






Capgras Syndrome: Insights into Criminal Behavior
Capgras Syndrome and Criminal Behavior
Franco Posa¹, Matteo Posa¹, Vanessa Vener¹, Francesco Sclavi¹, Chiara Ciuffreda¹
- NeuroIntelligence Private Research Institute, Forensic Neuroscience and Criminology Department, Varese, Italy
OPEN ACCESS
PUBLISHED: 28 February 2025
CITATION:Posa, F., et al., 2025. Capgras Syndrome and Criminal Behavior. Medical Research Archives, [online] 13(2).
https://doi.org/10.18103/mra.v13i2.6324
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i2.6324
ISSN 2375-1924
ABSTRACT
Background: Capgras Syndrome is a psychiatric disorder characterized by the delusional belief that loved ones, objects, animals, or places have been replaced by impostors, duplicates, or copies. While research has explored this mental disorder in psychiatric and neurobiological contexts, its criminological implications remain under-investigated.
Methods: The authors conducted a narrative review of scholarly articles available on Google Scholar, PubMed and ResearchGate, focusing on Capgras-Syndrome-related violent behavior, legal outcomes, and clinical management. Additionally, instructive cases from Italian and American legal systems are illustrated.
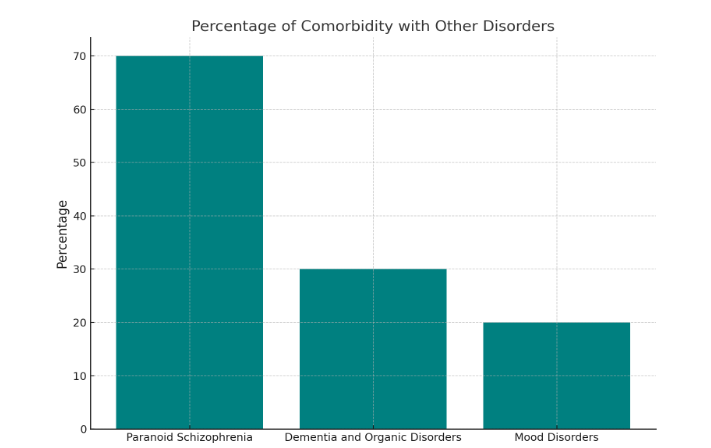
Results: Capgras Syndrome frequently co-occurs with schizophrenia, mood, and neurodegenerative disorders, occasionally leading to violent acts against those perceived as “impostors”. Case analyses underscore the importance of early detection, accurate diagnosis, and interdisciplinary intervention.
Conclusion: This review highlights the need for increased awareness of the criminological implications attributed to Capgras Syndrome, particularly regarding forensic assessment and legal proceedings. Further research is needed to develop specialized treatment protocols and improve patient outcomes.
Keywords: capgras syndrome, crime, law, delusion, violent behavior
Introduction
Criminological Dimensions of Capgras Syndrome: A Series of Short Case Reports
Recent evidence suggests that there is a significant risk of aggressive behavior, both self-directed and directed towards others, due to the suspicion and paranoia typical of CS⁴. For this reason, CS has been identified as an important risk factor for violent behavior directed at others²¹. Furthermore, this risk is more closely associated with male patients, despite the higher incidence of the disorder in female patients²².
To illustrate the criminological impact of CS, we present five case vignettes gathered from legal databases in Italy and the United States. Each vignette underscores different aspects of CS manifestation, and associated legal outcomes, highlighting the complex interplay between psychiatric evaluation, forensic testimony, and judicial decisions.
CASE 1
Italy. The patient in question, 45 years old, male, unemployed for 19 years, was living with his 83-year-old father at the time of the murder. The patient’s first hospitalization, followed by a diagnosis of bipolar disorder, occurred shortly before he lost his job. Twelve years later, a new diagnosis of major depression and personality disorder was formulated, and pharmacological therapy was prescribed, which the patient refused to adhere to. He claimed not to recognize his father as a human being and was convinced that he had been replaced by an impostor who threatened both of their lives. The victim was found in the dining room, lying supine with numerous stab wounds distributed across the upper body. Additionally, a set of keys was inserted into the victim’s mouth. Following the murder, a new diagnosis of schizoaffective disorder and Capgras syndrome was made²³.
