





Cerebral Small Vessel Disease in Alzheimer’s Patients
Differences in Cerebral Small Vessel Disease in Patients with Dementia in Alzheimer’s Disease Compared to Patients with Dementia in Vascular Dementia
Ivan V. Maksimovich
- Clinic of Cardiovascular Diseases named after Most Holy John Tobolsky, Building 2, Block 15, 6th Lazareki Str., 119619 Moscow, Russia
OPEN ACCESS
PUBLISHED:30 December 2024
CITATION: Maksimovich, I.V., 2024. Differences in Cerebral Small Vessel Disease in Patients with Dementia in Alzheimer’s Disease Compared to Patients with Dementia in Distal Cerebral Atherosclerosis. Medical Research Archives, [online] 12(12).
https://doi.org/10.18103/mra.v1i2.6219
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v1i2.6219
ISSN 2375-1924
ABSTRACT
Background: The number of people with dementia is constantly increasing and currently amounts to over 55 million people worldwide. Common causes leading to its progression are Alzheimer’s disease and distal cerebral atherosclerosis. These diseases are accompanied by the development of specific Cerebral Small Vessel Disease.
Aims: This research is devoted to comparing Cerebral Small Vessel Disease caused by Alzheimer’s dementia to Cerebral Small Vessel Disease, developing in dementia caused by distal cerebral atherosclerosis.
Methods: For the research, 1024 dementia patients aged 28–81 (mean age 77.5) were selected, 719 males (70.22%), 305 females (29.78%).
Test Group 1: 93 (9.08%) patients had Alzheimer’s disease. According to dementia severity, the patients were divided into: a preclinical stage (dementia TDR-0) – 10, a mild stage (dementia TDR-1) – 26, a moderately severe stage (dementia TDR-2) – 40, a severe stage (dementia TDR-3) – 17 people.
Test Group 2: 931 (90.92%) patients had distal cerebral atherosclerotic lesions. Of these: 52 (5.59%) had early signs of chronic cerebrovascular insufficiency, 484 (51.99%) had pronounced signs of chronic cerebrovascular insufficiency, 306 (32.87%) had severe chronic cerebrovascular insufficiency, 27 (2.90%) had Binswanger’s disease, 62 (6.66%) had vascular parkinsonism. According to dementia severity, patients were divided into: 445 (47.80%) with unpronounced dementia, 332 (35.66%) with CDR-1 dementia, 132 (14.18%) with CDR-2 dementia, and 22 (2.36%) with CDR-3 dementia.
Results:
Test Group 1. In all 93 cases, dyscirculatory angiopathy of Alzheimer’s type was detected, which is manifested in atherosclerosis absence, reduction of capillaries in the temporal regions, large arteriovenous shunts development, venous trunks expansion, discharge of arterial blood into the venous bed, and venous stasis.
Test Group 2. In all 931 cases, multiple distal cerebral atherosclerotic lesions were detected, combining stenosis and occlusion, small arteriovenous shunts, absence of pathological venous trunks, venous stasis.
Conclusion: In Alzheimer’s disease, Cerebral Small Vessel Disease has a specific type of changes characteristic only to this disease, which are manifested in dyscirculatory angiopathy of Alzheimer’s type.
In distal cerebral atherosclerosis, Cerebral Small Vessel Disease manifests itself in atherosclerotic lesions of the distal arteries, arterioles and capillaries. These lesions are not found in Alzheimer’s disease.
Keywords:
Cerebral Small Vessel Disease; CSVD; Dementia; Alzheimer’s disease; AD; Dyscirculatory angiopathy of Alzheimer’s type; Distal Cerebral Atherosclerosis; Binswanger’s Disease; BD; Vascular Parkinsonism; VP.
Introduction
The number of people with signs of dementia is constantly increasing among the population of various countries. According to the World Health Organization, there are currently over 55 million people suffering from dementia in the world. Every year, the number of patients with dementia increases by 10 million people, which is associated with an increase in life expectancy and an increase in neurodegenerative and ischemic diseases¹,².
The most common causes leading to the development of dementia are Alzheimer’s disease (AD) and various types of cerebral atherosclerosis.
The brain is an extremely complex organ anatomically and physiologically. Due to the need for high blood supply, 1 cubic centimeter of cerebral tissue contains from 3 to 4 thousand capillaries. No other human organ has so many microvessels. As a result, the brain is the organ most actively supplied with blood. This leads to the fact that even a minor violation of cerebral hemodynamics and blood supply causes or contributes to the development of ischemic or non-degenerative lesions³.
Both AD and distal cerebral atherosclerosis are united not only by the fact that they lead to dementia, but also by the fact that these diseases are accompanied by the development of Cerebral small vessel disease (CSVD) specific to each of the two diseases⁴–⁶. The causes, etiology, pathogenesis, period of development, and localization of CSVD are different, but they all disrupt cerebral microcirculation and metabolic processes in cerebral tissue.
In terms of incidence, AD ranks first among neurodegenerative diseases accompanied by the development of dementia. In 2024, 6.9 million people with AD were registered in the United States. Even though in 5% of cases the disease develops at a fairly young age, only patients aged 65 years and older were considered⁷. It is important to take into account that the correct diagnosis of AD is not made in all cases, therefore, the total number of patients with AD is much higher⁹. According to preliminary estimates, by 2060 the number of patients with AD in the USA may exceed 14 million people⁸.
The etiology and pathogenesis of AD are complex and have not yet been fully studied¹,²,⁸,¹⁰,¹¹. The disease begins to develop latently, early cerebrovascular and atrophic cerebral changes appear 20–30 years or more before the onset of clinical manifestations of the disease. Changes in the intracerebral arterial, microcirculatory and venous bed, as well as involutional changes in the temporal lobes are observed in direct descendants of patients suffering from AD, which indicates the congenital, hereditary nature of these disorders. Since patients do not present classical complaints, such an extremely long preclinical stage, AD is quite difficult to detect¹,⁴,⁵,¹⁰,¹³.
Considering the causes of AD, it is necessary to take into account that the disease develops not only as a result of disruption of the exchange of amyloid beta (Aβ) and tau protein in the cerebral tissue and vascular wall, but also as a result of changes in cerebral angioarchitectonics, microcirculation and hemodynamics that are specific only to this disease⁵,¹⁰,²¹.
For the first time, in the first third of the last century, vascular changes in AD were discovered by the Swiss psychiatrist F. Morel. He described cerebral dysoric or drusen angiopathy in this disease²².
According to modern data, vascular and microcirculatory changes in AD are extremely specific in nature, associated with a decrease in the number of cerebral capillaries and disruption of cerebral microcirculation. These lesions constitute Cerebral small vessel disease (CSVD)⁵,¹⁰,²¹.
