

HPV and Cervical Cancer: Epidemiology in Burkina Faso
Epidemiological profile of human papillomavirus infections and cervical cancer prevention among sexually active women in Burkina Faso: Literature Review
Pierre Zabre1, Tani Sagna1,2,*, Rogomenoma Alice Ouedraogo1, Jacques Simpore1,3
- Laboratory of Molecular Biology and Genetics (LABIOGENE), Joseph KI-ZERBO University, Ouagadougou, Burkina Faso.
- National Center for Scientific and Technological Research, Research Institute of Health Sciences (IRSS), Ouagadougou, Burkina Faso.
- Pietro Annigoni Biomolecular Research Center (CERBA), Ouagadougou, Burkina Faso
*Correspondence to: [email protected] (0000-0002-8775-0693)
OPEN ACCESS
PUBLISHED 30 November 2024
CITATION Zabre, P., Sagna, T., et al., 2024. Epidemiological profile of human papillomavirus infections and cervical cancer prevention among sexually active women in Burkina Faso: Literature Review. Medical Research Archives, [online] 12(11). https://doi.org/10.18103/mra.v12i11.5883
DOI https://doi.org/10.18103/mra.v12i11.5883
ISSN 2375-1924
ABSTRACT
Cervical cancer is one of the biggest public health challenges in developing countries. According to the Global Cancer Observation in 2022, Burkina Faso recorded 988 new cases, with 775 deaths. Caused mainly by the human papillomavirus (HPV), this cancer is a heavy burden on our populations. The aim of this review was to assess the current state of human papillomavirus infections and cervical cancer prevention among sexually active women in Burkina Faso. Original studies were extracted from PubMed/Medline, Google Scholar, semanticscholar, Hinari and Science Direct using appropriate MeSH terms. Results were extracted and reviewed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyse method (PRISMA). Twenty-four studies from three regions of Burkina Faso were included in the systematic review, with most of the articles from the “Centre” region. Out of a total of 5480 participants for the pooled analyses, the review showed a prevalence of HPV, varying according to population type and region and ranging from 20.6% to 87.2%. In contrast, the overall prevalence of HPV 16 and 18 infections were low compared to the global trend. With a low screening rate, the prevalence of cancerous lesions ranged from 1.5% to 15.42%. The level of knowledge was lower among rural than urban residents. Bivalent and quadrivalent vaccines had low coverage for the genotypes identified. In the fight against cervical cancer in Burkina, concerted efforts are needed to strengthen screening programs, increase HPV vaccination coverage, and raise public awareness. Large-scale national studies are needed to map HPV genotypes in order to make appropriate decisions for cervical cancer control.
Keywords
Epidemiology; Prevention; Cervical cancer; HPV; Burkina Faso.
INTRODUCTION
Human Papillomavirus (HPV) is the world’s most common sexually transmitted infection. Today there are more than 200 HPV genotypes, with over 120 genotypes identified and sequenced. Depending on their oncogenic potential, they are divided into two groups: high-risk oncogenic HPV (HR-HPV) and low-risk oncogenic HPV (LR-HPV). They are responsible for several infections of the epithelium of the anogenital tract and other mucous membranes, and are also involved in a variety of cancers, including vaginal, penile, vulvar, anal, and oropharyngeal cancers. Low Risk HPV such as HPV 6 and 11 are responsible for condylomatous lesions (warts) of the anogenital tract and laryngeal papillomatosis, most common benign tumor of the larynx. Cervical cancer is an infectious pathology of the cervical mucosa. In approximately 99% of cervical cancer cases, women have been exposed to HPV. Several studies have shown that worldwide, HPV genotypes 16, 18, 31, 33, 35, 45, 52 and 58 are the most common among women with precancerous lesions and cervical cancer. Some low-grade precancerous lesions induced by specific HPV genotypes have the potential to develop into cervical cancer if left untreated. It is the fourth most common cancer in women worldwide, after breast, colorectal and lung cancers. It is one of the world’s major public health problems. In 2018, the World Health Organization (WHO) estimated that over 311000 women had died of cervical cancer and around 570000 new cases recorded worldwide. Around 85% of these deaths occurred in low-and middle-income countries. Women in sub-Saharan Africa show the highest prevalence, which appears to be rising steadily. According to the WHO, cervical cancer will kill more than 443,000 women a year worldwide by 2030, nearly 90% of them in sub-Saharan Africa. According to GLOBOCAN, since 2020, cervical cancer has been the second leading cancer in terms of incidence and mortality in women in Burkina Faso, with 988 new cases and 775 deaths, as of 2022. For a more effective prevention of HPV infections, persistent HPV disease and cervical cancer, HPV vaccination is widely recommended. The WHO estimates that HPV vaccination significantly reduces cervical cancer morbidity and mortality. However, epidemiological data on HPV and cervical cancer from sub-Saharan African countries are necessary for the choice of available vaccines, as the distribution of HPV genotypes varies from one country to another, with more genotype diversity in African countries. The three licensed HPV prophylactic vaccines available are genotype-specific. In fact, the bivalent Gardasil (genotypes 16/18), the quadrivalent Cervarix (genotypes 6/11/16/18) and the nonavalent Gardasil 9 (6/11/16/18/31/33/45/52/58) have been shown to be safe and effective for primary prevention of the targeted genotypes. In Burkina Faso, since April 26, 2022, the quadrivalent human papillomavirus vaccine has been included in the vaccination schedule of the Expanded Program on Immunization to combat cervical cancer. However, are the genotypes identified in the general female population, in populations at high risk of HPV infection, in high-grade precancerous lesions and invasive cervical cancers predominantly covered by the vaccine available in the vaccination program? A systematic review of the epidemiology of human papillomavirus infection and cervical cancer in sexually active women in Burkina Faso therefore seems necessary to make better decisions on the control of HPV infections and cervical cancer, which carries a heavy burden in Burkina Faso. The aim of this review was to examine the epidemiological profile of HPV and the prevention of cervical cancer in sexually active women in Burkina Faso.
METHODS
STUDY DESIGN
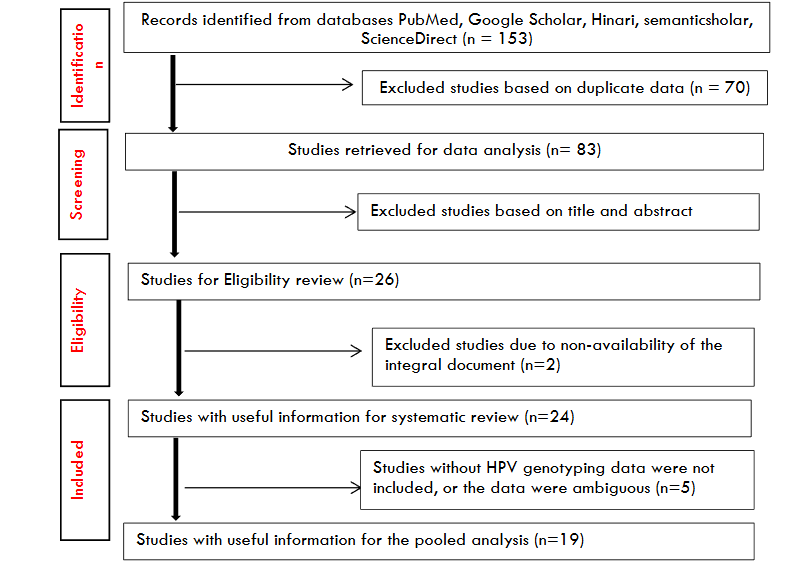
This study was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyse method (PRISMA). Research results and the number of articles included and excluded are presented in Figure 1.
