





Clinicians’ Attitudes Toward Physical Activity in CAMHS
Clinicians’ Knowledge, Attitudes, and Practices Regarding Physical Activity Interventions in Irish Child and Adolescent Mental Health Services (CAMHS)
David Killeen1, Sonita Sharma2, Maeve Haran3, Katie Haugh3, Fiona McNicholas2,4,5
- Linn Dara Child and Adolescent Mental Health Services, Dublin, Ireland.
- Lucena Child and Adolescent Mental Health Services, Dublin, Ireland.
- Dublin North City and County Child and Adolescent Mental Health Services, Dublin, Ireland.
- Department of Child and Adolescent Psychiatry, School of Medicine, University College Dublin, Dublin, Ireland.
- Department of Paediatric Liaison Psychiatry, Children’s Health Ireland (CHI), Dublin, Ireland.
OPEN ACCESS
PUBLISHED 31 January 2026
CITATION Killeen, D., Sharma, S., et al., 2026. Clinicians’ Knowledge, Attitudes, and Practices Regarding Physical Activity Interventions in Irish Child and Adolescent Mental Health Services (CAMHS). Medical Research Archives, [online] 14(1). https://doi.org/10.18103/mra.v14i1.7136
Copyright © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v14i1.7136
ISSN 2375-1924
ABSTRACT
Objectives: Physical Activity (PA) offers significant mental health benefits for young people, yet its integration into Child and Adolescent Mental Health Services (CAMHS) remains limited. This study explored Irish CAMHS clinicians’ knowledge, attitudes, and practices regarding Physical Activity Interventions (PAIs).
Methods: A cross-sectional online survey was distributed nationally to clinicians working in CAMHS across Ireland, including consultants, non-consultant hospital doctors (NCHDs), nurses, psychologists, and allied health professionals. The study-specific questionnaire assessed three domains—knowledge of Physical Activity guidelines, perceived evidence, and clinical practice—alongside personal attitudes toward Physical Activity. Non-parametric analyses were conducted to examine inter-group differences and associations between domains.
Results: While 84% agreed that incorporating Physical Activity should be a Child and Adolescent Mental Health Services responsibility, 65% reported that no team member currently delivered Physical Activity Interventions. Knowledge of guideline-recommended Physical Activity levels was limited (mean score = 1.2/3), and factual knowledge showed no association with practice. Perceived evidence was strongest for depression and Attention Deficit Hyperactivity Disorder and correlated positively with frequency of Physical Activity Interventions recommendations (r = .48, p < .01). Practice varied significantly by professional role (p = .008), with Non-Consultant Hospital Doctors recommending Physical Activity Interventions less often than consultants or nurses. Personal attitudes were uniformly positive across roles (M = 4.1/5).
Conclusions: Irish Child and Adolescent Mental Health Services clinicians endorse the value of physical activity but demonstrate variable implementation and limited guideline knowledge. Perceived strength of evidence for Physical Activity Interventions rather than factual knowledge drives clinical behaviour. Enhancing clinician confidence in the evidence base and embedding structured Physical Activity training within Child and Adolescent Mental Health Services could strengthen integration of Physical Activity Interventions into youth mental healthcare.
Keywords: Child and adolescent psychiatry; physical activity; clinician attitudes; implementation; CAMHS; mental health promotion; Ireland.
INTRODUCTION
Regular physical activity is essential for maintaining and enhancing health across all age groups. It contributes to improved cardiovascular and muscular fitness, bone and cardiometabolic health, and supports mental well-being. Moreover, it plays a significant role in reducing the risk of non-communicable diseases such as cardiovascular diseases, type 2 diabetes, and certain cancers. Recognizing its importance, the World Health Organization has endorsed a Global Action Plan on Physical Activity aiming to reduce physical inactivity worldwide.
In 2023, approximately 20.3% of children aged 8 to 16 years in England were identified as having a probable mental disorder, reflecting a continued increase from previous years. Comparable data for Ireland are limited, but smaller-scale studies and clinical reports suggest similar high rates with increased post-COVID CAMHS service demand and emotional difficulties among youth. Using the WHO-5 Well-Being Index, 36% of Irish children were classified as having low mood or being at risk of depression—26% of boys and 46% of girls.
Although estimates vary depending on methodology, a recent systematic review of Irish studies reported current mental health disorder rates of up to 15.5%, with lifetime prevalence ranging from 19.9% to 31.2%. Alongside these trends, recent studies have highlighted a concerning increase in sedentary behaviour, particularly during adolescence. Globally, 81% of adolescents fail to meet the World Health Organization’s recommended physical activity levels, often spending between 4 and 12 hours per day in sedentary activities.
Accelerometer-based assessments show that average sedentary time increases from around 5 hours per day in childhood to 7.5 hours in adolescence. Irish national guidelines recommend that children and adolescents engage in at least 60 minutes of moderate-to-vigorous physical activity daily and include muscle- and bone-strengthening activities at least three times per week.
