Council. 2024. https://www.gmc-uk.org/-/media/documents/good-medical-practice-2024—english-102607294.pdf
- American Medical Association Code of Medical Ethics Medical Student Involvement in Patient Care. 2024. https://code-medical-ethics.ama-assn.org/ethics-opinions/medical-student-involvement-patient-care-0
- Council CnnLM. Guide to Professional Conduct & Ethics for Registered Medical Practitioners. 2024. https://www.medicalcouncil.ie/news-and-publications/publications/guide-to-professional-conduct-and-ethics-for-registered-medical-practitioners-2024.pdf
- Elendu C, Amaechi DC, Okatta AU, et al. The impact of simulation-based training in medical education: A review. Medicine. 2024;103(27):e38813.
- Broadmore J, Hutton J, Langdana F. Medical students’ experience of vaginal examinations of anaesthetised women. BJOG: An International Journal of Obstetrics & Gynaecology. 2009;116(5):731-733.
- Cartwright Sylvia. Report of the committee of inquiry into allegations concerning the treatment of cervical cancer at National Women’s Hospital and into other related matters. Accessed 12/3/13, https://www.womenshealthcouncil.org.nz/the-cartwright-inquiry
- Rowland P, Anderson M, Kumagai AK, McMillan S, Sandhu VK, Langlois S. Patient involvement in health professionals’ education: a meta-narrative review. Advances in Health Sciences Education. 2019/08/01 2019;24(3):595-617. doi:10.1007/s10459-018-9857-7
- Rassie K. The apprenticeship model of clinical medical education: time for structural change. The New Zealand Medical Journal (Online). 2017;130(1461):66.
- Bagg W, Adams J, Anderson L, et al. Medical Students and informed consent: A consensus statement prepared by the Faculties of Medical and Health Science of the Universities of Auckland and Otago, Chief Medical Officers of District Health Boards, New Zealand Medical Students’ Association and the Medical Council of New Zealand. The New Zealand Medical Journal. 2015;128(1414):27.
- Lave J, Wenger E. Situated learning: Legitimate peripheral participation. Cambridge university press; 1991.
- New Zealand Medical Council. Kevin Morris, ed. Cole’s Medical Practice in New Zealand. 14th ed. 2021. Accessed 10/9/22. https://www.mcnz.org.nz/assets/standards/08588745c0/Coles-Medical-Practice-in-New-Zealand.pdf
- Bunniss S, Kelly DR. ‘The unknown becomes the known’: collective learning and change in primary care teams. Medical education. 2008;42(12):1185-1194.
- Caldwell G. Whatever happened to apprenticeship learning? The Clinical Teacher. 2011;8(4):272-275.
- Moffitt TE, Caspi A, Ambler A, et al. Deep-seated psychological histories of COVID-19 vaccine hesitance and resistance. PNAS nexus. 2022;1(2):pgac034.
- Health and Disability Commissioner. Case 19HDC01260. 2024. Accessed 16/10/24, https://www.hdc.org.nz/decisions/search-decisions/2024/19hdc01260/
- Silber JH, Rosenbaum PR, Niknam BA, et al. Comparing outcomes and costs of medical patients treated at major teaching and non-teaching hospitals: a national matched analysis. Journal of general internal medicine. 2020;35:743-752.
- Nestel D, Kidd J. Peer assisted learning in patient-centred interviewing: the impact on student tutors. Medical teacher. 2005;27(5):439-444.
- Stone S, Ellers B, Holmes D, Orgren R, Qualters D, Thompson J. Identifying oneself as a teacher: the perceptions of preceptors. Medical education. 2002;36(2):180-185.
- Schaefer GO, Emanuel EJ, Wertheimer A. The Obligation to Participate in Biomedical Research. JAMA. 2009;302(1):67-72. doi:10.1001/jama.2009.931
- Ballantyne A, Schaefer GO. Consent and the ethical duty to participate in health data research. Journal of medical ethics. 2018;44(6):392-396.
