

Factors Influencing Suicidal Ideation in Spiritist Individuals
A Cross-Sectional Study on Factors Related to Suicidal Ideation in Individuals with Spiritist Involvement: Comparison before and during the Covid-19 Pandemic
Tiago Medeiros Sales1, Rosa Maria Salani Mota2, Raimunda Hermelinda Maia Macena3
- Statistician and Professor in the Department of Statistics and Applied Mathematics at the Federal University of Ceará.
- Nurse and Professor in the Department of Physical Therapy and the Graduate Program in Public Health at the Faculty of Medicine of the Federal University of Ceará.
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Sales, TM., Mota, RMS., et al., 2024. A Cross-Sectional Study on Factors Related to Suicidal Ideation in Individuals with Spiritist Involvement: Comparison before and during the Covid-19 Pandemic. Medical Research Archives, [online] 12(11). https://doi.org/10.18103/mra.v12i11.6057
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.6057
ISSN 2375-1924
Abstract
Purpose: Suicide increases in Brazil annually and the population search for spiritual care, as in Spiritism, a religion that attracts people in psychic pain. We sought to identify the factors associated with suicidal ideation among persons with some Level of Spiritism Engagement (LSE), before and during COVID-19.
Methods: This cross-sectional analytical research with 848 inhabitants from Ceará, Brazil, with some LSE, was conducted through digital data collection via snowball, with a bivariate (p < 0,30), multivariate (p < 0,30) and multinomial analysis (p < 0,05) of sociodemographic factors, psychic status, psychic care, spiritual belief and LSE related to suicidal ideation. Afterward, a multinomial regression analysis (p < 0.05) was conducted on all significant factors to identify those most strongly associated with suicidal ideation.
Results: Risk factors of mild/moderate suicidal ideation were to be single (OR=2,32; CI 1,19-4,52), previous psychotherapy before COVID-19 (OR=1,81; CI 1,10-2,98) and to be spiritist (OR=2,43; CI 1,34-4,38). Risk factors of severe suicidal ideation were: to be single (OR=4,05; CI 1,89-8,69), unemployed (OR=2,93; CI 1,45-5,92), have a regular/bad/worse self-perception of emotional health (OR=4,84; CI 2,55-9,17), previous psychotherapy before COVID-19 (OR=2,57; CI 1,40-4,71) and to be spiritist (OR=2,13; CI 1,00-4,52). Pre-pandemic regular/high/very high LSE was a protective factor for severe suicidal ideation during COVID-19 (OR=0,38; CI 0,16-0,90).
Conclusion: Negative self-perception of emotional health, psychotherapeutic follow-up, and identification as spiritist were associated with severe suicidal ideation, which appears to support the notion that spiritism attracts individuals experiencing psychic distress. Despite this disease profile, higher levels of spiritist engagement before the pandemic were protective against severe suicidal ideation during COVID-19, suggesting a potential positive effect of spiritism on mental health.
Keywords
Suicidal Ideation, Spiritism, COVID-19, Suicide, Spirituality.
List of Abbreviations
ICPs = Integrative and Complementary Practices
LSE = Level of Spiritist Engagement
MAST = Multi Attitude Suicide Tendency Scale
NCH = National Council of Health
Introduction
Suicide is a challenge for public health. Suicidal ideation stands out and it means the thought of actively provoking the self-death. Underdeveloped and developing countries are the most vulnerable with 800.000 deaths / year around the world. Brazil’s suicide incidence grows annually, at a 6,36 persons by 100.000 inhabitants rate, mainly among youngsters and adults aged under 30 yrs. Suicidal ideation and suicide are closely associated with Common Mental Disorders (CMDs), a term coined by David Goldberg and Peter Huxley, which corresponds to the set of mental disorders most commonly found in the general population, such as insomnia, fatigue, somatizations, stress, anxiety, depression, among others. Among CMDs, anxiety, depression, and stress stand out, recognized for their high prevalence and high rate of comorbidities.
The Brazilian National Health System hardly tackles suicide, due to an ineffective promotion of the main preventing factor – the treatment of psychiatric disorders such as anxiety, stress, depression, and suicidal ideation. Consequently, the Brazilian population with almost 90% of Christians seeks for mental health care of religious origin. The use of spirituality as a health resource is a common practice of most societies, that fortify themselves through faith, benefit from social and personal care and from community help.
Previous studies show that spirituality is linked to better mental health, as it plays a significant role in enhancing psychological well-being. Spiritual practices offer social and emotional support, reduce stress, anxiety, and depression levels. Additionally, spirituality fosters greater psychological resilience, helping individuals cope with trauma and find purpose and meaning in life. It serves as a psychological resource to face mental and emotional challenges, ultimately contributing to improved overall quality of life and mental health. Recently, the benefit of spirituality on mental health was seen during COVID-19.
Regarding spirituality in Brazil, Spiritism is widely spread and is considered a scientific-philosophical doctrine, in addition to being a religion. It offers a free assistance system aimed at improving mental health, regardless of the religion of the individuals involved. Thus, many people in need of healthcare engage with Spiritist therapy, making Spiritism a religion of psychological demand. The specific mechanisms of how Spiritist engagement influences mental health may vary based on individual beliefs and spiritual practices. Despite this, scarce studies have sought to understand this phenomenon.
During the pandemic, there was an increase in mental health issues, including a rise in suicidal ideation, which possibly led to a higher level of Spiritist engagement. However, this engagement was affected by limited access to Spiritist centers due to the lockdown. Thus, COVID-19 created a time divide, altering parameters related to suicidal ideation as well as Spiritist engagement, even among individuals who already had some level of engagement before the pandemic. This study, conducted during the pandemic, aimed to determine the factors associated with suicidal ideation among people with some Level of Spiritist Engagement (LSE), comparing before and during COVID-19 periods.
Materials and Methods
STUDY DESIGN, SETTING AND PARTICIPANTS
This cross-sectional analytical research was conducted with persons with some LSE in the state of Ceara, Brazil. This study was conducted throughout the year 2021, during the second wave of COVID-19. Inclusion criteria adopted were: being 18 years old or older and being an inhabitant of the state of Ceara. A total of 848 people participated in this study, more than double the minimum required.
SAMPLE SIZE
Although the number of Spiritists in the Brazilian population is known to be 2% of the total, the sample of people with Spiritist engagement is unknown, as well as the prevalence of Common Mental Disorders (CMDs) and suicidal ideation in this population. Therefore, since the prevalence of the outcome (suicidal ideation) is unknown, a prevalence of 50% was assumed, and the sample size was calculated for a 5% alpha with 95% power, resulting in a total of 350 individuals. Considering an assumed loss of 10%, the minimum desired sample size was 385 individuals, including both Spiritists and non-Spiritists.
The non-probabilistic snowball sampling method was used, which allows for the identification of rare characteristics in large populations, with recruitment done through the participants themselves. The digital approach for data collection was chosen due to the restrictions imposed by social distancing measures as a public health response to COVID-19, which temporarily closed community and social settings and hindered in-person approach to Spiritists and attendees of Spiritist centers. As an advantage, digital data collection enables finding samples within an extensive community network, and therefore, digital data collection has progressively become a dominant research instrument. However, as a disadvantage, it increases the possibility of sample bias.
INSTRUMENTS
The Informed Written Consent term was available with a questionnaire and the selected suicide scale. The questionnaire had sociodemographic data, variables connected to the psychic status and to psychic care and structured questions to measure spiritual belief and LSE before and during the pandemic. The suicide scale was the Multi Attitude Suicide Tendency Scale (MAST).
LEVEL OF SPIRITIST ENGAGEMENT (LSE)
To elaborate LSE, different scores (0 – 2) were attributed to related questions, with different answer scores (1 – 6), according to their higher or lower level of connection with spiritism. The final result was estimated by the addition and classification on 5 categories – very low (0-20%), low (21-40%), regular (41-60%), high (61-80%) and very high (81-100%). These categories were subdivided into 2 – very low/low and regular/high/very high. The instrument was elaborated in 3 blocks of questions to measure Sociodemographic Data, Psychic Status and Psychic Care, and Spiritual Beliefs and LSE.
MULTI ATTITUDE SUICIDE TENDENCY SCALE (MAST)
To assess suicidal ideation the MAST was used, and the index of suicide risk was obtained by subtracting the subindex “death” (attraction minus death aversion), by the subindex “life” (attraction minus life aversion), which generated a minimum and a maximum value. For bivariate analysis, 3 levels of suicidal ideation were used (mild, moderate and severe) and 2 levels for multivariate and multinomial analysis (mild/moderate and severe). Was developed by Orbach in 1991 and originally consisted of 30 items. The MAST is based on the assumption that suicidal behavior evolves around a conflict between four types of attitudes towards life and death: death repulsion, life repulsion, death attraction, and life attraction. The adapted Brazilian version of MAST allows for a principal component factor analysis, with items having a factor loading greater than |0.40|. As a result, a reduced version composed of 20 items was proposed. For this study, the adapted reduced version for the Brazilian context was used.
