






Cardiac Rehabilitation’s Role in Post-Event Work Return
The Role of Cardiac Rehabilitation in Facilitating Return to Work After Cardiovascular Events
Cholid Tri Tjahjono1, Maimun Zulhaidah Arthamin2
OPEN ACCESS
PUBLISHED: 31 December 2024
CITATION: TJAHJONO, Cholid Tri; ARTHAMIN, Maimun Zulhaidah. The Role of Cardiac Rehabilitation in Facilitating Return to Work After Cardiovascular Events. Medical Research Archives, [S.l.], v. 12, n. 12, dec. 2024. Available at: <https://esmed.org/MRA/mra/article/view/6016>. Date accessed: 02 nov. 2025. doi: https://doi.org/10.18103/mra.v12i12.6016.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i12.6016
ISSN 2375-1924
Abstract
Returning to work (RTW) after a cardiovascular event, such as acute coronary syndrome (ACS) or coronary artery bypass grafting (CABG), is a critical aspect of cardiac rehabilitation (CR). Effective CR not only enhances a patient’s quality of life but also ensures financial stability by reducing occupational disability-related costs. Multiple factors involved to return to work process, including physical health, psychological well-being, work-related factors, and the severity of the cardiac event. This review explores the role of CR in facilitating RTW for post-ACS and post-CABG patients, highlighting key considerations for a safe and successful transition to work and daily activities. Interdisciplinary approaches are crucial, as different medical and rehabilitation professionals contribute to optimizing patient outcomes. Furthermore, the type of work and associated physical demands must be carefully evaluated for each patient. Special attention is needed for developing countries, where cardiac rehabilitation programs are less established, to ensure these patients receive adequate support. The article concludes by discussing future strategies to improve return to work rates, improving quality of life, and minimize the economic burden of cardiovascular diseases.
Keywords
Return to work, Cardiovascular events, Cardiac rehabilitation, Acute coronary syndrome, Coronary artery bypass grafting
Introduction
Return to work (RTW) refers to a patient who, after being absent from work due to an illness or accident, comes back to work and resumes their duties. Returning to work is crucial for raising a patient’s sense of self-worth and quality of life. Cardiovascular events increase the risk of worsening job conditions, including reduced responsibilities, part-time work, salary reduction, and exclusion from work with an average loss of productivity. RTW in patients with ACS considers objective clinical data (e.g., left ventricular ejection fraction (LVEF), exercise capacity, and comorbidities), work-related factors (e.g., job satisfaction and expectations about returning), psychological conditions (e.g., anxiety, depression, fear of recurrence), and other general clinical conditions. In addition, cardiovascular events also have an impact on a patient’s ability to return to daily activities such as driving and sexual intercourse with a partner. Therefore, restoring work ability and mobility is a key goal in cardiac rehabilitation (CR), enhancing both personal and financial stability while reducing the healthcare costs associated with long-term disability.
Cardiac rehabilitation (CR) is a type of rehabilitation program designed to improve the health and quality of life of patients after a cardiac event so that they can resume their regular activities. It was initially focused on patients post-myocardial infarction or coronary artery disease, post-arterial bypass surgery, but is now being opened up more widely to patients post-coronary intervention and heart failure. The main goal of the program is to restore the individual’s condition, including optimal physical, mental, medical, psychological, social, emotional, sexual, vocational, and economic status. Numerous studies suggest that cardiovascular events have an impact on RTW levels and employability. The presence of comorbidities, low education and economic status, female, elderly, psychological conditions, and disease severity are some of the risk variables related to failed RTW after cardiovascular events.
Numerous studies further elucidate that a significant number of cardiovascular events patients struggle to maintain their jobs after RTW. CR is essential for managing cardiovascular events, improving patients’ quality of life, physical activity, and medical costs. Most patients can return to work after CR in the current era of invasive and intensive treatment for arrhythmias, ACS, and other types of heart disease. So we explored the role and impact of CR in improving quality of life, ability to perform activities of daily living independently, ability to drive, to have safe sex, and return to work.
Cardiovascular Events
1. Acute Coronary Syndrome
Acute coronary syndrome (ACS) are critical medical conditions that raise from a sudden reduction in blood flow to the heart. The ACS encompasses a spectrum of conditions, including ST elevation myocardial infarction (STEMI), non-ST elevation myocardial infarction (NSTEMI), and unstable angina. These are types of coronary heart disease (CHD), which are responsible for one-third of total deaths in people over the age of 35. ACS is a form of CHD that is always symptomatic. The retrospective study showed that return to work is an issue for ACS patients, both in the short and long term after hospital discharge. Moreover, in gaining a patient’s perspective, there are various factors that can influence this process and its end result. These different factors fall within the realm of different specialists, such as cardiologists, general practitioners, occupational health specialists, and insurance physicians, who may share responsibility for the cardiac patient’s return to work. Unfortunately, such interdisciplinary teams are currently rare. To facilitate vocational reintegration in the community, cardiac rehabilitation plays an important role, as it has been shown to increase the success of full-time RTW. In addition, patients attending cardiac rehabilitation programs return to work earlier and tend to take easier or lighter jobs.
1.1 CARDIAC REHABILITATION AFTER ACS
Cardiac rehabilitation or CR is essential for patients post-ACS, improving their physical, mental, and social well-being. Comprehensive CR programs provide tailored exercise regimens, psychological support, and guidance on lifestyle modifications to prevent recurrence. Cardiopulmonary exercise testing (CPET) and patient’s metabolic equivalents (METs), which helps assess a patient’s overall cardiopulmonary capacity and identify any remaining cardiovascular limitations during exercise. In some cases, CPET results can be correlated with the type of work the patient performed before the event, helping to ensure a safer return to their professional duties. Low-level exercise testing provides enough information to guide patients toward initial outpatient exercise therapy and suggest safe activities. Patients who do not receive exercise testing and revascularization, the occurrence of ST depression during low-intensity exercise, METs less than 5, and hypotensive exercise response have a worse prognosis. The treadmill test is recommended as the exercise modality of choice to determine ischemic threshold and electrical flow instability. If the treadmill test is not feasible, a 6-minute walk test may be a viable alternative.