The number of capillaries in the brain is reduced, and the distal arterial blood flow decreases⁷,¹¹,¹⁴. The process is accompanied by the disruption of venous outflow, which leads to a hemodynamic disorder specific to AD¹¹,¹²,²³. Changes in hemodynamics lead to the disruption of metabolic processes in the cerebral tissue and damage to the neurovascular unit (NVU)⁴,⁵,¹¹–¹⁶,¹⁷,¹⁸,²⁰,²¹.
Hypoxia and specific capillary changes disrupt the physiological metabolism of amyloid beta (Aβ), cause dysfunction of the blood-brain barrier (BBB) and lead to the development of AD and dementia¹⁴–¹⁸,²⁴–²⁶. The progression of AD leads to a decrease in natural physiological intracerebral angiogenesis²³,²⁶.
The combination of such changes in cerebral angioarchitectonics and microcirculation is called “Dyscirculatory angiopathy of Alzheimer’s type (DAAT)”¹⁰,¹³,²³,²⁶.
Atherosclerosis of distal intracerebral vessels develops in elderly people. This is a fairly slow process, accompanied by its own specific Cerebral small vessel disease (CSVD), which gradually leads to cerebrovascular insufficiency and the development of dementia¹³,¹⁴,²⁷,²⁹. About 29–37% of elderly people have varying degrees of atherosclerotic lesions of the distal intracerebral branches⁶.
In distal forms of intracerebral atherosclerosis, there occur atherosclerotic lesions of small arterial branches and capillaries³,⁶,²³,²⁷,²⁸,²⁹. This process can be accompanied by transient attacks and lacunar microstrokes. Progression of atherosclerotic lesions leads to the development of cortical, subcortical and mixed strokes. The severity of strokes and the level of dementia depend on the prevalence of atherosclerotic lesions and the volume of ischemic cerebral tissue.
In Binswanger disease (BD) and vascular parkinsonism (VP), the distal atherosclerotic process develops at the subcortical level, causing ischemic damage to the white cerebral matter²³,³⁰,³¹.
In BD, the microvascular atherosclerotic lesion is disseminated and extends to various subcortical areas. The greater the volume of cerebral tissue involved in the subcortical lesion is, the more severe the level of dementia is³¹–³³.
In VP, the microvascular atherosclerotic lesion is less widespread and is usually located in the pons, thalamus, and basal ganglia. Due to the small size and localization of the atherosclerotic lesion, dementia in VP is usually expressed to a lesser degree³⁰,³¹.
This research is devoted to the study of angioarchitectonics and Cerebral Small Vessel Disease developing in dementia caused by Alzheimer’s disease in comparison with Cerebral Small Vessel Disease developing in dementia caused by distal cerebral atherosclerosis in Binswanger’s disease and vascular parkinsonism.
Methods
Our study of microcirculation disorders in cerebral atherosclerosis and cerebral neurodegenerative lesions began in 1985 and continues to this day. In this research, all examinations were performed with the written consent of patients and their relatives, as well as with the approval of The Ethical Review Board (ERB) (Protocol No. 3 of 01-12-2003, Protocol No. 12 of 04-30-2014, Protocol No. 12 of 01-12-2018).
PATIENT SELECTION CRITERIA:
- consent of patients and their relatives to the examination;
- absence of concomitant diseases that could interfere with the examination;
- satisfactory somatic condition of patients allowing the examination to be carried out;
- complaints consistent with AD, signs of dementia and cognitive impairment consistent with this disease;
- complaints and signs of various forms of distal cerebral atherosclerosis, signs of dementia and cognitive impairment consistent with the severity of the lesion;
- cerebral involutional and atrophic changes corresponding to the severity of the lesion.
PATIENT EXAMINATION
- The severity of dementia was clinically assessed using the Clinical Dementia Rating scale (CDR)³⁴.
- Cognitive functions were assessed using the Mini-Mental State Examination (MMSE)³⁵.
- Laboratory tests were conducted in accordance with the requirements and principles of interventional neuroangiology.
- Cerebral blood flow and microcirculation were assessed with the classical method, in static and dynamic modes, using scintigraphy (SG) with TC 99M Pertechnetate 555.
- Cerebral perfusion blood filling was assessed in standard automatic modes, defining pulse blood filling disorders in the cerebral hemispheres using rheoencephalography (REG).
- Structural cerebral changes were assessed with the help of CT and MRI, using standard methods. In patients with AD, the digital morphometric scale “The Tomography Dementia Rating scale” (TDR) was used to objectively determine the severity of dementia³⁴,³⁷.
- Intracerebral vascular and microcirculatory bed was defined using cerebral multi-gated angiography (MUGA) with digital image processing.
The study included 1024 patients, of which:
Test Group 1 consisted of 93 (9.08%) patients from 34 to 80 years old (mean age 67.5), 32 males (34.40%) and 61 females (65.59%), suffering from AD with dementia of varying severity.
Test Group 2 included 931 (90.92%) people from 28 to 81 years old (mean age 78), 687 (73.79%) males and 244 females (26.21%), with distal cerebral atherosclerosis, accompanied by chronic cerebrovascular insufficiency of varying severity, cerebral involutional and atrophic changes without large ischemic foci.
Depending on the type of distal cerebrovascular atherosclerotic lesion and the prevalence of the process, patients were divided into the following groups:
- early signs of chronic cerebrovascular insufficiency with distal atherosclerotic lesion – 52 (5.59%) patients. Complaints of this group of patients pointed to cerebral hemodynamic disorders;
- more pronounced signs of chronic cerebrovascular insufficiency with distal atherosclerotic lesions – 484 (51.99%) patients. Medical history of transient disorders in cerebral blood flow – 165 (34.09%) patients of this group;
- a more severe form of chronic cerebrovascular insufficiency with widespread distal cerebral atherosclerotic lesions – 306 (32.87%) patients. These patients had a medical history of small focal strokes;
- Binswanger disease (BD) – 27 (2.90%) patients;
- vascular parkinsonism (VP) – 62 (6.66%) patients.