INFORMATION SOURCES AND RESEARCH STRATEGIES
We conducted a systematic literature review to identify relevant publications reporting on the epidemiology of human papillomavirus (HPV) infections and cervical cancer, as well as their prevention among sexually active women in Burkina Faso. Original studies in French and/or English were extracted from the PubMed/Medline, Google Scholar, semanticscholar, Hinari and Science Direct databases, using appropriate terms. The records identified have been downloaded in an appropriate format and linked to the zotero software. Boolean operators “AND” and “OR” were used to link mesh terms and to retrieve publications from PubMed/Medline (NCBI) databases. The keywords used were “Epidemiology OR prevention AND human papillomavirus OR cervical cancer” + “country name or country cities”. The crude prevalence of HPV infection was calculated based on the crude data available in the eligible studies.
ELIGIBILITY CRITERIA AND STUDY SELECTION PROCEDURE
After searching through the databases, the studies were then selected on the basis of the following criteria: data are published in a peer-reviewed scientific journal; articles are complete and available; articles relate only to patients residing in Burkina Faso; patients consulted for gynecological problems or participated in a cervical cancer screening campaign; cervical histology results are confirmed for patients with cervical cancer or precancerous lesions; HPV prevalence is calculated with at least five genotypes identified. The articles selected for analysis will be used to determine the prevalence and genotypic distribution of oncogenic HPV in sexually active women in some of the regions of the country. The HPV molecular diagnostic techniques selected were those based on molecular biology techniques, in particular polymerase chain reaction (PCR) and hybrid capture. HPV genotype classification was also considered. In addition, we systematically excluded journal articles, correspondences to editors, press releases, letters, book chapters, publications in languages other than English/French, and studies whose data were ambiguous or could not be extracted. We considered HIV-negative and HIV-positive populations, sex workers, articles on the epidemiology and prevention of HPV and cervical cancer. To get a true overview of circulating genotypes in Burkina Faso, HPV genotyping studies carried out on HPV-positive populations were selected. Studies on both Burkinabé and other female populations were included, but only data relating to the Burkinabé population were considered in this study. Articles addressing other sexually transmitted pathologies in addition to HPV in the case of cervical cancer were included in this systematic review. However, articles from the Knowledge, Attitude and Practice surveys on health workers were excluded from this study. For pooled analyses, we considered the total number of HPV-diagnosed samples to be the size of our study population.
DATA EXTRACTION AND ANALYSIS
The data were extracted from various studies carried out in the regions of Burkina Faso for systematic examination. For the articles included in this review, the variables extracted were, study population and study setting, type of study or data collection (cross-sectional, prospective or retrospective) and method of detection. In addition, the overall crude prevalence of HPV infection was determined as the ratio of the total number of women tested positive for at least one HPV to the total number of samples tested, expressed as a percentage. The frequency of HPV genotypes was calculated as the ratio of the genotype of interest to the total number of genotypes identified, taking into account single, multiple and undetermined genotypes. IBM SPSS Statistic 26 and Excel 2016 were used for frequency calculations and graphing.
RESULTS
SELECTION OF STUDIES FOR REVIEW
In our study, a total of 153 articles were extracted from the databases, and for the systematic review, 26 full-text articles were included. According to our inclusion criteria, 24 scientific studies on epidemiological studies of HPV and cervical cancer prevention in sexually active women conducted in 3 regions of Burkina Faso, including 19 articles on HPV genotyping and 5 articles on cervical cancer screening, knowledge, attitudes, and practices, were selected.
| Population | Reference | Region (cities) | Area of interest | Average age (age range) | Size | HPV Prevalence (%) |
|---|---|---|---|---|---|---|
| SA | Kabre et al | Centre (Ouagadougou) | HPV genotyping | 28.2 (18 – 40) | 100 | 23 |
| HIV+/HIV- | Djigma et al | Centre (Ouagadougou) | HPV genotyping | 33.91 (20 – 53) | 421 | 34.4 |
| SA | Ouedraogo et al | Centre (Ouagadougou) | HPV genotyping | 31 (15 – 63) | 300 | 43 |
| SA | Salambanga et al | Centre (Ouagadougou) | HPV genotyping | 34.7 (18-57) | 234 | 52.56 |
| HIV-/HIV+ | Djigma et al | Centre (Ouagadougou) | HPV genotyping | 34.1 (20 – 54) | 250 | 59.6 |
| SA/HIV+ | Zohoncon et al | Centre (Ouagadougou) | HPV genotyping | 33.7 (20-53) | 180 | 73.33 |
| SA | Ouedraogo et al | Centre-Est (Tenkodogo) | HPV genotyping | 35.5 (20 – 60) | 131 | 34.4 |
| SA | Ouedraogo et al | Centre-Est (Garango) | HPV genotyping | 39.2 | 135 | 43 |
| SA | Ouedraogo et al | Centre, Centre-Est, Hauts-Bassins | HPV genotyping | 28.02 (15 – 57) | 520 | 35.42 |
| SA | Sawadogo et al | Centre (Ouagadougou) | KAP | 29.37 (20-50) | 840 | – |
| SA | Compaore et al | Centre (Ouagadougou) | CC screening & KAP | 37.5 (18 – 72) | 351 | – |
| SA | Kagoné et al | Hauts-Bassins (Bobo-Dioulasso, Bama) | CC screening & KAP | 34.9 (18 – 60) | 577 | – |
| SA | Tassembedo et al | Centre-Nord (Boussé) | CC screening & KAP | 34 IQR (30-50) | 418 | – |
| SA | Diendéré et al | National | CC screening & KAP | 37.5 (25 – 49) | 2293 | – |
| SA | Traore et al | Hauts-Bassins (Bobo-Dioulasso) | CC screening & HPV genotyping | 35.3 (20-56) | 181 | 25.4 |
| SA | Ouattara et al | Hauts-Bassins (Bobo-Dioulasso) | CC screening & HPV genotyping | 30.7 (19 – 51) | 234 | 20.6 |
| SA/SW | Tovo et al | Centre (Ouagadougou) | HPV genotyping | 27.12 (17 – 50) | 182 | 54.94 |
| SA/SW | Ilboudo et al | Centre (Ouagadougou) | HPV genotyping | 27.3 (16 – 50) | 200 | 53 |
| SA/CC | Ouédraogo et al | Centre (Ouagadougou) | HPV genotyping | 41.5 (22 – 74) | 43 | 48.8 |
| SA/CC | Zohoncon et al | Centre (Ouagadougou) | HPV genotyping | 46.32 (21-84) | 65 | 72.31 |
| SA | Maria et al | Centre (Ouagadougou) | HPV genotyping | 41.3 (19 -76) | 444 | 39 |
| SA/HBV/HCV | Ouédraogo et al | Centre (Ouagadougou) | HPV genotyping | 37.8 (20 – 65) | 100 | 28 |
| SA/HIV+ | Chikandiwa et al | Centre (Ouagadougou) | HPV genotyping | 36 (IQR, 31–42) | 594 | 27.1 |
| SA/HIV+/SW | Didelot-Rousseau et al | Hauts-Bassins (Bobo-Dioulasso) | CC screening & HPV genotyping | 28 (16 – 54) | 360 | 66.1 |
| Total | 3 Regions | 9993 |
A total of 9993 participants from the sexually active female population were included for data extraction.
