

Impact of Scatter Bed Hospice Unit on Palliative Care Utilization
Impact of a Scatter Bed Hospice Unit (SBHU) on Palliative Care Utilization in an Academic Medical Center
Christian Voto, DO1; Raj Patel, MD1; Edith Burns, MD1,2; Hayley Fried, DO1; Alexander Rimar, MD1
- Northwell Health, Department of Medicine, Division of Geriatrics and Palliative Care, New Hyde Park, NY, USA
- Zucker School of Medicine at Hofstra/Northwell, Hempstead, NY, USA
OPEN ACCESS
PUBLISHED: 31 December 2025
CITATION: Voto, C., Patel, R., et al., 2025. Impact of a Scatter Bed Hospice Unit (SBHU) on Palliative Care Utilization in an Academic Medical Center. Medical Research Archives, [online] 13(12). https://doi.org/10.18103/mra.v13i12.7134
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i12.7134
ISSN 2375-1924
ABSTRACT
Introduction: Inpatient palliative units increase the utilization of palliative and hospice services, and are associated with greater patient and caregiver satisfaction, and lower cost at end of life. Not all hospital settings can accommodate a dedicated palliative unit due to limitations in space, staffing, and cost. An alternative model, such as the Scatter Bed Hospice Unit (SBHU), which disperses hospice patients amongst those requiring standard acute care has been proposed. Despite its potential, limited data exists on the effectiveness of this model. This initiative aimed to increase palliative and hospice utilization through implementation of a SBHU within an academic acute care facility.
Methods: In December 2022, a Scatter Bed Hospice Unit (SBHU) was implemented at an urban tertiary care hospital. Retrospective chart review was conducted of patients who received palliative care consultation during the six months prior to SBHU implementation (July–December 2022) and the six months following implementation (January–June 2023). The primary aims were to perform a pre-post assessment of the number of Geriatric and Palliative (GAP) consultations and patients discharged with hospice services. Secondary outcomes included documented goals of care discussions, patients with comfort measures orders, patients who expired without hospice enrollment, reasons for GAP consultation, and time from hospice referral to admission.
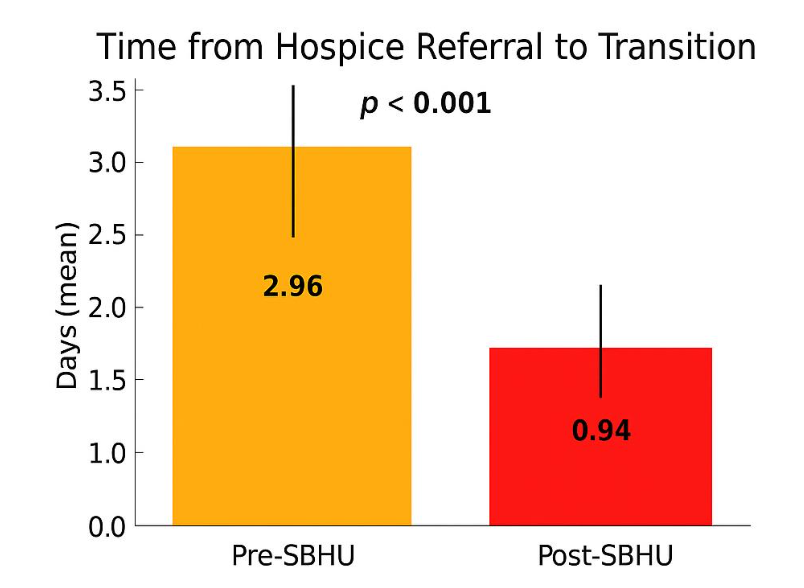
Results: There was a significant increase in GAP consults (p=0.0021) post-implementation of our SBHU. The number of patients discharged with hospice services, documented goals of care discussions, and patients with comfort measures orders all showed increasing trends (non-significant). Amongst patients with a comfort measures order, there was a significant increase in patients discharged with hospice services from 32.7% vs 44.7% post SBHU implementation (p = 0.02). Post-SBHU, the time from inpatient hospice referral to hospice admission decreased from nearly three days to less than one (p < 0.001).
Conclusions: The SHBU improved utilization of palliative and hospice services through increased consultation and overall hospice enrollment amongst terminally ill patients. Transition to hospice care is more efficient with this model as evidenced by decreased time from inpatient hospice referral to hospice admission post-implementation of the SBHU model.