The MAST contains 20 items that address content related to life and death, and thus assumes that the risk of suicide increases as a conflict arises between the desire to live and the possibility of death.
DATA COLLECTION
Digital collection was used due to social distancing that closed communities, including spiritist houses. This was advantageous because it allowed to access a small and specific sample among a wide community. However, the sample bias mounted, which was hampered by the snowball technique and complemented by the use of several digital platforms.
Instagram, Facebook and WhatsApp were chosen due to the enormous popularity. Digital pages of research were made available for the general public in Instagram and Facebook with data about the study and with the link to access software SurveyMonkey®, used for data collection. WhatsApp worked to spread information through individuals and groups with some LSE, that posted the informative invitation video and the links for Instagram, Facebook and SurveyMonkey®.
DATA ANALYSIS
To analyse data, SurveyMonkey® database was downloaded to Excel® for Windows 2013. After digital analysis, data was exported to SPSS® software, version 23.0 (SPSS, Inc, USA). A bivariate analysis of questionnaire data (sociodemographic factors, psychic status, psychic care, spiritual belief and LSE) was conducted associated to the index of suicide risk with a significance level up to 30%. After, a multivariate analysis with the same significance level was done, which originated data that was submitted to multinomial regression with a 5% significance. Finally, a multinomial regression analysis (p < 0.05) was performed on all significant factors associated with suicidal ideation, identifying the factors most strongly associated with suicidal ideation.
ETHICAL CONSIDERATIONS
The research met the Law 466/2012 of the National Council of Health (NCH), related to Research Ethics involving Human Beings, with approval of the Ethics Committee of the Federal University of Ceará (n. 2.237.838).
Results
SOCIODEMOGRAPHIC FACTORS
Considering the bivariate analysis with a significance level of 30%, the highest prevalence of severe suicidal ideation was observed in females (21.5%), younger individuals (29.7%), white individuals (21.2%), homosexuals (24.3%), singles (30.0%), those with low education (complete secondary school/incomplete higher school/technical – 29.3%), those with a daily workload greater than 8 hours (20.4%), those who were not the main household income providers (15.9%), and those with a low household monthly income (up to R$ 2.600.00 – 30.3%).
The multivariate analysis showed that being single (OR = 4.45; CI 2.30 – 8.60, p < 0.001), having the lowest education level (OR = 2.35; CI 1.26 – 4.39, p = 0.006), and having a lower family income (R$ 0 to R$ 2.600 – OR = 2.54; CI 1.24 – 5.02, p = 0.037) were associated with a higher risk of severe suicidal ideation. Conversely, being the main income provider was found to be a protective factor against severe suicidal ideation (OR = 0.54; CI 0.32 – 0.90, p = 0.037).
| Sociodemographic Factors | Levels of Suicidal Ideation | Related to Suicidal Ideation Level: | Mild / Moderate | Severe | p Value | OR¹ | 95% CI² | OR* | 95% CI² |
|---|---|---|---|---|---|---|---|---|---|
| Gender | n | % | |||||||
| Female | 494 | 82 | 16.6 | 306 | 61.9 | 106 | 21.5 | 0.926 | 0.586 1.463 |
| Male | 192 | 32 | 16.7 | 129 | 67.2 | 31 | 16.1 | 1.000 | – |
| Age | n | % | |||||||
| Between 18 and 34 years | 101 | 16 | 15.8 | 55 | 54.5 | 30 | 29.7 | 0.945 | 0.494 1.809 |
| Between 35 and 54 years | 340 | 54 | 15.9 | 220 | 64.7 | 66 | 19.4 | 1.120 | 0.716 1.752 |
| 55 years or over | 245 | 44 | 18.0 | 160 | 65.3 | 41 | 16.7 | 1.000 | – |
| Race | n | % | |||||||
| White | 345 | 58 | 16.8 | 214 | 62.0 | 73 | 21.2 | 1.123 | 0.459 2.747 |
| “Pardo” (Brown) | 304 | 49 | 16.1 | 198 | 65.1 | 57 | 18.8 | 1.230 | 0.499 3.031 |
| Others | 37 | 7 | 18.9 | 23 | 62.2 | 7 | 18.9 | 1.000 | – |
| Marital Status | n | % | |||||||
| Married or in a stable relationship | 401 | 85 | 21.2 | 251 | 62.6 | 65 | 16.2 | 1.000 | – |
| Single | 170 | 15 | 8.8 | 104 | 61.2 | 51 | 30.0 | 2.348 | 1.296 4.255 |
| Widower/Widow/ Divorced/ Separated | 115 | 14 | 12.2 | 80 | 69.6 | 21 | 18.3 | 1.935 | 1.042 3.593 |
| Education Level | n | % | |||||||
| Complete Secondary School /Incomplete Higher Education /Technical | 140 | 18 | 12.9 | 81 | 57.9 | 41 | 29.3 | 1.238 | 0.708 2.164 |
| Bachelor’s Degree/Graduation/Post-Graduation | 538 | 96 | 17.8 | 349 | 64.9 | 93 | 17.3 | 1.000 | – |
| Workload / Daily Workload | n | % | |||||||
| Up to 8 hours | 308 | 48 | 15.6 | 200 | 64.9 | 60 | 19.5 | 1.000 | – |
| 8 hours or more | 279 | 53 | 19.0 | 169 | 60.6 | 57 | 20.4 | 0.765 | 0.492 1.189 |
| None | 99 | 13 | 13.1 | 66 | 66.7 | 20 | 20.2 | 1.218 | 0.622 2.388 |
| Main Household Income Provider | 353 | 65 | 18.4 | 232 | 65.7 | 56 | 15.9 | 0.026 | 0.887 0.579 |
| Household Monthly Income | n | % | |||||||
| R$ 0 up to R$ 2.600 | 119 | 15 | 12.6 | 68 | 57.1 | 36 | 30.3 | 1.189 | 0.630 2.246 |
| R$ 2.601 up to R$ 7.800 | 262 | 46 | 17.6 | 165 | 63.0 | 51 | 19.5 | 0.941 | 0.603 1.469 |
| R$ 7.801 or more | 305 | 53 | 17.4 | 202 | 66.2 | 50 | 16.4 | 1.000 | – |
Sociodemographic factors that significantly influenced (p < 0.05) the shift in suicidal ideation were civil status and being the main household income provider. Single individuals had double the risk of severe suicidal ideation compared to widowers/widows/separated individuals. Being the main income provider was shown to be protective against the risk of severe suicidal ideation.
PSYCHIC STATUS
Bivariate analysis of psychic status with 30% significance showed that severe suicidal ideation was most prevalent in illicit drug users (87.5%) and in people’s self-harm (64.7%). Social distancing that affected very/totally emotional health prevailed in severe suicidal ideation (32.4%) than in those “noted “affected (10.6%), little (18.0%) or reasonably (21.3%). The self-perception of mental health as regular/bad/worse was more prevalent among individuals with severe suicidal ideation than in those who perceived themselves with good/excellent mental health (35.4% vs 9.0%).