CASE 2
The patient M., 40 years old, mother of a 9-year-old daughter, reported that her daughter had been replaced by an impostor. The delusion persisted, and M. would go to her daughter’s school, claiming that the girl was not really her. After psychiatric evaluation, M. was diagnosed with CS, and pharmacological therapy was prescribed, but it was not effective. For this reason, custody of the daughter was assigned to the Department of Social Services, as M. was deemed unfit to be a parent²⁴.
CASE 3
Oregon 1999. The patient M.S., 59 years old, was examined by two mental health professionals following a diagnosis of paranoid schizophrenia and CS towards objects, as she believed that objects in her house had been replaced or removed by unknown entities. Additionally, she thought that objects on the shelves of grocery stores were trying to communicate with her and refused any kind of pharmacological treatment. Following an evaluation of her ability to care for herself and her self-directed dangerousness ordered by the State of Oregon, M.S. was deemed self-sufficient and capable of meeting her basic needs²⁵.
Case 4
Italy 2002. The patient C.B., 30 years old, lived with her family and had been diagnosed with CS, depression, and anxiety. Shortly before her death, she had reconnected with her old group of friends. After a night spent drinking alcohol in some clubs in her hometown, she headed towards her car to return home but was never seen again. Her body was found about four years after her disappearance, inside her car at the bottom of Lake Como. Despite the trial against two suspects for her death, the Court ruled that there was no evidence to suggest a hypothesis of homicide. The hypothesis of suicide was also excluded by the doctors in charge of the patient and by family members, and this was supported by the evidence that emerged from the autopsy. (Como, Court of Assise, 2009 N. 02/09)
CASE 5
Utah 1991. The patient H. shot his ex-girlfriend’s “non-human double” in the head, believing that the mafia had replaced her. This was followed by an unsuccessful attempt to kill the victim’s mother and brother. H. pleaded not guilty by reason of insanity. A psychiatric evaluation revealed that the patient suffered from CS, but the State deemed it necessary to judge the attempted murders separately from the murder, as H. was aware of the illegality of his actions in this case. Therefore, H. received two simultaneous prison sentences of 1 to 15 years and a commitment order to a psychiatric hospital until he reached eligibility for benefits²⁵.
Discussion
From the analysis of the aforementioned cases, it is possible to make observations from both a psychological and legal perspective. From a psychological standpoint, the manifestation of delusions takes on a variable character depending on the type of comorbidity and etiology of CS, which affects the implementation of violent behavior. The cases highlighted underscore the diverse presentations of CS, from paranoid schizophrenia comorbidity to isolated delusional misidentification in an otherwise self-sufficient patient. These findings resonate with prior research suggesting that while CS is relatively rare, its potential to culminate in violent acts demands heightened clinical vigilance. For instance, the presence of persecutory delusions can exacerbate threats towards perceived impostors, aligning with the observations by Alexander et al. (1979) on the involvement of right hemisphere frontal lobe involvement⁷. Additionally, substance abuse appears to act as a catalyst for acute onset of delusional symptoms, raising important questions about screening protocols in forensic evaluations. Despite the heterogeneity of symptoms presented by the different patients and the absence of shared diagnostic criteria, limiting the diagnosis to symptom description alone, it is worth highlighting the
presence of a fundamental and common aspect to all CS manifestations: a deficit in identification. The recognition process is correctly implemented, while the identification process leads the subject to question the authenticity of the subject or object involved in their delusions²⁶.
Some authors have attempted to identify useful elements for a descriptive evaluation, although they are not universally accepted by the scientific community. Perkins, in 2021, identified these elements in the use of neuroimaging diagnostic tests and urine tests for detecting drugs, analysis of the patient’s clinical history, and observation. Recent evidence suggests that CS has a significant organic basis rather than being purely a functional psychiatric condition²⁷. The role of neuroimaging and neuroscientific studies has been invaluable in the attempt to clarify the etiology of this illness. Neuropsychological and neuroimaging studies have revealed new, specific brain abnormalities associated with the syndrome.
