

Hypothyroidism and Serum Creatine Kinase Levels in DTC
Correlation between hypothyroidism and serum creatine kinase levels
Mingzhen Guo1 Cheng Bing1, Yinhan Wang1, Xinya Cheng2
- Mingzhe Guo Department of Nuclear Medicine, The First Affiliated Hospital of Zhengzhou University
- Cheng BingDepartment of Nuclear Medicine, The First Affiliated Hospital of Zhengzhou University
- Yinhan Wang Department of Nuclear Medicine, The First Affiliated Hospital of Zhengzhou University
- Xinya Cheng Hong Kong Baptist University
OPEN ACCESS
PUBLISHED: April 30 2025
CITATION: GUO, Mingzhen et al. Correlation between hypothyroidism and serum creatine kinase levels. Medical Research Archives, [S.l.], v. 13, n. 4, apr. 2025. Available at: <https://esmed.org/MRA/mra/article/view/6426>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i4.6426
ISSN 2375-1924
Abstract
Objective: To investigate the correlation between hypothyroidism and serum creatine kinase (CK) levels in patients with differentiated thyroid cancer (DTC) during radioactive iodine (131I) therapy following total thyroidectomy.
Methods: This prospective study enrolled 170 DTC patients (50 males and 120 females) with a mean age of 39.41±9.45 years, who were treated at the First Affiliated Hospital of Zhengzhou University from January 2023 to June 2023. Thyroid-related hormones and serum CK levels were measured at two time points: one month postoperatively (before 131I therapy) and seven months postoperatively (before 131I therapy follow-up), both under hypothyroid conditions. Paired t-tests (two-tailed) were used to compare changes in serum biomarkers between the two time points within the same patients, and Pearson correlation analysis (correlation coefficient r) was employed to assess the relationship between thyroid-related hormones and serum CK levels.
Results: At one month postoperatively (before 131I therapy), the mean serum CK level in hypothyroid DTC patients was 160.22±130.95 U/L, with mean FT3, FT4, and TSH levels of 2.89±0.60 pmol/L, 1.87±130.98 pmol/L, and 135.99±68.23 mIU/L, respectively. At seven months postoperatively (before 131I therapy follow-up), the mean serum CK level increased to 253.80 ±429.10 U/L, while mean FT3, FT4, and TSH levels were 3.29±0.58 pmol/L, 1.84±422.61 pmol/L, and 109.87±53.02 mIU/L, respectively. A significant difference was observed in serum CK levels between one month and seven months postoperatively (t = -2.94, p = 0.004). Pearson correlation analysis revealed a negative correlation between FT3 and serum CK levels at both one month (r = -0.196, p = 0.01) and seven months (r = -0.153, p = 0.047) postoperatively.
Conclusion: The elevation of serum CK levels in DTC patients after total thyroidectomy is primarily attributed to hypothyroidism rather than surgical trauma, with FT3 being a key contributing factor. These findings highlight the importance of closely monitoring thyroid function and CK levels in postoperative DTC patients to optimize clinical management strategies.
Keywords
Hypothyroidism; Creatine kinase; Thyroid hormone; Thyroid-stimulating hormone; Myalgia
Introduction
Creatine Kinase (CK) is a crucial enzyme involved in cellular energy metabolism and muscle function. This enzyme consists of three isoenzymes: CK-MM (primarily found in skeletal muscle), CK-MB (primarily found in cardiac muscle), and CK-BB (primarily found in brain tissue). Elevated serum CK levels can result from various physiological and pathological factors, including intense physical activity (such as marathons, fitness training, and stretching), crush injuries (e.g., crush syndrome), burns, electric shock, fractures, muscle twitching (e.g., seizures or chills), toxic muscle damage (e.g., from excessive alcohol consumption or crayfish ingestion), electrolyte imbalances (e.g., hypokalemia), hypothyroid myopathy, hyperthermia, fever, and medication use (e.g., statins, beta-blockers, psychotropic drugs, and herbal remedies).
Thyroid tissue and differentiated thyroid cancer cells possess the unique ability to absorb 131I, which forms the theoretical basis for 131I therapy in differentiated thyroid cancer. Through its internal radiation effects, 131I effectively eliminates residual thyroid tissue and cancer cells post-surgery, thereby achieving therapeutic outcomes. Prior to conventional 131I therapy, patients with differentiated thyroid cancer are typically required to discontinue levothyroxine sodium tablets (e.g., Synthroid) for 3 to 4 weeks. This approach aims to induce a hypothyroid state artificially, thereby stimulating the secretion of thyroid-stimulating hormone (TSH) and enhancing the uptake of 131I by residual thyroid tissue and cancer cells, ultimately improving treatment efficacy.