Key Message: Implementation of an inpatient scatter bed hospice was associated with greater use of palliative care consultation, increased documentation of goals-of-care, increased hospice utilization, and reduced time from hospice referral to transition.
Keywords:
Hospice Utilization, Palliative Care, Goals of care, Scatter bed hospice unit, Inpatient palliative unit
Introduction
The integration of palliative care with primary inpatient teams enables a comprehensive and patient-centered approach to care. Palliative care has been shown to improve patients’ quality of life, preserve dignity, support informed decision-making, enhance satisfaction, and reduce healthcare costs. Multiple randomized controlled trials evaluating early palliative care interventions in advanced illnesses such as cancer and Parkinson’s disease have demonstrated clinically meaningful improvements in both quality of life and survival. Similar benefits have been reported for caregivers’ mental health and quality of life. For example, family caregivers of patients with recently diagnosed lung or gastrointestinal malignancies experienced significantly lower psychological distress, depression, and anxiety symptoms at three and six months before the patient’s death when early palliative care consultations were provided. Despite these well-documented benefits, palliative care services remain underutilized.
Several barriers to palliative care utilization have been identified including (1) limited interaction between primary inpatient providers and the palliative care team, (2) provider attitudes toward palliative care, (3) inadequate education and training, (4) negative perceptions of palliative care by patients and families, and (5) a misunderstanding of the role of palliative care. Common misconceptions include the belief that palliative care is synonymous with hospice care or is a “last resort” limited to end-of-life situations. Addressing these misconceptions is critical to fostering earlier integration of palliative care, improving patient outcomes, and optimizing healthcare utilization.
Proposed strategies to overcome these barriers include increased “marketing and promotion” of palliative care among physicians and targeted educational interventions. The concept of “strategic visibility,” in which palliative care providers maintain a stronger presence on general wards to facilitate interprofessional collaboration and communication, has been shown to be effective in prior research. One such approach to increase the visibility and utilization of palliative care in the inpatient setting is the development of inpatient palliative units (IPUs) within hospitals. Traditionally, IPUs function as closed units with their own nurses, case managers, social workers, and managing geriatrics and palliative teams.
Inpatient palliative units (IPU) have been associated with numerous benefits for end-of-life care, including improved utilization of palliative and hospice services, increased patient and caregiver satisfaction, and reduced healthcare costs. Several studies have shown that the development of an IPU leads to greater clarification of patient goals of care, as evidenced by higher rates of code status changes and comfort measures orders among seriously ill patients. One study demonstrated that hospice utilization and inpatient hospice length of stay increased following the implementation of a traditional IPU, as terminally ill patients were able to access these services more easily and in a timelier manner. Another found that the creation of an IPU significantly reduced ICU mortality and length of stay by facilitating the transition of terminally ill patients out of the ICU for end-of-life care. This not only reduced costs associated with prolonged ICU stays but also enabled patients and families to receive care more consistent with their goals and preferences—such as more liberal visiting hours, fewer invasive procedures, less intensive monitoring, and more effective pain and symptom management.
While the benefits of inpatient palliative units (IPU) are well established, not all hospitals have the resources to provide dedicated units. Successful IPUs require a consistently high census of appropriate patients to maintain bed utilization, which may not be feasible for institutions with fluctuating patient volumes or lower acuity populations. In addition, some hospitals face space constraints and/or have limited availability of palliative care–trained staff, further challenging the establishment of a dedicated unit.
An alternative scatter bed model—where hospice patients are dispersed among other medical patients on existing hospital floors—may be used to deliver inpatient hospice-level care. Although this approach is not a novel concept, there is limited data on its effectiveness in improving the utilization of palliative and hospice services. This study evaluates the impact of implementing an inpatient scatter bed hospice unit (SBHU) on palliative care and hospice service utilization. We hypothesized that increasing direct access to the palliative care team through the SBHU would encourage primary inpatient care providers to utilize palliative care more frequently and for a broader range of clinical needs, such as hospice referral and symptom management.
Methods:
This quality improvement study was reviewed by the IRB and determined to be exempt from formal review.