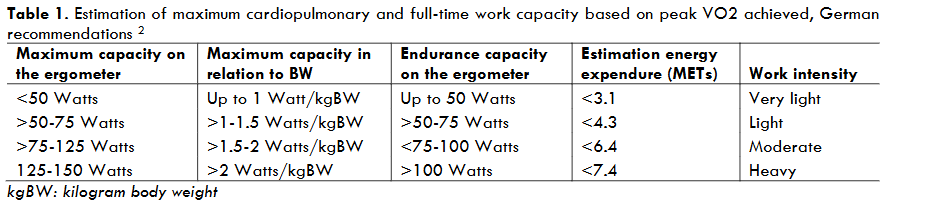
In Germany, patients’ maximum bicycle exercise capacity and endurance are interpreted as absolute values, which are also related to body weight, called the Ludwigshafen model, as shown in Table 1. In addition, there is a correlation between the energy requirement in METs according to body weight and the load performed during cycle ergometry. This scheme can be used for all patients but has limitations, such as not taking into consideration age and sex. The combination of these schemes in CPET makes it a more effective and objective method, although there is limited data for work intensity grouping using peak oxygen consumption (VO2). Cycle ergometry is usually sufficient for low- or moderate-intensity activities but not for high-intensity activities. The correlation between oxygen uptake and energy expenditure under specific work conditions is necessary to determine a patient’s ability to perform physical activity. Maximum cardiopulmonary and full-time work capacity is one of the considerations that must be made before patients can return to work. However, other aspects also need to be considered to determine the appropriate work that can be performed by patients after CR, including: age, gender, work-related factors, comorbidities (diabetes mellitus, hypertension, dyslipidemia, obesity, and chronic kidney disease), cardiac rhythm stability, complaints of shortness of breath, history of cardiogenic shock, cardiac arrest survivor, psychosocial status, and CR compliance.
1.2 FACTORS THAT INFLUENCE RETURN TO WORK
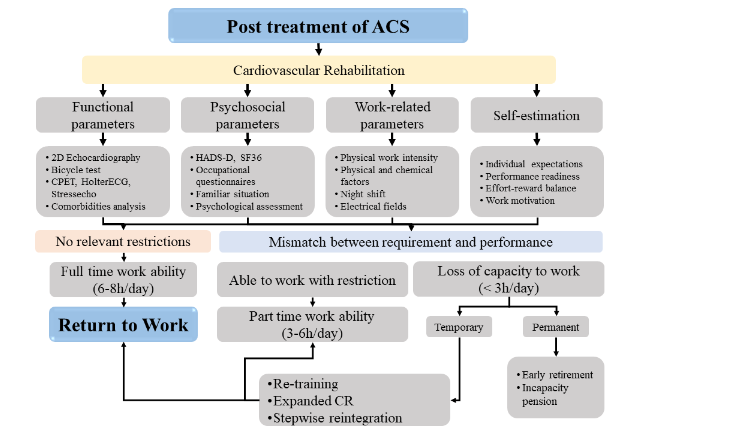
Return to work considerations are based on various factors, such as clinical, psychological, and work-related factors. Understanding these factors is essential for developing rehabilitation strategies that improve patient outcomes and facilitate a smoother transition back to employment, as shown in Figure 1. Dyspnea, chest pain, and other physical complaints may slightly hinder RTW. On the other hand, higher exercise capacity, measured by workload and VE/VCO2 slope, is independently associated with a higher probability of RTW. Comorbidities including chronic obstructive pulmonary disease, diabetes, and psychiatric illnesses (such as schizophrenia and depression) are associated with lower rates of RTW. The importance of understanding the factors that can facilitate the return to work process helps improve effective communication between doctors and patients. Facilitating factors associated with return to work include no complaints of heart disease, advice from a cardiologist, younger age, high education level, high income level, a good work environment, and supportive colleagues. Employment conditions and social security are embedded in the social environment and are outside the domain of cardiology. However, discussing returning to work early in the recovery process can motivate patients. A comprehensive assessment of these factors is needed to determine the likelihood of a successful return to the same level of work for ACS patients.
Chronic stress in the workplace results from high demands and low decision-making potential, or from a combination of high expectations and low professional satisfaction. Especially for patients with psychological vulnerabilities, persistent shift work, night shift work, or overtime hours can aggravate individuals. Objectively, job strain has an important impact on the risk of cardiovascular disease, for example, the incidence of atrial fibrillation. Women with a double burden of work and family also increase the risk of CAD. A prospective Dutch cohort study found a significant correlation between the absence of RTW and depression (odds ratio (OR) 3.48, 95% CI 1.45-8.37) and anxiety disorders (OR 2.90, 95% CI 1.00-6.38). Professional reintegration is often limited by fear of self-harm due to physical or emotional stress caused by or resulting from work. Thus, the patient’s self-assessment of their ability to adequately perform previous activities has a high prognostic value for RTW.
1.3 THE ROLE OF THE DISCIPLINES IN PREPARING ACS PATIENTS FOR A RETURN TO WORK
Working prior to coronary intervention has a higher predictive impact for RTW, but the characteristics of the tasks performed are important to evaluate to determine the probability of RTW. Patients with overt cardiovascular disease with clear pathophysiology need to be measured and evaluated for consideration of being able to perform tasks at previous jobs. Cardiologists play a central role in assessing a patient’s cardiovascular health, determining physical readiness for work, and guiding the overall rehabilitation plan. They monitor key indicators such as left ventricular ejection fraction (LVEF), exercise capacity, and heart rhythm stability to ensure that the patient can safely resume professional activities. Cardiologists also determine whether additional treatments, like revascularization, are necessary and assess the patient’s response to medication and physical exertion. Occupational physicians are responsible for determining whether the patient can return to their previous position or if adjustments, such as reduced hours, modified tasks, or gradual reintegration, are necessary. Psychological tasks, including shift and night work, production line work, piece work, or work under time pressure, are important professional parameters in the assessment of reintegration ability. Workers in three rotating shifts or permanent night shift schedules show modifications in their cardiac neurovegetative regulation due to increased sympathetic tone both at night and during daytime sleep. Work-related factors affecting occupational reintegration, including the intensity of physical effort to be performed (lifting, carrying, and moving heavy objects) and workplace situations of a physical and chemical nature (toxic fumes, high pressure or low pressure in the atmosphere, high noise levels, fine dust load, hot or cold temperatures, being in an electric field, etc.), should also be considered. Furthermore, patients with manual and physically demanding jobs are at risk of poor work outcomes. Patients with driving restrictions may be limited in their ability to travel (reach the workplace on foot, by using a vehicle, or by using public transportation).