Multivariate analysis, with a statistical significance < 30%, showed that severe suicidal ideation was the most found in unemployed (p < 0.001; OR = 3.88; CI 2.19 – 6.89) in relation to employed persons; individuals with physical disease (p = 0.002; OR = 2.81; CI 1.46 – 5.42) than those who were not affected; people in a marital crisis (p = 0.007; OR = 2.86; CI 1.28 – 6.37) than those not affected; alcohol /smoking users (p = 0.007; OR = 6.37; CI 1.41 – 28.66) than non-users; and victims of suffered violence (p = 0.015; OR = 3.07; CI 1.19 – 7.94) compared to those who did not suffer violence. During COVID-19, people that suffered reasonably with social distancing presented a higher risk of severe suicidal ideation (p = 0.002; OR = 2.82; CI 1.17 – 6.80) than those who were not affected; whereas those who were very/totally affected by social distancing had higher risk (p = 0.002; OR = 3.09; CI 1.24 – 7.67) when compared to those nothing affected. The self-perception of emotional health has shown that persons who perceived emotional health as regular/bad/worse had a higher risk (p < 0.001; OR = 6.07; CI 3.51 – 10.51) of severe suicidal ideation than those that perceived it as good/excellent.
| Psychic status factors | Levels of Suicidal Ideation | Related to Suicidal Ideation Level | Mild / Moderate | Severe | p Value | OR¹ | 95% CI² | OR¹ | 95% CI² |
|---|---|---|---|---|---|---|---|---|---|
| Unemployment | 201 | 22 | 10.9 | 113 | 56.2 | 66 | 32.8 | 0.000 | 1.468 0.879 2.449 |
| Physical disease | 134 | 15 | 11.2 | 78 | 58.2 | 41 | 30.6 | 0.002 | 1.442 0.795 2.616 |
| Close person’s disease | 247 | 36 | 14.6 | 154 | 62.3 | 57 | 23.1 | 0.245 | 1.187 0.764 1.846 |
| Mourning | 86 | 13 | 15.1 | 53 | 61.6 | 20 | 23.3 | 0.716 | 1.078 0.566 2.055 |
| Marital Crisis | 81 | 9 | 11.1 | 45 | 55.6 | 27 | 33.3 | 0.007 | 1.346 0.638 2.842 |
| Alcohol or smoking | 34 | 2 | 5.9 | 18 | 52.9 | 14 | 41.2 | 0.007 | 2.417 0.553 10.573 |
| Illicit Drugs | 8 | 0 | 0.0 | 1 | 12.5 | 7 | 87.5 | – | – |
| Suffered Violence | 57 | 6 | 10.5 | 31 | 54.4 | 20 | 35.1 | 0.015 | 1.381 0.562 3.396 |
| Violence Committed | 14 | 1 | 7.1 | 7 | 50.0 | 6 | 42.9 | – | – |
| Self-harm | 34 | 0 | 0.0 | 12 | 35.3 | 22 | 64.7 | 0.000 | – |
| Social Distancing affecting Emotional Health | 0.002 | Nothing | 104 | 21 | 20.2 | 72 | 69.2 | 11 | 10.6 |
| A little | 289 | 45 | 15.6 | 192 | 66.4 | 52 | 18.0 | 1.244 | 0.694 2.233 |
| Reasonable | 188 | 27 | 14.4 | 121 | 64.4 | 40 | 21.3 | 1.307 | 0.689 2.480 |
| Very/ Totally | 105 | 21 | 20.0 | 50 | 47.6 | 34 | 32.4 | 0.694 | 0.343 1.404 |
| Self-perception of Emotional Health status | 0.000 | Good / Excellent | 401 | 78 | 19.5 | 287 | 71.6 | 36 | 9.0 |
| Regular / Bad / Worse | 285 | 36 | 12.6 | 148 | 51.9 | 101 | 35.4 | 1.117 | 0.718 1.738 |
Psychic factors that significantly influenced suicidal ideation at a 5% significance level were: unemployment and self-perception of emotional health. Unemployed presented a higher risk (OR = 2.53; CI 1.38 – 4.62) of severe suicidal ideation than the employed individuals; regular/bad/worse self-perception of emotional health presented a higher risk (OR = 4.83; CI 2.74 – 8.51) of severe suicidal ideation when comparing to the individuals who perceived their own emotional health as good/excellent.
PSYCHIC CARE
When comparing severe suicidal ideation before and during the pandemic, bivariate analysis with approximately 30% significance related to psychic care showed that psychiatric follow-up decreased from 32.0% to 31.4%; the diagnosis of psychiatric disorders increased from 35.5% to 42.1%; the use of psychiatric drugs in general increased for psychiatric disorders, from 27.7% to 30.5%, and for non-psychiatric diseases, from 27.6% to 33.3%. Severe suicidal ideation was reported by 25.4% of individuals attending psychotherapy before the pandemic and 24.7% during the pandemic, while 21.8% were treated with Integrative and Complementary Practices (ICPs) before the pandemic and 19.5% during the pandemic.
Multivariate analysis with a statistical significance level of < 30% for psychiatric care before the pandemic indicated that severe suicidal ideation was higher among individuals with psychiatric follow-up (p < 0.001; OR = 3.05; CI 1.69 – 5.52), those diagnosed with psychiatric disorders (p < 0.001; OR = 3.67; CI 1.92 – 7.01), users of psychiatric drugs for psychiatric disorders (at least once) (p < 0.001; OR = 2.88; CI 1.67 – 4.97), and users of psychiatric drugs for non-psychiatric diseases (p = 0.026; OR = 1.82; CI 1.18 – 2.80). During the pandemic, severe suicidal ideation was higher among individuals with psychiatric follow-up (p = 0.002; OR = 2.98; CI 1.49 – 5.93), those diagnosed with psychiatric disorders (p < 0.001; OR = 7.42; CI 3.01 – 18.27), users of psychiatric drugs for psychiatric disorders (p = 0.002; OR = 2.31; CI 1.28 – 4.17), and users of psychiatric drugs for non-psychiatric diseases (p = 0.003; OR = 2.59; CI 1.26 – 5.30). Severe suicidal ideation before the pandemic was higher among individuals undergoing psychotherapy (p < 0.001; OR = 3.10; CI 1.82 – 5.26) and those receiving Integrative and Complementary Practices (ICPs) (p = 0.023; OR = 1.93; CI 1.13 – 3.31), while during the pandemic, it was higher among individuals with active psychotherapy follow-up (p = 0.036; OR = 2.21; CI 1.19 – 4.07) compared to those without follow-up.
| Psychic Care factors before and during COVID-19 | Levels of Suicidal Ideation | Related to Suicidal Ideation Level | Mild / Moderate | Severe | p Value | OR¹ | 95% CI² | OR¹ | 95% CI² |
|---|---|---|---|---|---|---|---|---|---|
| Psychiatric follow-up | 172 | 20 | 11.8 | 95 | 56.2 | 54 | 32.0 | 0.000 | 1.313 0.770 2.239 |
| Psychiatric Disorder | 141 | 15 | 10.9 | 74 | 53.6 | 49 | 35.5 | 0.000 | 1.353 0.744 2.460 |
| Psychiatric drugs for psychiatric disorder | 0.000 | Never | 427 | 80 | 18.7 | 286 | 67.0 | 61 | 14.3 |
| Yes, at least once | 238 | 30 | 12.6 | 142 | 59.7 | 66 | 27.7 | 1.324 | 0.831 2.109 |
| Psychiatric drugs for non-psychiatric disease | 154 | 25 | 16.4 | 85 | 55.9 | 42 | 27.6 | 0.026 | 1.157 0.699 1.913 |
| Psychiatric follow-up | 121 | 13 | 10.7 | 70 | 57.9 | 38 | 31.4 | 0.002 | 1.490 0.792 2.802 |
| Psychiatric disorder | 95 | 6 | 6.3 | 49 | 51.6 | 40 | 42.1 | 0.000 | 2.285 0.953 5.477 |
| Psychiatric drugs for psychiatric disorder | 154 | 21 | 13.6 | 86 | 55.8 | 47 | 30.5 | 0.002 | 1.091 0.643 1.852 |
| Psychiatric drugs for non-psychiatric disease | 98 | 12 | 12.5 | 52 | 54.2 | 32 | 33.3 | 0.003 | 1.154 0.594 2.243 |
| Psychotherapy | 304 | 32 | 10.8 | 188 | 63.7 | 75 | 25.4 | 0.000 | 1.950 1.243 3.060 |
| Integrative and Complementary Practices (ICPs) | 264 | 30 | 11.7 | 171 | 66.5 | 56 | 21.8 | 0.023 | 1.814 1.146 2.870 |
| Psychotherapy | 174 | 19 | 11.2 | 109 | 64.1 | 42 | 24.7 | 0.036 | 1.672 0.976 2.864 |
| Integrative and Complementary Practices (ICPs) | 162 | 21 | 13.2 | 107 | 67.3 | 31 | 19.5 | 0.387 | 1.445 0.858 2.433 |
Factors of psychic care that greatly influenced (p < 0,05) suicidal ideation were: the use of psychiatric drugs for psychiatric disorders at least once before the pandemic, which presented a higher risk (OR = 2.25; CI 1.27 – 3.97) of severe suicidal ideation when compared to individuals who had never used this kind of medication; and psychotherapy follow-up before the pandemic, with a discreet higher risk (OR = 2.08; CI 1.28 – 3.36) on mild/moderate suicidal ideation and higher risk (OR=2.50; CI 1.41-4.42) on severe suicidal ideation if compared to people without follow-up.