CHARACTERISTICS OF INCLUDED STUDIES
Studies included in this systematic review provided data from the Burkinabe population and met our selection criteria. Among 5480 sexually active women in the general population, 2232 were infected with at least one of the HR-HPV (16/18/31/33/35/39/45/51/52/56/59/66/68/82) and/or LR-HPV (6/11/40/41/42/43/44/55/54/61/62/82/67/69/71/70/72/73/74/84) genotypes. Of the 24 scientific studies included in the review, 19 had information on the genotypic distribution of HPV and were therefore eligible for pooled analysis. Multiple infections with at least two specific HPV types were reported in the majority of studies.
EPIDEMIOLOGY OF HUMAN PAPILLOMAVIRUS INFECTION
Prevalence of Human Papillomavirus infection in Burkina Faso
This systematic review reports on the prevalence and distribution of HPV genotypes among sexually active women in Burkina Faso. The analysis of selected studies shows that the prevalence of HPV infections is very high in the general population of women in this low-income country. HPV prevalence varied according to population type and locality in Burkina Faso. In the sexually active female population with unknown risk of HPV infection, it ranged from 20.6% to 52.56% in the studies included in this review.
Among the studies analyzed, 11 involved HIV-positive women, cases of high-grade precancerous lesions (CIN1/2/3) or cervical cancer, sex workers and HBV/HCV-positive women, thus representing populations at high risk of HPV infection. Indeed, these studies reported that the maximum prevalence of HPV in this at-risk population was 87.2%, 66.1%, 97.59%, 28% respectively in confirmed cases of precancerous lesions or cervical cancer, sex workers, HIV-positive women, and those with hepatitis B and/or C.
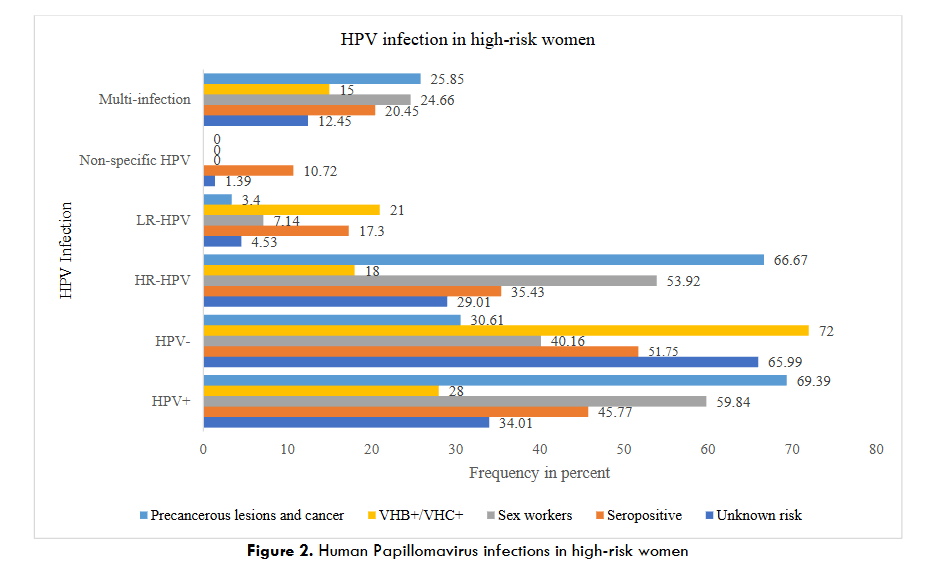
The pooled analysis reported that the overall prevalence of HPV in these different at-risk populations was 69.39%, 59.84%, 45.77%, 28% respectively in confirmed cases of precancerous lesions or cervical cancer, sex workers, HIV-positive women, and HBV/HCV-positive women. This prevalence was 34.01% for the population with unknown high risk of HPV infection.
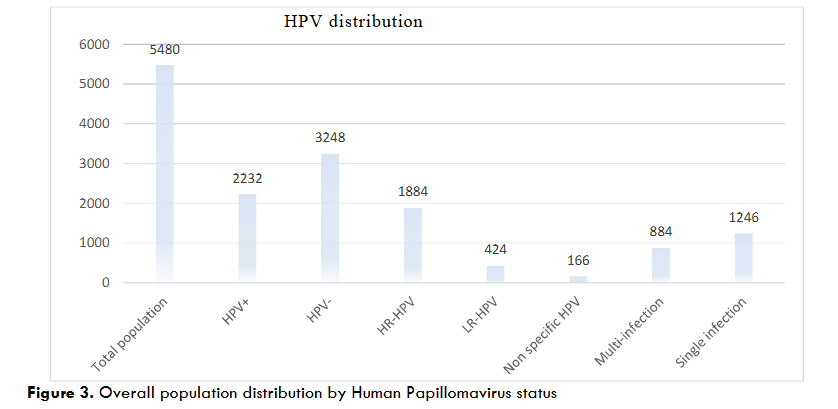
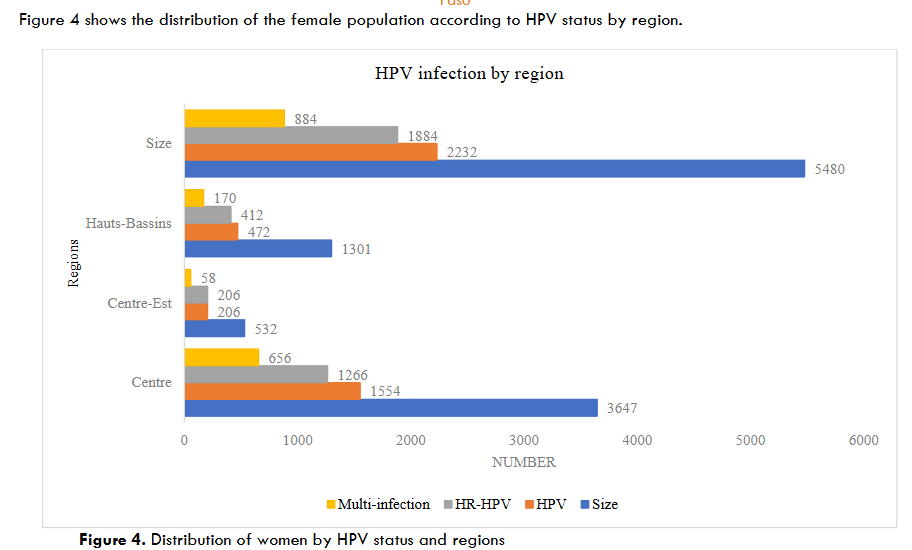
From the pooled analysis of data extracted from eligible studies, only three regions benefited from the HPV epidemiological studies, with the majority conducted in the “Centre” region. Indeed, among the 5480 participants, 3647 were from the “Centre” region, 1201 from the “Hauts-Bassins” region and 532 from the “Centre-Est” region. HPV prevalence reached 40.72% (2232/5480) in the general female population, 51.55% (1082/2099) in the population at high risk of HPV infection, and 34.01% (1150/3381) in the female population with unknown history of HPV risk. In addition, among HPV-infected women, single and multiple infections were 55.82% (1246/2232) and 39.60% (884/2232) respectively, versus 7.44% (166/2232) of unspecified HPV infections.