Hypothyroidism is defined by significantly elevated TSH levels (TSH >10μIU/ml), accompanied by reduced levels of free thyroxine (FT4) and free triiodothyronine (FT3), along with the presence of typical clinical signs and symptoms of hypothyroidism. Research indicates that hypothyroid patients may exhibit elevated serum CK and other muscle enzymes. Notably, CK elevation due to hypothyroidism is typically not associated with a significant increase in CK-MB (primarily of myocardial origin), and the CKMB/CK ratio is significantly lower, distinguishing it from myocardial injury (where CKMB/CK is markedly elevated). In addition to the classic clinical manifestations well-known to endocrinologists (e.g., lethargy, cold intolerance, and depressed mood), hypothyroid patients frequently report muscle-related symptoms, including exercise intolerance, myalgia, muscle spasms, stiffness, and myxedema, all of which significantly impair patients’ quality of life.
Clinical observations have revealed that patients with differentiated thyroid cancer often report the aforementioned muscle-related symptoms accompanied by elevated serum CK levels within six months following total thyroidectomy. This phenomenon may be attributed to muscle damage caused by the surgery or a series of physiological responses induced by hypothyroidism. The aim of this study is to investigate the correlation between hypothyroidism and serum CK levels.
Information and Methods
1. Study Subjects.
This study was a prospective clinical study, approved by the Research and Clinical Trial Ethics Committee of our hospital, and all patients signed a written informed consent. This study included a total of 170 patients who underwent total thyroidectomy for differentiated thyroid cancer at the First Affiliated Hospital of Zhengzhou University between January 2023 and June 2023 (with detailed surgical records and imaging tests confirming complete removal of the lesion), were scheduled for 131I therapy, and completed postoperative follow-up.
Inclusion Criteria: 1. Patients exhibit no clinical signs or symptoms associated with myalgia. 2. During the study period, patients did not receive any medication unrelated to radioactive iodine therapy, except for levothyroxine (LT4). 3. Levothyroxine sodium was discontinued for at least 3 weeks prior to the 1-month and 7-month postoperative iodine therapy follow-ups. 4. Patients have complete clinical data available for effective analysis.
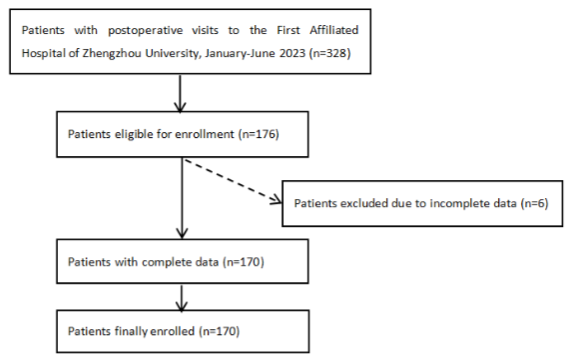
Exclusion Criteria: 1. Patients with a history or current diagnosis of severe systemic diseases, including but not limited to: Malignancies other than differentiated thyroid cancer; Autoimmune diseases (e.g., systemic lupus erythematosus, rheumatoid arthritis); Diabetes and chronic kidney disease (CKD≥stage 3). 2. Use of medications that may interfere with study outcomes, including: Statins (e.g., atorvastatin, simvastatin); Immunosuppressants (e.g., cyclosporine, methotrexate); Glucocorticoids (e.g., prednisone, dexamethasone). 3. Pregnancy-related exclusions: Positive HCG test; Pregnant or lactating women; Patients planning to become pregnant within 6 months. This study ultimately included 170 patients, consisting of 50 males and 120 females, with an average age of (39.41 ± 9.45) years (the screening and enrollment process is shown in Figure 1).
Collected clinical data included age, sex, height, and weight, with body mass index (BMI) calculated using the formula weight (kg)/height (m)². Blood pressure was measured for all patients after 10 minutes of rest. Additionally, a comprehensive medical history, including a history of myalgia, was recorded in detail.