SPIRITUAL BELIEF
Bivariate analysis with a significance level up to 30% has shown a higher prevalence of moderate suicidal ideation among individuals who classified themselves as spiritists (67.9%), those who reported a reasonable/high/very high preference for spiritism (66.8%), those with regular/high/very high levels of spiritual engagement (LSE) pre-pandemic (74.1%) and during the pandemic (73.4%), and those working in spiritist houses, including Public Lectures (62.3%), Spiritual Care (66.3%), and Charity/Volunteering (82.3%). On the other hand, the higher prevalence of severe suicidal ideation was observed among agnostics (46.2%), individuals with very low/low LSE pre-pandemic (21.2%) and during the pandemic (21.3%), and those who sought spiritism due to mental pain (26.1%).
Multivariate analysis with a significance level of up to 30% has shown that self-classification as Catholic is a protective factor against both mild/moderate suicidal ideation (p = 0.001; OR = 0.41; CI 0.26 – 0.65) and severe suicidal ideation (p = 0.001; OR = 0.48; CI 0.27 – 0.83). In contrast, individuals who self-classified as Spiritists presented a higher risk of mild/moderate suicidal ideation (p < 0.001; OR = 3.19; CI 2.00 – 5.08). A strong preference for Spiritism, rated as reasonable/very/totally, was associated with a higher risk of mild/moderate suicidal ideation (p < 0.001; OR = 3.23; CI 1.93 – 5.41). Regular/high/very high LSE before the pandemic was revealed as a protective factor, reducing the risk of severe ideation (p = 0.015; OR = 0.42; CI 0.19 – 0.96). Seeking Spiritism due to mental pain was associated with a higher risk of severe suicidal ideation (p = 0.034; OR = 2.11; CI 1.11 – 3.99). Engagement in Public Lectures reduced the risk of both mild/moderate suicidal ideation (p = 0.019; OR = 0.37; CI 0.18 – 0.75) and severe ideation (p = 0.019; OR = 0.33; CI 0.12 – 0.93). Similarly, working in Spiritual Care reduced the risk of both mild/moderate suicidal ideation (p = 0.039; OR = 0.44; CI 0.22 – 0.83) and severe ideation (p = 0.039; OR = 0.37; CI 0.15 – 0.93).
| Spiritual Belief factors | Levels of Suicidal Ideation | Related to Suicidal Ideation Level | Mild / Moderate | Severe | p Value | OR¹ | 95% CI² | OR¹ | 95% CI² |
|---|---|---|---|---|---|---|---|---|---|
| Self-classified Religiousness | Without religion | 26 | 5 | 19.2 | 9 | 34.6 | 12 | 46.2 | 0.002 |
| Agnostic | 10 | 2 | 20.0 | 2 | 20.0 | 6 | 60.0 | – | – |
| Evangelist | 29 | 7 | 24.1 | 13 | 44.8 | 9 | 31.0 | 0.079 | – |
| Africa-Derived Religion | 38 | 5 | 13.2 | 24 | 63.2 | 9 | 23.7 | 0.761 | – |
| Catholic | 157 | 42 | 26.8 | 85 | 54.1 | 30 | 19.1 | 0.001 | 0.416 0.266 0.652 |
| Spiritist | 545 | 73 | 13.4 | 370 | 67.9 | 102 | 18.7 | 0.000 | 3.197 2.009 5.087 |
| Preference for Spiritism | None / A little | 102 | 31 | 30.4 | 45 | 44.1 | 26 | 25.5 | 1.000 |
| Reasonable / Very / Totally | 584 | 83 | 14.2 | 390 | 66.8 | 111 | 19.0 | 3.237 | 1.934 5.418 |
| Level of Spiritist Engagement before COVID-19 | Very low / Low | 523 | 78 | 14.9 | 334 | 63.9 | 111 | 21.2 | 1.000 |
| Regular / High / Very high | 112 | 18 | 16.1 | 83 | 74.1 | 11 | 9.8 | 1.077 | 0.611 1.897 |
| Level of Spiritist Engagement during COVID-19 | Very low / Low | 607 | 101 | 16.6 | 377 | 62.1 | 129 | 21.3 | 1.000 |
| Regular / High / Very high | 79 | 13 | 16.5 | 58 | 73.4 | 8 | 10.1 | 1.195 | 0.630 2.267 |
| Motivation to search for the spiritist doctrine | Origin / familial influence | 102 | 16 | 15.7 | 63 | 61.8 | 23 | 22.5 | 0.570 |
| Friends/socio-familial influence | 141 | 20 | 14.2 | 91 | 64.5 | 30 | 21.3 | 0.770 | |
| Curiosity | 203 | 34 | 16.7 | 131 | 64.5 | 38 | 18.7 | 0.747 | |
| Mental pain | 153 | 18 | 11.8 | 95 | 62.1 | 40 | 26.1 | 0.034 | |
| Self-reported mediumship | 126 | 15 | 11.9 | 84 | 66.7 | 27 | 21.4 | 0.489 | |
| Scientific/philosophical interest | 228 | 31 | 13.6 | 163 | 71.5 | 34 | 14.9 | 0.056 | |
| Necessity/ familial pain | 25 | 7 | 28.0 | 15 | 60.0 | 3 | 12.0 | 0.173 | |
| Worker/facilitator in the spiritist centre | 288 | 42 | 14.6 | 205 | 71.2 | 41 | 14.2 | 0.046 | |
| Public Lecture | 61 | 16 | 26.2 | 38 | 62.3 | 7 | 11.5 | 0.019 | |
| Spiritual Care | 101 | 22 | 21.8 | 67 | 66.3 | 12 | 11.9 | 0.039 | |
| Systematic study of Spiritist doctrine | 122 | 19 | 15.6 | 86 | 70.5 | 17 | 13.9 | 0.929 | |
| Mediumship studies | 94 | 14 | 14.9 | 67 | 71.3 | 13 | 13.8 | 1.000 | |
| Fraternal service | 62 | 10 | 16.1 | 42 | 67.7 | 10 | 16.1 | 0.767 | |
| Fluidotherapy (magnetised/fluidic water) | 66 | 8 | 12.1 | 51 | 77.3 | 7 | 10.6 | 0.489 | |
| Mediumship meeting | 142 | 21 | 14.8 | 103 | 72.5 | 18 | 12.7 | 1.000 | |
| Charity/ volunteering | 62 | 6 | 9.7 | 51 | 82.3 | 5 | 8.1 | 0.096 | |
| Administrative role | 78 | 12 | 15.4 | 57 | 73.1 | 9 | 11.5 | 0.761 |
Spiritual belief factors with 5% significance have demonstrated that the meaningfully influenced suicidal ideation were spiritist self-classification and pre-pandemic LSE. The former presented a higher risk of mild/moderate suicidal ideation (OR = 2.52; CI 1.42 – 4.47); whereas regular/high/very high LSE before the pandemic was a protective factor, with lower risk (OR = 0.37; CI 0.16 – 0.85) of severe suicide ideation.
MULTINOMIAL REGRESSION: ALL THE FACTORS
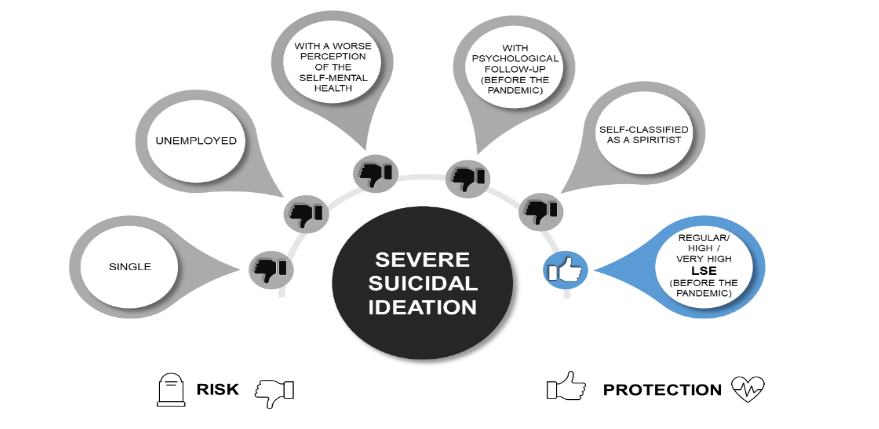
Multinomial regression analysis of all significantly factors associated to suicidal ideation indicated that to be single presented a higher risk of mild/moderate suicidal ideation (OR = 2.32; CI 1.19 – 4.52) and severe (OR = 4.05; CI 1.89 – 8.69). Unemployment has displayed a higher risk (OR = 2.93; CI 1.45 – 5.92) of severe suicidal ideation. Pre-COVID-19 follow-up was associated with mild/moderate suicidal ideation (OR = 1.81; CI 1.10 – 2.98) and showed a higher risk (OR = 2.57; CI 1.40 – 4.71) of severe ideation. The same happened to the spiritist self-classification that showed higher risk (OR = 2.43; CI 1.34 – 4.38) for mild/moderate suicidal ideation and higher risk (OR = 2.13; CI 1.00 – 4.52) for severe ideation. The only protection factor of high significance was pre-COVID-19 regular/high/very high LSE with lower risk (OR=0.38; CI 0.16-0.90) for severe ideation.