SCATTER BED MODEL
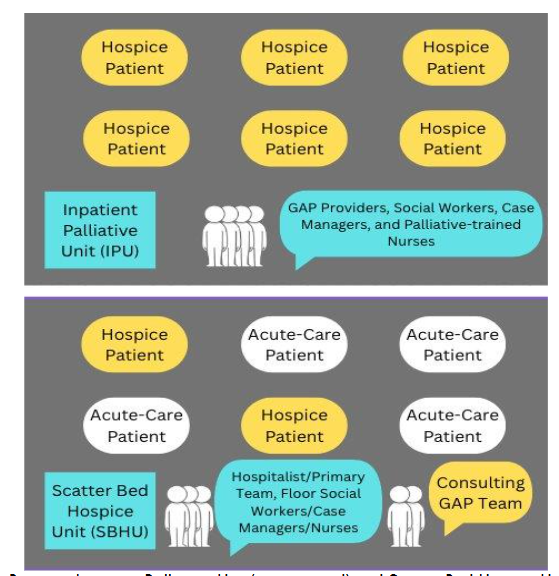
In December 2022, a scatter bed model was implemented to provide inpatient hospice care for terminally ill patients requiring acute end-of-life care. This included community hospice patients directly admitted from the ER for acute symptom stabilization. In this model, patients were dispersed among other hospitalized patients requiring standard acute care within one medical unit, creating a distinct area within the hospital for this purpose.
The model provided services in key domains of palliative care including management of actively dying patients, pain and symptom management, advanced care planning, and hospice referral. Patients admitted to the scatter bed hospice unit (SBHU) were co-managed by the Geriatrics and Palliative Care (GAP) team and the general hospitalist teams. They also had access to GAP social workers and other supportive services. Team members participated in daily interdisciplinary rounds to assist with symptom management and discharge planning.
The daily unit census varied from one to four patients depending on demand. Withdrawal of interventions such as mechanical ventilation or continuous inotropic medications was not performed in this unit; these treatments were discontinued in the intensive care unit prior to transfer.
IMPLEMENTATION PROCESS
This quality improvement initiative was preceded by identifying a critical need for dedicated inpatient hospice beds to enhance end-of-life care. Prior to implementation, patients requiring inpatient hospice care were either transferred to outside hospice facilities or received end-of-life care in the hospital without formal hospice enrollment. Dependence on external bed availability was a major barrier to hospice enrollment for patients who were too ill to be discharged home or safely transported to another facility.
To implement this model, the GAP team engaged hospital leadership, including the Chief Medical Officer and the Quality Department, to gain support for the initiative. Leadership then facilitated a collaborative partnership and contracted with a local hospice agency. This included a quarterly review of quality metrics (e.g., length of stay, number of deaths, average daily census, time from referral to admission).
The hospice partner and in-house GAP team presented overviews of the hospice benefit, the proposed model of care, and the referral process at staff meetings for the Division of Hospital Medicine. Process maps were distributed to the Internal Medicine Residency program, and an internal memo was sent to all other service lines within the hospital. Nurses received both in-person training and online module assessments with certifications provided by the hospice agency.
The internal informatics team assisted with integration of workflow and metrics into the electronic medical record, incorporating flags that clearly identified patients admitted to the hospice service. Bed Management assisted in establishing procedures for transferring patients into private rooms within the SBHU, ensuring smooth operational flow. Communication with bed management and care team members was streamlined using a team collaboration platform. This facilitated timely identification of potential palliative care consults and improved handoffs for patients transitioning to inpatient hospice.
PROGRAM SETTING AND EVALUATION
The SBHU was established within a 632-bed tertiary care hospital located in a major urban metropolitan area and part of a large integrated healthcare system. A retrospective review of all palliative care consultations during the 6 months preceding (July 1, 2022–December 31, 2022) and the 6 months following (January 1, 2023–June 30, 2023) implementation was conducted to evaluate impact.
DATA COLLECTION
Data was collected through EMR review of all patients receiving a GAP consult during the specified time periods (pre- and post-implementation). Demographic, clinical and process measures included: age, sex, race/ethnicity, primary diagnosis, reason for GAP consultation, discharge disposition, number of goals-of-care notes, whether a comfort measures order was placed, and time from hospice referral to hospice admission.
The reason for GAP consult was taken from the first listed problem on the initial consult note. All patients who received a palliative care consultation during the study period—regardless of age, admitting service, or diagnosis—were included in the analysis.
MEASURES
The primary aim of the study was to perform a pre–post assessment of (1) the number of Geriatrics and Palliative Care (GAP) consultations and (2) the number of patients discharged with hospice services. Because the total number of hospitalized patients differed between the two time periods, relative proportions were used when comparing these endpoints.