Results
TEST GROUP 1
CT and MRI with digital morphometry of cerebral tissues according to the Tomography Dementia Rating scale (TDR)³⁴,³⁶,³⁷. As a result of using the TDR scale, specific involutional and atrophic changes in the temporal lobes were revealed in patients, which allow determining the stages of AD and the severity of dementia:
- preclinical stage of AD – TDR-0 – 10 (10.75%) people. In patients of this group, involutional changes in the brain are manifested by atrophy of the temporal lobes with a decrease in tissue mass by 4–8%; there is no dementia, but there are increasing memory disorders; cognitive functions are reduced to 26–28 MMSE points. Each of these patients had direct relatives suffering from AD (Fig. 1A), (Table 1);
- mild stage of AD – TDR-1 – 26 (27.96%) people. In patients of this group, involutional changes in the brain are manifested by atrophy of the temporal lobes with a decrease in tissue mass by 9–18%; mild dementia, corresponding to CDR-1; cognitive functions are reduced to 20–25 MMSE points. History of the disease is 2 years (Fig. 1B), (Table 1);
- moderately severe stage of AD – TDR-2 – 40 (43.01%) people. In patients of this group, involutional changes in the brain are manifested by atrophy of the temporal lobes with a decrease in tissue mass by 19–32%; moderate dementia, corresponding to CDR-2; cognitive functions are reduced to 12–19 MMSE points. History of the disease is 2–6 years (Fig. 1C), (Table 1);
- severe AD stage – TDR-3 – 17 (18.28%) people. In patients of this group, involutional changes in the brain are manifested by atrophy of the temporal lobes with a decrease in tissue mass by 33–62%; severe dementia, corresponding to CDR-3; cognitive functions are reduced to 7–11 MMSE points. History of the disease is 7–12 years (Fig. 1D), (Table 1).
Involutional and atrophic changes in the temporal lobes, as well as general cerebral changes in patients of Test Group 1 and Test Group 2, are presented in Table 1.
FIGURE 1
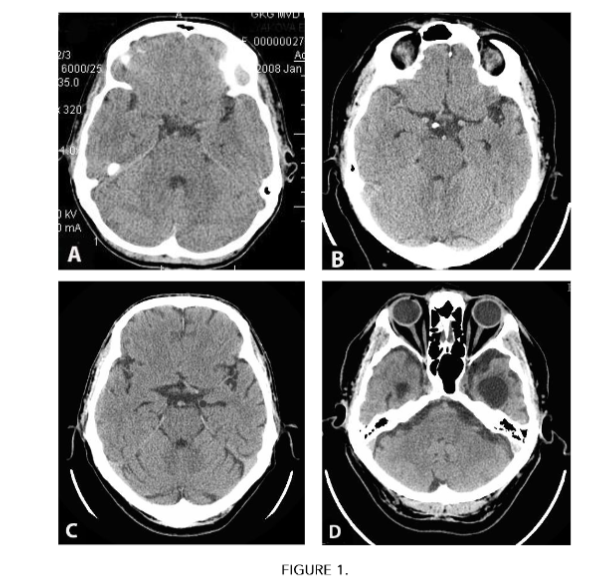
CT scans of the brain of patients with different AD stages according to The Tomography Dementia Rating scale.
A – preclinical stage TDR-0, decrease in tissue mass of the temporal lobes: on the right by 7%, on the left by 8%.
B – mild stage TDR-1, decrease in tissue mass of the temporal lobes: on the right by 9%, on the left by 14%.
C – moderately severe stage TDR-2, decrease in tissue mass of the temporal lobes: on the right by 19%, on the left by 22%.
D – severe stage TDR-3, decrease in tissue mass of the temporal lobes: on the right by 41%, on the left by 58%
Table 1. Cerebral changes in the examined patients according to CT and MRI data
| CEREBRAL CHANGES | Test Group 1 N=93 | Test Group 2 N=931 | p (chi-square) |
|---|---|---|---|
| Changes in temporal areas | |||
| Local involutive changes of the brain cortex in temporal areas | 93 (100%) | 0 | |
| Local atrophy of temporal lobes with 4–8% decrease in tissue mass (TDR-0) | 10 (10.75%) | 0 | |
| Local atrophy of temporal lobes with 9–18% decrease in tissue mass (TDR-1) | 26 (27.96%) | 0 | p<0.01 |
| Local atrophy of temporal lobes with 19–32% decrease in tissue mass (TDR-2) | 40 (41.67%) | 0 | |
| Local atrophy of temporal lobes with 33–62% decrease in tissue mass (TDR-3) | 17 (17.71%) | 0 |
| General cerebral changes | | | |
| Multiple calcium salts deposits in intracranial vessels | 0 | 918 (98.60%) | p<0.01 |
| Foci of gliosis in the gray and white matter of the brain | 0 | 198 (21.27%) | p<0.01 |
| Small postischemic cysts of the gray and white matter of the brain | 0 | 312 (33.51%) | p<0.01 |
| General neurodegenerative changes in the cortex of the brain | 48 (51.61%) | 803 (86.25%) | p<0.01 |
| Sylvian fissures widening signs | 93 (100%) | 884 (94.96%) | Not significant |
| Leucoaraiosis signs | 0 | 176 (18.90%) | p<0.01 |
| Occlusive hydrocephaly signs | 57 (61.29%) | 412 (44.25%) | p<0.01 |
To define the differences of the symptoms under study, we conducted an analysis of contingency tables with Chi-square criterion. All the figures except for “Sylvian fissures widening signs” revealed significant differences (p<0.01). The statistical analysis was accomplished with the help of Statsoft Statistica 10 program.
Laboratory tests:
- Increased blood lipid levels were noted in 35 (37.63%) cases.
- Hypercoagulation phenomena were noted in 39 (41.94%) cases.
Cerebral SG:
A decrease in blood flow in the cerebral hemispheres was noted in all 93 (100%) cases.
Cerebral REG:
A decrease in the volumetric perfusion blood filling in the carotid system was noted in all 93 (100%) cases.
Cerebral MUGA with digital image processing revealed “Dyscirculatory angiopathy of Alzheimer’s type” (DAAT):
- There were no signs of atherosclerotic changes in extra- and intracranial arteries in 84 (90.32%) cases; weak signs of initial atherosclerotic changes were revealed in 9 (9.68%) cases (Table 2).
- A decrease in the number (reduction) of capillaries with the development of hypovascular zones in the temporal and frontoparietal regions were detected in all 93 (100%) cases (Table 2), (Fig. 2 A(1), Fig. 2 B(1)).
- Local arteriovenous shunts in the basins of the anterior villous arteries supplying the temporal lobes, as well as in the basins of the distal arterial branches supplying the frontoparietal regions of the brain were detected in all 93 (100%) cases (Table 2), (Fig. 2 A(2), Fig. 2 B(2), Fig. C(2), Fig. D(2)).
- Local early discharge of arterial blood into the venous bed, accompanied by simultaneous contrasting of arteries and veins, were detected in all 93 (100%) cases (Table 2), (Figure 2 C(3)).
- Abnormally dilated venous trunks, into which blood flows through arteriovenous shunts of the temporal and frontoparietal regions, were detected in 84 (90.32%) cases (Table 2), (Fig. 2 C(3), Fig. D(3)).
- Abnormal stasis of venous blood at the borders of the frontal and parietal lobes, caused by increased blood flow through arteriovenous shunts, was detected in 85 (91.40%) cases (Table 2), (Fig. 2 D(4)).