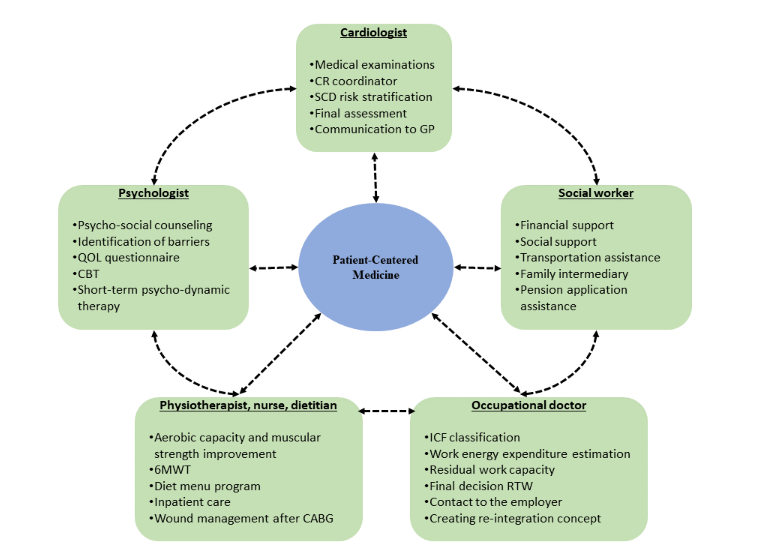
Therefore, the remaining work capacity after ACS (partial-total/temporary-permanent disability) depends on the measured parameters. The RTW and subsequent vocational reintegration may be significantly improved with CR because of the time required for assessment and consideration by the institutional team (cardiologist, occupational physician, psychologist, and workplace owner) as shown in Figure 2. A recently published meta-analysis of 18 studies focusing on RTW rates after individually delivered psychosocial and vocational interventions showed better employment rates at 3 months compared with usual care, but the effect is neutralized after 6–12 months. Identification of patients at risk of poor work outcomes should occur early in the reintegration period, ideally during post-acute CR. In general, career-related information is rarely taken into consideration during CR. A survey in France showed that only 53% of ACS patients were advised to consider RTW. Therefore, treatment of the underlying heart disease and CR is given relatively high priority, while reintegration strategies leave room for improvement.
1.4 AIR TRAVEL SAFETY AFTER ACS
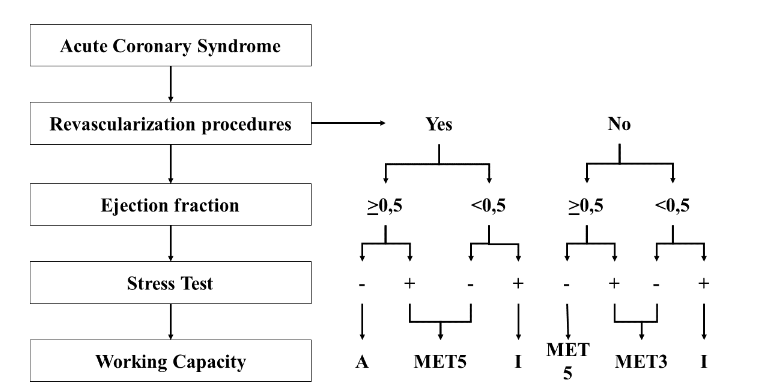
The following is an algorithm for considering an individual return to work after an ACS event, as shown in Figure 3. Patients with ACS who undergo complete revascularization, either percutaneous or surgical, with an ejection fraction >0.5 and a negative result on the stress test are able to perform all types of work. Patients undergoing complete revascularization with an ejection fraction >0.5 but a positive stress test or an ejection fraction <0.5 and a negative stress test may perform tasks requiring <5 METs. Similarly, patients who have not undergone complete revascularization with an ejection fraction >0.5 and a negative stress test result may perform tasks requiring <5 METs. Patients who underwent complete revascularization with an ejection fraction <0.5 but positive stress test results could not perform all types of work. Similarly, patients who did not undergo complete revascularization with an ejection fraction <0.5 and a positive stress test could not perform all types of work. Meanwhile, patients who have not undergone complete revascularization with an ejection fraction >0.5 and a positive stress test result, or with an ejection fraction <0.5 and a negative stress test result, can perform tasks that require <3 METs. The stress test performed was a symptom-limited stress test, defined as negative if no clinical or electrocardiographic abnormalities (ST depression >1 mm or ventricular arrhythmia) occurred at >7 METs.
1.5 FITNESS TO DRIVE AFTER ACS
After ST-segment elevation myocardial infarction (MI), patients are at risk for sudden arrhythmic death within one to two years, especially if early thrombolysis or primary angioplasty were not performed. The risk of sudden cardiac death or cardiac arrest in patients with a recent MI is highest in the first 30 days after the MI.
| Cardiac conditions | Private driving | Commercial driving |
|---|---|---|
| ACS: PCI performed | may return to driving after 1 month | may return to driving after 2 weeks |
| STEMI, LVEF <40% | may return to driving after 1 month | may return to driving after 3 months |
| STEMI, LVEF >40% | may return to driving after 2 weeks | may return to driving after 1 month |
| NSTEMI, LVEF <40% | may return to driving after 1 month | may return to driving after 3 months |
| NSTEMI, LVEF >40% | may return to driving after 2 weeks | may return to driving after 1 month |
| Unstable angina | may return to driving after 48 hours | may return to driving after 3 months |
The risk of sudden cardiac death (SCD) after acute coronary syndrome (ACS) is a significant concern. Studies have shown that patients with reduced left ventricular ejection fraction (LVEF) are at higher risk of SCD after ACS, regardless of the type of ACS (ST-segment elevation myocardial infarction [STEMI] or non-STEMI [NSTEMI]). The incidence of SCD among patients with an LVEF of 40% within 3 months after ACS was found to be 0.76%. Therefore, it is reasonable to continue restricting commercial driving for 3 months after myocardial infarction (MI) in patients with an LVEF of 40% or less. However, in post-MI patients with normal EF and high rates of revascularization, the risk of SCD ranges from 0.5% to 0.6% at 1 year. In a contemporary registry study, the SCD rate between 1 and 3 months was found to be well below the acceptable threshold of 0.083% per month (1% per year). This suggests that driving restrictions can be eased for post-MI patients with LVEF >40%.
The risk of SCD after hospitalization for unstable angina is relatively low compared to STEMI or NSTEMI. Data from a study of patients with unstable angina showed that the incidence of cardiovascular death, including SCD, was 2.6% at 2-year follow-up compared to 5.2% for NSTEMI and 3.7% for STEMI. Therefore, the consensus is to prohibit driving for 48 hours after a recent ACS with intervention and 7 days for ACS patients without intervention.