In Ireland, the 2022 Health Behaviour in School-aged Children (HBSC) study found that only 41% of boys and 28% of girls met the recommended threshold of engaging in vigorous physical activity at least four times per week, while 8% of boys and 11% of girls reported participating in vigorous exercise less than once per week. Physical activity declined significantly with age, and children from lower social class groups were consistently less likely to meet activity recommendations. These patterns of increasing inactivity and widening socioeconomic disparities further compound mental health risks and highlight the need for targeted, accessible interventions.
In parallel, childhood obesity remains a pressing public health issue. In England, 22.1% of children aged 10 to 11 years were classified as obese in the 2023/24 school year, with nearly one in three affected in the most deprived areas. Irish children are similarly affected: the Childhood Obesity Surveillance Initiative (COSI) 2022–23 reported that almost a fifth (17.7%) of primary-school children were living with overweight or obesity, including 4.1% classified as obese.
Physical Activity and Mental Health:
Physical activity interventions show promising effects on mental health in young people. Meta-analyses demonstrate reductions in depression and anxiety symptoms. Exercise improves mood, self-esteem, and cognitive function. Both aerobic and strength-based activities are effective in improving mental health outcomes. School- and community-based programs consistently yield benefits, potentially through neurobiological mechanisms and enhanced social interaction.
Despite this strong evidence base, physical activity interventions remain underused within Child and Adolescent Mental Health Services (CAMHS) settings. This gap is especially notable in Ireland, where formal integration of physical activity into CAMHS remains largely absent and where standardized national guidance in this area is currently lacking.
Barriers to Implementation:
Several barriers hinder the integration of physical activity interventions into CAMHS. Structural challenges such as limited resources, lack of trained staff, and time constraints are commonly cited. Clinicians often prioritize pharmacological and psychological treatments, influenced by traditional care models and high service demands. Successful implementation depends heavily on clinician engagement and support.
International surveys conducted in Australia and the UK report mixed levels of clinician enthusiasm and emphasize the need for additional training and organizational support. However, little is known about these issues in the Irish context, where no large-scale investigations have been conducted to date. Understanding Irish CAMHS clinicians’ knowledge, attitudes, perceived barriers, and support needs is essential to developing feasible and effective strategies for integrating physical activity into services.
Study Aim:
Given the sparsity of research within the Irish CAMHS setting, there is a clear need to better understand clinician perspectives. Therefore, the objective of this study was to examine Irish clinicians’ knowledge, attitudes, and practice regarding the use of physical activity interventions in CAMHS services.
Study Design:
A cross-sectional survey design was employed to assess the knowledge, attitudes, and practices (KAP) of clinicians regarding physical activity interventions (PAIs) in the treatment of mental health disorders among service users in Child and Adolescent Mental Health Services (CAMHS) in Ireland. The study used a study-specific questionnaire informed by existing literature and tailored to the Irish clinical context.
Study Population and Setting:
The study population comprised clinicians working within Child and Adolescent Mental Health Services (CAMHS) in Ireland. Eligible participants included consultant psychiatrists, non-consultant hospital doctors (NCHDs), nurses, psychologists, and allied health professionals involved in the assessment and treatment of children and adolescents with mental health difficulties. Clinicians working in both public and private CAMHS settings were eligible to participate.
The study was conducted within the context of Irish CAMHS, which provides specialist, multidisciplinary mental health care to children and adolescents with moderate to severe mental health disorders across community and inpatient settings. Recruitment focused primarily on clinicians working in public CAMHS services. In addition to national recruitment through the College of Psychiatrists of Ireland, two large CAMHS service clusters were also recruited to maximise clinician representation.
Study Instrument:
A study-specific questionnaire was developed for this research, informed by existing literature examining physical activity and mental health outcomes in young people, clinician attitudes toward lifestyle interventions, and barriers to implementation within mental health services. The questionnaire was reviewed by clinicians with experience in CAMHS and physical activity research to ensure clarity, relevance, and face validity prior to dissemination.
The questionnaire consisted of 18 items organised into three domains: knowledge, practice, and attitudes toward physical activity interventions. The knowledge domain (Items 1–7) assessed clinicians’ familiarity with national physical activity guidelines and physical health considerations relevant to young people with mental disorders. These items included multiple-choice questions examining recommended daily levels of moderate-to-vigorous physical activity for children and adolescents, recommended frequency of muscle- and bone-strengthening activities, and awareness of national epidemiological data regarding the proportion of children meeting recommended physical activity levels.
The practice domain (Items 8–15) examined clinicians’ use of physical activity interventions in clinical practice. Items assessed perceived responsibility of CAMHS for incorporating physical activity into treatment, frequency of recommending physical activity interventions as adjunctive treatments across diagnostic groups (psychotic disorders, anxiety disorders, depressive disorders, and attention-deficit/hyperactivity disorder), frequency of enquiring about patients’ physical activity levels, provision of guidance regarding recommended activity levels, and whether physical activity interventions were delivered within participants’ CAMHS services.
The attitudes domain (Items 16–18) explored clinicians’ personal and professional perspectives on physical activity. These items assessed incorporation of physical activity into clinicians’ own daily routines, perceived importance of exercise for maintaining personal mental wellbeing, and perceived value of physical activity interventions in counteracting metabolic side effects of antipsychotic medication in community CAMHS settings.