| Suicidal Ideation Factors | Related to Suicidal Ideation Level | Mild / Moderate | Severe | OR¹ | 95% CI² | OR¹ | 95% CI² |
|---|---|---|---|---|---|---|---|
| Civil Status | Married or in a stable relationship | 1.000 | – | 1.000 | – | ||
| Single | 2.358 | 1.252 4.441 | 4.242 | 2.099 8.571 | |||
| Widower/ Widow / Divorced/ Separated | 2.036 | 1.081 3.835 | 2.253 | 1.036 4.900 | |||
| Main Household Income Provider | 0.814 | 0.525 1.262 | 0.501 | 0.293 0.857 |
Discussion
SOCIODEMOGRAPHIC FACTORS
Sociodemographic data indicated that the absence of a steady relationship was associated with suicidal ideation, which was higher among single individuals compared to those who had lost their partners. Single individuals had twice the chance of experiencing mild to moderate suicidal ideation, and this risk doubled for severe suicidal ideation. Individuals with low education had a higher probability of suicidal ideation. Being the main income provider had a protective effect against severe suicidal ideation, while individuals with lower household income were at a higher risk. However, the multinomial analysis of sociodemographic factors revealed that only the absence of a steady relationship was a risk factor, while being the main income provider was a protective factor.
Not being in a steady relationship and living alone have already been listed as relevant aspects for suicide, regardless of the culture. In Brazil, this trend is corroborated by regional data, as in Pernambuco, where more than 400 women legally separated committed suicide between 2013 and 2017; and in Ceará, divorce is linked to suicide, as over the double of national data. Low education has already been connected to suicide in Brazil, e.g., in Curitiba, where people with mental disorders and with education between 0 and 8 years (p = 0.016), or 9 and 12 (p = 0.013) were significantly associated to suicide. Similarly, persons holding 4 to 7 years of education presented the highest prevalence of suicide in Goiás, from 2009 to 2014, as well as in Ceará, from 2015 to 2017. In fact, more than half of Ceará’s inhabitants have not completed the elementary or secondary school.
Indeed, poverty raises the risk of mental disorders worldwide. In Brazil, the quintile of the population with the lowest income presented a 2 to 5 times higher risk of mental disorder, and who was born in a poor family or has impoverished after childhood have a higher risk to try suicide. In Ceará, low income was identified as one of the factors most connected to suicide, and more than half of this population has an income less than 1 minimum salary (up to R$ 1.046,00), which makes visible the state’s vulnerability. In parallel, to be the main household income provider, regardless of the value, has a lower risk for suicide due to parenthood and also family relationships are a protective factor for suicide, which is in line with the current study.
PSYCHIC STATUS
Bivariate analysis of psychic status with 30% significance showed that severe suicidal ideation was most prevalent in illicit drug users (87.5%) and in people’s self-harm (64.7%). Social distancing that affected very/totally emotional health prevailed in severe suicidal ideation (32.4%) than in those “noted” affected (10.6%), little (18.0%) or reasonably (21.3%). The self-perception of mental health as regular/bad/ worse was more prevalent among individuals with severe suicidal ideation than in those who perceived themselves with good/excellent mental health (35.4% vs 9.0%) (TABLE 3).
Multivariate analysis, with a statistical significance < 30%, showed that severe suicidal ideation was the most found in unemployed (p < 0.001; OR = 3.88; CI 2.19 – 6.89) in relation to employed persons; individuals with physical disease (p = 0.002; OR = 2.81; CI 1.46 – 5.42) than those who were not affected; people in a marital crisis (p = 0.007; OR = 2.86; CI 1.28 – 6.37) than those not affected; alcohol /smoking users (p = 0.007; OR = 6.37; CI 1.41 – 28.66) than non-users; and victims of suffered violence (p = 0.015; OR = 3.07; CI 1.19 – 7.94) compared to those who did not suffer violence. During COVID-19, people that suffered reasonably with social distancing presented a higher risk of severe suicidal ideation (p = 0.002; OR = 2.82; CI 1.17 – 6.80) than those who were not affected; whereas those who were very/totally affected by social distancing had higher risk (p = 0.002; OR = 3.09; CI 1.24 – 7.67) when compared to those nothing affected. The self-perception of emotional health has shown that persons who perceived emotional health as regular/bad/worse had a higher risk (p < 0.001; OR = 6.07; CI 3.51 – 10.51) of severe suicidal ideation than those that perceived it as good/excellent (TABLE 3).
Table 3 – Bivariate and multivariate analysis of factors related to psychic status connected to suicidal ideation levels of people with spiritist engagement in the state of Ceará. Fortaleza/CE, 2022.
| Psychic status factors | Levels of Suicidal Ideation | Related to Suicidal Ideation Level |
|---|---|---|
| Mild | Moderate | |
| N | n | |
| Unemployment | 201 | 22 |
| Physical disease | 134 | 15 |
| Close person’s disease | 247 | 36 |
| Mourning | 183 | 13 |
| Marital Crisis | 81 | 9 |
| Alcohol or smoking | 47 | 5 |
| Illicit Drugs | 8 | 0 |
| Suffered Violence | 57 | 6 |
| Violence Committed | 14 | 1 |
| Self-harm | 34 | 0 |
| Social Distancing affecting Emotional Health | ||
| Nothing | 104 | 20 |
| A little | 289 | 45 |
| Reasonable | 187 | 26 |
| Very / Totally | 105 | 21 |
| Self-perception of Emotional Health Status | ||
| Good / Excellent | 401 | 78 |
| Regular / Bad / Worse | 285 | 36 |
Source: Author(s) (2022)
¹Odds Ratio, ²Confidence Interval, ³Lower Limit, ⁴Upper Limit
Factors that significantly influenced suicidal ideation at a 5% significance level were: unemployment and self-perception of emotional health. Unemployed presented a higher risk (OR = 2.53; CI 1.38 – 4.62) of severe suicidal ideation than the employed individuals; regular/bad/worse self-perception of emotional health presented a higher risk (OR = 4.83; CI 2.74 – 8.51) of severe suicidal ideation when comparing to those individuals who perceived their own emotional health as good/excellent (TABLE 4).
Table 4 – Multinomial regression of psychic status associated with levels of suicidal ideation of people with spiritist engagement in the state of Ceará. Fortaleza/CE, 2022.
| Psychic status | Related to Suicidal Ideation Level |
|---|---|
| Mild / Moderate | |
| OR¹ | |
| LL³ | |
| Unemployment | 1.456 |
| Self-perception of Emotional Health | |
| Good / Excellent | 1.000 |
| Regular / Bad / Worse | 1.028 |
Source: Author(s) (2022)
¹Odds Ratio, ²Confidence Interval, ³Lower Limit, ⁴Upper Limit
PSYCHIC CARE
When comparing severe suicidal ideation before and during the pandemic, bivariate analysis with approximately 30% significance related to psychic care showed that psychiatric follow-up decreased from 32.0% to 31.4%; the diagnosis of psychiatric disorders increased from 35.5% to 42.1%; the use of psychiatric drugs in general increased for psychiatric disorders, from 27.7% to 30.5%, and for non-psychiatric diseases, from 27.6% to 33.3%. Severe suicidal ideation was reported by 25.4% of individuals attending psychotherapy before the pandemic and 24.7% during the pandemic, while 21.8% were treated with Integrative and Complementary Practices (ICPs) before the pandemic and 19.5% during the pandemic (TABLE 5).