- Increased looping of distal intracranial arterial branches was detected in 74 (79.57%) cases (Table 2).
The angioarchitectonic and CSVD abnormalities of patients from Test Group 1 and Test Group 2 are presented in Table 2.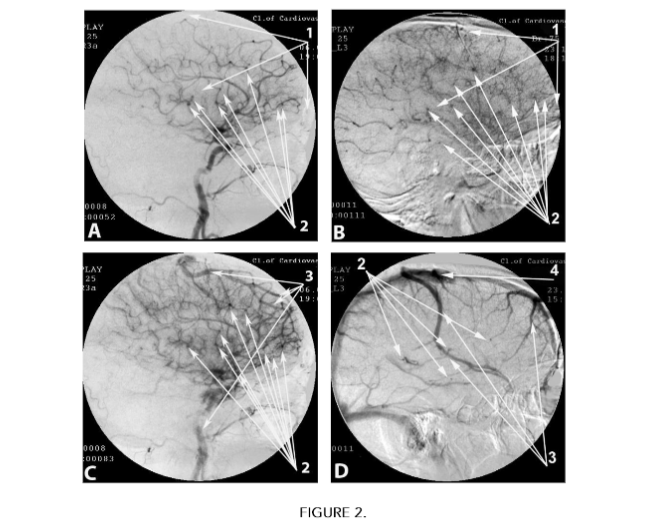
Cerebral MUGA of patients with Dyscirculatory angiopathy of Alzheimer’s type (DAAT)
A. Arterial phase:
- Capillary reduction with development of hypovascular zones in the temporal and frontoparietal regions.
- Local arteriovenous shunts.
B. Parenchymal stage:
- Capillary reduction with development of hypovascular zones in the temporal and frontoparietal regions.
- Local arteriovenous shunts.Simultaneous contrast of arteries and veins.
D. Late venous phase.
2. Local arteriovenous shunts.
3. Abnormally dilated venous trunks.
4. Abnormal venous congestion.
Table 2. Cerebral small vessel disease of the examined patients according to MUGA data
CEREBRAL VASCULAR CHANGES
Test Group 1 N=93
Test Group 2 N=931
p (chi-square)
Reduction of capillaries with the development of hypovascular zones in the temporal and frontoparietal regions
93 (100%)
0
p<0.01
Local multiple arteriovenous shunts in temporal and frontoparietal regions
93 (100%)
0
p<0.01
Local early discharge of arterial blood into the venous bed in temporal and frontoparietal regions
93 (100%)
0
p<0.01
Local development of abnormally widened lateral venous branches in temporal and frontoparietal regions
84 (90.32%)
0
p<0.01
Abnormal stagnation of venous blood at the border of frontal and parietal regions
85 (91.40%)
0
p<0.01
Increased looping of distal intracranial branches
74 (79.57%)
69 (7.41%)
p<0.01
Atherosclerotic changes of intracerebral distal arterial and capillary bed
0
931 (100%)
p<0.01
Stenosis of distal arterial branches and capillaries at the level of cerebral gray and white matter
0
931 (100%)
p<0.01
Occlusions of distal arterial branches and capillaries at the level of cerebral gray and white matter
0
348 (37.38%)
p<0.01
Decreased capillary blood flow at the level of cerebral gray and white matter
0
768 (82.49%)
p<0.01
Multiple disseminated small diameter arteriovenous shunts at the level of the gray matter of the brain
0
386 (41.46%)
p<0.01
Subcortical, disseminated, early arterial blood flow into the venous bed without the development of abnormal venous trunks and venous blood stagnation
0
245 (26.32%)
p<0.01
Subcortical atherosclerotic occlusions of distal capillary branches of cerebral white matter
0
89 (9.56%)
p<0.01
Subcortical disseminated and local decrease in capillary blood flow at the level of cerebral white matter
0
89 (9.56%)
p<0.01
Subcortical multiple disseminated small diameter arteriovenous shunts at the level of cerebral white matter
0
27 (2.90%)
p<0.01
Subcortical, multiple disseminated, early arterial-venous blood flow at the level of the white matter of the brain
0
27 (2.90%)
p<0.01
Subcortical, single local arteriovenous shunts of small diameter at the level of cerebral white matter
0
62 (6.66%)
p<0.01
Subcortical, local early flow of arterial blood into the venous bed at the level of the white matter of the brain
0
62 (6.66%)
p<0.01
To define the differences in the symptoms under study, we conducted an analysis of contingency tables with Chi-square criterion. All the figures revealed significant differences (p<0.01). The statistical analysis was accomplished with the help of Statsoft Statistica 10 program.
TEST GROUP 2
CT and MRI:
No AD-specific involutional and atrophic changes in the temporal lobes were detected in any case (Table 1).
General cerebral neurodegenerative and involutional changes of varying severity and localization are presented (Table 1).
Determination of the clinical stage of dementia (CDR) and the severity of cognitive impairment (MMSE):
In 52 (5.59%) patients with early manifestations of chronic cerebrovascular insufficiency and distal atherosclerotic lesions, clear signs of dementia and cognitive impairment were not detected in any case.
In 484 (51.99%) patients with more pronounced signs of chronic cerebrovascular insufficiency and distal atherosclerotic lesions, dementia at the CDR-1 level was detected in 121 (25.00%) cases, while the decline in cognitive functions reached 20–25 MMSE points.
In 306 (32.87%) patients with a more severe form of chronic cerebrovascular insufficiency and widespread distal cerebral atherosclerotic lesions, dementia at the CDR-1 level was detected in 163 (53.27%) cases, dementia at the CDR-2 level was detected in 125 (40.85%) cases, at the CDR-3 level in 18 (5.88%) cases, while the decline in cognitive functions was 11–25 MMSE points.
In 27 patients suffering from Binswanger disease (BD), dementia at the CDR-1 level was detected in 16 cases (59.26%), at the CDR-2 level in 7 cases (25.93%), and at the CDR-3 level in 4 cases (14.81%), while the decline in cognitive functions was 11–25 MMSE points.
In 62 patients (6.66%) suffering from vascular parkinsonism (VP), the absence of clear signs of dementia was detected in 30 cases (48.39%), dementia at the level (CDR-1) in 32 cases (51.61%), while the decline in cognitive functions was 20–27 MMSE points.
Laboratory tests:
Increased blood lipid levels were noted in 726 cases (77.98%).
Hypercoagulation phenomena were noted in 698 (74.97%) cases.
Cerebral SG:
Decreased blood flow in the cerebral hemispheres was noted in 931 (100%) cases.
Cerebral REG:
Decreased volumetric perfusion blood filling in the carotid system was noted in 931 (100%) cases.