Knowledge items were assessed using fixed-response multiple-choice questions, while practice and attitude items were measured using five-point Likert scales. Higher scores reflected greater knowledge, more frequent clinical use of physical activity interventions, or more positive attitudes, as appropriate. The full questionnaire is available from the authors on request.
Recruitment and Data Collection Procedure
The survey was administered using a secure online platform and remained open for a predefined data collection period. Prior to accessing the survey, participants were provided with an information page outlining the aims of the study, the voluntary nature of participation, and data protection procedures. Consent was implied through completion of the questionnaire, and no identifying information was collected.
Participants were recruited primarily through the College of Psychiatrists of Ireland, with email invitations distributed to active members of the Faculty of Child and Adolescent Psychiatry, including both trainees and consultants. In addition, a convenience sampling approach was employed, with clinicians working within CAMHS teams at the Linn Dara Clinical Directorate and the Lucena Clinic also invited to participate via email. Survey links were distributed electronically through these channels, and responses were collected anonymously. Based on the number of clinicians invited through these channels, the approximate response rate was 19%.
Ethical Considerations:
Ethical approval for the study was obtained from the University College Dublin Human Research Ethics Committee – Life Sciences (HREC-LS) under protocol number LS-LR-24-200-McNicholas. Participation was voluntary, information was provided about the study and completion of the survey implied informed consent. No identifiable personal information was collected.
Statistical Analysis:
Statistical analysis was conducted using IBM SPSS 29, with overall constructs formed by averaging individual item scores within each domain. Normality testing revealed non-normal distributions across variables, necessitating the use of non-parametric statistical procedures. Kruskal-Wallis tests were employed to examine differences between professional roles, while Spearman rank correlations were calculated to assess relationships between knowledge, perceived evidence, practice, and attitudes. For the purpose of inferential statistics, psychologists and speech and language therapists were considered along with the “Others group” due to very low sample sizes (N=2 each).
Results:
The study recruited 106 CAMHS clinicians across Ireland, with consultants representing the largest professional group (42.5%, n=45), followed by non-consultant hospital doctors (NCHDs) at 33.0% (n=35). Nursing staff comprised 15.1% (n=16) of respondents, while other disciplines including psychologists, speech and language therapists, and other professionals made up the remaining 8.5%. The overwhelming majority of participants (95.3%, n=101) worked in public sector services, with only 4.7% (n=5) in private practice.
Regarding training status, 61.3% (n=65) of respondents had completed their professional training, while 30.2% (n=32) were still in training programs. A smaller proportion (8.5%, n=9) worked as standalone practitioners or locums. Community CAMHS represented the primary workplace setting for most participants (65.1%, n=69), followed by inpatient CAMHS (13.2%, n=14) and specialist CAMHS services such as eating disorder or ADHD clinics (10.4%, n=11). Liaison CAMHS accounted for 8.5% (n=9) of respondents.
The majority of clinicians (84.0%, n=89) believed that incorporating physical activity into service users’ treatment should be a CAMHS responsibility. However, among the 16.0% (n=17) who disagreed with this position, respondents indicated that parents, schools, and general practitioners should share or assume this responsibility instead. Despite this general agreement on CAMHS responsibility, actual delivery of physical activity interventions remained limited. Nearly two-thirds of participants (65.1%, n=69) reported that no team member in their clinic was delivering physical activity interventions for mental illness treatment. Only 13.2% (n=14) indicated regular delivery of such interventions, while 12.3% (n=13) reported ad hoc provision. A notable 9.4% (n=10) were uncertain about whether their team delivered any physical activity interventions.
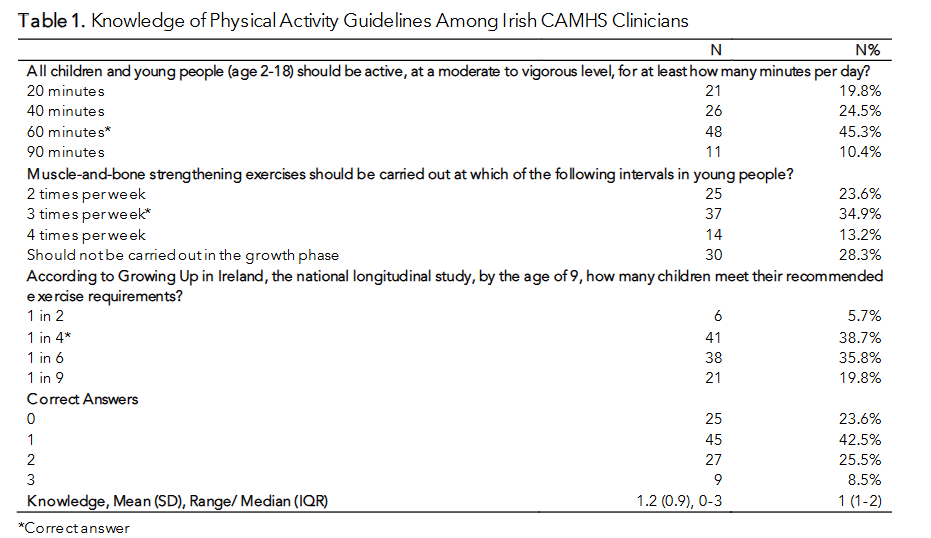
Knowledge of established physical activity guidelines among CAMHS clinicians showed considerable variation across the three assessed domains. For daily moderate-to-vigorous activity requirements, less than half of respondents (45.3%, n=48) correctly identified the 60-minute guideline, while 24.5% (n=26) underestimated the requirement at 40 minutes and 19.8% (n=21) selected 20 minutes. A smaller proportion (10.4%, n=11) overestimated the requirement at 90 minutes.