Patients discharged with hospice services included those discharged to the SBHU as well as those discharged home with hospice or to an outside inpatient hospice facility. For analyses of hospice utilization, we further stratified the data to examine proportions among (1) all patients receiving GAP consultation and (2) patients with a comfort measures order who were discharged with hospice services.
Secondary outcome measures included documentation of goals-of-care discussions, the number of patients with comfort measures orders, the number of patients who expired in the hospital without hospice enrollment, reasons for GAP consultation, and time from inpatient hospice referral to hospice admission.
STATISTICAL ANALYSIS
Categorical variables were reported as frequencies and percentages, whereas continuous variables were summarized using means and 95% confidence intervals (CIs). Comparisons between pre- and post-intervention measures were performed using t-tests for continuous variables and chi-square or z-tests for categorical variables, as appropriate. A two-sided p-value < 0.05 was considered statistically significant.
Results:
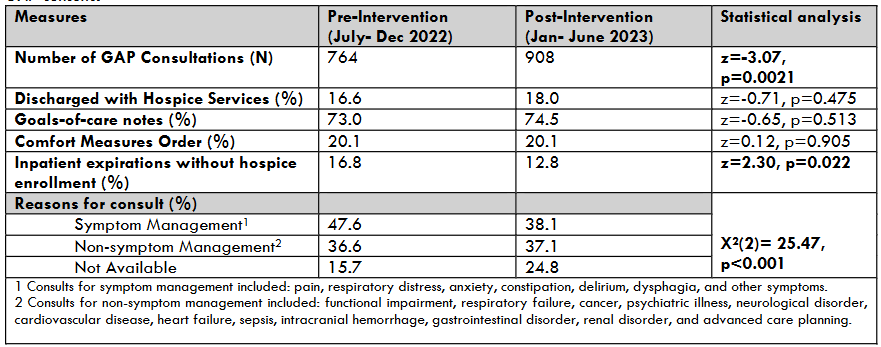
The total number of adult patients admitted to the hospital during the pre-intervention period was 13,461 and 13,824 in the post-intervention period. The number of Geriatrics and Palliative Care (GAP) consults increased from 764 during the pre-intervention period to 908 during the post-intervention period, representing a rise from 5.7% to 6.6% post-scatter bed hospice unit (SBHU) implementation (z = -3.07, p=0.0021).
Patients seen in GAP consultation pre- and post-SBHU were similar in age- mean + SD 78.2 + 14.9 vs. 78.3 + 14.6, (t=-0.14, p=0.89), proportion of women (51.6% vs. 54%) (X2(2)= 1.41, p=0.49), and race (X2(6)= 5.88, p=0.44). The proportion of consults for patients aged greater than 65 was 82.3% and 85.7% respectively (z=-1.87, p=0.0615).
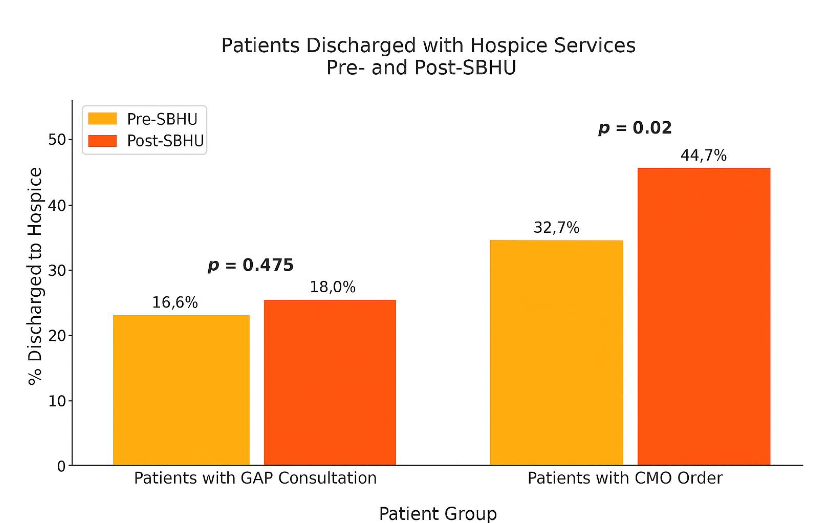
Among those receiving GAP consults, the total number of patients discharged with hospice services trended upwards, 16.6 vs 18% (z=-0.71, p=0.475). Similarly, the number of patients with documented goals-of-care notes also showed a non-significant increase, 73% vs 74.5% (z= -0.65, p=0.513). Patients with a comfort measures order designation remained stable post- SBHU implementation, 20.1% for both time periods (z=0.12, p=0.905). Inpatients who expired without hospice enrollment decreased significantly post-SBHU implementation (16.8% vs 12.8%) (z=2.30, p=0.022). The proportion of consults for symptom management significantly decreased in the post-intervention period (47.6% vs 38.1%) (X2(2)= 25.47, p<0.001) while the proportion where reasons were “not available” increased.