Cerebral MUGA with digital image processing:
Atherosclerotic changes in the intracerebral distal arterial and capillary bed were detected in 931 (100%) cases (Table 2).
Atherosclerotic stenosis of intracerebral distal arterial branches and capillaries was detected in 931 (100%) cases (Fig. 3 A(1)) (Table 2).
Atherosclerotic occlusions of distal arterial branches and capillaries at the level of the gray cerebral matter were detected in 348 (37.38%) cases (Fig. 3 A(2)) (Table 2).
Decreased capillary blood flow at the level of the gray cerebral matter in 768 (82.49%) cases (Fig. 3 A(3)) (Table 2).
Multiple, disseminated arteriovenous shunts of small diameter within the gray matter of the brain were detected in 386 (41.46%) cases (Fig. 3 B(4)) (Table 2).
Subcortical, disseminated early flow of arterial blood into the venous bed, without the development of abnormal venous trunks and venous blood stasis, was detected in 245 (26.32%) cases (Fig. 3 C(5)), (Fig. 3 C(6)), (Table 2).
Subcortical atherosclerotic occlusions of the distal capillary branches of the white cerebral matter were noted in 89 (9.56%) cases (Table 2).
Subcortical disseminated and local decrease in capillary blood flow at the level of the cerebral white matter
- Subcortical disseminated decrease in capillary blood flow at the level of the white matter of the brain was detected in 89 (9.56%) cases (Fig. 3 D(3)), (Table 2).
- Subcortical, disseminated, multiple small-diameter arteriovenous shunts at the level of the white matter of the brain were detected in 27 (2.90%) cases (Fig. 3 D(4)), Fig. 3 E(4)), (Table 2).
- Subcortical, multiple, disseminated, early flow of arterial blood into the venous bed at the level of the white matter of the brain was detected in 27 (2.90%) cases (Table 2).
- Subcortical, single, local arteriovenous shunts of small diameter within the white matter of the brain in the area of the pons, thalamus, and basal ganglia were detected in 62 (6.66%) cases (Fig. 3 F(4)), (Table 2).
- Subcortical, local, early flow of arterial blood into the venous bed at the level of the white matter of the brain was detected in 62 (6.66%) cases (Fig. 3 F(5)), (Table 2).
- Increased looping of distal intracranial arterial branches was noted in 69 (7.41%) cases (Table 2).
- AD-specific reduction of the capillary bed in the temporal and frontoparietal regions of the brain was not detected in any case (Table 2).
- AD-specific multiple arteriovenous shunts in the basins of arterial branches, supplying the temporal and frontoparietal regions of the brain, were not detected in any case (Table 2).
- AD-specific local early discharge of arterial blood into the venous bed through shunts in the temporal and frontoparietal regions was not detected in any case (Table 2).
- AD-specific abnormally dilated lateral venous trunks at the level of the frontoparietal regions were not detected in any case (Table 2).
- AD-specific venous blood stasis at the border of the frontal and parietal regions was not detected in any case (Table 2).
FIGURE 3
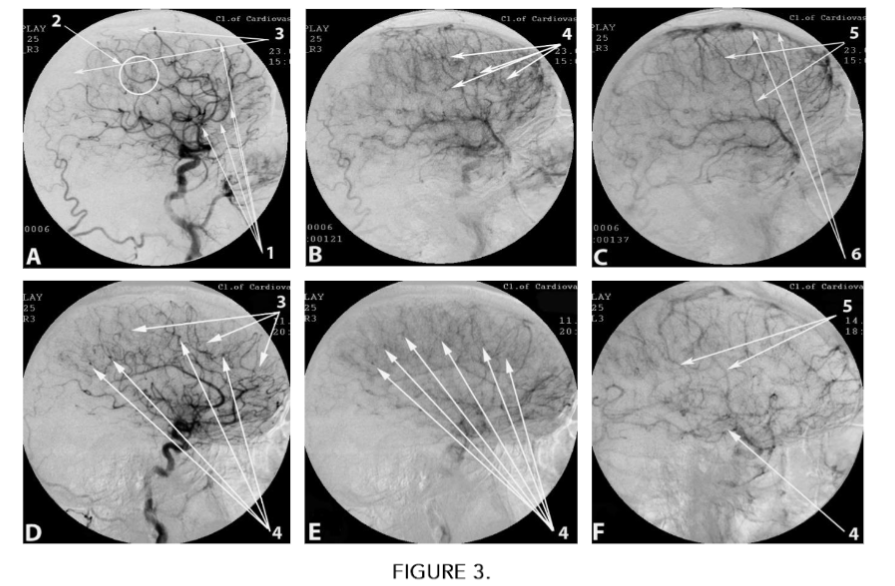
Cerebral MUGA of patients with distal cerebral atherosclerosis.
A. Arterial phase:
- Atherosclerotic changes in intracerebral branches.
- Atherosclerotic occlusions of distal arterial branches and capillaries at the level of the cerebral gray matter.
- Decreased capillary blood flow at the level of the cerebral gray matter.
B. Parenchymal stage:
4. Multiple small-diameter arteriovenous shunts.
C. Venous phase:
5. Disseminated early flow of arterial blood into the venous bed without the development of abnormal venous trunks.
6. No venous blood stasis.
D. (BD). Arterial phase:
3. Decreased capillary blood flow at the level of the white cerebral matter.
4. Multiple subcortical arteriovenous shunts of small diameter.
E. (BD). Parenchymal phase:
4. Multiple disseminated subcortical arteriovenous shunts of small diameter.
F. (VP). Parenchymal phase:
4. Single, local arteriovenous shunts of small diameter in the region of the pons, thalamus, and basal ganglia.
5. Disseminated early local flow of arterial blood into the venous bed without the development of abnormal venous trunks.
Discussion
In AD and distal cerebral atherosclerosis, the study of cerebral vascular disorders and CSVD have usually been conducted on postmortem materials, which does not provide a complete picture of the changes. At the same time, the comparison of characteristics of the changes that occur in AD and distal cerebral atherosclerosis has practically not been carried out⁵,¹⁸,²⁰,³³.
In AD, research was conducted to study cerebral vascular changes and CSVD on laboratory animals with an experimental model of the disease, which also does not allow a full interpretation of the data obtained for humans suffering from AD⁵,¹⁵,¹⁶.
In contrast to the above works, this study was conducted on the basis of clinical materials.
In this study, patients of Test Group 1 and Test Group 2 are similar in the severity of dementia and the severity of cognitive impairment. But vascular changes and CSVD in these groups of patients are completely different.