Human Papillomavirus genotype distribution
The studies included in this review showed that the predominance of HPV genotypes in women was a population-based and locality-based variable. In fact, several high-risk and low-risk oncogenic HPV genotypes were found in the pooled analysis of 19 studies. Among the genotypes, the most frequent HR-HPV were HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68 and the most frequent LR-HPV were HPV 6, 11, 43, 44/55, 54, 69/71, 70. Considering the three most predominant genotypes in the population at high risk of HPV infection, the studies show, in order of respective presence, HPV 18; 31; 52/35/68; 39; 45; 16.
| HR-HPV | Number (%) | LR-HPV | Number (%) |
|---|---|---|---|
| HPV 16 | 153 (6.85) | HPV 6 | 101 (4.52) |
| HPV 18 | 308 (13.80) | HPV 11 | 11 (0.49) |
| HPV 31 | 195 (8.74) | HPV 40 | 10 (0.45) |
| HPV 33 | 74 (3.31) | HPV 42 | 4 (0.17) |
| HPV 35 | 230 (10.30) | HPV 43 | 17 (0.76) |
| HPV 39 | 153 (6.85) | HPV 44/55 | 56 (2.50) |
| HPV 41 | 2 (0.09) | HPV 54 | 29 (1.30) |
| HPV 45 | 146 (6.54) | HPV 61 | 3 (0.13) |
| HPV 51 | 173 (7.75) | HPV 62/81 | 14 (0.63) |
| HPV 52 | 298 (13.35) | HPV 67 | 11 (0.49) |
| HPV 53 | 36 (1.61) | HPV 69/71 | 25 (1.12) |
| HPV 56 | 280 (12.54) | HPV 70 | 26 (1.16) |
| HPV 58 | 182 (8.15) | HPV 72 | 4 (0.18) |
| HPV 59 | 175 (7.84) | HPV 74 | 37 (1.66) |
| HPV 66 | 182 (8.15) | HPV 84 | 1 (0.04) |
| HPV 68 | 134 (6.00) | HPV 82 | 19 (0.85) |
| Total | 2740 |
Risk factors associated with Human Papillomavirus infections
Several risk factors favoring HPV infections have been described worldwide. In Burkina Faso, HIV/AIDS, age, multiparity, residence, early age at 1st sex, use of oral contraception, condom use, level of education, number of sexual partners, etc., have been described as risk factors for HPV infection by the eligible studies included in this systematic review.
EPIDEMIOLOGY OF CERVICAL CANCER
Prevalence, incidence, mortality and morbidity
For more than a decade, cervical cancer has been a major public health problem in Burkina Faso, despite the efforts made to prevent it. According to GLOBOCAN, since 2008 the crude incidence rate per 100,000 people has fluctuated between 15 and 26, and the crude morbidity rate per 100,000 people between 11 and 21.
| Year | Incidence | Morbidity |
|---|---|---|
| 2008 | 1230 (16.1) | 838 (11.0) |
| 2018 | 2517 (25.4) | 2081 (21.0) |
| 2020 | 1132 | 839 |
| 2022 | 988 (15.9) | 775 (13.0) |
Influence of Human Papillomavirus infection and Human Papillomavirus genotype distribution on the occurrence of cervical cancer in Burkina Faso
According to the pooled analyses in this study, around 70% of women with precancerous lesions and cervical cancer are infected with at least one HPV genotype, and around 67% are infected with at least one high-risk oncogenic HPV genotype.
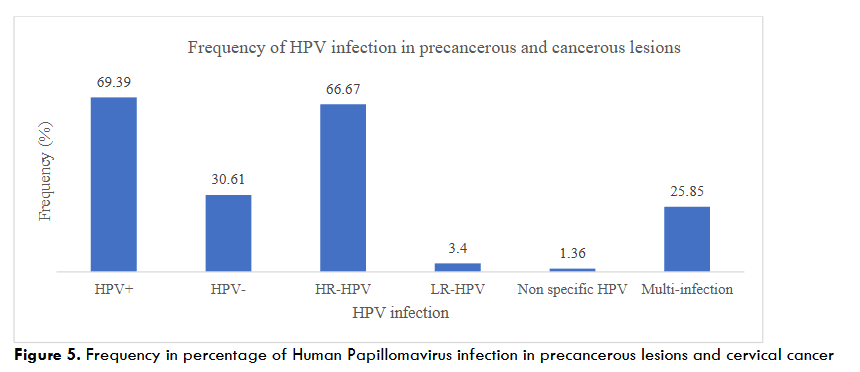
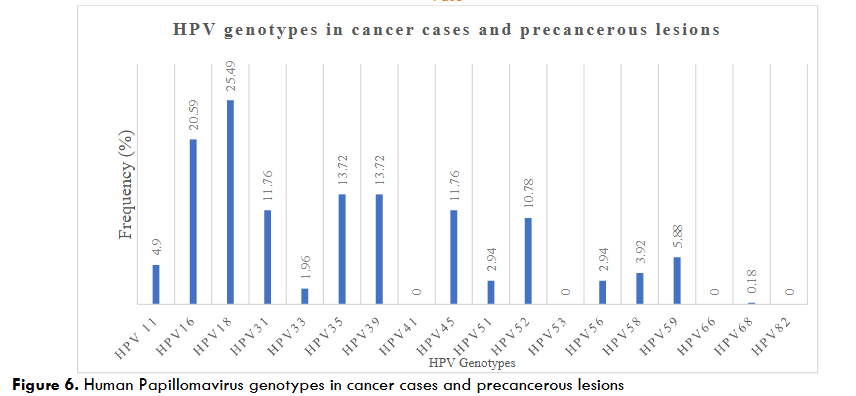
Among the high-risk oncogenic genotypes, HPV18, HPV16, HPV35 and HPV39 are the most frequent, with prevalence rates of 25.49%, 20.59% and 13.72% respectively.
PREVENTION OF HUMAN PAPILLOMAVIRUS INFECTION AND CERVICAL CANCER
Risk factors associated with cervical cancer
In addition to persistent infection with high-risk oncogenic HPV genotypes, considered to be the main cause of precancerous lesions and cervical cancer, several risk factors were associated. According to the articles included in this review, these were HIV serology, age, knowledge of risk factors and parity.
Screening and Knowledge, attitudes and practices on cervical cancer in Burkina Faso
The knowledge, attitudes and practices of sexually active women towards Cervical cancer remain major prevention factors. In fact, the studies selected for this review revealed a low level of cervical cancer knowledge. Most women are still unaware of preventive measures, and less than 10% of women in the various targeted studies were screened.
