

Epilepsy Care in Kenya: Gaps for Health Workers
Epilepsy Care in Kenya: Gaps and Opportunities from Targeted Survey of Health Workers
Angela Wabulya¹, Norbert A Odero², Antony Mugambi Kimathi³, Edith Kamaru Kwobah⁴, Daniel S Malawsky⁵, Robert Agans¹, Erin Kim³, Jeremiah Bonnet⁶, Pamela Bolton⁷, Meghan Moretti³, Muna Muday⁹, Yael Shiloh-Malawsky¹*
- University of North Carolina at Chapel Hill, USA
- Independent Consultant, Chapel Hill, NC, USA
- The Addis Clinic
- Moi Teaching and Referral Hospital, Eldoret, Kenya
- Wellcome Sanger Institute, University of Cambridge, UK
- New York University, USA
- Tech Care for All
*Correspondence: [email protected]; Department of Neurology, University of North Carolina at Chapel Hill, 170 Manning Dr, Chapel Hill, NC 27599-7025, USA
OPEN ACCESS
PUBLISHED:30 October 2024
CITATION:Wabulya, A., et al., 2024. Epilepsy Care in Kenya: Gaps and Opportunities from Targeted Survey of Health Workers. Medical Research Archives, [online] 12(1).
https://doi.org/10.18103/mra.v12i10.5923
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i10.5923
ISSN 2375-1924
ABSTRACT
Background:
The epilepsy treatment gap in sub-Saharan Africa is 75 to 90%, compared to less than 10% in high-income countries. The Addis Clinic, a U.S.-based nongovernmental organization, uses telemedicine technology to connect frontline health workers in Kenya with specialist physicians. Epilepsy specialists hypothesized that The Addis Clinic platform and network of healthcare workers in Kenya could be utilized to identify factors contributing to the epilepsy treatment gap and point to opportunities for intervention.
Methods:
Online survey of frontline health workers in The Addis Clinic network, and health professionals associated with Kenya’s Moi Teaching and Referral Hospital examined six domains: demographics and practice type, epilepsy understanding, formal training and confidence, utilization of Kenya National Guidelines for the Management of Epilepsy, resources and barriers, and use of telemedicine.
Results:
Among 210 health care workers, survey response rate was 62.9%. There were no statistically significant associations between healthcare worker characteristics, practice setup and region. Respondents were generally knowledgeable about the causes, diagnosis, and treatment of epilepsy, though some gaps in knowledge were identified. 67.9% of respondents defined epilepsy based on the longstanding definition, and 22.9% knew the new definition. Approximately 60% of respondents reported receiving formal epilepsy training, 45% received post-graduation continued education. Over 95% provide care to patients with epilepsy, and over 95% expressed interest in further training. Majority of respondents reported some or extreme barriers to epilepsy care related to community beliefs, stigma, limited access or high costs of testing, medications, and specialists.
Conclusion:
Health workers commonly reported awareness of the Kenya National Guidelines for the Management of Epilepsy, had exposure to epilepsy and experience in epilepsy care, and showed basic background knowledge of epilepsy; however, knowledge gaps were identified. The greatest barriers to epilepsy care reported include community beliefs, stigma, and lack of resources, with regional variability found. The Addis Clinic partnership with regional local leaders and epilepsy specialists will utilize these findings to develop focused interventions.
Keywords:
Online survey, Epilepsy, Low- and middle-income countries, Treatment gap, Kenya.
Introduction
Epilepsy, the tendency to have unprovoked epileptic seizures, affects over 50 million people worldwide of whom 80% are in low- and middle-income countries.¹ Poorly controlled epilepsy is linked to injury, early death and poor social, education and employment outcomes. With appropriate management, 70% of patients with epilepsy can achieve seizure control and have improved health and social outcomes.² The epilepsy treatment gap is defined as the proportion of people with active epilepsy whose seizures are not treated appropriately. Multiple epidemiological studies show that the epilepsy treatment gap in Sub-Sahara Africa is 75 to 90% or higher, compared with less than 10% in high-income countries.³ ⁷
Kenya’s Ministry of Health (KMOH) has implemented guidelines for management of epilepsy (KMOH, 2016),⁸ however, KMOH remains burdened dominantly by infectious diseases such as HIV/AIDS, and often faces challenges with adequate training of health care workers at the rural health facilities to diagnose and manage epilepsy. In a study in Kilifi, Kenya, 74% of patients with epilepsy reported seeking treatment from a health facility, but 66% were not on anti-seizure medication (ASM) based on drug levels.⁹ In another study across five African countries, only 20% of people with epilepsy benefited from ASM, according to optimal drug levels.¹⁰
Telemedicine practices have provided additional tools for access to diagnosis and treatment of epilepsy.¹¹ ¹² The Addis Clinic, a U.S.-based non-governmental organization (NGO), was established to increase access to high-quality healthcare through digital health solutions (https://www.addisclinic.org/). To bridge healthcare gaps, The Addis Clinic recruits volunteer physicians globally to help with the management plans of patients who are under the care of lower- and middle-level skilled health workers in medically underserved areas.¹³ ¹⁴ During these referrals, the local healthcare workers have reported challenges with epilepsy management such as the lack of training for efficient management of their patients. Prior publications have shown that targeted epilepsy training can improve knowledge and confidence among nonphysician providers in frontline African settings.¹¹ To better understand the specific regional challenges to epilepsy care in Kenya, we surveyed a targeted population of health care workers affiliated with The Addis Clinic and/or with Moi Teaching and Referral Hospital (MTRH) in Eldoret, Kenya. We hypothesized that The Addis Clinic platform and the network of frontline health workers in Kenya could be utilized to identify factors contributing to the epilepsy treatment gap and point to opportunities for intervention.
STUDY MAIN OBJECTIVES:
-
Investigate resources, current practices and challenges faced by health care workers in the daily management of seizures and epilepsy among their patients presented to their facilities.
-
Investigate the training of the health care workers and level of comfort as pertains to the management of epilepsy, including baseline and continued medical education and their utilization by health care workers.
-
Investigate the utilization of the Kenya National Guidelines by health care workers in the management of epilepsy.
-
Study the use of telemedicine by surveyed healthcare workers.