1.6 SAFE SEXUAL ACTIVITY FOLLOWING ACS
In patients without or with mild angina pectoris (class I or II), sexual activity can be performed, while in other patients it should be postponed until their condition is stabilized or optimally controlled. In patients with intermediate symptoms or whose risk is unknown, an exercise stress test can provide additional information on exercise tolerance and estimate the severity of ischemia. If the person can achieve energy consumption of ≥3-5 METs, then the risk of ischemia during sexual activity is very low. After myocardial infarction, asymptomatic patients, patients without signs of ischemia during exercise stress tests, and subjects who have undergone complete coronary revascularization have a low cardiovascular risk during sexual activity. The ACC/AHA guidelines for managing non-ST elevation MI suggest that patients can start walking immediately after hospital discharge and cardiac rehabilitation, resuming sexual activity as early as one week after myocardial infarction.
Post- Coronary Artery Bypass Grafting (CABG) Procedure
Coronary artery bypass grafting (CABG) is the primary treatment for patients with coronary artery disease (CAD) and most common treatment performed in 60% of cases of advanced heart disease. In Canada, 15,000 patients undergo coronary artery bypass grafting (CABG) surgery each year. However, after surgery, patients face challenges in managing their symptoms, returning to a normal life, and fulfilling their plans. Heart surgery significantly impacts the patient’s career and professional life. Patients undergoing CABG typically require a hospital stay of almost a week, and after discharge from the hospital, they typically require a recovery period of 2 to 6 weeks to resume normal activities and return to work if possible. Most patients need to address residual issues such as heart failure, anemia, atrial fibrillation, pulmonary abnormalities, and pain associated with thoracotomy and saphenectomy. Patients face the risk of recurrent angina or ACS later in the follow-up period due to the progression of coronary artery disease in the native coronary circulation or bypass failure, particularly with vein grafts that are more susceptible to stenosis after several years. In geriatric and debilitated patients, an increased length of hospital stay was associated with a fivefold increased risk of poor 1-year functional survival. Patients after CABG are prescribed complex medications and encouraged to adopt a healthy lifestyle, including smoking cessation, diet, moderate exercise, and psychological stress control.
2.1 RETURN TO WORK AFTER CABG
Surgery procedure is a dramatic event and most people who have the ability and need to return to work fail to do so. Furthermore, due to long waiting lists for angiography and bypass surgery, many patients lose their jobs and have no work to return to. One study found that patients who lost their jobs more than 6 months before surgery had a lower return to work rate (35%) than patients who lost their jobs less than 6 months before surgery. Occlusion of the graft causes angina recurrence at a lower rate than before (4% per year), but it still has an impact on long-term employment plans. Although return to work (RTW) is faster after angioplasty than after CABG, the long-term employment outlook is the same for both.
The RTW is an important aspect of life for post-CABG patients, leading to improved quality of life, financial security, and a sense of well-being. Although RTW has an impact on improving people’s health after surgery, research shows that factors such as the type of job, workplace accommodations, flexibility, and support from co-workers and employers affect patients’ motivation to RTW. Another study in Poland showed that economic needs, emotional factors, anxiety, and low self-esteem were factors to consider when returning to work after CABG. Failure to return to work causes irreparable harm to the individual, family, and society. Identifying facilitators and barriers to returning to work can help plan effective interventions and improve patients’ quality of life after cardiac surgery.
Guidelines from the Dutch Society of Occupational Physicians describe how to guide employees with ischemic heart disease through the return-to-work process, based on international research, and recommend return-to-work during CR to overcome possible barriers of fear and anxiety. The guidelines suggest partial or full RTW within approximately six weeks for patients after CABG, as long as postoperative biological recovery is good. Younger age, good job satisfaction, high job expectations, and absence of comorbidities are factors that facilitate faster RTW but cannot be considered comprehensive as they are all individualized internal factors. In RTW models, such as the ecological model of case management, external factors, factors outside the individual, i.e., work-related factors, and other factors influence the disability process. However, this model has never been applied to post-CABG patients. Advice from cardiologists and occupational physicians plays a role in patients’ consideration of RTW. Work-related barriers such as work stressors (i.e., excessive workload, busy workplace, staff shortage) and communication with supervisors (i.e., difficult relationships) are the most important barriers in the RTW process.
2.2 CARDIAC REHABILITATION AFTER CABG
An important goal of CR is to optimize social participation in various aspects of daily life, such as household, work, and leisure activities. Although participants were positive about their CR program, they also mentioned that the lack of follow-up after CR led to feelings of uncertainty about their activities at home and in continuing their work. This feeling of uncertainty was exacerbated by the fact that participants were advised to begin the RTW process only after completing CR, which is contrary to guideline recommendations. Return to work during CR requires coordination between the occupational physician and the cardiac rehabilitation team, which is in line with the suggestions for improvement mentioned in the Dutch rehabilitation guidelines. A specialist managing the case as the primary contact is not sufficiently embedded in current practice, resulting in treatment and RTW plans not being sufficiently aligned.
The acute phase of CR is performed under supervision in the intensive care unit (ICU), cardiac care unit (CCU), or hospital ward. Acute CR aims to restore the patient’s ability to safely perform activities of daily living (ADLs), such as feeding, toileting, and bathing, and prepare for secondary prevention. CR is also used to achieve hemodynamic stability after hospitalization for AMI or heart failure or after surgery. Prolonged bed rest can reduce exercise capacity and weakness. The CR program begins with early mobilization from the bedside, in parallel with acute care, and ends with a 6-minute walk test. If the patient can walk more than 300 m, the program moves from an ambulation program to an exercise training program. Patient and family education about disease progression is also important for subsequent lifestyle interventions and coronary risk factor management, as well as motivating the patient to continue with the CR program.