As in our earlier works¹³,³⁶,³⁷, this study showed that in AD the severity of dementia depends on the severity of atrophic changes in the cerebral temporal lobes. According to the digital morphometric scale “The Tomography Dementia Rating scale” (TDR), at the preclinical stage of AD (TDR-0), cerebral involutional changes are manifested in a decrease in the tissue mass of the temporal lobes by 4–8% of normal volume (Fig. 1(A)). In mild AD stage (TDR-1), temporal lobe atrophy is 9–18% (Fig. 1(B)), in moderate AD stage (TDR-2), temporal lobe atrophy is 19–32% (Fig. 1(C)), in severe AD stage (TDR-3), temporal lobe atrophy is 33–62% (Fig. 1(D)), (Table 1).
As in our earlier works¹³,²³,²⁶, this study shows that patients from Test Group 1 have virtually no signs of intracerebral atherosclerosis (Table 2). The existing cerebrovascular disorders and CSVD have their own clear specificity and are manifested in Dyscirculatory angiopathy of Alzheimer’s type (DAAT), which is an important factor in the development of AD (Table 2). In all patients from Test Group 1, the main manifestation of DAAT development is a decrease in the number (reduction) of capillaries, first in the temporal and then in the frontoparietal cerebral lobes with the formation of hypovascular zones in these areas (Fig. 2 A(1), Fig. 2 B(1)), (Table 2). These changes are not a consequence of stenosis or occlusion, they have their own specificity, and, unlike atherosclerosis, are hereditary (Table 2).
Reduction of capillaries, their thinning, and a decrease in further branching lead to disruption of cerebral hemodynamics, reduction in the distal inflow of arterial blood with the development of hypoxia specific to AD. The blood, flowing through intracerebral arterial branches, is unable to pass through the reduced number of arterioles and capillaries. As a result, in the temporal and frontoparietal regions, fairly large arteriovenous shunts develop, through which “excess” arterial blood is discharged into the venous bed (Fig. 2 A(2), Fig. 2 B(2), Fig. 2 C(2), Fig. 2 D(2)), (Table 2). The opening of arteriovenous shunts is a natural protective reaction of the body to the disruption of blood flow through the distal arteries and capillaries. As a result of the active flow of arterial blood into the venous bed, lateral, abnormally dilated venous trunks develop (Table 2). During MUGA, this is manifested in simultaneous contrasting of arteries and veins (Fig. 2 C(3), Fig. 2 D(3)). Active flow of arterial blood into the venous bed leads to venous overflow and stasis (Fig. 2 D(4)), (Table 2). These changes cause further increase in cerebrovascular dysfunction, which causes disturbances in metabolic processes in cerebral tissue. Arterial, capillary and venous changes in DAAT are equally determined at all stages of AD regardless of the severity of the disease, which indicates the congenital nature of the changes (Table 2).
Our data confirm the results of studies by other authors who studied microcirculatory changes in AD¹⁵,²⁰,²¹,²⁷,⁴⁰. Microcirculatory disorders in AD lead to destruction of synapses, degeneration and death of neurons, death of mitochondria in the cells of the smooth endoplasmic reticulum and Golgi apparatus, and general cerebral neurodegeneration. The combination of microvascular and tissue cerebral changes causes degeneration of the neurovascular unit (NVU)¹⁵,¹⁶,³⁸. A decrease in the capillary inflow of arterial blood and a simultaneous change in venous outflow causes a disruption in the process of natural metabolism of amyloid beta (Aβ). As a result, in cerebral tissues and vascular walls, there is a decrease in the natural physiological excretion of Aβ and an increase in its accumulation¹⁴. The combination of these processes further contributes to the disruption of cerebral microcirculation and leads to increased hypoxia, accompanied by dysfunction of the blood-brain barrier (BBB)²⁴,²⁵. Specific CSVD and Aβ accumulation in cerebral tissue cause the development and progression of AD.
The combination of DAAT with temporal lobe atrophy is the most important distinguishing feature of AD. DAAT, which is manifested in complex changes in cerebral hemodynamics, occurs only in AD and does not occur in other cerebrovascular lesions, including distal cerebral atherosclerosis.
Atherosclerosis of intracerebral vessels usually begins to develop in middle-aged and elderly people. The process occurs quite slowly, gradually causing a decrease in blood supply, the development of chronic cerebrovascular insufficiency and subsequent dementia³⁶,³⁷. Atherosclerosis can affect both main and distal intracerebral arterial branches and capillaries³,²⁷,³⁰,³³,⁴⁰.
In patients from Test Group 2, vascular changes and CSVD are of an atherosclerotic nature and are completely different from vascular changes and CSVD in patients from Test Group 1 (Table 2).
In patients from Test Group 2, atherosclerosis causes disseminated damage to small arterial branches and capillaries, manifested in stenosis and subsequent occlusions at the level of gray and white cerebral matter (Fig. 3 A(1), A(2)). This leads to depletion of the capillary bed in the corresponding areas, gradually developing hypoxia and ischemia (Fig. 3 A(3)), (Table 2).
In the early stages of development, these microcirculatory disorders occur without pronounced clinical symptoms, but trigger the mechanism of dementia development³,⁴,⁶,²⁸,⁴². Against the background of the atherosclerotic process, slowly developing hypoxia and ischemia disrupt the metabolism of adenosine triphosphate (ATP) in the mitochondria of neurons, which causes death of individual cells and their conglomerates³,⁶,²⁸,²⁹.
The spread of the atherosclerotic process leads to the development of multiple small-focal strokes in various parts of the white and gray matter of the brain. This course of distal cerebral atherosclerosis causes increasing neurodestruction and neurodegeneration, gradually leading to the development of dementia, cognitive impairment and worsening daily life. The severity of dementia and cognitive impairment depends on the prevalence of the process and the volume of affected cerebral tissue. Against the background of distal atherosclerotic lesions, arteriovenous shunts can form, but they are smaller in size and disseminated (Fig. 3 B(4)), (Table 2). Unlike AD, these arteriovenous shunts cause a minor discharge of arterial blood into the venous bed, which does not lead to the development of large venous trunks (Fig. 3 C(5)) and does not cause venous blood stasis (Fig. 3 C(6)), (Table 2).
In the case of the development of the atherosclerotic process at the subcortical level with localization of the lesion in one or another part of the white cerebral matter, patients develop Binswanger’s disease (BD) or vascular parkinsonism (VP), gradually leading to dementia³⁰,³¹.
In the early stages of the development of Binswanger’s disease (BD), subcortical foci of gliosis are small and disseminated, which may be accompanied by the development of mild dementia at the CDR-1 level. As the disease progresses, ischemic foci merge and, uniting into larger areas of demyelination, lead to the development of leukoaraiosis and more severe dementia at the CDR-2, CDR-3 level.