Methods
ETHICAL APPROVAL OF STUDY:
This study was reviewed and approved by the University of North Carolina Institutional Review Board.
STUDY DESIGN:
An observational online survey of frontline health workers in Kenya including healthcare workers of The Addis Clinic network and additional Kenyan healthcare professionals associated with MTRH.
STUDY PHASES:
Phase 1. Survey development:
A survey tool tailored to the study’s specific aims was developed through review of literature, the International League Against Epilepsy (ILAE), and the Kenya National Guidelines of epilepsy management,⁸ 15 17 and in consultations of local Kenyan patients, healthcare workers (AMK) and specialists of in Kenya (EKK) and in the USA (AW, YSM). Experts in population-based research methods, questionnaire development and language translation (PB, RA) reviewed and contributed to the survey development. The survey questions were formed in a combination of multiple-choice single select, select all that apply and Likert scale. The tool was tested in a small pilot of the target population in Kenya, with responses informing the final modification of the survey. The final version of the survey included a total of 54 questions in six content segments, corresponding to the study objectives. (Supplementary Data 1)
A. Investigate the demographic characteristics of health care providers and their practice setting.
B. Investigate the knowledge and attitudes pertaining to epilepsy.
C. Investigate the training of the health care workers in management of epilepsy, and level of comfort including baseline and continued medical education and their utilization.
D. Investigate the utilization of the Kenya National Guidelines for the Management of Epilepsy (KNG) by health care workers.
E. Investigate resources, current practices and challenges faced by rural health care workers in the daily management of seizures and epilepsy amongst patients presenting to health care facilities in Kenya.
F. Examine the current use of telemedicine tools by the local healthcare system, including the impact of the COVID-19 pandemic on epilepsy care, and examine the current use of virtual platforms or telemedicine tools for education before and after the Covid-19 pandemic.
Phase 2.
Administration of the survey, over the course of 2 months, from October to November 2021
Phase 3.
Data analysis
STUDY POPULATION:
Health care workers including clinical officers (COs), nurses and medical doctors taking care of adult and pediatric patients within the The Addis Clinic network in Kenya, and health care professionals associated with MTRH.
RECRUITMENT STRATEGY:
Health care providers within The Addis Clinic network were introduced to the survey through phone and email and offered an opportunity to participate. Providers associated with MTRH were introduced to the study by the local study team and requested to participate. Study participants received a compensation of $5.00 for their participation in the study.
SAMPLE SIZE:
Of the 210 health care workers asked to participate, a total of 132 (67%) completed the survey.
CONSENT PROCEDURES:
Consent prior to participation was obtained via the survey platform. In addition, the local study coordinator and the study’s principal investigators were available to respond to any questions that study participants had.
DATA COLLECTION AND MANAGEMENT:
The SurveyMonkey online data collection application, accessible via smartphone or computer, was used to administer the survey. The study did not collect any protected health information. Responses obtained from the survey were held in a secure password protected server with access limited to authorized study personnel only. Also, to ensure true anonymity, all data was de-identified and anonymized prior to analysis.
STATISTICAL METHODS:
Descriptive statistics and generalized linear models were used for survey analysis. Descriptive statistics and generalized linear models were generated in R using base R functions. Continuous variables were analyzed via linear regression using the lm function and binary variables were analyzed with a logistic regression using the glm function. Covariates included age, sex, region of practice, medical title, healthcare practice setting (Level 4 or higher), type of medical care, patient population (young pediatric, older pediatric, and adult).¹
Results
SURVEY RESPONSE RATE
Of 210 healthcare workers approached and asked to participate in the survey, a total of 132 completed the survey, a response rate of 67%. Completion rates for questions in segments A through E of the survey were greater than 97%, with 129 to 132 participants responding to each one of the questions. (Section A 99.2–100%, section B 100%, section C 98.5–99.2%, section D 97.7–99.2%, section E 98.5–99.2%). Response rates to segment F were lower; 37 to 59 participants responded to questions in this segment (28.1–29.5%).
DEMOGRAPHICS AND PRACTICE CHARACTERISTICS (TABLE 1)
The majority of healthcare professionals surveyed were Clinical Officers (COs) (46.9%) and nurses (43.6%), with lower representation of medical doctors (6.1%). This is consistent with the reported composition of the health professionals workforce registered in Kenya, according to the Kenya Health Workforce Report: The Status of Healthcare Professionals in Kenya, 2015, published in 2019,¹⁸ and reflects the model of care in this region. Per the report, in 2015, there were 31,896 nurses, 10,562 COs, and 5,660 active medical doctors in Kenya (66%, 22% and 12%, respectively).
The largest group of respondents, 42.4%, reported Nyanza province to be their main province of practice, followed by 20.5% in Rift Valley province. Both provinces are located in the western region of Kenya, reflecting the geographical distribution of The Addis Clinic network. The remaining 37% of participants’ main practice was in five other provinces, only the North Eastern province was not represented. A majority of the respondents were in the 20–29-year age group (75%), and the majority had practiced for four years or less (65.1%). Most of the respondents practice general medical care, and their healthcare practice settings represented all levels of care from level 1 through level 6. The vast majority of respondents see greater than 10 patients per day, and over a third see more than 30 patients in a day. All participants except for 5 (3.8%) reported that they have seen epilepsy patients in the past six months, the majority have seen 1 to 10 patients and 35% have seen more than 10 patients with epilepsy in the six months period. The great majority, 92.4%, know someone with epilepsy, and nearly all have witnessed a seizure.
There were no statistically significant associations between healthcare workers’ demographic characteristics, practice type or practice settings. Overall, medical doctors, and health workers practicing in healthcare settings at levels 4 to 6 were more likely to report managing over 10 patients with epilepsy in the past six months. In comparison, 68% of nurses and 60% of COs reported seeing one to 10 patients with epilepsy in the same period. Among senior COs, 66.7% managed more than 10 patients, and 33% managed over 20 patients with epilepsy in the past six months. All eight medical doctors surveyed had seen epilepsy patients in the past six months: three managed one to 10 patients, three managed 11 to 20 patients, and two managed 21 to 30 patients.
EPILEPSY KNOWLEDGE, UNDERSTANDING AND PRACTICE (TABLE 2.)