Multivariate analysis with a statistical significance level of < 30% for psychiatric care before the pandemic indicated that severe suicidal ideation was higher among individuals with psychiatric follow-up (p < 0.001; OR = 3.05; CI 1.69 – 5.52), those diagnosed with psychiatric disorders (p < 0.001; OR = 3.67; CI 1.92 – 7.01), users of psychiatric drugs for psychiatric disorders (at least once) (p < 0.001; OR = 2.88; CI 1.67 – 4.97), and users of psychiatric drugs for non-psychiatric ones (p = 0.026; OR = 1.82; CI 1.118 – 2.80). During the pandemic, severe suicidal ideation was higher among individuals with psychiatric follow-up (p = 0.002; OR = 2.98; CI 1.49 – 5.93), those diagnosed with psychiatric disorders (p < 0.001; OR = 7.42; CI 3.01 – 18.27), users of psychiatric drugs psychiatric drugs for psychiatric disorders (p = 0.002; OR = 2.31; CI 1.28 – 4.17), and users of psychiatric drugs for non-psychiatric diseases (p = 0.003; OR = 2.59; CI 1.26 – 5.30). Severe suicidal ideation before the pandemic was higher among individuals undergoing psychotherapy (p < 0.001; OR = 3.10; CI 1.82 – 5.26) and those receiving Integrative and Complementary Practices (ICPs) (p = 0.023; OR = 1.93; CI 1.13 – 3.31), while during the pandemic, it was higher among individuals with active psychotherapy follow-up (p = 0.036; OR = 2.21; CI 1.19 – 4.07) compared to those without follow-up (TABLE 5).
Table 5 – Bivariate and multivariate analysis of factors associated with psychic care before and during COVID-19 connected to suicidal ideation levels of people with spiritist engagement in the state of Ceará. Fortaleza/CE, 2022.
| Psychic Care factors before and during COVID-19 | Levels of Suicidal Ideation | Related to Suicidal Ideation Level |
|---|---|---|
| Mild | Moderate | |
| N | n | |
| Psychiatric Care before COVID-19 | ||
| Psychiatric follow-up | 172 | 20 |
| Psychiatric Disorder | 141 | 15 |
| Psychiatric drugs for psychiatric disorder | ||
| Never | 427 | 80 |
| Yes, at least once | 238 | 30 |
| Psychiatric drugs for non-psychiatric disease | 154 | 26 |
| Psychiatric Care during COVID-19 | ||
| Psychiatric follow-up | 121 | 13 |
| Psychiatric disorder | 95 | 6 |
| Psychiatric drugs for psychiatric disorder | 154 | 21 |
| Psychiatric drugs for non-psychiatric disease | 98 | 12 |
| Non-medical assistance before COVID-19 | ||
| Psychotherapy | 304 | 32 |
| Integrative and Complementary Practices (ICPs) | 264 | 30 |
| Non-medical assistance during COVID-19 | ||
| Psychotherapy | 220 | 21 |
| Integrative and Complementary Practices (ICPs) | 162 | 21 |
Source: Author(s) (2022)
¹Odds Ratio, ²Confidence Interval, ³Lower Limit, ⁴Upper Limit
Factors of psychic care that greatly influenced (p < 0.05) suicidal ideation were: the use of psychiatric drugs for psychiatric disorders at least once before the pandemic, which presented a higher risk (OR = 2.25; CI 1.27 – 3.97) of severe suicidal ideation when compared to individuals who had never used this kind of medication; and psychotherapy follow-up before the pandemic, with a discreet higher risk (OR = 2.08; CI 1.28 – 3.36) on mild/moderate suicidal ideation and higher risk (OR = 2.50; CI 1.41 – 4.42) on severe suicidal ideation if compared to people without follow-up (TABLE 6).
Table 6 – Multinomial regression of psychic care associated with levels of suicidal ideation of people with spiritist engagement in the state of Ceará. Fortaleza/CE, 2022.
| Psychic care | Related to Suicidal Ideation Level |
|---|---|
| Mild / Moderate | |
| OR¹ | |
| LL³ | |
| Psychic Care before and during COVID-19 | |
| Psychiatric drugs for psychiatric disorder (before COVID-19) | |
| Never | 1.000 |
| Yes, at least once | 1.089 |
| Psychotherapy follow-up (before COVID-19) | 2.081 |
Source: Author(s) (2022)
¹Odds Ratio, ²Confidence Interval, ³Lower Limit, ⁴Upper Limit
SPIRITUAL BELIEF
Bivariate analysis with a significance level up to 30% has shown a higher prevalence of moderate suicidal ideation among individuals who classified themselves as spiritists (67.9%), those who reported a reasonable/high/very high preference for spiritism (66.8%), those with regular/high/very high levels of spiritual engagement (LSE) pre-pandemic (74.1%) and during the pandemic (73.4%), and those working in spiritist houses, including Public Lectures (62.3%), Spiritual Care (66.3%), and Charity/Volunteering (82.3%). On the other hand, the higher prevalence of severe suicidal ideation was observed among agnostics (46.2%), individuals with very low/low LSE pre-pandemic (21.2%) and during the pandemic (21.3%), and those who sought spiritism due to mental pain (26.1%) (TABLE 7).
Table 8 – Multinomial regression of spiritual belief associated with levels of suicidal ideation of people with spiritist engagement in the state of Ceará. Fortaleza/CE, 2022.
| Spiritual belief | Related to Suicidal Ideation Level |
|---|---|
| Mild / Moderate | |
| OR¹ | |
| LL³ | |
| Self-classified Religiousness — Spiritism | 2.431 |
| Level of Spiritist Engagement before COVID-19 | |
| Very low / Low | 1.000 |
| Regular / High / Very high | 0.908 |
Source: Author(s) (2022)
¹Odds Ratio, ²Confidence Interval, ³Lower Limit, ⁴Upper Limit
MULTINOMIAL REGRESSION: ALL THE FACTORS
Multinomial regression analysis of all significantly factors associated to suicidal ideation indicated that to be single presented a higher risk of mild/moderate suicidal ideation (OR = 2.32; CI 1.19 – 4.52) and severe (OR = 4.05; CI 1.89 – 8.69). Unemployment has displayed a higher risk (OR = 2.93; CI 1.45 – 5.92) of severe suicidal ideation. Pre-COVID-19 follow-up was associated with mild/moderate suicidal ideation (OR = 1.81; CI 1.10 – 2.98) and showed a higher risk (OR = 2.57; CI 1.40 – 4.71) of severe ideation. The same happened to the spiritist self-classification that showed higher risk (OR = 2.43; CI 1.34 – 4.38) for mild/moderate suicidal ideation and higher risk (OR = 2.13; CI 1.00 – 4.52) for severe ideation. The only protection factor of high significance was pre-COVID-19 regular/high/very high LSE with lower risk (OR = 0.38; CI 0.16–0.90) for severe ideation (TABLE 9).
Table 9 – Multinomial regression of all significantly factors associated to suicidal ideation of people with spiritist engagement in the state of Ceará. Fortaleza/CE, 2022.
| Suicidal Ideation Factors | Related to Suicidal Ideation Level |
|---|---|
| Mild / Moderate | |
| OR¹ | |
| LL³ | |
| Civil Status | |
| Married or in a stable relationship | 1.000 |
| Single | 2.321 |
| Widower/Widow/Divorced/Separated | 1.923 |
| Unemployment | 1.750 |
| Self-perception of Emotional Health status | |
| Good / Excellent | 1.000 |
| Regular / Bad / Worse | 1.031 |
| Psychotherapy follow-up before COVID-19 | 1.812 |
| Self-classified Religiousness — Spiritism | 2.431 |
| Level of Spiritist Engagement before COVID-19 | |
| Very low / Low | 1.000 |
| Regular / High / Very high | 0.908 |
Source: Author(s) (2022)
¹Odds Ratio, ²Confidence Interval, ³Lower Limit, ⁴Upper Limit
Discussion
SOCIODEMOGRAPHIC FACTORS
Sociodemographic data indicated that the absence of a steady relationship was associated with suicidal ideation, which was higher among single individuals compared to those who had lost their partners. Single individuals had twice the chance of experiencing mild to moderate suicidal ideation, and this risk doubled for severe suicidal ideation. Individuals with low education had a higher probability of suicidal ideation. Being the main income provider had a protective effect against severe suicidal ideation, while individuals with lower household income were at a higher risk. However, the multinomial analysis of sociodemographic factors revealed that only the absence of a steady relationship was a risk factor, while being the main income provider was a protective factor.
Not being in a steady relationship and living alone also increased poverty rates, which in turn raised the risk of mental disorders and suicide attempts. In Ceará, low income was identified as one of the main factors connected to suicide, as more than half of this population earns less than one minimum salary (up to R$ 1,046.00), increasing the state’s vulnerability. In parallel, being the main household income provider, regardless of value, has a lower risk for suicide due to parenthood, and family relationships are a protective factor, in line with this study.
PSYCHIC STATUS
During the pandemic, emotional health was impacted by unemployment, physical disease, the use of alcohol and/or smoking, and social distancing that affected mental health. The self-perception of mental health as regular/bad/worse also triggered severe suicidal ideation. Only unemployment and poor self-perception of emotional health significantly contributed to the development of suicidal ideation.