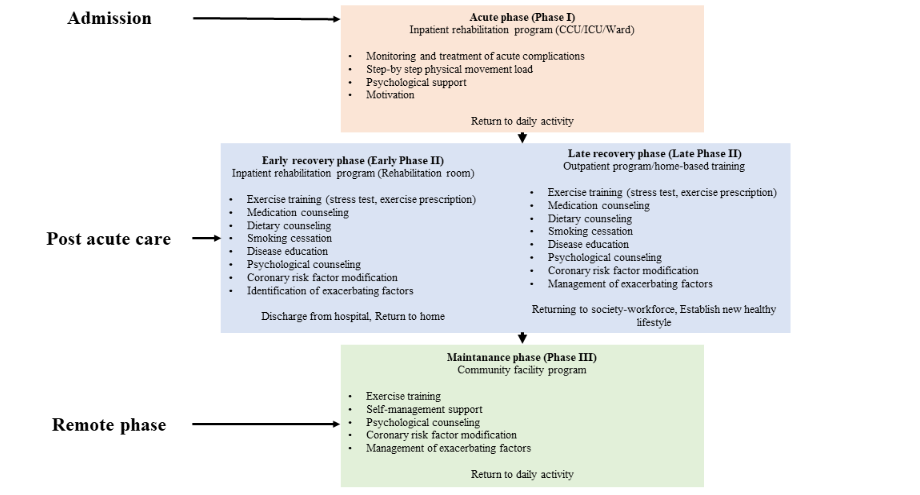
The CR takes place during the recovery phase, starting from the patient’s discharge to outpatient care and continuing until their condition stabilizes upon their return to the community. Early recovery CR begins under supervision in the CR room during hospitalization and is followed by supervised exercise training in the outpatient CR unit after discharge. Late-recovery CR involves exercise training in the outpatient CR unit and at home. In low-risk patients, unsupervised exercise training may be performed at home with themselves. An exercise plan is prescribed based on disease severity converted to risk classification, then exercise capacity is determined by cardiopulmonary exercise testing (CPET), and a treatment and CR plan are made. If CPET cannot be performed because of complications, low physical fitness, or low left ventricular function, exercise capacity should be confirmed by a 6-minute walk test. In addition, counseling programs for lifestyle modification and medication adherence, identification and management of comorbidities, and psychological counseling should be provided, especially for patients planning to undergo RTW. Patients with heart disease are prone to depression after hospital discharge due to anxiety about their physical health, financial problems, and concerns about returning to work or sexual potential.
2.3 AIR TRAVEL SAFETY AFTER CABG
After CABG, patients are able to perform daily activities according to their capabilities, taking into consideration safety issues. Airline companies also set rules for pilots and flight crews to avoid life-threatening symptoms and disruptions to flight activities. In addition, since 2004, airlines, especially those with passenger-carrying aircraft with a maximum payload of >7500 pounds, are required to have ≥1 flight crew member trained in basic life support (CPR), carry ≥1 automated external defibrillator, and have emergency medical equipment in accordance with Federal Aviation Administration (FAA) regulations. According to epidemiology, more than 2.75 billion passengers travel by air each year, many of whom are cardiac patients with implanted pacemakers or automatic defibrillators, recent revascularization, or surgery that may predispose them to deep vein thrombosis (DVT). An observational study using data from 744 million airline passengers between 2008 and 2010 reported a medical event rate of 1.6 per 100,000 passengers, with 36 medical deaths. Cardiac arrest is the most common cause of medical death and flight diversion, accounting for 8% of medical emergencies.
Although there are no specific guidelines from the American Heart Association or the American College of Cardiology for air travel after CABG, patients should not travel by air until 10 days after uncomplicated CABG due to the risk of trapped gas expansion. A post-operative clinical evaluation must be performed before travel to rule out congestive heart failure, serious arrhythmias, or residual ischemia. Various factors can affect cardiovascular health during flight, including reduced atmospheric pressure, reduced humidity, gas expansion, prolonged immobility, and increased physical and emotional stress. Most commercial aircraft fly at cruising altitudes between 22,000 and 44,000 feet, with a decrease in the partial pressure of inhaled oxygen of approximately 4 mmHg per 1,000 feet altitude. At this altitude, the atmospheric pressure decreases by about 65–85%, and the partial pressure of inspired oxygen decreases by about 60–90% from sea level. Most aircraft compress and pipe atmospheric air into the cabin to pressurize it to atmospheric pressure, typically around 7500 feet (only 25% lower than sea level) but not exceeding 8000 feet (cabin altitude). This represents only a 30% reduction in the partial pressure of inhaled oxygen, which, although close to the rapid decline of the oxyhemoglobin dissociation curve, should maintain arterial blood oxygen saturation >90% in a healthy individual. Healthy individuals typically compensate for this condition by increasing their tidal volume and heart rate. However, during turbulence or in bad weather, higher cruising altitudes may be required, resulting in a further loss of cabin pressure. In these situations, cabin altitudes above 10,000 feet are practically prohibited, as all crew and passengers must use supplemental oxygen. Therefore, passengers with ischemic heart disease and underlying heart failure (especially those with pulmonary disease) may be more susceptible to increased hypoxia because lower initial oxygen levels may lead to a further decrease in the steep portion of the oxyhemoglobin dissociation curve as atmospheric oxygen pressure decreases. It can also raise the blood pressure in the pulmonary arteries and the heart rate, systemic blood pressure, myocardial contractility, and cardiac output.
Pilots and cardiac surgery patients require a long period of intensive postoperative observation and evaluation, and returning to flight earlier than six months postoperatively is not considered. The stability of the sternum after median sternotomy is clinically assessed in flight crews as well as in the general population. The AMS may deem pilots who have undergone cardiac surgery and meet the regulatory requirements “fit to fly” to prevent unnecessary license restrictions in the future. Pilots who have undergone uncomplicated MI or PCI in a coronary artery other than the left main coronary artery may experience a shortened recovery period of approximately 3 months. Recommended tests include angiography, electrocardiogram (ECG), and treadmill stress tests no earlier than the recovery period. Imaging modalities such as stress echocardiography and nuclear imaging are reserved for those with uninterpretable ECG stress tests. A maximum ECG treadmill stress test should achieve 100% of the predicted maximal heart rate, last ≥9 minutes, and show no evidence of ischemia. It is well known and documented that CABG is better than PCI for revascularization of left main, left anterior descending, and multivessel disease. In addition, PCI is known to be less effective than surgery at achieving complete revascularization in complex CAD, which is a revalidation criterion for flight crews. The European Aviation Safety Agency (EASA) in Europe has published the medical requirements for flight crew licenses in a unique document known as Part-MED. Part-MED represents an additional set of legally binding regulations that surgeons should be aware of when operating on a professional flight crew. For pilots undergoing cardiac surgery, there are many limitations to the surgical procedure and post-operative therapy modalities. Anticoagulation remains a disqualifying condition for most commercial pilots, and partial revascularization often results in a loss of license in many countries.