The majority of respondents, 78.8%, correctly identified epilepsy as a brain disease. In addition, 67.9% were aware of the commonly used definition of epilepsy: two unprovoked seizures separated by 24 hours (Table 2.). However, only 22.3% were aware of the new diagnostic criteria for epilepsy added in 2014: a single isolated seizure with risk factors of seizures. Epilepsy diagnosis is typically a clinical
diagnosis, EEG and brain imaging are used to identify an etiology and guide management but are not required for making a diagnosis of epilepsy. Approximately one third (35.6%) correctly responded that in order to diagnosed epilepsy one may not need imaging or EEG. Approximately two thirds incorrectly responded that one must obtain brain imaging or EEG to make a diagnosis of epilepsy (36.4% and 28.6%, respectively). Multiple causes of epilepsy were correctly identified by the great majority of participants, reflecting general understanding of multiple possible causes of epilepsy, only a small minority considered unrelated factors such as excessive worry (6.8%) and witchcraft or evil spirits (0.8%), as causes of epilepsy.
All respondents recommend to their patients a health facility for treatment of epilepsy, with a small minority recommending prayers in addition to health facilities. A majority reported that they believe that epilepsy is a brain disease (Table 2.), and the majority that epilepsy is a psychiatric disorder, which deviates from the accepted medical definition. One quarter of responders (26.5%) believe that epilepsy is intellectual disability. While intellectual disability is seen in some patients with epilepsy, this is not a consistent finding or part of the definition of epilepsy. Duration of treatment of epilepsy with daily medication for at least 2 years was correctly selected by 68.9%, the rest selected shorter duration or were not sure of duration of the treatment.
All 132 survey respondents reported that they have prescribed one or more ASMs. The vast majority, 128 (97.0%) reported that they have prescribed one of the chronic ASMs, such as phenobarbital, carbamazepine and phenytoin. Only four participants (3.1%) report prescribing only diazepam, which is commonly used for emergency treatment, but might have been used for chronic treatment (Table 2.). The great majority correctly recommend that a person living with epilepsy can hold a job, with 81.1% indicating “when possible” and 15.2% indicating “always”. When treating women with epilepsy and considering pregnancy, 85.6% of respondents consider the effect of ASMs on the fetus, and approximately half (52.3%) correctly recommend preconception treatment with folate supplementation. When selecting ASMs for patients being treated with antiretroviral medications, 95.5% of respondents correctly consider drug-drug interactions, 43.9% consider medication side effects, and 36.4% consider organ dysfunction.
On sub-group analysis there were several associations of healthcare workers’ demographics and practice characteristics with epilepsy knowledge. For example, nurse respondents had lower odds than COs of incorrect responses to some questions assessing knowledge, such as that one must get brain imaging to make a diagnosis of epilepsy (OR 0.28 p-value 0.009). On the other hand, nurses had lower odds than COs to correctly recommend treatment with ASM for two years (OR 0.30, p-value 0.02). Health workers from the Rift Valley province had greater odds than Nyanza province health workers of incorrectly considering epilepsy to be mental retardation (OR 3.46, p-value 0.045), but on the other hand, they were more likely to correctly recommend that treatment with ASMs should be prescribed for two years (OR 8.33, p-value 0.01).
We concluded that although a few group associations were statistically significant, the magnitude of these differences was generally low, and there was no clear direction of associations (in relation to health worker type, for example). The survey results indicate a solid foundation of basic knowledge and understanding regarding the causes, diagnosis, and treatment of epilepsy, as well as the fundamentals of care. Additionally, there is common personal experience in the management of epilepsy and seizures. However, some gaps in knowledge were identified, highlighting opportunities for improvement.
EPILEPSY TRAINING AND LEVEL OF CONFIDENCE
More than half of respondents reported having undergone training in epilepsy: 62.9% had epilepsy-specific education during their clinical certification training, an additional 25.8% and 20.5% had post-graduation and on-the-job training (Table 3). The great majority, 91.7% to 97.0%, reported that they felt confident in their knowledge of different aspects of management of seizures and epilepsy; about half felt very confident and half somewhat confident. Only a small minority, 1.5% to 7.6%, reported feeling not confident at all about aspects of epilepsy and seizure care (Table 2.). When asked about sources used to support care in epilepsy, three quarters reported using Kenya National Guidelines of Management of Epilepsy. In addition, half reported consulting a colleague, and half seek consult through telemedicine.
We found several group associations in training and level of confidence. There were greater odds of training in epilepsy reported by health care workers from Eastern, and Rift Valley provinces in comparison to Nyanza province (OR 7.46, 6.05, 3.35, p-value 0.02, 0.049, 0.04, respectively). Lower odds of post-graduation training (continuing professional education) were found in NGO and publicly funded institutions (OR 0.03, 0.08, p-value 0.023, 0.049, respectively), and in the Eastern and Rift Valley provinces (OR 0.09, 0.21, p-value 0.046, 0.048, respectively). Female responders felt less confident than male responders in evaluation of seizures, making epilepsy diagnosis and starting treatment (OR 0.26, 0.28, 0.22, p-value 0.005, 0.011, 0.003, respectively), and nurses felt less confident than COs in the same three elements of epilepsy care: evaluation, epilepsy diagnosis and starting treatment (OR 0.25, 0.19, 0.31, p-value 0.005, 0.0016, 0.022, respectively). The only geographic group association found was lower level of confidence in making epilepsy diagnosis reported by health workers from the Eastern province (OR 0.12, p-value 0.039). Interestingly, in comparing health workers practicing less than four years with those practicing five years or longer, we found no significant difference in correct responses to knowledge questions, and no difference in the level of confidence in management of epilepsy and seizures.
We noted that while there were no statistically significant differences between female and male respondents in correct responses to knowledge questions, and no clear differences in knowledge between nurses and COs, both females and nurses reported less confidence on the management of epilepsy.
UTILIZATION OF KENYA NATIONAL GUIDELINES FOR THE MANAGEMENT OF EPILEPSY
The Kenya National Guidelines (KNG) for the management of epilepsy were launched in 2014 with the aim of demystifying epilepsy, providing a step-by-step guide for healthcare workers across all cadres and levels of care, from primary to tertiary, and harmonizing the treatment of epilepsy by establishing standards of care. A majority of respondents (77.7%) were aware of the KNG, and 75.0% referred to the KNG for epilepsy management (Table 3), despite only 53.3% having received training on use of the guidelines.