According to our data, because of the progression of atherosclerosis in Binswanger’s disease (BD), multiple subcortical occlusions of the capillary bed develop at the level of the white cerebral matter (Fig. 3 D(3)) (Table 2). Arteriovenous shunts are small and subcortical, disseminated (Fig. 3 D(4), Fig. 3 E(4)), (Table 2). Due to the insignificant flow of arterial blood into the venous bed, the development of pathological venous trunks and venous blood stagnation does not occur (Table 2).
In vascular parkinsonism (VP), the atherosclerotic process occurs in a similar manner, but more locally in the area of the thalamus, basal ganglia and pons. In these same areas, capillary occlusions develop, the capillary bed is depleted and single small arteriovenous shunts open (Fig. 3 F(4)) (Table 2). Due to the locality of the lesion, pathological changes in the venous bed do not occur (Fig. 3 F(5)) (Table 2). In VP, due to the local nature of the lesion, dementia is expressed to a lesser extent – within CDR-1. In Test Group 2, signs of Dyscirculatory angiopathy of Alzheimer’s type (DAAT) were not detected in any case, which indicates a completely different nature of cerebrovascular disorders and CSVD in patients with AD and with distal cerebral atherosclerosis.
Conclusions
In this study, patients with AD and patients with distal cerebral atherosclerosis are similar in the severity of dementia and the severity of cognitive impairment. All patients have decreased blood flow in the cerebral hemispheres and decreased volumetric perfusion blood filling in the carotid system. However, cerebral angioarchitectonics and CSVD in these groups of patients are completely different.
In patients with AD, regardless of the severity of dementia, Dyscirculatory angiopathy of Alzheimer’s type develops, caused by local reduction of capillaries in the temporal and frontoparietal regions, development of hypovascular zones in the same regions, development of large local arteriovenous shunts in the arterial basins supplying the temporal and frontoparietal regions, local early discharge of arterial blood through these shunts into the venous bed, leading to the development of abnormally dilated venous trunks and venous blood stagnation. At the same time, in patients suffering from AD, there are practically no atherosclerotic changes in intracerebral arteries, arterioles and capillaries. Dyscirculatory angiopathy of Alzheimer’s type is a cerebral blood supply disorder specific to AD, which is not observed in other cerebrovascular diseases, including distal cerebral atherosclerosis.
In patients with distal cerebral atherosclerosis, regardless of the severity of dementia, arterial changes and CSVD develop because of the spread of atherosclerotic lesions, leading to stenosis and subsequent occlusion of distal cerebral arteries, arterioles and capillaries. The process can occur at the cortical and subcortical level. Most often, these changes are disseminated. In this case, venous outflow disorders do not occur. Local subcortical lesions develop in vascular parkinsonism but are also atherosclerotic in nature.
Declaration of Conflicting Interests:
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The authors received no financial support for the research, authorship, and/or publication of this article.
References
1. 2024 Alzheimer’s disease facts and figures. Journal of Alzheimer’s & Dementia 2024; 20,5:3708-3821. https://doi.org/10.1002/alz.13809
2. World Health Organization. Dementia: Key facts. https://www.who.int/news-room/fact-sheets/detail/dementia
3. Gjulev NM, Pustozertsev VG, Gjulev SN. Cerebrovascular Diseases. Moscow BINOM, 2002.
4. Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 2010; 9, 7: 689–701. DOI: 10.1016/S1474-4422(10)70104-6
5. Cai Z, Wang C, He W, et al. Cerebral small vessel disease and Alzheimer’s disease. Clin Interv Aging. 2015; 23, 10: 1695-1704. https://doi.org/10.2147/CIA.S90871
6. Sabayan B, Goudarzi R, Ji Y, Borhani‐Haghighi A et al. Intracranial Atherosclerosis Disease Associated With Cognitive Impairment and Dementia: Systematic Review and Meta‐Analysis. JAHA, 2023; 12, 22: 1-11.
https://doi.org/10.1161/JAHA.123.032506
7. Grammas P, Martinez J, Sanchez A, et al. A new paradigm for the treatment of Alzheimer’s disease: targeting vascular activation. J Alzheimers Dis 2014; 40, 3: 619-630. https://doi.org/10.3233/JAD-2014-132057
8. Alzheimer’s Association. 2019 Alzheimer’s Disease Facts and Figures. Special report: Alzheimer’s detection in the primary care setting — connecting patients with physicians. Alzheimer’s & Dementia 2019; 15, 3: 321-387.
https://doi.org/10.1016/j.jalz.2019.01.010
9. Mormino EC, Papp KV, Rentz DM, et al. Early and late change on the preclinical Alzheimer’s cognitive composite in clinically normal older individuals with elevated amyloid-β. J Alzheimer’s & Dementia February 27, 2017; 1-9, http://dx.doi.org/10.1016/j.jalz.2017.01.018
10. Maksimovich IV and Polyaev Yu A The importance of early diagnosis of dyscircular angiopathy of Alzheimer’s type in the study of heredity of Alzheimer’s disease. Journal of Alzheimer’s & Dementia, 2010; 6, e43.
https://doi.org/10.1016/j.jalz.2010.08.133
11. Maksimovich IV. Dyscirculatory Angiopathy of Alzheimer’s Type. Journal of Behavioral and Brain Science. 2011; 1, 2: 57-68. doi: 10.4236/jbbs.2011.12008
12. Maksimovich IV. Certain new aspects of etiology and pathogenesis of Alzheimer’s disease. Advances in Alzheimer’s Disease, 2012; 1, 3:68-76. doi: 10.4236/aad.2012.13009
13. Maksimovich IV. Cerebrovascular Changes and Cerebral Atrophy in the Development of Dementia during Alzheimer’s Disease. Medical Research Archives. 2023; 11 (5): 1-10. https://doi.org/10.18103/mra.v11i5.3869
14. Zlokovic BV. Neurodegeneration and the neurovascular unit. Nat Med 2010; 16, 12 1370-1371. doi: 10.1038/nm1210-1370.
15. Iadecola C. The overlap between neurodegenerative and vascular factors in the pathogenesis of dementia. Acta Neuropathol 2010; 120, 3 287-396. doi: 10.1007/s00401-010-0718-6.
16. Zlokovic BV Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nature Reviews Neuroscience. 2011; 3 723-738. https://doi.org/10.1038/nrn3114
17. Kalaria R Small vessel disease and Alzheimer’s dementia: Pathological considerations. Cerebrovascular Diseases. 2002; 13: 48-52. doi: 10.1159/000049150.