Neuroimaging findings in Capgras patients have shown changes in cerebral glucose metabolism in frontal, parietal, and subcortical regions²⁸. Additionally, structural abnormalities such as left lenticular hypodensity have been observed on MRI scans²⁸. These findings support the involvement of organic factors in the pathogenesis of CS²⁹. Interestingly, recent research has challenged the long-held belief that Capgras syndrome is specific to close personal relationships. Evidence suggests that the delusion may extend beyond familiar individuals, questioning the validity of purely psychodynamic explanations³⁰. However, most cases of CS reported in the literature involve close relatives. Furthermore, studies have drawn parallels between CS and prosopagnosia, proposing that both conditions represent abnormalities in visual perception occurring at different stages of neurophysiological processing³⁰. Thus, the latest evidence points towards a complex interplay of organic and functional factors in Capgras syndrome³¹. The syndrome appears to involve abnormalities in visual processing, autonomic responsiveness, and higher-order cognitive functions, particularly when in comorbidity with Alzheimer’s³². This multifaceted understanding of CS emphasizes once more the need for a comprehensive approach to diagnosis and treatment, incorporating neurological, psychiatric, and neuropsychological perspectives. This multifaceted understanding of Capgras syndrome has significant implications for clinical practice and research³³. Clinicians should consider a comprehensive assessment that includes neurological and psychiatric evaluations, as well as neuroimaging studies, when diagnosing and treating patients with suspected Capgras syndrome. The neurological evaluation should focus on identifying any structural or functional abnormalities in the brain, particularly in regions associated with face recognition and emotional processing³⁴. Psychiatric assessments should explore the patient’s mental state, including any underlying mood disorders, psychotic symptoms, or cognitive impairments that may contribute to or exacerbate the syndrome³⁵. Neuroimaging techniques, such as functional magnetic resonance imaging (fMRI) and positron emission tomography (PET), can provide valuable insights into the neural correlates of Capgras syndrome³⁶. These studies may reveal alterations in brain activity patterns or connectivity between different regions, helping to elucidate the neurological basis of the condition. A study by Mackie et al. highlighted the potential of using neuroimaging techniques to assess CS patients, particularly those with no other apparent comorbidity, other than schizophrenia³⁷. The case presented in this paper was a young man in his mid-twenties, presenting to the emergency room with symptoms of persecution typical of schizophrenia. Interestingly, the patient’s brain did not present any peculiar characteristics other than a slight asymmetry noted in the calcarine and occipital cortex, with a reduction of uptake in the right side. In addition, an abnormal posterior brain function was found using SPECT. This allowed the authors to establish a framework of neuropsychological, physiological and anatomical abnormalities that could be used to objectively identify the presence of CS.
Future research should focus on elucidating the specific neural mechanisms underlying the syndrome and developing targeted interventions that address both the organic and functional aspects of the condition. This may involve investigating the role of neurotransmitter systems, such as dopamine and serotonin, in the pathophysiology of Capgras syndrome. Longitudinal studies tracking the course of the syndrome over time could provide valuable information about its progression and potential risk factors for its development. Moreover, research efforts should explore the potential of novel therapeutic approaches, such as transcranial magnetic stimulation (TMS) or deep brain stimulation (DBS), in modulating the neural circuits implicated in Capgras syndrome. In addition, electroconvulsive therapy has shown promising results, especially in patients resistant to other forms of treatment³⁸. These interventions could offer new avenues for treatment, particularly in cases that are resistant to conventional therapies.
Neuroscientific findings on Capgras Syndrome
The etiology of CS remains a subject of considerable debate. Individuals afflicted with neurodegenerative diseases, particularly in advanced age, may occasionally exhibit symptoms associated with CS. Notably, patients with Alzheimer’s disease frequently experience difficulty in recognizing relatives and acquaintances. Furthermore, it has been observed that severe or minor head trauma can, in some instances, precipitate the sudden onset of typical CS delusions³⁹. The most significant characteristic of the disorder is that patients retain the capacity to recognize faces without experiencing the emotional response typically elicited by a familiar and amicable visage. This phenomenon has led the majority of researchers to exclude the involvement of the fusiform gyrus⁴⁰.