Some group associations were identified regarding the implementation of the KNG. Medical doctors, healthcare workers caring for older pediatric patients, specialist care practices, and those working in level 4 to 6 practice settings had higher odds of being aware of the KNG for the management of epilepsy (OR 31.5, 5.53, 4.41, 3.97, p-value 0.012, 0.034, 0.022, 0.017, respectively). Conversely, respondents from the Rift Valley province had lower awareness of the guidelines (OR 0.15, p-value 0.015).
RESOURCES AND BARRIERS FOR EPILEPSY CARE
The great majority of respondents reported some or severe barriers to multiple aspects of epilepsy care (Graph 1). Barriers to evaluation include lack of access to EEG, laboratory testing and brain imaging. In addition, they reported lack of access to trained personnel and medications, and high cost of medications, EEG and imaging. Infrastructural challenges, such as poor roads and lack of transportation to the health center, were reported as common and frequently severe barriers. Tendency in the community not to seek medical care, presence of traditional beliefs and practices, and epilepsy stigma were barriers reported by over 95% of the respondents, with about half reporting these to be extreme barriers (41.2%, 48.9%, and 55.7% respectively).
A few statistically significant regional differences were found. Respondents from the Eastern and Rift Valley provinces report less frequently the lack of access to EEG as a limitation (OR 0.0005, 0.012 p-value 0.012, 0.043, respectively). On the other hand, healthcare workers caring for adult patient populations reported greater limitation of access to EEG (OR 27.1, p-value 0.043). Lack of access to blood tests and brain imaging was more commonly reported by health workers caring for older pediatric patients (OR 5.64, 5.75, p-value 0.005, 0.004, respectively). Extreme barrier of access to imaging was less commonly reported by health workers practicing in Levels 4 to 6 healthcare settings (OR 3.32, p-value 0.024).
We did not find group associations in barriers to epilepsy care related to patients not seeking medical care, and traditional beliefs. However, patient stigma was less commonly reported as an extreme barrier by medical doctors than other cadres (OR 0.10, p-value 0.042), and stigma was more commonly reported as an extreme barrier by health workers in the Eastern province in comparison to Nyanza, and by health workers serving adult patient population (OR 6.36, 4.10, p-value 0.021, 0.041, respectively).
USE OF TELEMEDICINE
Only one-third of the participants completed the section related to the use of telemedicine; we suspect that a technical issue caused the low response rate to questions in this section of the survey. Among the 39 participants who did respond, 36 (92.3%) reported using telemedicine consultations to assist in patient management, while only 3 (7.7%) reported not using telemedicine. Nineteen participants utilized phone calls or text messages, 10 used the WhatsApp video or audio application, and 30 used The Addis Clinic platform.
Regarding the frequency of telemedicine use, 11 participants (30%) reported using telemedicine for fewer than one case per week, while 26 participants (70.1%) used these channels more than once a week; among them, 5 (13.5%) reported using telemedicine for more than five cases per week. In the treatment of epilepsy or seizures, 39% of respondents rarely used telemedicine to support clinical decision-making (in less than 10% of epilepsy cases), about half (55.3%) used telemedicine 10% to 50% of the time, and only 5.3% (2 respondents) used telemedicine for more than 50% of epilepsy or seizure-related cases.
Challenges reported in using telemedicine included delayed responses, which was reported by 29 participants (74% of those who responded to this section), not receiving a response was reported by 9 participants (23%), and the cost associated with telemedicine was reported by 18 participants (46%).
Barriers to telemedicine use, associated with odds of using telemedicine, were found. For example, health workers in the Eastern province had lower odds of using telemedicine platforms compared to those in the Nyanza province (OR 0.05, p-value 0.019). Respondents caring for younger pediatric patients had greater odds of using telemedicine (OR 3.56, p-value 0.03) and higher odds of using telemedicine for consultation (OR 6.49, p-value 0.02). Conversely, medical doctors were much less likely than other cadres to use telemedicine consultations (OR 0.02, p-value 0.006).
Table 1. Participants demographics and practice characteristics (n=132)
| n | (%) | n | (%) | ||
|---|---|---|---|---|---|
| Gender | Type of medical care | ||||
| Male | 81 | 61.4% | General medical care only | 92 | 70.2% |
| Female | 51 | 38.6% | General & specialized medical care | 37 | 28.2% |
| Specialized medical care only | 2 | 1.5% | |||
| Medical title | Healthcare practice setting (all that applies)* | ||||
| Clinical Officer | 62 | 47.0% | Level 1 | 13 | 9.8% |
| Nurse | 56 | 42.4% | Level 2 | 42 | 31.8% |
| Medical doctor | 8 | 6.1% | Level 3 | 52 | 39.4% |
| Senior clinical officer | 6 | 4.5% | Level 4 | 52 | 39.4% |
| Level 5 | 34 | 18.2% | |||
| Level 6 | 5 | 3.8% | |||
| Main province of practice | Total number of patients personally seen per day | ||||
| Nyanza | 56 | 42.4% | 1–10 | 12 | 9.2% |
| Rift Valley | 27 | 20.5% | 11–20 | 42 | 32.1% |
| Nairobi | 15 | 11.4% | 21–30 | 28 | 21.4% |
| Eastern | 16 | 12.1% | More than 30 | 49 | 37.4% |
| Western | 11 | 8.3% | Total number of epilepsy patients seen in past six months | ||
| Central | 4 | 3.0% | None | 5 | 3.8% |
| Coastal | 3 | 2.3% | 1–10 | 80 | 61.5% |
| 11–20 | 22 | 16.9% | |||
| Age (years) | 21–30 | 13 | 10.0% | ||
| 20–29 | 99 | 75.0% | More than 30 | 10 | 7.7% |
| 30–39 | 28 | 21.2% | Know someone with epilepsy | ||
| 40–49 | 2 | 1.5% | Yes | 122 | 92.4% |
| 50–59 | 2 | 1.5% | No | 10 | 7.6% |
| >60 | 1 | 0.8% | Witnessed a seizure | ||
| Years in practice | Yes | 129 | 97.7% | ||
| Less than 1 year | 7 | 5.3% | No | 3 | 2.3% |
| 1–4 years | 79 | 59.8% | |||
| 5–9 years | 37 | 28.0% | |||
| 10–15 years | 6 | 4.5% | |||
| More than 20 years | 3 | 2.3% |
Footnote:
* Kenya has defined six levels of medical care infrastructure. Levels 1 (community) and 2 (dispensary) have outpatient care only. Level 3 comprises small hospitals. Level 4 health facilities are larger hospitals with at least 150 beds (with male, female, paediatric, antenatal, and postnatal wards). Level 5 hospitals act as tertiary care centers, providing specialized services including advanced diagnostics, surgeries, and treatments; they handle cases referred from lower-level hospitals. Level 6 comprises the most advanced and specialized medical services in the country. These facilities handle complex cases and serve as training and research centers. Moi Teaching and Referral Hospital is a Level 6 facility.