Understanding of muscle-and-bone strengthening exercise frequency was similarly limited, with only 34.9% (n=37) correctly identifying the three-times-per-week recommendation. Nearly a quarter of respondents (23.6%, n=25) believed twice weekly was sufficient, while 13.2% (n=14) thought four times weekly was necessary. More than a quarter (28.3%:n=30) incorrectly believed strengthening exercises should not be performed during the growth phase, representing a significant knowledge gap that could impact clinical recommendations.
Knowledge of national epidemiological data from the Growing Up in Ireland study, 2019, showed the strongest performance, with 38.7% (n=41) correctly identifying that only one in four children meet recommended exercise requirements by age nine. However, 35.8% (n=38) underestimated this figure at one in six, while smaller proportions selected one in two (5.7%, n=6) or one in nine (19.8%, n=21).
Nearly a quarter of clinicians (23.6%, n=25) answered none of the questions correctly, while 42.5% (n=45) achieved only one. A further quarter (25.5%, n=27) answered two correctly, and just 8.5% (n=9) achieved full marks. The mean knowledge score was 1.2 (SD = 0.9; median = 1, IQR = 1–2), indicating generally limited awareness of physical activity guidelines relevant to clinical practice.
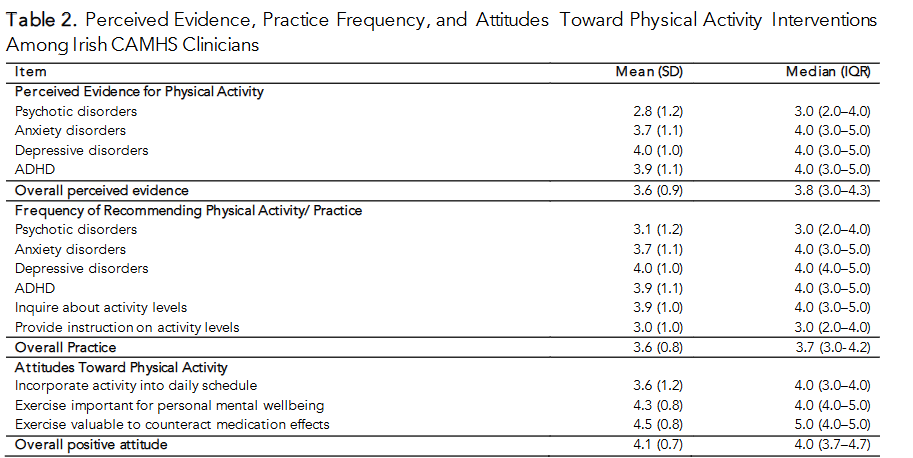
Clinicians’ perceptions of the evidence base for PAI (rated on a 5-point scale: 1=no evidence to 5=strong evidence) varied considerably across mental health conditions. Evidence perception was lowest for psychotic disorders (M=2.8, SD=1.2), indicating clinicians viewed the evidence base as limited, with responses clustering around “reasonable evidence” (median=3.0). In contrast, perceived evidence was strongest for depressive disorders (M=4.0, SD=1.0), suggesting clinicians recognized good empirical support for physical activity interventions in this population. ADHD (M=3.9, SD=1.1) and anxiety disorders (M=3.7, SD=1.1) received similarly high evidence ratings, both with medians of 4.0. The overall perceived evidence score (M=3.6, SD=0.9) indicated that clinicians generally viewed the evidence base as between reasonable and good.
Practice patterns (rated on a 5-point scale: 1=never to 5=always) closely mirrored perceived evidence ratings across conditions. Clinicians reported recommending physical activity interventions most frequently for depressive disorders (M=4.0, SD=1.0), with a median of 4.0 indicating “often” to “always” recommendations. ADHD (M=3.9, SD=1.1) and anxiety disorders (M=3.7, SD=1.1) showed similar recommendation frequencies. Psychotic disorders again received the lowest recommendation frequency (M=3.1, SD=1.2), consistent with lower perceived evidence.
Clinicians frequently inquired about patients’ activity levels (M=3.9, SD=1.0) but were less likely to provide specific instruction on activity levels (M=3.0, SD=1.0), indicating a gap between assessment and intervention guidance. The overall practice score (M=3.6, SD=0.8) suggested moderate to frequent use of physical activity recommendations.