Screening detects pre-cancerous lesions, which represent the sub-clinical or asymptomatic stage of the disease, and which, if untreated, can progress to cancer. Its aim is to identify individuals with a high probability of contracting or developing the disease. In low-income countries, screening by visual inspection with acetic acid and Lugol’s iodine (VIA/VILI) is recommended by the WHO in addition to cervical smear. With this technique, the frequency of detection of precancerous lesions varies from 1.5% to 24% across the studies included. With a low screening rate as previously suggested, several factors such as level of education, age and residence were associated with screening, according to the studies examined. Like HPV infection, several factors are thought to be associated with the development of cervical cancer in women.
| Article | Size | Risk factors associated with precancerous lesions and cervical cancer (p-value) |
|---|---|---|
| Kagoné et al | 577 | – Age (0.0005) |
| Ouédraogo et al | 43 | – HPV status (< 0.001) |
| Didelot-Rousseau et al | 379 | – Age (0.001) |
| Sawadogo et al | 840 | – Think at risk of cervical cancer (0.02) |
Screening and related factors
| Article | Size | Technic | Lesion frequency | Screening-related factors |
|---|---|---|---|---|
| Compaore et al | 351 | – | – | – Education (<0.001) |
| Kagoné et al | 577 | VIA | 15.42% | – |
| Tassembedo et al | 418 | VIA/VILI | 5% | – |
| Ouedraogo et al | 1321 | VIA/VILI | 4.39% | – |
| Didelot-Rousseau et al | 379 | Cervical smear | 24.0% | – |
Knowledge, attitudes and practices on cervical cancer
| Article | Size | Knowledge, attitudes and practices (frequencies in %) |
|---|---|---|
| Kagoné et al | 577 | – Heard about cervical cancer (49%) |
| Sawadogo et al | 840 | – Knowledge of CC (64.2%) |
| Diendéré et al | 2293 | – Already screened (6.2%) |
Genotypic coverage of Human Papillomavirus vaccines in Burkina Faso
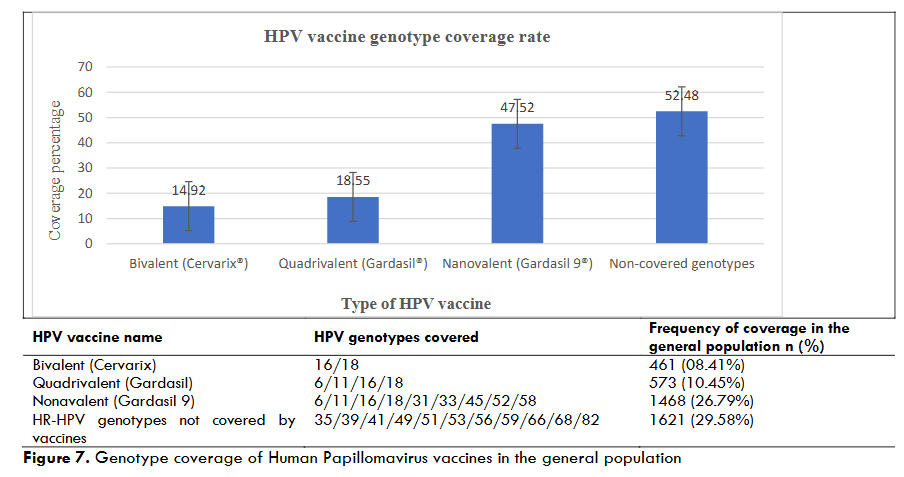
HPV vaccination remains one of the most effective methods of primary prevention of cervical cancer. The genotypic coverage rate of HPV vaccines is a factor that guides the choice of vaccine among the three licensed vaccines available on the market. Based on a pooled analysis of the studies collected, the genotypes covered by the vaccines are shown in the following table.
| HPV vaccine name | HPV genotypes covered | Frequency of coverage in the general population n (%) |
|---|---|---|
| Bivalent (Cervarix) | 16/18 | 461 (08.41%) |
| Quadrivalent (Gardasil) | 6/11/16/18 | 573 (10.45%) |
| Nonavalent (Gardasil 9) | 6/11/16/18/31/33/45/52/58 | 1468 (26.79%) |
| HR-HPV genotypes not covered by vaccines | 35/39/41/49/51/53/56/59/66/68/82 | 1621 (29.58%) |
DISCUSSION
In Burkina Faso, initiatives are underway to combat cervical cancer. However, up-to-date epidemiological data on HPV and cervical cancer are needed to assess the potential impact of these initiatives on cervical cancer prevention, and to identify effective strategies. Based on 24 studies, this systematic review highlights the epidemiological profile of HPV and the prevention of cervical cancer among sexually active women in Burkina Faso. This study shows poor coverage of epidemiological data on HPV and cervical cancer. Only studies from three of the 13 regions in Burkina Faso were included in this review. The majority of studies were carried out in the “Centre” region, more precisely in the city of Ouagadougou. Despite this low coverage, we noted a high prevalence of HPV and a varied distribution, both genotypically and geographically in the regions covered by the study. This prevalence varied from 20.6 to 97.59%, depending on the type of population. It was close to the results of other studies, which reported 8.9% and 81.8% in women from the general West African population and 10.7 to 97.2% in women from sub-Saharan Africa. It was high among women living with HIV, cervical cancer, sex workers and women infected with the hepatitis virus, with respective prevalences of 45.77%, 69.39%, 59.84% and 28%. Like all sexually transmitted infections (STIs), sex workers are exposed to the HPV infection. With high unemployment, sex work remains a common practice in our countries, and it is not without risks, as it is a key factor in the high rate of STIs in sub-Saharan African countries. Studies on HPV prevention among sex workers in African countries reveal a much higher rate than ours. This could be explained by the number of daily clients, the means of protection used by these sex workers, and also by the technique used for HPV genotyping in the various studies. Immunodepression due to HIV infection is a major public health problem. However, according to UNAIDS, women and girls account for the majority of new HIV infections. Women living with HIV have a higher prevalence of genital high-risk oncogenic HPV (HR-HPV) infection than those in the general population. They are more likely to be infected with several types of HR-HPV and have greater persistence of infection. Cervical cancer and CIN2/3 precancerous lesions are mostly caused by HR-HPV. The prevalence recorded in the present review was close to the 75.3% reported by Kelly et al. in 2017 in Burkina Faso. Human Papillomavirus prevalence among women with unknown risk factors for HPV infection, based on collective analysis of data from the three regions of Burkina Faso, was 34.01%. These results corroborate those of Mkunde et al in 2023 who recorded 38.1%, 34% recorded by Seyoum et al in sub-Saharan Africa, and the 33.6% by Ouedraogo et al in West Africa. For women in the general population of Burkina Faso, the pooled analysis shows an overall prevalence of 40.73%. This result is significantly higher than that of Ouédraogo et al. who recorded a prevalence of 28.6% in West Africa, and closer to that of Ogembo et al. who reported a prevalence of 50.5% in 2015 in a meta-analysis in Africa. This variation in the prevalence of HPV infection could be explained by the difference in sample sizes and also the inclusion of cases of precancerous lesions, cervical cancer and female populations at high risk of HPV infection in some studies. In this review, the HPV genotypes included were