Table 2. General understanding and management of epilepsy among frontline health workers, confidence in management and training history (n=132)
Epilepsy Knowledge
| Definition of epilepsy | n | % |
|---|---|---|
| ≥ / = 2 unprovoked seizures (older definition) | 93 | 70.5% |
| One seizure & risk factors (new definition) | 30 | 22.7% |
Causes of epilepsy (all that applies)
| Cause | n | % |
|---|---|---|
| Trauma | 125 | 94.7% |
| Brain tumor | 109 | 82.6% |
| Genetic or congenital | 105 | 79.5% |
| Infections | 92 | 69.7% |
| Stroke | 68 | 51.5% |
| Excessive worry | 9 | 6.8% |
| Witchcraft, evil spirits | 1 | 0.8% |
To diagnose epilepsy, one…
| Statement | n | % |
|---|---|---|
| May not need EEG or brain imaging | 47 | 35.6% |
| Must obtain an EEG | 50 | 37.9% |
| Must obtain brain imaging | 35 | 26.5% |
For a patient with epilepsy, do you recommend? (all that applies)
| Recommendation | n | % |
|---|---|---|
| Health facility | 132 | 100.0% |
| Prayers | 8 | 6.1% |
| Herbal medicine | 1 | 0.8% |
| No treatment, epilepsy cannot be treated | 1 | 0.8% |
| I am not sure | 1 | 0.8% |
How long should ASM* be given in epilepsy?
| Duration | n | % |
|---|---|---|
| Every day for at least two years | 91 | 68.9% |
| Everyday for one year | 24 | 18.2% |
| Only at the time of seizure, or for one week | 12 | 9.1% |
| I am not sure | 7 | 5.3% |
* ASM = anti-seizure medication
Confidence in management
Evaluating seizures
| Confidence level | n | % |
|---|---|---|
| Very confident | 62 | 47.0% |
| Somewhat confident | 66 | 50.0% |
| Not confident at all | 2 | 1.5% |
Making new epilepsy diagnosis
| Confidence level | n | % |
|---|---|---|
| Very confident | 51 | 38.6% |
| Somewhat confident | 75 | 56.8% |
| Not confident at all | 5 | 3.8% |
Starting treatment and long-term management
| Confidence level | n | % |
|---|---|---|
| Very confident | 54 | 40.9% |
| Somewhat confident | 67 | 50.8% |
| Not confident at all | 10 | 7.6% |
Instructing family members of seizure first aid
| Confidence level | n | % |
|---|---|---|
| Very confident | 92 | 69.7% |
| Somewhat confident | 36 | 27.3% |
| Not confident at all | 3 | 2.3% |
Epilepsy Practice
Have prescribed these ASMs* (all that applies)
| ASM | n | % |
|---|---|---|
| Phenobarbital | 115 | 87.1% |
| Carbamazepine | 106 | 80.3% |
| Diazepam | 99 | 75.0% |
| Phenytoin | 84 | 63.6% |
| Lorazepam | 35 | 26.5% |
| Depakote | 31 | 23.5% |
| Levetiracetam | 17 | 12.9% |
Table 3. Epilepsy training, perceptions and information sources
Epilepsy training
| Category | n | % |
|---|---|---|
| Prior epilepsy/seizure management training | ||
| Yes | 78 | 59.5% |
| No | 53 | 40.5% |
Type of training (all that applies)
| Type | n | % |
|---|---|---|
| Formal clinical training in school of certification | 83 | 62.9% |
| Post-certification continued professional education | 53 | 25.8% |
| On the job training | 27 | 20.5% |
Epilepsy perceptions, FHW and the community
I believe that epilepsy is (all that applies)
| Belief | n | % |
|---|---|---|
| Brain disease | 104 | 78.8% |
| Mental retardation or intellectual disability | 41 | 31.1% |
| Psychiatric disorder | 35 | 26.5% |
| Madness | 2 | 1.5% |
| Spirit possession | 0 | 0% |
People in my community generally believe that epilepsy is (all that applies)
| Belief | n | % |
|---|---|---|
| Spirit possession | 97 | 73.5% |
| Brain disease | 43 | 32.6% |
| Psychiatric disorder | 39 | 29.5% |
| Madness | 40 | 30.3% |
| Mental retardation or intellectual disability | 32 | 24.2% |
Resources used for epilepsy care
Aware of the KNGME?**
| Response | n | % |
|---|---|---|
| Yes | 101 | 77.7% |
| No | 29 | 22.3% |
Where did you learn about KNGME?**
| Source | n | % |
|---|---|---|
| Colleague | 44 | 38.6% |
| Formal training | 33 | 28.9% |
| Continued professional development | 28 | 24.6% |
| Other | 9 | 7.9% |
Sources of information used for seizures/epilepsy care (all that applies)
| Source | n | % |
|---|---|---|
| Kenya National Guidelines for Epilepsy management | 99 | 75.0% |
| A colleague at same workstation or another location | 75 | 56.8% |
| Tele-platform consultation to other clinicians | 66 | 50.0% |
| Electronic resources such as the ILAE | 39 | 29.5% |
** KNGME – Kenya National Guidelines for the Management of Epilepsy
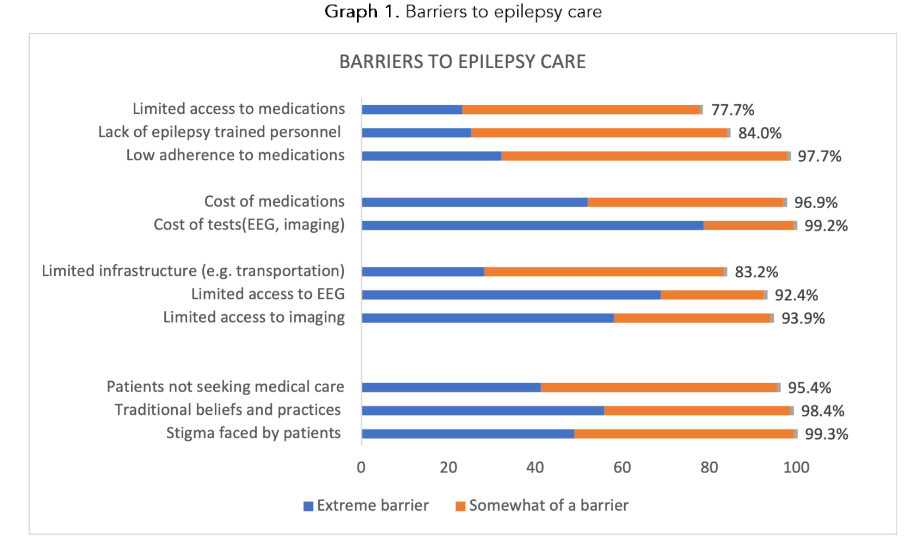
Graph 1. Barriers to epilepsy care
Discussion
Epilepsy affects over 50 million people globally, with higher prevalence in low- and middle-income countries,¹ where over 85% of worldwide cases of epilepsy occur. In Kenya epilepsy has become the 19th leading cause of disability-adjusted life years (DALYs) in 2017, up from 21st in 2013. In this study we aim to identify region-specific elements contributing to the epilepsy treatment gap, a measure of untreated active epilepsy, which studies have shown to be 75% to 90% in Sub-Saharan Africa, and greater than 96% in specific populations.⁷,¹⁹,²⁰