During the post-intervention period, a total of 163 patients were discharged with hospice services. Of these, 49 patients were admitted to the SBHU, while the remaining were discharged either with home hospice or to external hospice-capable facilities. The average time from inpatient hospice referral to admission to the SBHU was 0.94 days, compared to 2.96 days prior to implementation, when patients were referred to outside inpatient hospice facilities (p < 0.001).
Discussion:
This retrospective study examined hospitalized patients at a tertiary care facility pre-and post-implementation of a scatter bed hospice unit (SBHU) over a total 12-month period. The implementation of the SBHU was associated with increased Geriatrics and Palliative (GAP) consultations and decreased number of inpatient expirations without hospice enrollment. Among patients with a comfort measures order, hospice utilization increased significantly (i.e., use of SBHU), with a significantly shortened interval from hospice referral to admission.
The observed increase in GAP consultations likely reflects enhanced visibility of and access to the palliative care team following SBHU implementation. The significant increase in hospice utilization among patients with a comfort measures order, along with the reduction in time from hospice referral to admission and the decrease in inpatient deaths without hospice enrollment, suggests that the SBHU facilitated more timely hospice transitions and promoted care that was better aligned with patients’ goals and preferences.
There were trends of increased goals-of-care notes, comfort measures orders, and overall hospice enrollment following SBHU implementation, which accompanied the significant increase in GAP consultations. These changes, however, did not reach statistical significance. A likely explanation is that these outcomes were analyzed as proportions of the total number of GAP consultations. As consultation volume grew, the relative proportions of these measures remained stable, diminishing the likelihood of detecting significance. In other words, the increase in consultations may have created more opportunities for these outcomes without raising their probability on a per-consult basis.
We observed a decrease in the proportion of consultations for symptom management following SBHU implementation, contrary to our initial hypothesis. Based on our educational initiatives and promotion of services across multiple departments, we anticipated an increase in such consultations as clinicians became more familiar with the scope of palliative care. Upon reviewing our data collection process, we noted that the “reason for consult” was determined by the first problem listed in the patient’s problem list within our internal database. This method of classification may have contributed to the apparent decline. Furthermore, the change could also reflect the impact of our educational interventions. By enhancing knowledge of basic palliative care principles, primary teams may have felt more confident managing symptoms independently, which led them to consult the GAP team for issues other than symptom management.
While the benefits of a traditional inpatient palliative unit (IPU) have been well documented in the literature, evidence on the effectiveness of scatter bed hospice models for improving palliative and hospice care utilization remains limited. A literature search conducted in PubMed using keywords such as “inpatient hospice,” “scatter bed hospice unit,” and “palliative care utilization” identified only two articles that specifically addressed palliative and hospice care utilization with this model. One was a retrospective study that evaluated costs and hospice length of stay (LOS) before and after implementation of an SBHU. The authors reported a 69% reduction in end-of-life costs and a hospice LOS that was four times longer than the LOS after a do-not-resuscitate order in the pre-implementation period. The second trial compared hospice LOS and costs for patients admitted to a traditional IPU versus a scatter bed model within the same institution. Both the IPU and SBHU were associated with improved hospice utilization; however, hospice LOS was significantly higher and average total costs per day were significantly lower among patients in the traditional IPU model. These authors hypothesized that hospitals may face challenges in maintaining hospice-focused care when patients are placed in scattered beds alongside those receiving curative treatment, which could result in unintended deviations from the hospice plan.
Prior to the SBHU, patients at our institution received care across the spectrum of their illness; however, there was not a standardized approach for end-of-life care. At the end of life, patients were often transferred to outside facilities under the care of new providers with whom they had no prior relationship. Implementing the SBHU improved the ability of the GAP team to deliver effective end-of-life services while allowing patients to remain in a familiar environment with trusted providers when they needed it most. This is reflected in the reduced proportion of patients who died without hospice enrollment following the intervention.