2. Research Methods.
Measure serum creatine phosphokinase (CPK) levels in patients with differentiated thyroid cancer who underwent total thyroidectomy at 1 month and 7 months postoperatively, following radioactive iodine therapy. Blood samples were collected after an 8-hour overnight fast. Following collection, the samples were allowed to stand for 60 minutes and centrifuged within 2 hours at room temperature (20-25°C) under conditions of 3000-3800 r/min for 10-15 minutes to obtain optimal serum. Serum levels of FT3, FT4, and TSH were measured using a commercially available automated chemiluminescence system kit (Beckman Coulter, Inc., USA) and the UniCel Dxl Access immunoassay system. Serum creatine kinase levels were determined using a commercially available creatine kinase assay kit (colorimetric method) (Roche Diagnostics Products Shanghai Co., Ltd.).
3. Statistical Analysis.
Normally distributed quantitative data are presented as mean ± standard deviation(𝑋̅±s). Normality was tested using the Kolmogorov-Smirnov test. Differences within the same group before and after intervention were analyzed by the paired Student’s t-test (two-tailed). Linear correlations between variables were assessed via Pearson’s bivariate correlation analysis, with the correlation coefficient (r) and its 95% confidence interval (95% CI) reported. A statistical significance threshold was set at P < 0.05. All analyses were two-tailed and performed using SPSS 27.0 software (IBM SPSS, Armonk, NY, USA).
Results
1. Comparison of Clinical Data on Hypothyroid Status at 1 Month and 7 Months Postoperatively in Patients with DTC.
The serum CK and thyroid function parameters of the study group are shown in Table 1. In patients with DTC, the average CK level at 1 month postoperatively was 160.22 ± 130.95 U/L, the average FT3 level was 2.89 ± 0.60 U/L, the average FT4 level was 1.87 ± 130.98 U/L, and the average TSH level was 135.99 ± 68.23 U/L. At 7 months postoperatively, the average CK level was 253.80 ± 429.10 U/L, the average FT3 level was 3.29 ± 0.58 U/L, the average FT4 level was 1.84 ± 422.61 U/L, and the average TSH level was 109.87 ± 53.02 U/L. Statistically significant differences were observed in serum creatine kinase levels between 1 month and 7 months postoperatively, with CK levels significantly higher at 7 months compared to 1 month. Similarly, significant differences were noted in FT3 and TSH levels, with FT3 levels higher and TSH levels lower at 7 months compared to 1 month.
| groups | BMI (kg /m2) | Systolic/diastolic blood pressure (mmHg) | FT3 (U/L) | FT4 (U/L) | TSH (U/L) | CK (U/L) |
|---|---|---|---|---|---|---|
| 1 month after surgery | 20.76±2.42 | 125.0±8.77/78.0±8.87 | 2.89±0.60 | 1.87±130.98 | 135.99±68.23 | 160.22±130.95 |
| 7 months after surgery | 20.89±2.33 | 121.3±10.93/77.2±8.82 | 3.29±0.58 | 1.84±422.61 | 109.87±53.02 | 253.80±429.10 |
t-value -0.45 1.62/1.71 -7.63 0.14 -26.19 -2.94
p-value 0.66 0.14/0.12 <0.001 0.89 <0.001 0.004
p<0.05 was statistically significant.
2. Results of Pearson Correlation Analysis.
In patients with DTC, FT3 levels showed a significant negative correlation with serum creatine kinase at both 1 month and 7 months postoperatively under hypothyroid conditions (r = -0.196, p = 0.01; r = -0.153, p = 0.047).
Discussion
It has been documented that hypothyroidism is often associated with skeletal muscle damage, with serum CK concentrations significantly elevated in 57%-90% of patients. The American Thyroid Association (ATA) guidelines emphasize that elevated CK is a common manifestation of hypothyroid myopathy and recommend thyroid function screening as a routine test for unexplained hyperCKemia. Studies have shown that serum CK levels are positively correlated with serum TSH and negatively correlated with FT3 and FT4, and are associated with the severity of biochemical hypothyroidism, but not with the severity of clinical muscle symptoms. The pathophysiological mechanisms of hypothyroid myopathy have not been fully elucidated, with one possible mechanism being abnormal glycogenolysis and oxidative metabolism. Thyroid hormone deficiency leads to the deposition of mucopolysaccharides and mucoproteins in skeletal muscle tissue, causing muscle myxedema, muscle fiber hypertrophy, vacuolar degeneration, and even rupture and necrosis, resulting in the leakage of muscle enzymes from cells, which is the primary cause of elevated CK levels. Additionally, reduced Triiodothyronine (T3) levels in hypothyroidism may impair CK clearance, further contributing to elevated serum CK. Furthermore, hypothyroidism leads to decreased intracellular protein synthesis, reduced mitochondrial respiratory enzymes, and decreased ATP production, resulting in impaired calcium homeostasis in muscle cells (e.g., decreased sarcoplasmic reticulum Ca²⁺-ATPase activity), which in turn causes cellular damage and CK release. These mechanisms collectively may play a key role in the development and progression of hypothyroid myopathy.