Emotional pain and suicide were associated with physical disease, especially in the elderly. The use of illicit drugs and alcohol increased the risk of injury and suicide (including self-inflicted), and both were strongly linked to suicidal ideation, suicide attempt (OR = 3.13), and completed suicide (OR = 2.59). Social distancing, even alone, was associated with active and passive suicidal ideation, representing a “second pandemic” due to its mental health impact.
Unemployment caused emotional pain, one of the strongest predictors of suicide. In the U.S., job loss was the second main cause of mental disorder during the pandemic. In Ceará, unemployment doubled the risk of suicide compared to the rest of Brazil.
PSYCHIC CARE
Before the pandemic, psychiatric disorders, medication use, and psychotherapy follow-up were substantially associated with severe suicidal ideation. These remained relevant during COVID-19. Multinomial analysis showed that only the use of psychiatric drugs for psychiatric disorders and psychotherapy follow-up increased the risk of severe suicidal ideation.
The analysis confirmed that severe suicidal ideation was higher among individuals undergoing psychiatric follow-up before COVID-19. This group had a higher prevalence of psychiatric disorders and treatment compared to the general population, possibly due to better access to care through private means.
SPIRITUAL BELIEF
Self-declared spiritists and those who preferred Spiritism showed a higher risk of mild and moderate suicidal ideation, whereas self-classified Catholics showed protective effects. Those who sought Spiritism due to mental pain had higher suicidal risks, while those active in public lectures or spiritual care roles had lower risks.
Before COVID-19, high spiritual engagement (LSE) and Catholic self-identification were protective against suicidal ideation.
LIMITATIONS AND FUTURE RESEARCH
Despite significant findings, causal relationships could not be fully established because the study was cross-sectional. Future longitudinal research is needed to explore the impact of Spiritist engagement on mental health, its potential protective or aggravating effects, and subjective experiences related to spirituality and psychological resilience.
Conclusion
Individuals with Spiritist engagement at risk of having mild/moderate suicidal ideation were single, unemployed, receiving psychotherapy before COVID-19, and self-classified as Spiritists. Severe suicidal ideation was associated with unemployment and poor self-perception of emotional health.
A higher level of spiritual engagement before the pandemic proved to be a relevant protective factor against suicidal ideation during COVID-19.
Although Spiritism may attract individuals with psychological suffering, higher engagement may also mitigate suicidal tendencies, showing the complex dual role of spirituality in mental health.
Figure 1: Summary of the results of the multinomial regression of all significantly factors associated to severe suicidal ideation of people with spiritist engagement in the state of Ceará. Fortaleza/CE, 2022.
Ethics approval and consent to participate
The research met the Law 466/2012 of the National Council of Health (NCH), related to Research Ethics involving Human Beings, with approval of the Ethics Committee of the Federal University of Ceará (n. 2.237.838).
Human and animal rights
No animals were used in this research. All human research procedures followed the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
Consent for publication
Informed consent was obtained from all participants.
Availability of data and materials
The authors confirm that the data supporting the findings of this study are available within the manuscript.
Funding
None.
Conflict of interest
The authors declare no conflict of interest, financial or otherwise.
Acknowledgements
Declare none.
References
1. Miranda AGM, de Souza MF, Caldeira VC, Martins MC, Alves JBG, editors. Suicídio: aspectos epidemiológicos relacionados ao sexo, idade, escolaridade, estado civil, CID-10. Anais Colóquio Estadual de Pesquisa Multidisciplinar (ISSN-2527-2500) & Congresso Nacional de Pesquisa Multidisciplinar; 2018.
2. Sadock BJ, Sadock VA, Ruiz P. Compêndio de Psiquiatria: ciência do comportamento e psiquiatria clínica. 11 ed. Porto Alegre: Artmed; 2017. 1466 p.
3. OPAS/OMS-Brasil. Folha Informativo – Suicídio 2018 [https://www.paho.org/bra/index.php?option=com_content&view=article&id=5671:folha-informativa-suicidio&Itemid=839].
4. Arruda VL, Freitas B, Marcon SR, Fernandes FY, Lima NVP, Bortolini J, et al. Suicide in young Brazilian adults: 1997-2019 time series. Cien Saude Colet., 2021. p. 2699-708.
5. Veisani Y, Mohamadian F, Delpisheh A. Prevalence and comorbidity of common mental disorders and associations with suicidal ideation in the adult population. Epidemiology and Health. 2017;39:e2017031-e.
6. Scott J. Common mental disorders: A bio-social model by David Goldberg and Peter Huxley. London: Tavistock/Routledge. No. of pages: 194. Price £12.99. Stress Medicine. 1992;8(4):267-8.
7. Krueger RF. The Structure of Common Mental Disorders. Archives of General Psychiatry. 1999;56(10):921-.
8. Machado DB, Santos DNd. Suicídio no Brasil, de 2000 a 2012. Jornal Brasileiro de Psiquiatria. 2015;64:45-54.
9. Hegerl U. Prevention of suicidal behavior. Dialogues Clin Neurosci. 2016;18(2):183-90.
10. Filgueiras JC, Hippert MIS. A polêmica em torno do conceito de estresse. Psicologia: Ciência e Profissão. 1999;19(3):40-51.
11. Malhi GS, Mann JJ. Depression. The Lancet. 2018;392(10161):2299-312.
12. Martínez LS, Wasser AC. Depresión e ideación suicida en mujeres víctimas de violencia de pareja. Psicología, Conocimiento y Sociedad. 2019;9(1).
13. Barbosa RMR, Lima DF, Cavalcanti DB. Algumas ações para prevenção de suicídio desenvolvidas na UFPE. Revista dos Mestrados Profissionais. 2020;9(1):73-91.
14. IBGE. Censo 2010.
15. Bazley R, Pakenham K, Watson B. Perspectives on Suicide Prevention Amongst Members of Christian Faith-Based Organizations. Community Ment Health J. 2019;55(5):831-9.
16. Lace JW, Evans LN, Merz ZC, Handal PJ. Five-Factor Model Personality Traits and Self-Classified Religiousness and Spirituality. J Relig Health. 2020;59(3):1344-69.
17. Paul Victor CG, Treschuk JV. Critical Literature Review on the Definition Clarity of the Concept of Faith, Religion, and Spirituality. J Holist Nurs. 2020;38(1):107-13.
18. Peres MFP, Kamei HH, Tobo PR, Lucchetti G. Mechanisms Behind Religiosity and Spirituality’s Effect on Mental Health, Quality of Life and Well-Being. Journal of Religion and Health. 2018;57(5):1842-55.
19. Vitorino LM, Lucchetti G, Leão FC, Vallada H, Peres MFP. The association between spirituality and religiousness and mental health. Sci Rep. 2018;8(1):17233.
20. Tavares C. Dimensões do cuidado na perspectiva da espiritualidade durante a pandemia pelo novo coronavírus (COVID-19). Journal Health NPEPS. 2020;5:1-4.
21. Diego-Cordero R, Ávila-Mantilla A, Vega-Escaño J, Lucchetti G, Badanta B. The Role of Spirituality and Religiosity in Healthcare During the COVID-19 Pandemic: An Integrative Review of the Scientific Literature. J Relig Health. 2022;61(3):2168-97.
22. Del Castillo FA. Health, spirituality and Covid-19: Themes and insights. J Public Health (Oxf). 2021;43(2):e254-e5.
23. Kardec A. O que é o Espiritismo. 60, editor. Araras: Instituto de Difusão Espírita; 2004.
24. Kardec A. O Livro dos Espíritos. 1 ed. Rio de Janeiro: Celd; 2008.
25. FEB. Orientação ao Centro Espírita. 2006.
26. Dalgalarrondo P. Estudos sobre religião e saúde mental realizados no Brasil: histórico e perspectivas atuais. Archives of Clinical Psychiatry (São Paulo). 2007;34:25-33.
27. Moreira-Almeida A, Costa MdA, Coelho HS. The Idea of Survival of the Soul in the History of Religions and Philosophy. In: Moreira-Almeida A, Costa MdA, Coelho HS, editors. Science of Life After Death. Cham: Springer International Publishing; 2022. p. 5-11.
28. Isaia AC. Bezerra de Menezes e Gonçalves de Magalhães: muito além do cérebro. Tentativas de enfrentamento ao materialismo científico do século XIX. Revista Brasileira de História. 2020;40:267-88.
29. Swihart DL, Yarrarapu SNS, Martin RL. Cultural Religious Competence In Clinical Practice2023.
30. Shah AK, Becicka R, Talen MR, Edberg D, Namboodiri S. Integrative Medicine and Mood, Emotions and Mental Health. Primary Care: Clinics in Office Practice. 2017;44(2):281-304.