Personal attitudes toward physical activity (rated on a 5-point scale: 1=strongly disagree to 5=strongly agree) were notably positive across all domains. Clinicians showed strongest agreement that exercise interventions would be valuable for counteracting metabolic side effects of antipsychotic medication (M=4.5, SD=0.8), with a median of 5.0 indicating strong endorsement. They also strongly agreed that exercise was important for their own personal mental wellbeing (M=4.3, SD=0.8). Personal incorporation of activity into daily schedules received more moderate ratings (M=3.6, SD=1.2), suggesting a gap between recognizing benefits and personal implementation. The overall positive attitude score (M=4.1, SD=0.7) demonstrated strong professional endorsement of physical activity’s therapeutic value.
Comparison between professional groups:
(I) KNOWLEDGE AND PERCEIVED EVIDENCE
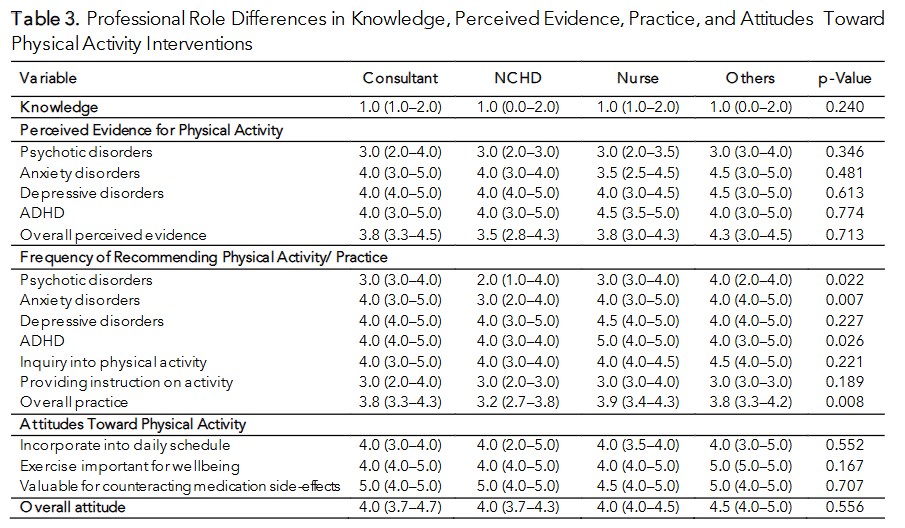
No significant differences emerged between professional groups in knowledge of physical activity guidelines (p=0.240), with all groups showing similarly limited understanding (median=1.0 across all roles). Perceived evidence for physical activity interventions also showed no significant variation across professional roles for any mental health condition. All groups demonstrated lowest confidence in evidence for psychotic disorders (median=3.0) and highest confidence for depressive disorders and ADHD (median=4.0-4.5). The overall perceived evidence scores remained consistent across roles (p=0.713), suggesting uniform awareness of the evidence base regardless of professional background.
(II) PRACTICE PATTERNS SHOW SIGNIFICANT PROFESSIONAL DIFFERENCES
For psychotic disorders, consultants and nurses reported more frequent recommendations (median=3.0) compared to NCHDs (median=2.0, p=0.022). The most pronounced difference appeared in anxiety disorder recommendations (p=0.007), where consultants, nurses, and other professionals frequently recommended physical activity (median=4.0), while NCHDs showed lower recommendation rates (median=3.0). ADHD treatment recommendations also varied significantly (p=0.026), with nurses showing the highest frequency (median=5.0) compared to other groups (median=4.0). The overall practice score demonstrated significant professional differences (p=0.008), with NCHDs showing lower overall recommendation of physical activity (median=3.2) compared to consultants (median=3.8) and nurses (median=3.9).
(III) ATTITUDES REMAIN CONSISTENT ACROSS ROLES
Despite practice differences, attitudes toward physical activity showed remarkable consistency across professional groups. All roles demonstrated strong positive attitudes, with no significant differences in personal incorporation of activity (p=0.552), recognition of exercise importance for wellbeing (p=0.167), or valuation of exercise for counteracting medication effects (p=0.707). These findings suggest that while knowledge and attitudes are consistent across CAMHS professional roles, significant practice gaps exist, particularly among NCHDs who demonstrate lower recommendation of physical activity despite similar evidence perception and positive attitudes.
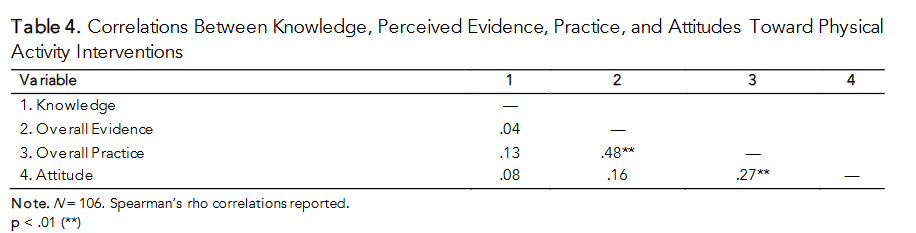
The correlation analysis revealed that knowledge of physical activity guidelines operates independently from other domains, showing weak and non-significant relationships with perceived evidence, practice, and attitudes. This suggests that factual knowledge alone does not drive clinical behaviour or professional perspectives regarding physical activity interventions.