2.4 GETTING STARTED WITH SAFE DRIVING AFTER CABG
The Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery (SYNTAX) trial, which compared causes of death after PCI versus CABG in patients with complex CAD, showed that patients who underwent CABG had a 0.9% risk of SCD within 30 days, 1.5% risk of SCD within 1 year, and 1.9% risk of SCD within 5 years. Other studies have shown lower rates of SCD after CABG surgery. The Coronary Revascularization Demonstrating Outcome Study in Kyoto (CREDO-Kyoto) PCI/CABG registry study showed that the SCD rate at 1 year after CABG for multivessel CAD was only 0.3%. The Surgical Treatment for Ischemic Heart Failure (STICH) trial showed that people with LVEF <35% were going to have CABG. It found that among 1,411 people who were going to have CABG, the risk of SCD was 0.35 percent at 30 days, 1.25 percent at 3 months, 2.0 percent at 6 months, and 2.8 percent at a year. According to the Canadian Cardiovascular Society’s 2023 Executive Summary on fitness to drive after cardiac surgery, post-CABG patients can drive private transportation 4 weeks after discharge and public transportation 12 weeks after discharge.
2.5 SAFE SEXUAL ACTIVITY FOLLOWING CABG
Sexual activity is an important component of quality of life for patients and partners, particularly those with CVD. Cardiopulmonary bypass (CPB) for on-pump CABG can affect serum levels of androgenic hormones, particularly testosterone, which maintain normal sexual activity. Male sexual dysfunction affects approximately 10–25% of middle-aged men worldwide. At least 75% of patients with heart disease experience one or more types of sexual dysfunction. A study by Faisal Mourad et al. (2017) assessed sexual dysfunction using the Sexual Behavior Questionnaire (SBQ) in a study of all Arab male patients younger than 60 who were candidates for on-pump CABG at Ain Shams University Hospital. The study compared patients’ sexual function before and after surgery. The data showed a significant decrease in sexual function in patients who underwent surgery compared to their preoperative status. The decline in sexual function was evident in the elements of ejaculation, erection, sexual arousal, masturbation, and spousal satisfaction.
During foreplay and sexual arousal, blood pressure and heart rate increase and rise to a maximum during orgasm. Thereafter, both quickly return to normal levels. Sexual activity is equivalent to a light or moderately short duration of physical activity (such as stairs or brisk walking), which is equivalent to 3–4 METs. Heart rate and systolic blood pressure are usually less than 130 bpm and 170 mmHg, respectively. In medical and emotional conditions, older age is a risk for difficulty in achieving orgasm and imposes greater demands on the cardiovascular system. Exercise stress testing is reasonable in patients with unknown cardiovascular risk to assess exercise capacity and the development of symptoms, ischemia, or arrhythmias. Thus, patients with ≥3-5 METs without angina, exaggerated dyspnea, ischemic ST-segment changes, cyanosis, hypotension, or arrhythmias can be evaluated. CR and regular exercise in patients with CVD are useful in reducing the risk of complications during sexual activity. This increases maximum exercise capacity and leads to a decrease in maximum blood pressure and pulse rate. Sexual activity can be resumed a few days after percutaneous coronary intervention or 6–8 weeks after coronary artery bypass grafting or non-coronary open-heart surgery. If revascularization is incomplete, an exercise stress test may provide information on residual ischemia.
Conclusion
Returning to work after a cardiovascular event can cause physical, emotional, and financial challenges. Physically, patients may experience limited stamina, while emotionally, anxiety and depression can undermine motivation. Financial and social support are also important factors. Addressing these diverse challenges through comprehensive support, customized rehabilitation programs, ongoing education, and workplace adjustments is crucial to helping patients navigate the return-to-work process successfully. By providing a supportive and accommodating environment, healthcare providers and employers can facilitate a smoother transition back to work for patients recovering from cardiovascular events, ultimately improving their overall well-being and quality of life.
Author contributions
All authors collected the data for the article, contributed substantially to the discussion of its content, wrote the article, and revised and/or edited the manuscript before submission.
Conflict of interest
The author declares no conflict of interest in the preparation of the article.
Acknowledgments
All authors collected the data for the article, contributed substantially to the discussion of its content, wrote the article, and revised and/or edited the manuscript before submission.
Funding
This research received no external funding.
Ethics approval and consent to participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
References
- Figueredo JM, García-Ael C, Gragnano A, Topa G. Well-Being at Work after Return to Work (RTW): A Systematic Review. Int J Environ Res Public Health. 2020;17(20):7490. doi:10.3390/ijerph17207490
- Reibis R, Salzwedel A, Abreu A, et al. The importance of return to work: How to achieve optimal reintegration in ACS patients. Eur J Prev Cardiol. 2019;26(13):1358-1369. doi:10.1177/2047487319839263
- Català Tella N, Serna Arnaiz C, Real Gatius J, Yuguero Torres O, Galván Santiago L. Assessment of the length of sick leave in patients with ischemic heart disease. BMC Cardiovasc Disord. 2017;17(1):32. doi:10.1186/s12872-016-0460-7
- Hu Y, Zhou T, Li X, et al. Factors influencing return to work 3 months after percutaneous coronary intervention in young and middle-aged patients with coronary heart disease: A single-center, cross-sectional study. PLOS ONE. 2023;18(4):e0284100. doi:10.1371/journal.pone.0284100