31. Sales TM. Magnitude e fatores associados ao envolvimento espírita, transtornos mentais comuns e ideação suicida: Um estudo seccional no Ceara. Fortaleza: Universidade Federal do Ceara; 2023.
32. IBGE. Censo 2010 2010 [Available from: https://sidra.ibge.gov.br/pesquisa/censo-demografico/series-temporais/series-temporais/.
33. Berg S. Snowball sampling—I. Encyclopedia of statistical sciences. 2004;12.
34. Chu IY, Alam P, Larson HJ, Lin L. Social consequences of mass quarantine during epidemics: a systematic review with implications for the COVID-19 response. J Travel Med. 27: International Society of Travel Medicine 2020.; 2020.
35. Both LM, Zoratto G, Calegaro VC, Ramos-Lima LF, Negretto BL, Hauck S, et al. COVID-19 pandemic and social distancing: economic, psychological, family, and technological effects. Trends Psychiatry Psychother. 432021. p. 85-91.
36. Granovetter M. Network sampling: Some first steps. American journal of sociology. 1976;81(6):1287-303.
37. Grandcolas U, Rettie R, Marusenko K. Web Survey Bias: Sample or Mode Effect? Journal of Marketing Management. 2003;19(5-6):541-61.
38. Pasquali L. Princípios de Elaboração de Escalas. In: Gorenstein C, Yuan-Pang, Hungerbühler I, editors. Instrumentos de Avaliação em Saúde Mental. Porto Alegre: Artmed; 2016.
39. Gorenstein C, Wang Y, Hungerbuhler I. Instrumentos de avaliação em saúde mental. Porto Alegre: Artmed; 2016.
40. Aquino TAA. Atitudes e intenções de cometer o suicídio: seus correlatos existenciais e normativos. João Pessoa: Universidade Federal da Paraíba, Universidade Federal do Rio Grande do Norte; 2009.
41. Osman A, Barrios FX, Grittmann LR, Osman JR. The multi-attitude suicide tendency scale: Psychometric characteristics in an american sample. Journal of Clinical Psychology. 1993;49(5):701-8.
42. Aquino TAAd. Atitudes e intenções de cometer o suicídio: seus correlatos existenciais e normativos. João Pessoa, 2009. p. 1-280.
43. Santos WSd, Ulisses SM, Costa TMd, Farias MG, Moura DPFd. The influence of risk or protective factors for suicide ideation. Psicologia, Saúde & Doença. 2016;17(3):515-26.
44. Bethlehem J. Selection Bias in Web Surveys. International Statistical Review / Revue Internationale de Statistique. 2010;78(2):161-88.
45. Calati R, Ferrari C, Brittner M, Oasi O, Olié E, Carvalho AF, et al. Suicidal thoughts and behaviors and social isolation: A narrative review of the literature. J Affect Disord. 2019;245:653-67.
46. Sampaio GN. Uma investigação da relação entre divórcios e suicídios no Brasil e no Estado do Ceará. 2021.
47. Borba LO, Ferreira ACZ, Capistrano FC, Kalinke LP, Maftum MA, Maftum GJ. Fatores associados à tentativa de suicídio por pessoas com transtorno mental. Revista Mineira de Enfermagem. 2020;24:1-9.
48. Barros TF, Borges SM, da Costa VA, dos Santos Santiago JC. Análise do perfil epidemiológico de suicídios no Ceará de 2015 a 2017.
49. Marbin D, Gutwinski S, Schreiter S, Heinz A. Perspectives in poverty and mental health. Front Public Health. 2022;10:975482.
50. Barros FC, Matijasevich A, Santos IS, Horta BL, da Silva BGC, Munhoz TN, et al. Social inequalities in mental disorders and substance misuse in young adults. Social Psychiatry and Psychiatric Epidemiology. 2018;53(7):717-26.
51. Stack S. Contributing factors to suicide: Political, social, cultural and economic. Prev Med. 2021;152(Pt 1):106498.
52. Magnani RM, Staudt ACP. Estilos parentais e suicídio na adolescência: uma reflexão acerca dos fatores de proteção. Pensando famílias. 2018;22(1):75-86.
53. Santos EDGM, Rodrigues GOL, Santos LO, Alves MES, Araújo LF, Santos JVSA. Suicídio entre idosos no Brasil: uma revisão de literatura dos últimos 10 anos. Psicología, Conocimiento y Sociedad. 2019;9:205-20.
54. Bierstetel SJ, Slatcher RB. Couples’ behavior during conflict in the lab and diurnal cortisol patterns in daily life. Psychoneuroendocrinology. 2020;115:104633.
55. McEwen BS, Akil H. Revisiting the Stress Concept: Implications for Affective Disorders. J Neurosci. 2020;40(1):12-21.
56. Chikritzhs T, Livingston M. Alcohol and the Risk of Injury. Nutrients. 132021.
57. Darvishi N, Farhadi M, Haghtalab T, Poorolajal J. Alcohol-related risk of suicidal ideation, suicide attempt, and completed suicide: a meta-analysis. PLoS One. 2015;10(5):e0126870.
58. Sher L. The impact of the COVID-19 pandemic on suicide rates. QJM: An International Journal of Medicine. 2020;113(10):707-12.
59. Patwardhan P. COVID-19: Risk of increase in smoking rates among England’s 6 million smokers and relapse among England’s 11 million ex-smokers. BJGP Open. 2020;4(2).
60. Leigh-Hunt N, Bagguley D, Bash K, Turner V, Turnbull S, Valtorta N, et al. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health. 2017;152:157-71.
61. Alkandari A, Law J, Alhashmi H, Alshammari O, Bhandari P. Staying (Mentally) Healthy: The Impact of COVID-19 on Personal and Professional Lives. Tech Innov Gastrointest Endosc. 2021;23(2):199-206.
62. Ganesan B, Al-Jumaily A, Fong KNK, Prasad P, Meena SK, Tong RK. Impact of Coronavirus Disease 2019 (COVID-19) Outbreak Quarantine, Isolation, and Lockdown Policies on Mental Health and Suicide. Front Psychiatry. 2021;12:565190.
63. Bhattacharjee B, Acharya T. “The COVID-19 Pandemic and its Effect on Mental Health in USA – A Review with Some Coping Strategies”. Psychiatr Q. 912020. p. 1135-45.
64. John A, Eyles E, Webb RT, Okolie C, Schmidt L, Arensman E, et al. The impact of the COVID-19 pandemic on self-harm and suicidal behaviour: update of living systematic review. F1000Research. 2020;9.
65. Amaral CEM, Treichel C, Francisco P, Onocko-Campos RT. [Mental healthcare in Brazil: a multifaceted study in four large cities]. Cad Saude Publica. 2021;37(3):e00043420.
66. Gourret Baumgart J, Kane H, El-Hage W, Deloyer J, Maes C, Lebas MC, et al. The Early Impacts of the COVID-19 Pandemic on Mental Health Facilities and Psychiatric Professionals. Int J Environ Res Public Health. 182021.
67. Neelam K, Duddu V, Anyim N, Neelam J, Lewis S. Pandemics and pre-existing mental illness: A systematic review and meta-analysis. Brain Behav Immun Health. 10: © 2020 The Authors.; 2021. p. 100177.
68. Sukut O, Ayhan Balik CH. The impact of COVID-19 pandemic on people with severe mental illness. Perspect Psychiatr Care. 57: 2020 Wiley Periodicals LLC.; 2021. p. 953-6.
69. Nason I, Stein DT, Frank RG, Stein MB. Decline In New Starts Of Psychotropic Medications During The COVID-19 Pandemic. Health Aff (Millwood). 2021;40(6):904-9.
70. Gomes BP, da Costa Medeiros G, Aguilar FZ, Zattar T, Franco DCZ. Análise do uso de psicofármacos no Brasil no contexto da pandemia da COVID-19: Analysis of the use of psychotropic drugs in Brazil in the context of the COVID-19 pandemic. Archives of Health. 2022;3(2):94-8.
71. Alcântara AM, Figel FC, Campese M, da Silva MZ. Prescrição de Psicofármacos na Atenção Primária à Saúde no contexto da Pandemia da Covid-19. Research, Society and Development. 2022;11(4):e19911420210-e.
72. Sales TM, Mota RMS, Macena RHM. Formulário Deenvolvimento Espírita (FENE): development and validation of an instrument for assessing the level of spiritual development. Fortaleza: UFC; 2023. Available at: http://repositorio.ufc.br/handle/riufc/74736.
73. Sales TM. Spiritism, mental health, and public health: spiritist therapeutics under discussion. MOJ Public Health. 2023;12(3):145‒150.