The main findings of this study are as follows: First, in patients with DTC undergoing 131I therapy after total thyroidectomy, serum CK levels were significantly elevated during hypothyroidism and negatively correlated with FT3 levels. Second, compared to one month postoperatively, serum CK levels were further elevated at seven months postoperatively, accompanied by increased FT3 levels and decreased TSH levels, with no positive correlation observed between serum CK levels and the severity of hypothyroidism.
Various factors may influence serum CK levels, including age, sex, medications, and other medical conditions. In this study, due to the potential side effects of analgesics (e.g., gastrointestinal ulcers and bleeding, cardiovascular thrombosis risks, and hepatorenal toxicity), none of the included patients used analgesic medications. Additionally, no other conditions in the study participants interfered with the assessed parameters, making thyroid hormone and TSH levels the only variables that changed during the study.
The elevated CK levels observed one month postoperatively may be related to muscle damage caused by surgical trauma, while the further increase in CK levels at seven months postoperatively compared to one month may be attributed to hypothyroidism. Thyroid hormone levels, particularly FT3, appear to directly regulate serum CK levels. This finding provides important insights for further exploring the relationship between thyroid function and muscle metabolism.
A case report from Peking University Third Hospital described a patient with myopathy induced by rapid correction of hyperthyroidism (or relative hypothyroidism). A 25-year-old female patient with severe hyperthyroidism developed fatigue and myalgia after seven weeks of methimazole (MMI) treatment. Laboratory tests revealed significantly elevated serum CK levels, while FT3 and FT4 levels had returned to the normal range. After discontinuation of MMI, the patient’s muscle symptoms rapidly resolved with the recurrence of hyperthyroidism and normalization of CK levels. Subsequently, the patient underwent 131I treatment, and similar muscle symptoms reappeared when FT3 and FT4 levels dropped to the normal range. This time, L-T4 replacement therapy was administered, leading to rapid symptom improvement. This finding provides important clinical evidence for the prevention and management of myopathy caused by hypothyroidism.
Conclusion
In conclusion, in patients with DTC undergoing 131I therapy after total thyroidectomy, elevated serum CK levels during hypothyroidism may not be primarily caused by surgical trauma but are significantly associated with postoperative hypothyroidism, with changes in FT3 levels playing a major regulatory role. However, due to the limited number of cases included in this study, potential confounding factors (e.g., different surgical approaches) may not have been fully assessed. Therefore, future prospective studies with larger sample sizes are needed to further validate these findings and explore the relationship between thyroid function and serum CK levels, as well as the underlying mechanisms.
Declaration of interests:
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Author Contribution
Mingzhen Guo: Designed the research plan and wrote the initial draft, and was responsible for data collection, analysis, and visualization.
Cheng Bing: Responsible for overall project coordination and funding acquisition, and supervised and guided the research results.
Yinhan Wang: Participated in experimental design and methodology optimization, and performed data validation and statistical analysis.
Xinya Cheng: Provided clinical samples and technical support for the research, and participated in manuscript review and revision.
References:
- Zhang H, To KK. Serum creatine kinase elevation following tyrosine kinase inhibitor treatment in cancer patients: symptoms, mechanism, and clinical management. Clin Transl Sci. 2024;17(11):e70053. doi:10.1111/cts.70053.
- Thompson PD, Clarkson P, Karas RH. Statin-associated myopathy. JAMA. 2003;289(13):1681-1690. doi:10.1001/jama.289.13.1681.
- Matrone A, Campopiano MC, Nervo A, et al. Differentiated thyroid cancer, from active surveillance to advanced therapy: toward a personalized medicine. Front Endocrinol (Lausanne). 2019;10:884. doi:10.3389/fendo.2019.00884.