- Bagshaw P, Potter JD, Hornblow A, et al. The common good: reviving our social contract to improve healthcare. 2025. p. 9-13.
- Te Whatu Ora Health New Zealand, Te Aka Whai Ora Māori Health Authority. Finding a place to learn in health. https://www.tewhatuora.govt.nz/whats-happening/consultations/a-new-system-for-student-placements/
- Medical Council of New Zealand. Fact Sheet Strengthening our Workforce. 2025. https://www.mcnz.org.nz/assets/Uploads/Fact-sheet-PR.pdf?vid=9
- General Medical Council UK. The State of Medical Education and practice in the UK Workforce Report. 2023. https://www.gmc-uk.org/-/media/documents/workforce-report-2023-fullreport_pdf-103569478.pdf
- Yeomans ND. Demographics and distribution of australia’s medical immigrant workforce. J Migr Health. 2022;5:100109. doi:10.1016/j.jmh.2022.100109
- Nagarajan KK, Atul B, Varun MS, and Adhikari R. Prevalence of US-trained International Medical Graduates (IMG) physicians awaiting permanent residency: a quantitative analysis. Journal of Community Hospital Internal Medicine Perspectives. 2020/11/01 2020;10(6):537-541. doi:10.1080/20009666.2020.1816274
- Briana Northey. Outsourcing health care risks the next generation of specialists. Accessed April 11 2025, https://www.thepost.co.nz/nz-news/360631419/outsourcing-health-care-risks-next-generation-specialists
- Ministry of Health. New Zealand Health Survey 2022/23. 2024. https://www.health.govt.nz/publication/annual-update-key-results-2022-23-new-zealand-health-survey
- Walker S, Reid P, Anderson L, et al. Informed consent for medical student involvement in patient care: an updated consensus statement. The New Zealand Medical Journal (Online). 2023;136(1579):86-95.
- Gray B. (Bio)Ethics in a Pluralistic Society. Challenges. 2019;10(1):12.
- New Zealand Law Commission. Review of Adult Decision-Making Capacity Law. https://www.lawcom.govt.nz/assets/Publications/IssuesPapers/NZLC-IP49.pdf
- Te Ara Tika: Guidelines for Māori Research Ethics: a Framework for Researchers and Ethics Committee Members (Health Research Council of New Zealand) (2010).
- Manson NC, O’Neill Onora. Rethinking informed consent in bioethics. Cambridge University Press; 2007.
- Davey LMMD. The Oath of Hippocrates: An Historical Review. Neurosurgery. 2001;49(3):554-566.
- New Zealand Medical Association. Code of Ethics for the New Zealand Medical Profession. New Zealand Medical Association. 2021. https://assets-global.website-files.com/5e332a62c703f6340a2faf44/5fbd645fe15640fa981fa469_Code%20of%20Ethics%20Redesign%202020%20version%204.pdf
- Brown A, Kassam A, Paget M, Blades K, Mercia M, Kachra R. Exploring the global impact of the COVID-19 pandemic on medical education: an international cross-sectional study of medical learners. Can Med Educ J. 06/30 2021;12(3):28-43. doi:10.36834/cmej.71149
- Tolsgaard MG, Cleland J, Wilkinson T, Ellaway RH. How we make choices and sacrifices in medical education during the COVID-19 pandemic. Medical teacher. 2020;42(7):741-743.
- Murton SA, Pullon SRH. Assessment of training capacity in New Zealand general practices: a stocktake in the lower North Island and South Island. The New Zealand Medical Journal (Online). 2017 Sep 22-2022-11-08 2017;130(1462):11-26.
- New Zealand Medical Students Association. NZMSA Statement on Graduating Doctors Without Jobs. 2025. https://www.nzmsa.org.nz/_files/ugd/137253_9ae9b1640239468b9fd05c11861324b1.pdf
- National Ethics Advisory Committee. National Ethical Standards for Health and Disability Research and Quality Improvement. https://neac.health.govt.nz