- Salzwedel A, Koran I, Langheim E, et al. Patient-reported outcomes predict return to work and health-related quality of life six months after cardiac rehabilitation: Results from a German multi-centre registry (OutCaRe). Plos One. 2020;15(5):e0232752. doi:10.1371/journal.pone.0232752
- Bresseleers J, De Sutter J. Return to work after acute coronary syndrome: Time for action. Eur J Prev Cardiol. 2019;26(13):1355-1357. doi:10.1177/2047487319840183
- Cowie MR. Returning to Work: A Forgotten Aspect of Rehabilitation for Heart Failure. Circulation. 2016;134(14):1010-1012. doi:10.1161/CIRCULATIONAHA.116.024635
- Slebus FG, Jorstad HT, Peters RJG, et al. Return to Work after an Acute Coronary Syndrome: Patients’ Perspective. Saf Health Work. 2012;3(2):117-122. doi:10.5491/SHAW.2012.3.2.117
- Nordgren L, Söderlund A. Being on sick leave due to heart failure: self-rated health, encounters with healthcare professionals and social insurance officers and self-estimated ability to return to work. Psychol Health Med. 2015;20(5):582-593. doi:10.1080/13548506.2015.1007148
- Nordgren L, Söderlund A. Being on sick leave due to heart failure: Encounters with social insurance officers and associations with sociodemographic factors and self-estimated ability to return to work. Eur J Cardiovasc Nurs. 2016;15(3):e27-36. doi:10.1177/1474515115571033
- Fiabane E. Return to work after an acute cardiac event: the role of psychosocial factors. Prev Res. Published online January 1, 2014. doi:10.11138/PER/2014.3.4.137
- Dreyer RP, Dickson VV. Return to Work After Acute Myocardial Infarction. Circ Cardiovasc Qual Outcomes. 2018;11(6):e004806. doi:10.1161/CIRCOUTCOMES.118.004806
- Taylor RS, Dalal HM, McDonagh STJ. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat Rev Cardiol. 2022;19(3):180-194. doi:10.1038/s41569-021-00611-7
- Singh A, Museedi AS, Grossman SA. Acute Coronary Syndrome. In: StatPearls [Internet]. StatPearls Publishing; 2023. Accessed March 25, 2024. https://www.ncbi.nlm.nih.gov/books/NBK459157/
- Slebus FG, Jorstad HT, Peters RJ, et al. Return to work after an acute coronary syndrome: patients’ perspective. Saf Health Work. 2012;3(2):117-122. doi:10.5491/SHAW.2012.3.2.117
- Razvi Y, Ladie DE. Cardiopulmonary Exercise Testing. In: StatPearls. StatPearls Publishing; 2024. Accessed September 22, 2024. http://www.ncbi.nlm.nih.gov/books/NBK557886/
- Winnige P, Vysoky R, Dosbaba F, Batalik L. Cardiac rehabilitation and its essential role in the secondary prevention of cardiovascular diseases. World J Clin Cases. 2021;9(8):1761-1784. doi:10.12998/wjcc.v9.i8.1761
- Vo TTD, Tuliao KV, Chen CW. Work Motivation: The Roles of Individual Needs and Social Conditions. Behav Sci. 2022;12(2):49. doi:10.3390/bs12020049
- Rørth R, Wong C, Kragholm K, et al. Return to the Workforce After First Hospitalization for Heart Failure: A Danish Nationwide Cohort Study. Circulation. 2016;134(14):999-1009. doi:10.1161/CIRCULATIONAHA.116.021859
- Döring D, Haberland BE, Ossig A, et al. Behavior of laboratory beagles: Assessment in a standardized behavior test using novel stimuli and situations. J Vet Behav. 2016;11:18-25. doi:10.1016/j.jveb.2015.10.004
- Lin P, Chen C, Pan S, et al. The association between rotating shift work and increased occupational stress in nurses. J Occup Health. 2015;57(4):307-315. doi:10.1539/joh.13-0284-OA
- De Jonge P, Zuidersma M, Bültmann U. The presence of a depressive episode predicts lower return to work rate after myocardial infarction. Gen Hosp Psychiatry. 2014;36(4):363-367. doi:10.1016/j.genhosppsych.2014.03.006
- Kostol AR, Mogstad M. How Financial Incentives Induce Disability Insurance Recipients to Return to Work. Am Econ Rev. 2014;104(2):624-655.
- Gragnano A, Negrini A, Miglioretti M, Corbière M. Common Psychosocial Factors Predicting Return to Work After Common Mental Disorders, Cardiovascular Diseases, and Cancers: A Review of Reviews Supporting a Cross-Disease Approach. J Occup Rehabil. 2018;28(2):215-231. doi:10.1007/s10926-017-9714-1
- Pinto N, Shah P, Haluska B, Griffin R, Holliday J, Mundy J. Return to work after coronary artery bypass in patients aged under 50 years. Asian Cardiovasc Thorac Ann. 2012;20(4):387-391. doi:10.1177/0218492312437881
- Batchelor WB, Anwaruddin S, Wang DD, et al. The Multidisciplinary Heart Team in Cardiovascular Medicine. JACC Adv. 2023;2(1):100160. doi:10.1016/j.jacadv.2022.100160
- Worcester MU, Elliott PC, Turner A, et al. Resumption of Work After Acute Coronary Syndrome or Coronary Artery Bypass Graft Surgery. Heart Lung Circ. 2014;23(5):444-453. doi:10.1016/j.hlc.2013.10.093
- Lamberti M, Ratti G, Gerardi D, et al. Work-related outcome after acute coronary syndrome: Implications of complex cardiac rehabilitation in occupational medicine. Int J Occup Med Environ Health. 2016;29(4):649-657. doi:10.13075/ijomeh.1896.00643
- O’Brien L, Wallace S, Romero L. Effect of Psychosocial and Vocational Interventions on Return-to-Work Rates Post–Acute Myocardial Infarction: A SYSTEMATIC REVIEW. J Cardiopulm Rehabil Prev. 2018;38(4):215-223. doi:10.1097/HCR.0000000000000261
- Latil F, Iliou MC, Boileau C, et al. Retour au travail après un accident coronarien aigu. Ann Cardiol Angéiologie. 2017;66(2):81-86. doi:10.1016/j.ancard.2016.12.006
- Alegria-Ezquerra’ ’Eduardo, Grima’ ’A. Reporting on coronary patients for return to work: an algorithm. 2012. Accessed April 16, 2024. https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-10/Reporting-on-coronary-patients-for-return-to-work-an-algorithm
- Ainsworth BE, Haskell WL, Leon AS, et al. Compendium of Physical Activities: classification of energy costs of human physical activities: Med Sci Sports Exerc. 1993;25(1):71-80. doi:10.1249/00005768-199301000-00011
- Bagshaw M, Illig P. The Aircraft Cabin Environment. In: Travel Medicine. Elsevier; 2019:429-436. doi:10.1016/B978-0-323-54696-6.00047-1
- Pearce E, Haffner F, Brady LB, et al. Nonurgent Commercial Air Travel after Acute Coronary Syndrome: A Review of 288 Patient Events. Air Med J. 2014;33(5):222-230. doi:10.1016/j.amj.2014.04.013