The strongest relationship emerged between perceived evidence and practice (r=.48, p<.01), indicating that clinicians who view the evidence base as stronger are significantly more likely to recommend physical activity interventions in their clinical work.
Attitudes toward physical activity showed a moderate positive correlation with practice (r=.27, p<.01), suggesting that clinicians with more favourable personal views of physical activity are more likely to incorporate these interventions into patient care.
Relationship Between Knowledge of Childhood Exercise Compliance and Clinical Practice
The correlation analysis revealed no significant relationship between clinicians’ knowledge of exercise recommendations for 9-year-olds and their overall clinical practice scores (r=.02, p>.05). This extremely weak correlation indicates that knowing the correct statistic about how many children meet exercise requirements has virtually no impact on how frequently clinicians recommend physical activity interventions in their practice.
Personal attitudes about exercise and beliefs regarding metabolic side effects
The correlation analysis with separated attitude constructs revealed distinct patterns between personal attitudes and professional beliefs about exercise interventions. Knowledge remained weakly correlated with all other variables, showing no significant relationships with overall evidence (r=.04), practice (r=.13), metabolic side effects beliefs (r=-.06), or personal attitudes (r=.11). This confirms the persistent knowledge-practice gap identified throughout the study.
Overall evidence showed the strongest correlation with practice (r=.48, p<.01), reinforcing that clinicians who perceive stronger evidence are more likely to recommend physical activity interventions. Evidence perception also correlated significantly with beliefs about exercise countering metabolic side effects (r=.32, p<.01).
Practice patterns correlated moderately with both attitude constructs, showing significant relationships with personal attitudes (r=.23, p<.05) and beliefs about metabolic benefits (r=.19, p<.05). The two attitude constructs themselves were moderately correlated (r=.30, p<.01), indicating that clinicians with positive personal exercise attitudes also tend to value exercise for counteracting medication side effects, though these represent distinct constructs.
Alignment of perceived evidence for interventions with established evidence base.
Utilising the scoping review carried out by Haran et al, 2024, clinicians assigned a level of evidence rating for the listed conditions as follows, in order to evaluate how the views of clinicians surveys aligned: Psychosis 2.5/5, Depression 4/5, Anxiety 3/5, ADHD 3.5/5.
The analysis compared clinicians’ perceptions of evidence strength against established evidence ratings for physical activity interventions across mental health disorders. For psychotic disorders, where the established evidence level is 2.5/5, clinicians’ perceptions closely aligned with this benchmark across all professional roles. Consultants (M=2.9, SD=1.2), NCHDs (M=2.5, SD=1.1), nurses (M=3.1, SD=1.2), and other professionals (M=3.2, SD=1.2) all demonstrated accurate awareness of the limited evidence base, with NCHDs showing the most precise alignment to the established rating.
Depression showed strong concordance between perceived and established evidence levels (4/5), with all professional groups correctly rating evidence strength appropriately high. Consultants (M=4.1, SD=1.0), NCHDs (M=4.0, SD=1.0), nurses (M=3.9, SD=0.8), and others (M=4.0, SD=1.2) all clustered around the established benchmark, indicating accurate recognition of the evidence base for physical activity interventions in treating childhood depression.
However, clinicians consistently overrated the evidence strength for both anxiety disorders and ADHD compared to established levels. For anxiety disorders (established level 3/5), all groups showed inflated perceptions, with means ranging from 3.5 to 4.0 across roles. Similarly, for ADHD (established level 3.5/5), clinicians rated evidence strength higher than warranted, with means between 3.8 and 4.1. No significant differences emerged between professional roles for any disorder (all p>0.05), indicating that evidence overestimation for anxiety and ADHD occurs consistently across the CAMHS workforce regardless of training background or clinical experience.
Characteristics of Clinicians Delivering Physical Activity Interventions
The analysis examined whether the 13% of clinicians whose teams delivered physical activity interventions (regularly) possessed unique characteristics compared to those without such services. No significant differences emerged across any measured domain.
Knowledge scores remained consistently low across all groups (median=1.0), with no significant differences between those offering interventions and those who did not (p=0.511). This finding indicates that teams delivering physical activity interventions do not possess better understanding of established guidelines compared to teams without such services. Similarly, overall evidence perception showed no meaningful variation (p=0.842), with all groups demonstrating moderate confidence in the evidence base regardless of their team’s intervention delivery status.
Practice patterns and attitudes also failed to distinguish between groups. Overall practice scores were remarkably similar across intervention delivery categories (p=0.435). Personal attitudes toward exercise (p=0.184) and beliefs about exercise value in counteracting metabolic side effects (p=0.961) showed no significant differences, indicating that positive individual attitudes do not necessarily translate into team-level service provision.
Discussion:
This study provides the first national examination of clinicians’ knowledge, attitudes, and practice regarding physical activity interventions within Irish Child and Adolescent Mental Health Services (CAMHS). Overall, clinicians demonstrated strong endorsement of the value of physical activity for young people’s mental health, yet reported limited and inconsistent implementation of physical activity interventions within routine clinical care. Knowledge of guideline-recommended physical activity levels and epidemiological data was low across professional groups and showed no meaningful association with clinical practice, highlighting a persistent knowledge–practice gap.