HR-HPV (16/18/31/33/35/39/45/51/52/56/58/59/66/68/82) and LR-HPV (6/11/43/44,55/54/69,71/70). It showed that the prevalence and distribution of these HPV genotypes in Burkina Faso varied according to region and study population, and 2232 of the 5480 women were infected with at least one of these HPV genotypes. The most frequent high-risk oncogenic genotypes were HPV18/52/56/35/31/58/66/59/51/16/39/45/68/33/53 in descending order for the general population. This distribution of HR-HPV genotypes could confirm the observations of Ouedraogo et al. in 2023, who reported that the distribution of HR-HPV in West Africa varied from country to country. Ouedraogo et al. in 2023 explained this difference in distribution by human genetic factors. The second most frequent genotype in this review, HPV52, also attracted the attention of Ouedraogo et al. in 2023, who reported that it was common among the five main genotypes in most of the West African countries included in their study. Unfortunately, it is not included in the licensed quadrivalent cervical cancer vaccine used in Burkina Faso, despite the fact that it has been included in the cases of cervical cancer reported in some African studies. Thanks to the support of Technical and Financial partners, the quadrivalent vaccine Gardasil 4 has been integrated into Burkina Faso’s Expanded Program on Immunization. This commitment would require particular attention to the coverage rate of the most frequent genotypes in Burkina Faso. Our pooled analysis of studies carried out on HPV-infected women in Burkina Faso revealed that the nine most frequent genotypes were HPV18/52/56/35/31/58/66/59/51. Only HPV18 of the 9 is covered by Gardasil 4, and four genotypes (HPV18/52/31/58) are covered by Gardasil 9. In this study, the bivalent Cervarix and quadrivalent Gardasil 4 vaccines were poorly covered in infected women. However, 14.92% of genotypes would be protected by Cervarix, 18.55% by quadrivalent Gardasil 4 and 52.48% not covered by the three vaccines. Only Gardasil 9 showed greater genotypic coverage. This low genotypic coverage had been reported in studies in Burkina Faso and West Africa despite the efficacy of these vaccines on the genotypes covered. Despite these vaccines having some cross-protection against other less common HR-HPV types, as reported by some authors, our results advocate the introduction of Gardasil 9 vaccine in Burkina as an excellent way to prevent cervical cancer, a silent killer of the female population.
Study limits
The main objective of this review was to assess the epidemiological profile of HPV and the prevention of cervical cancer in Burkina Faso. It provides important insights into this infection in the female population, but the applicability of its findings is limited. Thus, this study presents limitations such as the diversity of HPV genotyping kits used in the different studies, the number of regions that have been the subject of HPV epidemiological studies with available data (three regions out of the thirteen regions of the country), the non-inclusion of low-risk genotypes in most of our studies included in this systematic review. Studies reporting indeterminate genotypes would also be a limitation for our study.
Conclusion
In Burkina Faso, the fight against cervical cancer remains a major challenge, and HPV infection is a major health problem due to its high prevalence and involvement in the majority of cervical cancer cases. This prevalence varies from one region to another and depends on the type of population. The distribution of oncogenic HPV genotypes responsible for the development of cervical cancer varies according to the locality and population concerned in Burkina Faso. For more effective prevention of HPV infection and cancer, a large-scale vaccination program with Gardasil 9 would be beneficial. Large-scale national epidemiological studies are needed to determine the risk factors for HPV infections and progression to cervical cancer. In addition, it will be necessary to map HPV genotypes in cases of high-grade precancerous lesions and histologically confirmed cervical cancer, in order to make appropriate decisions for cervical cancer control. Women had insufficient knowledge of risk factors, prevention and screening for cervical cancer, which influenced their attitudes towards adherence to screening. A cervical cancer awareness program should focus on risk factors, prevention methods and the organization of screening campaigns. This information can be used to improve the planning and design of prevention interventions.
Authors’ contributions
Conceptualization: PZ and TS. Methodology: PZ, TS, RAO and JS participated in data collection. PZ, TS and RAO reviewed relevant articles; performed cluster analysis; participated in preparation of original project. Writing: PZ. Revision and editing: PZ, TS, RAO, JS. All authors contributed to data interpretation and discussion and approved the final manuscript.
Pierre Zabré : PZ ; Tani Sagna : TS, Rogomenoma Alice Ouedraogo : RAO, Jacques Simporé : JS
Conflict of interest
The authors declare that they have no conflicts of interest.
Funding
N/A
Acknowledgements
The authors thank Mr. James AMEDEKER and Ms. Clemence BANCE for their assistance with English-language editing.
References
- Maria H, Dana H, Françoise M, Michael P, Jürgen W. Human papillomaviruses in Western Africa: prevalences and risk factors in Burkina Faso. Arch Gynecol Obstet. 2018;298(4):789-796. doi:10.1007/s00404-018-4860-z
- Bernard HU, Burk RD, Chen Z, van Doorslaer K, zur Hausen H, de Villiers EM. Classification of Papillomaviruses (PVs) Based on 189 PV Types and Proposal of Taxonomic Amendments. Virology. 2010;401(1):70-79. doi:10.1016/j.virol.2010.02.002
- Ouedraogo RA, Kande A, Nadembega WMC, Ouermi D, Zohoncon TM, Djigma FW, Ouedraogo CMRN, Lompo OM, Simpore J. Distribution of high-and low-risk human papillomavirus genotypes and their prophylactic vaccination coverage among West African women: systematic review. J Egypt Natl Cancer Inst. 2023;35(1):39. doi:10.1186/s43046-023-00196-x
- Duport N. Données épidémiologiques sur le cancer du col de l’utérus. État Connaiss – Actual. Published online January 1, 2008:34.