- Meisinger C, Kirchberger I, Raake P, Linseisen J, Schmitz T. Fatigue, Depression and Health-Related Quality of Life in Patients with Post-Myocardial Infarction during the COVID-19 Pandemic: Results from the Augsburg Myocardial Infarction Registry. J Clin Med. 2023;12(19):6349. doi:10.3390/jcm12196349
- Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44(38):3720-3826. doi:10.1093/eurheartj/ehad191
- Guerra PG, Simpson CS, Van Spall HGC, et al. Canadian Cardiovascular Society 2023 Guidelines on the Fitness to Drive. Can J Cardiol. 2024;40(4):500-523. doi:10.1016/j.cjca.2023.09.033
- Bellicini MG, Cersosimo A, Cerini M, Bontempi L, Curnis A, Arabia G. ICD early after myocardial infarction: it is really necessary to wait 40 days before implantation? J Interv Card Electrophysiol. 2023;67(3):439-441. doi:10.1007/s10840-023-01711-9
- Faxén J, Jernberg T, Hollenberg J, Gadler F, Herlitz J, Szummer K. Incidence and Predictors of Out-of-Hospital Cardiac Arrest Within 90 Days After Myocardial Infarction. J Am Coll Cardiol. 2020;76(25):2926-2936. doi:10.1016/j.jacc.2020.10.033
- Gatzoulis KA, Tsiachris D, Arsenos P, et al. Arrhythmic risk stratification in post-myocardial infarction patients with preserved ejection fraction: the PRESERVE EF study. Eur Heart J. 2019;40(35):2940-2949. doi:10.1093/eurheartj/ehz260
- Alnasser SMA, Huang W, Gore JM, et al. Late Consequences of Acute Coronary Syndromes: Global Registry of Acute Coronary Events (GRACE) Follow-up. Am J Med. 2015;128(7):766-775. doi:10.1016/j.amjmed.2014.12.007
- Levine GN, Steinke EE, Bakaeen FG, et al. Sexual Activity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2012;125(8):1058-1072. doi:10.1161/CIR.0b013e3182447787
- Lange RA, Levine GN. Sexual Activity and Ischemic Heart Disease. Curr Cardiol Rep. 2014;16(2):445. doi:10.1007/s11886-013-0445-4
- Doenst T, Caldonazo T, Schneider U, et al. Cardiac Surgery 2020 Reviewed. Thorac Cardiovasc Surg. Published online July 29, 2021. doi:10.1055/s-0041-1729762
- De Waard D, Fagan A, Minnaar C, Horne D. Management of patients after coronary artery bypass grafting surgery: a guide for primary care practitioners. Can Med Assoc J. 2021;193(19):E689-E694. doi:10.1503/cmaj.191108
- Arora RC, Manji RA, Singal RK, Hiebert B, Menkis AH. Outcomes of octogenarians discharged from the hospital after prolonged intensive care unit length of stay after cardiac surgery. J Thorac Cardiovasc Surg. 2017;154(5):1668-1678.e2. doi:10.1016/j.jtcvs.2017.04.083
- Morice MC, Serruys PW, Kappetein AP, et al. Five-Year Outcomes in Patients With Left Main Disease Treated With Either Percutaneous Coronary Intervention or Coronary Artery Bypass Grafting in the Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery Trial. Circulation. 2014;129(23):2388-2394. doi:10.1161/CIRCULATIONAHA.113.006689
- Alahdab F, Zuhri Yafi R, Chaar A, et al. Aspirin dosage for the prevention of graft occlusion in people undergoing coronary surgery: A systematic review and meta-analysis. Avicenna J Med. 2020;10(4):198-207. doi:10.4103/ajm.ajm_17_20
- Soleimani M, Babagoli M, Baghdadi S, et al. Return to work following primary total hip arthroplasty: a systematic review and meta-analysis. J Orthop Surg. 2023;18(1):95. doi:10.1186/s13018-023-03578-y
- Frederix I, Solmi F, Piepoli MF, Dendale P. Cardiac telerehabilitation: A novel cost-efficient care delivery strategy that can induce long-term health benefits. Eur J Prev Cardiol. 2017;24(16):1708-1717. doi:10.1177/2047487317732274
- Izawa H, Yoshida T, Ikegame T, et al. Standard Cardiac Rehabilitation Program for Heart Failure. Circ J Off J Jpn Circ Soc. 2019;83(12):2394-2398. doi:10.1253/circj.CJ-19-0670
- Makita S, Yasu T, Akashi YJ, et al. JCS/JACR 2021 Guideline on Rehabilitation in Patients With Cardiovascular Disease. Circ J. 2022;87(1):155-235. doi:10.1253/circj.CJ-22-0234
- Hare DL, Toukhsati SR, Johansson P, Jaarsma T. Depression and cardiovascular disease: a clinical review. Eur Heart J. 2014;35(21):1365-1372. doi:10.1093/eurheartj/eht462
- Hammadah M, Kindya BR, Allard‐Ratick MP, et al. Navigating air travel and cardiovascular concerns: Is the sky the limit? Clin Cardiol. 2017;40(9):660-666. doi:10.1002/clc.22741
- Peterson DC, Martin-Gill C, Guyette FX, et al. Outcomes of Medical Emergencies on Commercial Airline Flights. N Engl J Med. 2013;368(22):2075-2083. doi:10.1056/NEJMoa1212052
- Mieske K, Flaherty G, O’Brien T. Journeys to High Altitude—Risks and Recommendations for Travelers with Preexisting Medical Conditions. J Travel Med. 2010;17(1):48-62. doi:10.1111/j.1708-8305.2009.00369.x
- Hobkirk JP, Damy T, Walters M, et al. Effects of reducing inspired oxygen concentration for one hour in patients with chronic heart failure: implications for air travel. Eur J Heart Fail. 2013;15(5):505-510. doi:10.1093/eurjhf/hft003
- Syburra T, Nicol E, Mitchell S, Bron D, Rosendahl U, Pepper J. To fly as a pilot after cardiac surgery. Eur J Cardiothorac Surg. 2018;53(3):505-511. doi:10.1093/ejcts/ezx346
- Authors/Task Force members, Windecker S, Kolh P, et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35(37):2541-2619. doi:10.1093/eurheartj/ehu278
- Mohr FW, Morice MC, Kappetein AP, et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial. Lancet Lond Engl. 2013;381(9867):629-638. doi:10.1016/S0140-6736(13)60141-5
- Sipahi I, Akay MH, Dagdelen S, Blitz A, Alhan C. Coronary artery bypass grafting vs percutaneous coronary intervention and long-term mortality and morbidity in multivessel disease: meta-analysis of randomized clinical trials of the arterial grafting and stenting era. JAMA Intern Med. 2014;174(2):223-230. doi:10.1001/jamainternmed.2013.12844
- European Aviation Safety Agency. Acceptable Means of Compliance and Guidance Material to Part-MED. Eur Aviat Saf Agency Hqrs. Published online 2011. https://www.easa.europa.eu/sites/default/files/dfu/AMC%20and%20GM%20on%20the%20medical%20certification%20of%20pilots%20and%20medical%20fitness%20of%20cabin%20crew.pdf
- Authors/Task Force members, Windecker S, Kolh P, et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35(37):2541-2619. doi:10.1093/eurheartj/ehu278