A key finding of this study is that clinicians’ perceived strength of the evidence base, rather than factual knowledge of guidelines, was the strongest predictor of clinical behaviour. Clinicians who viewed the evidence for physical activity interventions as stronger were significantly more likely to recommend such interventions across diagnostic groups. This finding is consistent with implementation science literature demonstrating that knowledge acquisition alone rarely leads to behaviour change in clinical practice, and that clinicians’ beliefs about capability, opportunity, and motivation are central determinants of implementation. Educational initiatives that focus solely on disseminating guidelines may therefore be insufficient unless they also address clinicians’ appraisal of the quality, relevance, and applicability of the evidence.
Attitudinal factors also played a meaningful, though secondary, role in shaping practice. Clinicians reported uniformly positive attitudes toward physical activity, both in terms of personal wellbeing and perceived therapeutic value for young people. These attitudes were moderately associated with clinical practice, suggesting that clinicians who personally value physical activity may be more inclined to integrate it into patient care. However, the consistency of positive attitudes across professional roles, contrasted with variability in practice, indicates that favourable attitudes alone are insufficient to ensure implementation. This aligns with prior research in mental health services showing that positive clinician attitudes frequently coexist with low intervention uptake in the absence of organisational support and service-level enablement.
Comparison of clinicians’ perceived evidence ratings with established evidence benchmarks revealed notable patterns. Perceptions aligned closely with the evidence base for depressive disorders and psychotic disorders, suggesting appropriate appraisal of areas where evidence is either strong or limited. In contrast, clinicians consistently overestimated the strength of evidence for physical activity interventions in anxiety disorders and ADHD. While physical activity is widely recognised as beneficial for general wellbeing, overestimation of disorder-specific evidence may lead to unrealistic expectations regarding clinical outcomes. This finding highlights the importance of targeted training that improves clinicians’ confidence in accurately interpreting and applying the evidence base, rather than assuming that enthusiasm for physical activity translates into evidence-informed practice.
Differences in practice patterns between professional groups were most evident among non-consultant hospital doctors (NCHDs), who reported lower frequencies of recommending physical activity interventions compared with consultants and nurses. This discrepancy occurred despite similar levels of knowledge, perceived evidence, and attitudes across groups. These findings likely reflect differences in role structure, continuity of care, and opportunities for lifestyle counselling within CAMHS. Nurses often have more sustained contact with patients through medication monitoring and follow-up appointments, facilitating greater integration of physical activity advice into routine care. Similar role-dependent differences in lifestyle intervention delivery have been described in youth mental health services internationally.
Importantly, clinicians working in services that reported regular delivery of physical activity interventions did not differ in knowledge, perceived evidence, or attitudes from those working in services without such interventions. This finding suggests that the presence of physical activity interventions within CAMHS is unlikely to be driven by individual clinician characteristics alone. Instead, it points toward service-level determinants, such as organisational priorities, leadership support, availability of trained staff, and access to appropriate resources. This interpretation is strongly supported by implementation frameworks that emphasise organisational context as a primary driver of sustained practice change.
Several limitations should be acknowledged. The cross-sectional design precludes causal inference, and reliance on self-reported data may introduce social desirability or recall bias. The response rate, while consistent with other web-based surveys of specialist clinicians, limits generalisability, and some professional groups were underrepresented. Additionally, the study employed a study-specific questionnaire that was not formally validated; however, it was grounded in existing literature and expert review and was appropriate for the exploratory aims of the study.
Despite these limitations, this study has several strengths, including its national scope, inclusion of multiple professional disciplines, and detailed examination of the relationships between knowledge, evidence perception, attitudes, and practice. The findings offer valuable insights into the factors that shape the implementation of physical activity interventions within Irish CAMHS and identify clear targets for future educational and organisational interventions.
Conclusion
This national survey demonstrates that while Irish Child and Adolescent Mental Health Services (CAMHS) clinicians strongly value physical activity as a therapeutic intervention, its implementation in routine practice remains inconsistent. Knowledge of physical activity guidelines was limited and did not influence clinical behaviour, highlighting a persistent knowledge–practice gap.
Clinicians’ perceived strength of the evidence base, rather than factual knowledge, was the strongest predictor of whether physical activity interventions were recommended. This suggests that implementation strategies should prioritise strengthening clinicians’ confidence in the evidence and its clinical applicability, rather than focusing solely on guideline dissemination. Differences in practice between professional roles and the lack of association with individual clinician characteristics further indicate that organisational and service-level factors are central to successful integration.
Overall, embedding physical activity interventions within CAMHS will require coordinated educational and structural supports. Addressing these factors may enhance the consistent use of physical activity interventions and improve mental and physical health outcomes for young people accessing CAMHS in Ireland.
Conflict of Interest Statement: None.
Funding Statement: None.
Acknowledgements: None.
References:
- Bull FC, Al-Ansari SS, Biddle S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451-1462. doi:10.1136/bjsports-2020-102955
- NHS Digital. Mental health of children and young people in England, 2023 (wave 4 follow-up to the 2017 survey). NHS England; 2023.