- Ishida W, Singto Y, Yuenyao P, Tassaneeyakul W, Kanjanavirojkul N, Ishida T. Contribution of epigenetic risk factors but not p53 codon 72 polymorphism to the development of cervical cancer in Northeastern Thailand. Cancer Lett. 2004;210:205-211. doi:10.1016/j.canlet.2004.03.039
- Muñoz N, Castellsagué X, Berrington de González A, Gissmann L. Chapter 1: HPV in the etiology of human cancer. Vaccine. 2006;24 Suppl 3:S3/1-10. doi:10.1016/j.vaccine.2006.05.115
- Jain M, Yadav D, Jarouliya U, Chavda V, Yadav AK, Chaurasia B, Song M. Epidemiology, Molecular Pathogenesis, Immuno-Pathogenesis, Immune Escape Mechanisms and Vaccine Evaluation for HPV-Associated Carcinogenesis. Pathogens. 2023;12(12). doi:10.3390/pathogens12121380
- Zohoncon TM, Ouedraogo TC, Brun LVC, Obiri-Yeboah D, Djigma WF, Kabibou S, Ouattara S, Gomina M, Yonli AT, Bazie VJTE, Ouedraogo C, Lompo O, Akpona SA, Simpore J. Molecular Epidemiology of High-Risk Human Papillomavirus in High-Grade Cervical Intraepithelial Neoplasia and in Cervical Cancer in Parakou, Republic of Benin. Pak J Biol Sci PJBS. 2016;19(2):49-56. doi:10.3923/pjbs.2016.49.56
- Clifford GM, Gallus S, Herrero R, Muñoz N, Snijders PJF, Vaccarella S, Anh PTH, Ferreccio C, Hieu NT, Matos E, Molano M, Rajkumar R, Ronco G, de Sanjosé S, Shin HR, Sukvirach S, Thomas JO, Tunsakul S, Meijer CJLM, Franceschi S, IARC HPV Prevalence Surveys Study Group. Worldwide distribution of human papillomavirus types in cytologically normal women in the International Agency for Research on Cancer HPV prevalence surveys: a pooled analysis. Lancet Lond Engl. 2005;366(9490):991-998. doi:10.1016/S0140-6736(05)67069-9
- Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri. Int J Gynecol Obstet. 2018;143:22-36. doi:10.1002/ijgo.12611
- Ferlay J, Colombet M, Soerjomataram I, Mathers C, Parkin DM, Piñeros M, Znaor A, Bray F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019;144(8):1941-1953. doi:10.1002/ijc.31937
- Marie Tebeu P, Saint Saba Antaon J, Adjeba M, Pikop F, Tsuala Fouogue J, Ndom P. Connaissances, attitudes et pratiques des professionnels de santé sur le cancer du col de l’utérus au Cameroun: Santé Publique. 2021;Vol. 32(5):489-496. doi:10.3917/spub.205.0489
- Mboumba Bouassa RS, Prazuck T, Lethu T, Meye JF, Bélec L. Cervical cancer in sub-Saharan Africa: an emerging and preventable disease associated with oncogenic human papillomavirus. Med Sante Trop. 2017;27(1):16-22. doi:10.1684/mst.2017.0648
- Debrah O, Agyemang-Yeboah F, Donkoh ET, Asmah RH. Prevalence of vaccine and non-vaccine human papillomavirus types among women in Accra and Kumasi, Ghana: a cross-sectional study. BMC Womens Health. 2021;21(1):372. doi:10.1186/s12905-021-01511-1
- Donkoh ET, Asmah RH, Agyemang-Yeboah F, Dabo EO, Wiredu EK. Prevalence and distribution of vaccine-preventable genital human papillomavirus (HPV) genotypes in Ghanaian women presenting for screening. Cancer Control. 2022;29:10732748221094721.
- Seyoum A, Assefa N, Gure T, Seyoum B, Mulu A, Mihret A. Prevalence and Genotype Distribution of High-Risk Human Papillomavirus Infection Among Sub-Saharan African Women: A Systematic Review and Meta-Analysis. Front Public Health. 2022;10:890880. doi:10.3389/fpubh.2022.890880
- Ogochukwu TN, Akabueze J, Ezeome IV, Aniebue UU, Oranu EO. Vaccination against human papilloma virus in adolescent girls: mother’s knowledge, attitude, desire and practice in Nigeria. J Infect Preve Med. 2017;5(151):2.
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int J Surg. 2010;8(5):336-341. doi:10.1016/j.ijsu.2010.02.007
- Madeleine KK, Djénéba O, Mahoukèdè ZT, Traore Fatié Porzé Wilfried, Gnoumou Ouamini Pulchérie De Prisca, Alice OR, Théophane YA, Prosper B, Paul O, Clarisse OTW, Edwige YT, Akouélé KKP, Dorcas OY, Ouedraogo Charlemagne Marie Ragnag-Néwendé, Jacques S. Molecular epidemiology of human papillomavirus in pregnant women in Burkina Faso. Biomol Concepts. 2022;13(1):334-340. doi:10.1515/bmc-2022-0026
- Djigma FW, Zohoncon TM, Douamba Z, Sorgho PA, Obiri-Yeboah D, Ouattara AK, Sagna T, Traore L, Ghilat-Avoid-Belem NW, Sanogo K, Sempore J, Yonli AT, Pietra V, Bisseye C, Ouedraogo C, Simpore J. Molecular Genotyping of Human Papillomavirus among HIV-infected and HIV-uninfected Women in Ouagadougou, Burkina Faso. Burkina Faso. 2020;8.
- Ouedraogo CMR, Djigma FW, Bisseye C, Sagna T, Zeba M, Ouermi D, Karou SD, Pietra V, Buelli F, Ghilat-Avoid-Belem NW, Sanogo K, Sempore J, Moret R, Pignatelli S, Nikiema JB, Simpore J. Épidémiologie et caractérisation des génotypes de papillomavirus humain dans une population de femmes à Ouagadougou. J Gynécologie Obstétrique Biol Reprod. 2011;40(7):633-638. doi:10.1016/j.jgyn.2011.05.012
- Salambanga C, Zohoncon TM, Traoré IMA, Ouedraogo RA, Djigma WF, Ouédraog C, Simpore J. High prevalence of high-risk human papillomavirus (HPV) infection among sexually active women in Ouagadougou. Médecine Santé Trop. 2019;29(3):302-305. doi:10.1684/mst.2019.0920
- Djigma FW, Ouédraogo C, Karou DS, Sagna T, Bisseye C, Zeba M, Ouermi D, Gnoula C, Pietra V, Ghilat-Avoid-Belem NW, Sanogo K, Sempore J, Pignatelli S, Ferri AM, Nikiema JB, Simpore J. Prevalence and genotype characterization of Human Papillomaviruses among HIV-seropositive in Ouagadougou, Burkina Faso. Acta Trop. 2011;117(3):202-206. doi:10.1016/j.actatropica.2010.12.007
- Zohoncon TM, Bisseye C, Djigma FW, Yonli AT, Compaore TR, Sagna T, Ouermi D, Ouédraogo CMR, Pietra V, Nikiéma JB, Akpona SA, Simpore J. Prevalence of HPV High-Risk Genotypes in Three Cohorts of Women in Ouagadougou (Burkina Faso). Mediterr J Hematol Infect Dis. 2013;5(1):e2013059. doi:10.4084/MJHID.2013.059
- Ouedraogo RA, Zohoncon TM, Guigma SP, Angèle Traore IM. Oncogenic human papillomavirus infection and genotypes characterization among sexually active women in Tenkodogo at Burkina Faso, West Africa. Papillomavirus Res. 2018;6:22-26. doi:10.1016/j.pvr.2018.09.001
- Ouedraogo RA, Zohoncon TM, Guigma SP, Ouattara AK, Simpore J. Prédominance du papillomavirus humain 56 dans une sous-population de femmes sexuellement actives à Garango, Centre-Est, Burkina Faso: Predominance of Human Papillomavirus 56 in a subpopulation of sexually active women in Garango, Central-East, Burkina Faso. J Appl Biosci. 2020;150(1):15499-15509.