While SBHU models may not increase hospice utilization to the same extent as a traditional IPU, they offer greater flexibility for institutions. We recognize that space and staffing limitations may make a traditional IPU unfeasible for some hospitals. By integrating inpatient hospice patients among regional medical floor patients, pressures related to census management and the higher operating costs of specialized units are reduced. At our institution, we initially piloted the scatter bed model on a single regional medical floor to ensure consistent staffing by nurses who had received dedicated training in end-of-life care. Nurses without such credentialing were not assigned to these patients. Expanding this model would increase placement flexibility to meet varying demands for end-of-life care.
Our study has several limitations. Changes in the utilization of various palliative care services may have been impacted by other unmeasured factors, such as recent initiatives towards shifting to an age-friendly health system and greater provider comfortability with palliative care. We did not assess primary inpatient teams’ knowledge of GAP services or resources before and after SBHU implementation, limiting our ability to draw conclusions about potential culture or practice shifts. Future studies should evaluate referring physicians’ understanding of palliative care and explore the presence of any biases both prior to and following the establishment of an inpatient palliative unit. Additionally, recent expansion of the GAP team at our institution may have increased service visibility and capacity, making it difficult to determine whether higher utilization rates were driven by increased staffing, the SBHU, or a combination of both.
Other potential limitations include the short study period. The six-month pre and post comparison period may not capture longer-term trends or delayed effects of the intervention. Additionally, “reason for consult” was determined by the first-listed problem in the problem list, which did not always accurately reflect the primary clinical reason for referral. Future initiatives should require a consult order to include the primary reason for consultation or use standardized note templates that highlight the primary reason for consult. Analysis of patient centered outcomes such as symptom control, quality of life, caregiver satisfaction, and institutional cost savings was outside the scope of this project, but future efforts would include examining the impact of SBHU on these outcomes.
Prior literature has raised concerns that scatter beds may be used for “hospice-flipping” as a strategy for health systems to reduce inpatient mortality rates. Although this maneuver may appear to benefit the hospital, the hospice agency, and the patient, it poses several questions. Is this practice truly in the patient’s best interest? And would an inpatient GAP consultation service alone be able to meet patient and family needs while providing effective end-of-life care without involving hospice? The major critique of hospice flipping in the literature is that it represents a change in designation rather than a meaningful change in care setting or delivery. Our study illustrates a distinct model that addresses this concern: a structured protocol enabling appropriate patients to be transferred from various units to a dedicated SBHU staffed by hospice-trained nurses and personnel who fully embody the hospice philosophy. Prior to implementing the SBHU, our institution faced significant bottlenecks when transitioning actively dying patients to inpatient hospice levels of care. The SBHU provided a streamlined system to transfer patients to an appropriate care setting designed to deliver goal-concordant hospice services, whether from regional hospital units, the ICU, or the emergency department.
Importantly, our evaluation extends beyond mortality reduction. Rather than examining hospice flipping as an administrative maneuver, we assessed the effects of this system on the broader landscape of palliative services, including consult volume, hospice transitions, time from referral to placement, and goals of care. We believe that when inpatient hospice services are the most appropriate option to meet the needs of a patient and family, clinicians should help facilitate that transition, regardless of the specific care model used. The SBHU demonstrates how a dedicated, hospice-aligned environment can support timely, patient-centered transitions while mitigating concerns about inappropriate hospice flipping.
Conclusions
This quality initiative fills an important gap in the literature by examining the impact of a Scatter Bed Hospice Unit (SBHU) on use of other palliative care services, including Geriatric and Palliative (GAP) consults, goals-of-care conversations, and consultations for symptom management. This model also offers a potentially adaptable framework for other institutions seeking to implement similar care models.
During this 6-month pilot intervention, the SHBU improved utilization of palliative and hospice services with increased GAP consultation and trend towards increased overall hospice enrollment amongst all patients seen by the GAP team. Transition to hospice care was made more efficient with this model as evidenced by a significant increase in hospice discharges amongst comfort-care patients, and decreased time from inpatient hospice referral to SBHU admission.
Our findings underscore the potential of SBHU models to enhance continuity of end-of-life care, decrease non-hospice hospital deaths, and address institutional priorities such as census management. Given that this model was implemented in a state with one of the lowest hospice enrollment rates in the country, increasing the number of beds offering hospice services may be a meaningful step toward improving access and utilization.
Disclosures/Conflicts of Interest
The authors declare that we have no relevant or material financial interests that relate to the research described in this paper.
Acknowledgments
We would like to thank Rebecca Slossberg, Mark Tursi, and Wazim Narain for providing valuable feedback on the manuscript and for technical support with data analysis.