- Pacini F, Fuhrer D, Elisei R, et al. 2022 ETA consensus statement: what are the indications for postsurgical radioiodine therapy in differentiated thyroid cancer? Eur Thyroid J. 2022;11(1). doi:10.1159/000521234.
- Almandoz JP, Gharib H. Hypothyroidism: etiology, diagnosis, and management. Med Clin North Am. 2012;96(2):203-221. doi:10.1016/j.mcna.2012.01.005.
- Sindoni A, Rodolico C, Pappalardo MA, et al. Hypothyroid myopathy: a peculiar clinical presentation of thyroid failure. Review of the literature. Rev Endocr Metab Disord. 2016;17(4):499-519. doi:10.1007/s11154-016-9383-y.
- Ramadhan A, Schondorf R, Tamilia M. Rhabdomyolysis and peroneal nerve compression associated with thyroid hormone withdrawal in the setting of remnant ablation: review of the literature. Endocr Pract. 2011;17(4):629-635. doi:10.4158/EP10345.RA.
- Benvenga S, Toscano A, Rodolico C, et al. Endocrine evaluation for muscle pain. J R Soc Med. 2001;94(8):405-407. doi:10.1177/014107680109400808.
- McKeran RO, Slavin G, Ward P, et al. Hypothyroid myopathy. A clinical and pathological study. J Pathol. 1980;132(1):35-54. doi:10.1002/path.1711320106.
- Shaheen D, Kim CS. Myositis associated with the decline of thyroid hormone levels in thyrotoxicosis: a syndrome? Thyroid. 2009;19(12):1413-1417. doi:10.1089/thy.2009.0279.
- Garber JR, Cobin RH, Gharib H, et al. Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Thyroid. 2012;22(12):1200-1235. doi:10.1089/thy.2012.0205.
- Hekimsoy Z, Oktem IK. Serum creatine kinase levels in overt and subclinical hypothyroidism. Endocr Res. 2005;31(3):171-175.
- Ferrari SM, Fallahi P, Galetta F, et al. Thyroid disorders induced by checkpoint inhibitors. Rev Endocr Metab Disord. 2018;19(4):325-333.
- Ni J, Zhang L, Zhang X. Marked elevation of creatine phosphokinase alone caused by sintilimab—beware of hypothyroid myopathy. Eur J Cancer. 2020;128:57-59.
- Zhou J, Gauthier K, Ho JP, et al. Thyroid hormone receptor α regulates autophagy, mitochondrial biogenesis, and fatty acid use in skeletal muscle. Endocrinology. 2021;162(8).
- Harper ME, Monemdjou S, Ramsey JJ, et al. Age-related increase in mitochondrial proton leak and decrease in ATP turnover reactions in mouse hepatocytes. Am J Physiol Endocrinol Metab. 1998;275(2):E197-E206.
- He H, Giordano FJ, Hilal-Dandan R, et al. Overexpression of the rat sarcoplasmic reticulum Ca²⁺ ATPase gene in the heart of transgenic mice accelerates calcium transients and cardiac relaxation. J Clin Invest. 1997;100(2):380-389.
- Berchtold MW, Brinkmeier H, Müntener M. Calcium ion in skeletal muscle: its crucial role for muscle function, plasticity, and disease. Physiol Rev. 2000;80(3):1215-1265.
- Bjarnason I, Scarpignato C, Holmgren E, et al. Mechanisms of damage to the gastrointestinal tract from nonsteroidal anti-inflammatory drugs. Gastroenterology. 2018;154(3):500-514.
- McGettigan P, Henry D. Cardiovascular risk with non-steroidal anti-inflammatory drugs: systematic review of population-based controlled observational studies. PLoS Med. 2011;8(9):e1001098.
- Larson AM, Polson J, Fontana RJ, et al. Acetaminophen-induced acute liver failure: results of a United States multicenter, prospective study. Hepatology. 2005;42(6):1364-1372.
- Fored CM, Ejerblad E, Lindblad P, et al. Acetaminophen, aspirin, and chronic renal failure. N Engl J Med. 2001;345(25):1801-1808.
- Lu R, Wang H, Hong T, et al. Myopathy after rapid correction of hyperthyroidism: a case report and review of literature. Medicine (Baltimore). 2020;99(3):e18878. doi:10.1097/MD.0000000000018878.