Kenya, like many African nations, has a healthcare workforce that heavily relies on nurses and Clinical Officers (COs), who are primarily responsible for delivering the majority of healthcare services, particularly in rural and underserved areas.²¹ In contrast, medical doctors typically provide specialized and advanced medical care, predominantly in urban and tertiary care settings. A 2017 report by the Kenya Medical Practitioners and Dentists Council surveyed frontline health workers in Kenya, revealing that 46.9% were COs, while only 6.1% were medical doctors.²² This distribution is consistent with the data noted by Okoroafor SC,²² which reflects the typical composition of the country’s healthcare workforce.¹⁸
We developed a novel, region-tailored survey (Appendix 1) for healthcare professionals to assess epilepsy care in rural Kenya. The survey was distributed via a tele-platform, leveraging the established telemedicine consultation platform and network of The Addis Clinic, which has a significant presence in the western rural regions of Kenya. Despite the survey’s length (approximately 30 minutes to complete), the response rate was robust, providing extensive data on various aspects of epilepsy care. This demonstrates the survey’s feasibility, cost-effectiveness, and ease of implementation. We propose that the epilepsy care assessment survey that we developed is a tool that can be used in other regions to identify region-specific needs related to epilepsy care and management.
The survey identified several key strengths among the Kenyan health workforce. It revealed a solid foundation of basic knowledge of epilepsy diagnosis and management and common personal experience with epilepsy or seizures, as well as witnessing seizures at all levels of medical training. Additionally, we majority of respondents reported regular experience managing epilepsy patients and a keen interest in further learning. Most healthcare workers were aware of the KNG for the management of epilepsy; however, many did not have formal training in their use. This practical guide is a valuable resource: greater familiarity, formal training, and an increase in its use could enhance competency in epilepsy care.
Another notable strength identified is that health workers uniformly recommended that epilepsy patients seek care in healthcare facilities, countering prevalent traditional beliefs in their communities that associate epilepsy with spirit possession or witchcraft, leading people to seek help from traditional and spiritual healers.
Most respondents identified limited resources and community perceptions and beliefs (Graph 1) as significant challenges impacting the delivery of care to people with epilepsy. Additionally, barriers related to access and costs of medications, diagnostics, and imaging were reported. Non-adherence to medications, which is likely multifactorial and influenced by both resource limitations and patients’ perceptions and beliefs, was also highlighted by the majority of respondents. Furthermore, gaps in respondents’ knowledge and limited formal training in epilepsy care were detected.
Despite national and global efforts to demystify epilepsy, patient stigma remains a major barrier reported by 99% of respondents to the survey. This challenging barrier will be important to address in any intervention aiming to decrease the epilepsy treatment gap.
INTERVENTIONS: PROPOSED ACTIONS TO ADDRESS THE EPILEPSY TREATMENT GAP
Building on the knowledge gained from the survey, we propose several actions leveraging existing strengths and resources to address factors contributing to the epilepsy treatment gap.
A significant impact can be achieved by addressing epilepsy knowledge gaps among frontline primary care health professionals, who have direct and daily contact with patients. A task-shifting paradigm, transitioning epilepsy care to community health professionals by integrating epilepsy care into primary care, is recommended by the World Health Organization (WHO) for low- and middle-income countries.²³,²⁴ This concept of shifting epilepsy care from medical doctors and specialty experts to epilepsy-trained community health workers was studied by the Bridging the Childhood Epilepsy Treatment Gap in Africa (BRIDGE) project.¹⁹ The task-shifting paradigm has demonstrated benefits in other conditions, including HIV care²⁵,²⁶ and preliminary evidence suggests its effectiveness in depression care as well.²⁷ The Addis Clinic platform and its network connections can serve as a link to implement epilepsy training programs, provide patient specific consultations, and support patient education resources.¹³
Use of an epilepsy screening questionnaire tool as part of routine primary care visits could help identify patients with undiagnosed epilepsy; an estimated 75% in this population.² We hypothesize that following this model, initiating active epilepsy screening practices in patients attending primary care health visits for other reasons, who may not openly discuss seizures, could increase the proportion of patients diagnosed and treated. Connecting primary healthcare professionals with epilepsy specialists through The Addis Clinic platform could support the management of complex cases and enhance in-practice experience and learning.