References
- Meier DE. Increased access to palliative care and hospice services: opportunities to improve value in health care. Milbank Q. 2011;89(3):343–380. doi: 10.1111/j.1468-0009.2011.00632.x.
- Maeda I, Miyashita M, Yamagishi A, et al. Changes in Relatives’ Perspectives on Quality of Death, Quality of Care, Pain Relief, and Caregiving Burden Before and After a Region-Based Palliative Care Intervention. J Pain Symptom Manage. 2016;52(5):637–645. doi: 10.1016/j.jpainsymman.2016.03.022.
- Ernecoff NC, Bilderback A, Bellon J, Arnold RM, Boninger M, Kavalieratos D. Associations between Reason for Inpatient Palliative Care Consultation, Timing, and Cost Savings. J Palliat Med. 2021;24(10):1525-1538. doi:10.1089/jpm.2020.0636
- El-Jawahri A, Greer JA, Pirl WF, et al. Effects of Early Integrated Palliative Care on Caregivers of Patients with Lung and Gastrointestinal Cancer: A Randomized Clinical Trial. Oncologist. 2017;22(12):1528–1534. doi: 10.1634/theoncologist.
- Temel JS, Greer JA, Muzikansky A, Gallagher ER, Admane S, Jackson VA, Dahlin CM, Blinderman CD, Jacobsen J, Pirl WF, Billings JA, Lynch TJ. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010 Aug 19;363(8):733-42. doi: 10.1056/NEJMoa1000678.
- Bojesson A, Brun E, Eberhard J, Segerlantz M. Quality of life for patients with advanced gastrointestinal cancer randomised to early specialised home-based palliative care: the ALLAN trial. Br J Cancer. 2024 Sep;131(4):729-736. doi: 10.1038/s41416-024-02764-x
- Abe H, Sumitani M, Matsui H, Inoue R, Fushimi K, Uchida K, Yasunaga H. Association between hospital palliative care team intervention volume and patient outcomes. Int J Clin Oncol. 2024 Oct;29(10):1602-1609. doi: 10.1007/s10147-024-02574-4.
- Kluger BM, Miyasaki J, Katz M, Galifianakis N, Hall K, Pantilat S, Khan R, Friedman C, Cernik W, Goto Y, Long J, Fairclough D, Sillau S, Kutner JS. Comparison of Integrated Outpatient Palliative Care With Standard Care in Patients With Parkinson Disease and Related Disorders: A Randomized Clinical Trial. JAMA Neurol. 2020 May 1;77(5):551-560. doi: 10.1001/jamaneurol.2019.4992.
- Bell CL, Kuriya M, Fischberg D. Hospice referrals and code status: outcomes of inpatient palliative care consultations among Asian Americans and Pacific Islanders with cancer. J Pain Symptom Manage. 2011 Oct;42(4):557-64.doi:10.1016/j.jpainsymman.2011.01.010
- Broom A, Kirby E, Good P, Wootton J, Adams J. Specialists’ experiences and perspectives on the timing of referral to palliative care: a qualitative study. J Palliat Med. 2012;15(11):1248-1253. doi:10.1089/jpm.2012.0264
- McDarby M, Carpenter BD. Barriers and Facilitators to Effective Inpatient Palliative Care Consultations: A Qualitative Analysis of Interviews With Palliative Care and Nonpalliative Care Providers. Am J Hosp Palliat Care. 2019;36(3):191-199. doi:10.1177/1049909118793635
- Tay J, Compton S, Phua G, et al. Perceptions of healthcare professionals towards palliative care in internal medicine wards: a cross-sectional survey. BMC Palliat Care. 2021;20(1):101. Published 2021 Jun 30. doi:10.1186/s12904-021-00787-2
- Bennardi M, Diviani N, Gamondi C, Stüssi G, Saletti P, Cinesi I, Rubinelli S. Palliative care utilization in oncology and hemato-oncology: a systematic review of cognitive barriers and facilitators from the perspective of healthcare professionals, adult patients, and their families. BMC Palliat Care. 2020 Apr 13;19(1):47. doi: 10.1186/s12904-020-00556-7.
- MacMartin MA, Sacks OA, Austin AM, Chakraborti G, Stedina EA, Skinner JS, Barnato AE. Association Between Opening a Palliative Care Unit and Hospital Care for Patients With Serious Illness. J Palliat Med. 2023 Sep;26(9):1240-1246. doi: 10.1089/jpm.2022.0447.