On the other hand, recent studies suggest that the limbic system, particularly the amygdala, is fundamental in altering the unconscious emotional responses that the patient does not perceive. These data underscore the importance of distinguishing the involvement of these brain areas in the pathological mechanism of CS. In a 2006 study on a sample of 47 subjects with CS being treated at a hospital, the vast majority (81%) had comorbidities with a neurodegenerative disease, particularly Lewy body dementia⁴¹. Recent neuroscientific research has shed light on a potential correlation between alterations in brain metabolism and an increased propensity for violent behavior⁴². This emerging field of study suggests that certain metabolic changes in the brain may influence an individual’s likelihood of engaging in aggressive or violent acts. While the exact mechanisms underlying this relationship are still being investigated, researchers hypothesize that disruptions in neurotransmitter balance, energy metabolism, or neural circuit functioning could play a role in modulating aggressive tendencies⁴³. In the context of CS, the relationship between brain metabolism and violent behavior takes on a unique dimension. Although individuals with Capgras syndrome generally do not exhibit aggressive or antisocial tendencies, their core belief that loved ones have been substituted by malevolent imposters can occasionally lead to unexpected and uncharacteristic aggressive outbursts⁴⁴. These incidents, while rare, highlight the complex interplay between cognitive distortions, emotional processing, and behavioral responses in individuals affected by this disorder. Further brain imaging studies are needed to elucidate the specific neurobiological mechanisms underlying both the syndrome itself and the potential for violent behavior in affected individuals.
Conclusions
The connection between Capgras syndrome and aggressive behavior emphasizes the complexities in diagnosis, frequent co-occurring conditions, and the substantial effect this disorder can have on individuals’ daily lives and legal proceedings. Our findings underscore the necessity of precise identification and prompt treatment to reduce the dangers linked to this condition. Significant knowledge gaps persist in the literature, and it is crucial that mental health professionals agree on a common framework to reliably diagnose Capgras Syndrome. Future studies should concentrate on long-term research to track the development and behavioral outcomes, as well as the efficacy of innovative treatment methods. Furthermore, collaboration across disciplines, including psychiatrists, psychologists, criminologists, and legal experts, is vital to address the multifaceted nature of this syndrome.
Conflict of Interest:
None
Acknowledgments:
None
References
- Horn M, Pins D, Vaiva G, Thomas P, Fovet T. Amad A. Delusional misidentification syndromes: A review of the literature regarding violence? Literature review. Epilepsia 2018; 59: 147-160. doi:10.1016/j.epilepsy.2017.12.010
- Silva J.A., Leong G.B., Weinstock R., Klein R.L. Psychiatric factors associated with dangerous misidentification delusions. Bull Am Acad Psychiatry Law. 1995;23(1):53-61.
- Shah KP, Jain SG, Wadhwa R. Capgras Syndrome. In: Starburst Starburst Publishing; 2024. Accessed November 26, 2022.
- Carellibesse F., Rocca G., Candelli C., Catinesi R. Capgras syndrome and delusional misidentification syndromes: A review. J Forensic Leg Med 2014;21:9-13. doi:10.1016/j.jflm.2013.10.012
- Bourget D, Whitehurst L. Capgras syndrome: A review of the neurobiological correlates and presenting clinical features in acute physical violence. Can J Psychiatry. 2004;49(1):17-25. doi:10.1177/070674370404901102
- Trotto A, Kang J, Stahl D. Interpretation Bias in Paranoia: A Systematic Review and Meta-Analysis. Clinical Psychological Science 2021;9(3):413-426. doi:10.1177/2167702620965125
- Uhlen TP, James JF. Capgras and Fregoli’s syndrome, aggression and parental training: a report of two cases. Can J Psychiatry. 1995;40(10):636-639. doi:10.1177/07067437950400108