The fundamental basis of epilepsy diagnosis lies in the patient’s history, gathered through personal accounts and witness reports of episodes, which requires no specialized equipment. After diagnosing epilepsy, the initial step in treatment involves prescribing ASM. While more expensive and less accessible resources such as blood tests, EEGs, and brain imaging are valuable, they are not required in order to start ASM treatment. Efficient use of imaging, EEG, and blood tests, along with avoiding unnecessary delays in initiating medication, are crucial for providing optimal care for people with epilepsy. Although barriers related to access to medical services and infrastructure present significant challenges, treatment protocols that emphasize resource-minded evaluations and prompt treatment based on clinical diagnosis can improve epilepsy care.
A critical barrier to epilepsy diagnosis lies in local community beliefs,²⁸ and traditional practices, which result in patients’ reluctance to seek care. As revealed by the survey, these community perspectives are in stark contrast to the perceptions of healthcare workers. Healthcare professionals who are in direct primary care relationships within these regions are uniquely positioned to mobilize a shift in community perceptions and beliefs, fostering an understanding of epilepsy as a treatable medical disorder. Community and patient education programs, along with engagement with community health professionals, may be effective steps in altering traditional stigma and promoting the use of medical treatments.
Respondents indicated that access to continued professional medical education is limited by availability and cost. The Addis Clinic network, a free access platform, can be used to introduce and promote online resources such as KNG for the Management of Epilepsy, WHO Mental Health Gap Action Programme (mhGAP) or the International League Against Epilepsy training and reference materials.²⁹
Finally, The Addis Clinic telemedicine platform could provide a tool for tracking patients diagnosed with epilepsy and collecting prospective data on practices, care, and outcomes. This data will enable assessment of the impact of interventions on epilepsy care.
If shown to be successful, similar approaches can be scaled to provide targeted and continuous community awareness, education, and sensitization about epilepsy through partnerships with the Ministry of Health and local communities. The primary workforce managing epilepsy at the frontline includes COs and nurses. Reviewing and updating training programs for these groups could help address existing gaps. Additionally, continued public-private partnerships are needed to tackle systemic barriers such as poor infrastructure and the costs of medication and imaging, among others.
The study team brought together essential partners:
The Addis Clinic’s leadership (AMK, EK, PB, MM, MM), and its network of hundreds of Kenyan primary healthcare professionals, most of whom are based in rural western Kenya; Dr. Kwobah, a specialist psychiatrist from Moi Teaching and Referral Hospital in Eldoret, western Kenya, whose ties in the medical community, knowledge of local epilepsy practice standards and understanding of the local healthcare system were critical for the project; and neurology epilepsy specialists (AW, YSM) from the University of North Carolina, who have experience consulting with The Addis Clinic and consulted for the study scientists with expertise in survey development methodology (RA, PB) and statistics (DSM). Public health scientist (NAO) and epilepsy specialist (AW) are the core project team since its inception, grew up in the region and helped guide epilepsy caring and connecting with stakeholders in the local community.
The study has several limitations. There were missing responses to the survey questions, most notably in the sixth section regarding the use of telemedicine, which had a low response rate. Additionally, since the survey was conducted within health facilities associated with The Addis Clinic network and Moi University in Rift Valley, the results may not be generalizable to represent the broader national landscape of epilepsy care. As with other surveys, the accuracy of the responses is difficult to verify. Lastly, epilepsy diagnosis in this study relied heavily on reports from patients or their caretakers, and the study was not designed to independently verify health information and practice data.
Conclusion
Kenya, like many African nations, faces a high burden of epilepsy, particularly in rural areas where healthcare infrastructure is underdeveloped. We report results from a survey assessing epilepsy care, resources, and barriers among frontline health workers in Kenya. Respondents commonly reported awareness of the Kenya National Guidelines for the Management of Epilepsy and experience in epilepsy care, showing basic knowledge of epilepsy. However, knowledge gaps were identified. The greatest reported barriers to epilepsy care include community beliefs, stigma, and a lack of resources and epilepsy-trained personnel.
The Addis Clinic provides a unique platform that proved useful in reaching a broad range of facilities, including those in rural areas, to conduct an online epilepsy care survey. This platform and network could also be leveraged to deliver targeted interventions aimed at addressing barriers to care, such as improving access to epilepsy resources, offering in-service education programs, and providing expert consultations and support. The knowledge gained from this study could be used in advancing a “task-shifting paradigm” that builds the competency of nonphysician primary care health workers in epilepsy care, particularly in regions with limited access to higher-level facilities and specialists.
The survey developed for this study is a tool that can be utilized for future similar studies in other countries and regions. The Addis Clinic’s partnership with healthcare professionals at the University of North Carolina and Moi Teaching and Referral Hospital (MTRH) serves as an example of a successful collaboration. We plan to continue using this collaborative model to work towards improving epilepsy management in Kenya and beyond.
The Clinical Relevance of the Study
The study informs us of healthcare resources, limitations and specific regional challenges, and points to potential strategies to take in an effort to decrease the epilepsy treatment gap. The study team aims to continue the collaboration of The Addis Clinic with healthcare centers to develop interventions and monitor impact.
Supplementary information
Supplementary Data 1 – The Addis Clinic Epilepsy Survey Questionnaire – Kenya
Conflict of interest disclosure:
The authors do not have conflicts of interest related to this study.
Funding statement:
Support from the faculty development grant from University of North Carolina.
Acknowledgements:
Wade Munday³, participants in the study
Ethics approval statement:
This study was reviewed and approved by the UNC-IRB under reference ID 397476.