- Zhang H, Barysauskas C, Rickerson E, Catalano P, Jacobson J, Dalby C, Lindvall C, Selvaggi K. The Intensive Palliative Care Unit: Changing Outcomes for Hospitalized Cancer Patients in an Academic Medical Center. J Palliat Med. 2017 Mar;20(3):285-289. doi: 10.1089/jpm.2016.0225.
- Jegier BJ, O’Mahony S, Johnson J, Flaska R, Perry A, Runge M, Sommerfeld T. Impact of a Centralized Inpatient Hospice Unit in an Academic Medical Center. Am J Hosp Palliat Care. 2016 Sep;33(8):755-9. doi: 10.1177/1049909115599157.
- Digwood G, Lustbader D, Pekmezaris R, Lesser ML, Walia R, Frankenthaler M, et al. The impact of a palliative care unit on mortality rate and length of stay for medical intensive care unit patients. Palliative and Supportive Care. 2011 Dec;9(4):387–92. doi: 10.1017/S147895151100040X.
- Eti S, O’Mahony S, McHugh M, Guilbe R, Blank A, Selwyn P. Outcomes of the Acute Palliative Care Unit in an Academic Medical Center. American Journal of Hospice and Palliative Medicine. 2014 Jun 1;31(4):380–4. doi: 10.1177/1049909113489164.
- Kellar N, Martinez J, Finis N, Bolger A, von Gunten CF. Characterization of an acute inpatient hospice palliative care unit in a U.S. teaching hospital. J Nurs Adm. 1996 Mar;26(3):16–20. doi: 10.1097/00005110-199603000-00011.
- Shinall MC Jr, Martin SF, Nelson J, Miller RS, Semler MW, Zimmerman EE, Noblit CC, Ely EW, Karlekar M. Five-Year Experience of an Inpatient Palliative Care Unit at an Academic Referral Center. Am J Hosp Palliat Care. 2018 Aug;35(8):1057-1062. doi: 10.1177/1049909117751878.
- Albanese TH, Radwany SM, Mason H, Gayomali C, Dieter K. Assessing the financial impact of an inpatient acute palliative care unit in a tertiary care teaching hospital. J Palliat Med. 2013 Mar;16(3):289-94. doi: 10.1089/jpm.2012.0243.
- Knight HP. St. Luke’s Hospice: Prioritizing Comfort, Not Cure, in the Hospital Setting. Bull Hist Med. 2020;94(2):268-288. doi:10.1353/bhm.2020.0037
- Chung K, Richards N, Burke S. Hospice agencies’ hospital contract status and differing levels of hospice care. Am J Hosp Palliat Care. 2015;32(3):341-349. doi:10.1177/1049909114524815
- Rezaeiahari M, Brown CC, Schmit T, Tilford JM. Economic Report of General Inpatient Hospice in an Academic Medical Center. Am J Hosp Palliat Care. 2024 Jun;41(7):800-804. doi: 10.1177/10499091231204971.
- Wismann A, Kleszynski K, Jelinek D, et al. An age-friendly approach to primary care in an academic health system. J Am Geriatr Soc. 2024;72 Suppl 3:S23-S35. doi:10.1111/jgs.18848
- King SE, Ruopp MD, Mac CT, et al. Early clinical and quality impacts of the Age-Friendly Health System in a Veterans Affairs skilled nursing facility. J Am Geriatr Soc. 2024;72(12):3865-3874. doi:10.1111/jgs.19083
- Meier DE, Morgan L. Key findings on the perceptions of palliative care. Center to Advance Palliative Care; 2019. Accessed November 13, 2025. https://www.capc.org/events/recorded-webinars/briefing-key-findings-perceptions-palliative-care
- Marks S. The questionable practice of hospice flipping to improve inpatient mortality. J Pain Symptom Manage. 2015;49(3):e1-e2. doi:10.1016/j.jpainsymman.2014.10.009
- Schorr CA, Angelo M, John G, LeCompte K, Dellinger RP. The Association of Increasing Hospice Use With Decreasing Hospital Mortality: An Analysis of the National Inpatient Sample. J Healthc Manag. 2020;65(2):107-120. doi:10.1097/JHM-D-18-00280
- Baugh CW, Ouchi K, Bowman JK, et al. A Hospice Transitions Program for Patients in the Emergency Department. JAMA Netw Open. 2024;7(7):e2420695. Published 2024 Jul 1. doi:10.1001/jamanetworkopen.2024.20695