- McNicholas F, Kelleher I, Hedderman E, et al. Referral patterns for specialist child and adolescent mental health services in the Republic of Ireland during the COVID-19 pandemic compared with 2019 and 2018. BJPsych Open. 2021;7(3):e91. doi:10.1192/bjo.2021.50
- Költő A, Gavin A, Lunney L, Nic Gabhainn S. Health Behaviour in School-aged Children (HBSC) Study 2022: National Report for Ireland. University of Galway; 2024.
- Lynch S, McDonnell T, Leahy D, Gavin B, McNicholas F. Prevalence of mental health disorders in children and adolescents in the Republic of Ireland: a systematic review. Ir J Psychol Med. 2023;40(1):51-62. doi:10.1017/ipm.2021.4
- Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys. Lancet Child Adolesc Health. 2019;3(4):203-212. doi:10.1016/S2352-4642(19)30198-1
- World Health Organization. Global Status Report on Physical Activity 2022. World Health Organization; 2022.
- Knaeps S, Hardy R, Kivimaki M, Brage S, Ong KK. Accelerometer-measured sedentary time and physical activity across childhood and adolescence: seven-year follow-up in the ALSPAC cohort. Int J Behav Nutr Phys Act. 2022;19(1):121. doi:10.1186/s12966-022-01234-5
- Department of Health. National Guidelines on Physical Activity for Ireland. Government of Ireland; 2019.
- House of Commons Library. Obesity profile: statistical commentary, November 2024. UK Parliament; 2025.
- Kilduff O, Slattery J, Lee C, O’Brien S, Murrin C, Kelleher C. The Childhood Obesity Surveillance Initiative in the Republic of Ireland: Findings from 2022 and 2023 (COSI Round 6). Health Service Executive; 2024.
- Bailey AP, Parker AG, Colautti LA, Hart LM, Liu P, Hetrick SE. The mental health and well-being benefits of exercise for children and adolescents: a systematic review and meta-analysis. Psychol Med. 2018;48(7):1068-1083. doi:10.1017/S0033291717002418
- Rodriguez-Ayllon M, et al. Physical activity and mental health in children and adolescents: an updated review of reviews and an analysis of causality. Psychol Med. 2019;49(9):1383-1397. doi:10.1017/S0033291718003314
- Lubans DR, Richards J, Hillman CH, et al. Physical activity for cognitive and mental health in youth: a systematic review of mechanisms. Prev Med. 2016;76:46-57. doi:10.1016/j.ypmed.2015.12.014
- Biddle SJH, Ciaccioni S, Thomas G, Vergeer I. Physical activity and mental health in children and adolescents: an updated review of reviews and an analysis of causality. Ment Health Phys Act. 2019;16:10-21. doi:10.1016/j.mhpa.2018.11.001
- Gorham LS, Barch DM. The impact of physical activity on depression in youth: a review of potential mechanisms. Curr Psychiatry Rep. 2020;22(10):52. doi:10.1007/s11920-020-01179-1
- Pascoe MC, Parker AG, Hetrick SE. Physical activity and exercise in youth mental health promotion: a scoping review. Early Interv Psychiatry. 2020;14(6):750-766. doi:10.1111/eip.12940
- Carter T, Morres I, Meade O, Callaghan P, O’Kane N. Barriers and facilitators to physical activity interventions in youth mental health services: a mixed methods study. BMJ Open Sport Exerc Med. 2021;7(1):e001038. doi:10.1136/bmjsem-2021-001038
- Kandola A, Ashdown-Franks G, Hendrikse J, Sabiston CM, Stubbs B. Physical activity and depression: toward understanding the antidepressant mechanisms of physical activity. Lancet Psychiatry. 2019;6(3):213-220. doi:10.1016/S2215-0366(19)30060-7
- Sami M, Omar R, Gudka S, Taylor D. Physical health interventions in child and adolescent mental health services: current practice and barriers to implementation. Child Adolesc Ment Health. 2022;27(2):103-113. doi:10.1111/camh.12508
- Rosenbaum S, Tiedemann A, Sherrington C, Curtis J, Ward PB. Implementing exercise interventions in mental health services: a critical review of the evidence. Int J Environ Res Public Health. 2018;15(5):967. doi:10.3390/ijerph15050967
- Carney R, Bradshaw T, Yung AR, Birchwood M. Physical health promotion for young people at ultra-high risk for psychosis: an exploratory study of clinicians’ attitudes and practices. Early Interv Psychiatry. 2016;10(5):413-420. doi:10.1111/eip.12207
- Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
- Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4:50. doi:10.1186/1748-5908-4-50
- Stubbs B, Koyanagi A, Hallgren M, et al. Physical activity and mental health. Lancet Psychiatry. 2018;5(11):873-874. doi:10.1016/S2215-0366(18)30335-6
- Firth J, Solmi F, Wootton RE, et al. A meta-review of lifestyle psychiatry: the role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry. 2020;19(3):360-380. doi:10.1002/wps.20773
- Lubans DR, Smith JJ, Eather N, et al. Implementing physical activity interventions in youth mental health services: challenges and opportunities. Early Interv Psychiatry. 2022;16(5):505-514. doi:10.1111/eip.13158