18. Baloiannis SJ and Baloiannis IS. The vascular factor in Alzheimer’s disease: A study in Golgi technique and electron microscopy. Journal of the Neurological Sciences 2012; 322: 117-121. doi: 10.1016/j.jns.2012.07.010
19. Kimbrough IF, Robel S, Roberson E D, Sontheimer H. Vascular amyloidosis impairs the gliovascular unit in a mouse model of Alzheimer’s disease. Brain 2015; 138, Pt 12 3716-3733. https://academic.oup.com/brain/article/138/12/3716/416119
20. Baloyannis SJ. Brain capillaries in Alzheimer’s disease. Hell J Nucl Med 2015; 18, Suppl 1 152.
21. De la Torre JC Cerebral Perfusion Enhancing Interventions: A New Strategy for the Prevention of Alzheimer Dementia. Brain Pathology 2016; 26, 5: 618–631. https://doi.org/10.1111/bpa.12405
22. Morel F. An apparently dyshoric and topical angiopathy. Monatsschr Psychiat Neurol 1950; 120, 5-6 352-357.
23. Maksimovich IV. Study of the Impact of Transcatheter Intracerebral Laser Photobiomodulation Therapy Treatment on Patients with Alzheimer’s Disease and Binswanger’s Disease. Medical Research Archives. 2022; 10, 12: 1-13. https://doi.org/10.18103/mra.v10i12.3420
24. Bell RD and Zlokovic BV. Neurovascular mechanisms and blood-brain barrier disorder in Alzheimer’s disease. Acta Neuropathologica. 2009; 118: 103-113. https://link.springer.com/article/10.1007/s00401-009-0522-3
25. Montagne A, Barnes SR, Sweeney MD, Halliday MR, Sagare AP. et all. Blood-brain barrier breakdown in the aging human hippocampus. Neuron. 2015; 85, 2: 296-302. doi: 10.1016/j.neuron.2014.12.032.
26. Maksimovich IV. Transcatheter intracerebral photobiomodulation in degenerative brain disorders: clinical studies (Part 1). In Photobiomodulation in the Brain, Edited by Michael R. Hamblin, Ying-Ying Huang. Academic Press is an imprint of Elsevier, London, 2019; p-p. 515-528. https://doi.org/10.1016/B978-0-12-815305-5.00038-5
27. Brown WR, Thore CR Review: cerebral microvascular pathology in ageing and neurodegeneration. Neuropathol Appl Neurobiol. 2011; 37, 1: 56-74. https://doi.org/10.1111/j.1365-2990.2010.01139.x
28. Maksimovich IV. Transcatheter intracerebral photobiomodulation in ischemic brain disorders: clinical studies (Part 2). Photobiomodulation in the Brain. Edited by Michael R. Hamblin, Ying-Ying Huang, Academic Press is an imprint of Elsevier, London, 2019; 529-544. https://doi.org/10.1016/B978-0-12-815305-5.00039-7.
29. Pasi M. Cordonnier Ch. Clinical Relevance of Cerebral Small Vessel Diseases. Stroke. 2020; 51, 1: 47-53.
https://doi.org/10.1161/STROKEAHA.119.024148
30. Tomimoto H. Subcortical vascular dementia. Neurosci Res. 2011; 71, 3 193-199.
https://doi.org/10.1016/j.neures.2011.07.1820
31. Maksimovich IV. Intracerebral Transcatheter Laser PBMT in the Treatment of Binswanger’s Disease and Vascular Parkinsonism: Research and Clinical Experience. Photobiomodul Photomed and Laser Surg. 2019; 37, 10: 606-614. https://doi.org/10.1089/photob.2019.4649
32. Akiguchi I, Budka H, Shirakashi Y, Woehrer A, et all. MRI features of Binswanger’s disease predict prognosis and associated pathology. Ann Clin Transl Neurol. 2014; 1, 10: 813-821. https://doi.org/10.1002/acn3.123
33. Grodstein F, Leurgans SE, Capuano AW, Schneider JA, Bennett DA. Trends in Postmortem Neurodegenerative and Cerebrovascular Neuropathologies Over 25 Years. JAMA Neurol. 2023; 80, 4: 370-376.
doi: 10.1001/jamaneurol.2022.5416
34. Morris JC. The Clinical Dementia Rating (CDR): Current Version and Scoring Rules. Neurology. 1993; 11 (43): 2412-2414. https://doi.org/10.1212/WNL.43.11.2412
35. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975; 12, 3: 189-198. https://doi.org/10.1016/0022-3956(75)90026-6
36. Maksimovich IV, and Gotman LN. Method of complex radiation diagnostics at preclinical and clinical stages of Alzheimer’s disease. Russian Patent, No. 2315559. 2006.
37. Maksimovich IV. The tomography dementia rating scale (TDR) – The rating scale of Alzheimer’s disease stages. Health. 2012; 4, 9 A: 712-719. doi: 10.4236/health.2012.429111
38. Nelson AR, Sweeney MD, Sagare AP, Zlokovic BV. Neurovascular dysfunction and neurodegeneration in dementia and Alzheimer’s disease. Biochim Biophys Acta. 2016; 1862, 5: 887-900. https://doi.org/10.1016/j.bbadis.2015.12.016
39. Henry-Feugeas MC. Alzheimer’s disease in late-life dementia: a minor toxic consequence of devastating cerebrovascular dysfunction. Med Hypotheses 2008; 70, 4:866–875. https://doi.org/10.1016/j.mehy.2007.07.027
40. Liu Y, Jun H, Becker A, Wallick C, Mattke S. Detection rates of mild cognitive impairment in primary care for the United States Medicare population. J Prev Alzheimers Dis 2024; 11, 1: 7-12. DOI: 10.14283/jpad.2023.131
41. Chen Y, He Y, Han J, Wei W et al. Blood-brain barrier dysfunction and Alzheimer’s disease: associations, pathogenic mechanisms, and therapeutic potential. Front Aging Neurosci. 2023; 13, 15:1258640. https://doi.org/10.3389/fnagi.2023.1258640
42. Maksimovich IV. Cerebral Angiogenesis and Neurogenesis in The Treatment of Ischemic Stroke in Elderly and Geriatric Patients. Gerontology & Geriatric Studies. 2024; 9, 2: 745-755.
DOI: 10.31031/GGS.2024.09.000706
Most read articles by the same author(s)
- Ivan V. Maksimovich, Study of the Impact of Transcatheter Intracerebral Laser Photobiomodulation Therapy Treatment on Patients with Alzheimer’s Disease and Binswanger’s Disease , Medical Research Archives: Vol 10 No 12 (2022): December issue, Vol.10 Issue 12
- Ivan V. Maksimovich, Cerebrovascular Changes and Cerebral Atrophy in the Development of Dementia during Alzheimer’s Disease , Medical Research Archives: Vol 11 No 5 (2023): May Issue, Vol.11, Issue 5
- Ivan V. Maksimovich, Various Methods of Laser Photobiomodulation Therapy for Alzheimer’s Disease , Medical Research Archives: Vol 11 No 9 (2023): September Issue, Vol.11, Issue 9