- Ouedraogo RA, Zohoncon TM, Traore IMA, Ouattara AK, Guigma SP, Djigma FW, Obiri-Yeboah D, Ouedraogo C, Simpore J. Genotypic distribution of human oncogenic papillomaviruses in sexually active women in Burkina Faso: Central, Central-Eastern and Hauts-Bassins regions. Biomol Concepts. 2020;11(1):125-136. doi:10.1515/bmc-2020-0011
- Sawadogo B, Gitta SN, Rutebemberwa E, Sawadogo M. Knowledge and beliefs on cervical cancer and practices on cervical cancer screening among women aged 20 to 50 years in Ouagadougou, Burkina Faso, 2012: a cross-sectional study. Pan Afr Med J. 2014;18(175). doi:10.11604/pamj.2014.18.175.3866
- Compaore S, Ouedraogo CMR, Koanda S, Haynatzki G, Chamberlain RM, Soliman AS. Barriers to Cervical Cancer Screening in Burkina Faso: Needs for Patient and Professional Education. J Cancer Educ Off J Am Assoc Cancer Educ. 2016;31(4):760-766. doi:10.1007/s13187-015-0898-9
- Kagoné TS, Paré PG, Dembélé A, Kania D, Zida S, Bonané/Thiéba B, Ouédraogo A, Testa J, Simporé J, Méda N. Cervical cancer in the Hauts-Bassins region of Burkina Faso: Results of a screening campaign by visual inspection with acetic acid (VIA screening in Burkina Faso). Afr J Reprod Health. 2022;26(6):97-103.
- Tassembedo S, Winter CH, Traore IT, Ouattara A, Sawadogo M, Meda N. Cervical pre-cancer screening by visual inspection of the cervix after application of acetic acid in rural Burkina Faso: evaluation of women’s knowledge, screening practice habits, acceptability and prevalence of risk factors and lesions in Boussé health district. Pan Afr Med J. 2023;45:135. doi:10.11604/pamj.2023.45.135.36933
- Diendéré J, Kiemtoré S, Coulibaly A, Tougri G, Ily NI, Kouanda S. Low attendance in cervical cancer screening, geographical disparities and sociodemographic determinants of screening uptake among adult women in Burkina Faso: results from the first nationwide population-based survey. Rev DÉpidémiologie Santé Publique. 2023;71(4):101845. doi:10.1016/j.respe.2023.101845
- Traore IMA, Zohoncon TM, Dembele A, Djigma FW, Obiri-Yeboah D, Traore G, Bambara M, Ouedraogo C, Traore Y, Simpore J. Molecular Characterization of High-Risk Human Papillomavirus in Women in Bobo-Dioulasso, Burkina Faso. BioMed Res Int. 2016;2016:7092583. doi:10.1155/2016/7092583
- Ouattara S, Somé DA, Dembélé A, Sanfo S, Zohoncon T, Ouattara AK, Bambara M, Dao B, Simporé J. Molecular Epidemiology of High-Risk Human Papilloma Virus Infection in Sexually Active Women at Bobo-Dioulasso University Teaching Hospital. Open J Obstet Gynecol. 2019;09(08):1178-1188. doi:10.4236/ojog.2019.98114
- Tovo SF, Zohoncon TM, Dabiré AM, Ilboudo R, Tiemtoré RY, Obiri-Yeboah D, Yonli AT, Dovo EE, Ouédraogo RA, Ouattara AK, Sorgho PA, Ouermi D, Djigma FW, Ouédraogo C, Sangaré L, Simpore J. Molecular Epidemiology of Human Papillomaviruses, Neisseria gonorrhoeae, Chlamydia trachomatis and Mycoplasma genitalium among Female Sex Workers in Burkina Faso: Prevalence, Coinfections and Drug Resistance Genes. Trop Med Infect Dis. 2021;6(2):90. doi:10.3390/tropicalmed6020090
- Ilboudo R, Traoré EM, Zohoncon TM, Ouédraogo RA, Traore MA, Bado P, Ouédraogo C, Djigma FW, Obiri D, Sakandé J, Simpore J, Ouedraogo C. Prevalence and Characterization of High-Risk Human Papillomavirus Genotypes among a Group of Sex Workers in Ouagadougou, Burkina Faso. Burkina Faso. Published online 2020.
- Ouédraogo C, Zohoncon TM, Traoré EMA, Ouattara S, Bado P, Ouedraogo CT, Djigma FW, Ouermi D, Obiri-Yeboah D, Lompo O, Akpona SA, Simpore J. Distribution of High-Risk Human Papillomavirus Genotypes in Precancerous Cervical Lesions in Ouagadougou, Burkina Faso. Open J Obstet Gynecol. 2016;6(4):196-204. doi:10.4236/ojog.2016.64025
- Zohoncon TM, Bado P, Ouermi D, Traoré EMA, Ouattara S, Djigma FW, Traore IMA, Yonli AT, Obiri-Yeboah D, Ouédraogo C, Akpona SA, Lompo O, Simpore J. Molecular characterization of high-risk human papillomavirus genotypes involved in invasive cervical cancer from formalin-fixed, paraffin-embedded tissues in Ouagadougou, Burkina Faso. Int J Curr Res. 2016;8(09):39314-39318.
- Ouédraogo E, Zohoncon TM, Bayala B, Bado P, Da RPC, Ouedraogo RA, Traoré IMA, Kuassi-Kpede PA, Ouédraogo S, Dovo EE, Traoré L, Yonli AT, Djigma FW, Lompo OM, Simpore J. HPV/HBV or HPV/HCV Co-Infections in Women Treated for Chronic Hepatitis at Hôpital Saint Camille in Ouagadougou, Burkina Faso. Am J Mol Biol. 2024;14(01):1-12. doi:10.4236/ajmb.2024.141001
- Chikandiwa A, Kelly H, Sawadogo B, Ngou J, Pisa PT, Gibson L, Didelot MN, Meda N, Weiss HA, Segondy M, Mayaud P, Delany-Moretlwe S, Group on behalf of the HS. Prevalence, incidence and correlates of low risk HPV infection and anogenital warts in a cohort of women living with HIV in Burkina Faso and South Africa. PLOS ONE. 2018;13(5):e0196018. doi:10.1371/journal.pone.0196018
- Didelot-Rousseau MN, Nagot N, Costes-Martineau V, Vallès X, Ouedraogo A, Konate I, Weiss HA, Van de Perre P, Mayaud P, Segondy M, Yerelon Study Group. Human papillomavirus genotype distribution and cervical squamous intraepithelial lesions among high-risk women with and without HIV-1 infection in Burkina Faso. Br J Cancer. 2006;95(3):355-362. doi:10.1038/sj.bjc.6603252
- Adams AR, Nortey PA, Dortey BA, Asmah RH, Wiredu EK. Cervical human papillomavirus prevalence, genotypes, and associated risk factors among female sex workers in Greater Accra, Ghana. J Oncol. 2019;2019.
- Tounkara FK, Téguété I, Guédou FA, Goma-Matsétsé E, Koné A, Béhanzin L, Traoré S, Aza-Gnandji M, Keita B, Guenoun J, Coutlée F, Alary M. Human papillomavirus genotype distribution and factors associated among female sex workers in West Africa. Grce M, ed. PloS One. 2020;15(11):e0242711-e0242711. doi:10.1371/journal.pone.0242711
- Diop-Ndiaye H, Beiter K, Gheit T, Sow Ndoye A, Dramé A, McKay-Chopin S, Tommasino M, Bouh Boye CS, Sylla B, Kane CT. Human Papillomavirus infection in senegalese female sex workers. Papillomavirus Res Amst Neth. 2019;7:97-101. doi:10.1016/j.pvr.2019.02.003
- Morhason-Bello IO, Baisley K, Pavon MA, Adewole IF, Bakare RA, de San