Patient consent statement:
N/A
Permission to reproduce material from other sources:
N/A
Clinical trial registration:
N/A
References
1. Epilepsy: A public health imperative. World Health Organization. License: CC BY-NC-SA 3.0 IGO. World Health Organization; Geneva; 2019;ISBN 978-92-4-151593-1. https://www.ilae.org/files/dmfile/19053_Epilepsy_A-public-health-imperative-For-Web.pdf
2. Kwan P, Brodie MJ. Early identification of refractory epilepsy. N Engl J Med. Feb 3 2000;342 (5):314-9. doi:10.1056/NEJM200002033420503
3. Chin JH. Epilepsy treatment in sub-Saharan Africa: closing the gap. Afr Health Sci. Jun 2012;12 (2):186-92. doi:10.4314/ahs.v12i2.17
4. Aliyu MH, Abdullahi AT, Iliyasu Z, et al. Bridging the childhood epilepsy treatment gap in northern Nigeria (BRIDGE): Rationale and design of pre-clinical trial studies. Contemp Clin Trials Commun. Sep 2019;15:100362.
doi:10.1016/j.conctc.2019.100362
5. Ngugi AK, Bottomley C, Kleinschmidt I, et al. Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: cross-sectional and case-control studies. Lancet Neurol. Mar 2013;12(3):253-63. doi:10.1016/S1474-4422 (13)70003-6
6. Ngugi AK, Bottomley C, Scott JA, et al. Incidence of convulsive epilepsy in a rural area in Kenya. Epilepsia. Aug 2013;54(8):1352-9. doi:10.1111/epi.12236
7. Meyer AC, Dua T, Ma J, Saxena S, Birbeck G. Global disparities in the epilepsy treatment gap: a systematic review. Bull World Health Organ. Apr 2010;88(4):260-6. doi:10.2471/BLT.09.064147
8. Kenya National Guidelines for the Management of Epilepsy: A Practical Guide for Healthcare Workers (2016).
9. Mbuba CK, Ngugi AK, Fegan G, et al. Risk factors associated with the epilepsy treatment gap in Kilifi, Kenya: a cross-sectional study. Lancet Neurol. Aug 2012;11(8):688-96. doi:10.1016/S1474-4422 (12)70155-2
10. Ibinda F, Odermatt P, Kariuki SM, et al. Magnitude and factors associated with nonadherence to antiepileptic drug treatment in Africa: A cross-sectional multisite study. Epilepsia Open. Jun 2017;2(2):226-235. doi:10.1002/epi4.12052
11. Patel AA, Wibecan L, Tembo O, Kalyelye P, Mathews M, Ciccone O. Improving paediatric epilepsy management at the first level of care: a pilot education intervention for clinical officers in Zambia. BMJ Open. Jul 24 2019;9(7):e029322. doi:10.1136/bmjopen-2019-029322
12. Patterson V. Managing Epilepsy by Telemedicine in Resource-Poor Settings. Front Public Health. 2019;7:321.
doi:10.3389/fpubh.2019.00321
13. Kim EJ, Fox S, Moretti ME, Turner M, Girard TD, Chan SY. Motivations and Barriers Associated With Physician Volunteerism for an International Telemedicine Organization. Front Public Health. 2019;7:224. doi:10.3389/fpubh.2019.00224
14. Chen L, Evans T, Anand S, et al. Human resources for health: overcoming the crisis. Lancet. Nov 27-Dec 3 2004;364(9449):1984-90. doi:10.1016/S0140-6736(04)17482-5
15. Birbeck GL, French JA, Perucca E, et al. Evidence-based guideline: Antiepileptic drug selection for people with HIV/AIDS: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Ad Hoc Task Force of the Commission on Therapeutic Strategies of the International League Against Epilepsy. Neurology. Jan 10 2012;78(2):139-45. doi:10.1212/WNL.0b013e31823efcf8
16. Menon S, Siewe Fodjo JN, Weckhuysen S, et al. Women with epilepsy in sub-Saharan Africa: A review of the reproductive health challenges and perspectives for management. Seizure. Oct 2019; 71:312-317. doi:10.1016/j.seizure.2019.08.016
17. Russell AJ, Macpherson H, Cairnie V, Brodie MJ. The care of pregnant women with epilepsy–a survey of obstetricians in Scotland. Seizure. Dec 1996;5(4):271-7. doi:10.1016/s1059-1311(96)80020-3
18. Kenya Health Workforce Report: The Status of Healthcare Professionals in Kenya, 2015 (2015).
19. Trevathan E. The Childhood Epilepsy Treatment Gap in Northern Nigeria. 2022:
20. Newton CR, Garcia HH. Epilepsy in poor regions of the world. Lancet. Sep 29 2012;380(984 8):1193-201. doi:10.1016/S0140-6736(12)61381-6
21. Sambo LGWHOROfA. The health of the people: what works: the African Regional Health Report 2014. 2014.
https://iris.who.int/handle/10665/137377
22. Okoroafor SC, Kwesiga B, Ogato J, et al. Investing in the health workforce in Kenya: trends in size, composition and distribution from a descriptive health labour market analysis. BMJ Glob Health. Aug 2022;7(Suppl 1) doi:10.1136/bmjgh-2022-009748
23. Birbeck GL. The health care workforce for epilepsy in resource-poor settings: what will work? What is realistic? Epilepsia. Sep 2008;49(9):1642-3. doi:10.1111/j.1528-1167.2008.01580_3.x
24. Abdulmalik J, Kola L, Fadahunsi W, et al. Country contextualization of the mental health gap action programme intervention guide: a case study from Nigeria. PLoS Med. Aug 2013;10(8):e1001501. doi:10.1371/journal.pmed.1001501
25. Aliyu MH, Blevins M, Audet CM, et al. Integrated prevention of mother-to-child HIV transmission services, antiretroviral therapy initiation, and maternal and infant retention in care in rural north-central Nigeria: a cluster-randomised controlled trial. Lancet HIV. May 2016;3(5):e202-11. doi:10.1016/S2352-3018(16)00018-7
26. Seidman G, Atun R. Does task shifting yield cost savings and improve efficiency for health systems? A systematic review of evidence from low-income and middle-income countries. Hum Resour Health. Apr 13 2017;15(1):29. doi:10.1186/s12960-017-0200-9
27. Gureje O, Abdulmalik J, Kola L, Musa E, Yasamy MT, Adebayo K. Integrating mental health into primary care in Nigeria: report of a demonstration project using the mental health gap action programme intervention guide. BMC Health Serv Res. Jun 21 2015;15:242. doi:10.1186/s12913-015-0911-3
28. Jacoby A. Epilepsy and stigma: an update and critical review. Curr Neurol Neurosci Rep. Jul 2008;8(4):339-44. doi:10.1007/s11910-008-0052-8
29. Carrizosa J, Braga P, Albuquerque M, et al. Epilepsy for primary health care: a cost-effective Latin American E-learning initiative. Epileptic Disord. Oct 1 2018;20(5):386-395. doi:10.1684/epd.2018.0997