





Improving Situation Awareness in Clinical Practice
Situation Awareness—Bridging Neuroscientific and Human Factors/Ergonomics Perspectives and Implications for Clinical Practice
Stavros Prineas
- Department of Anaesthetics and Pain Management, Nepean Hospital, Sydney, Australia
OPEN ACCESS
PUBLISHED: 30 April 2025
CITATION: Prineas, S., 2025. Situation Awareness and Bridging Neuroscientific and Human Factors/Ergonomics Perspectives and Implications for Clinical Practice. Medical Research Archives, [online] 13(4).
https://doi.org/10.18103/mra.v1 3i5.6457
COPYRIGHT: © 2025 European Society of Medicine. This is an open- access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v1 3i5.6457
ISSN 2375-1924
ABSTRACT
A key challenge for clinicians is to make sufficient sense of what is happening around them to anticipate what might happen next and take timely action. This review article examines the theoretical basis of Situation Awareness (SA) – defined by Endsley as “the perception of the elements in the environment within a volume of time and space, the comprehension of their meaning and a projection of their status in the near future” (SA Levels I, II and III respectively) – and its relevance to clinical practice. SA is fundamental to good decision-making, and in turn to safe and effective human performance. Traditional models of clinical history taking / examination / investigation / diagnosis / prognosis align with the basic components of SA and can be further refined when viewed through the prism of SA, and its scope further extended by incorporating psychological, neurocognitive and statistical (Bayesian) perspectives.
Stress, fatigue and environmental noise/distractions can significantly impair SA, while other factors can significantly improve it. Experts experience a different perceptual world to novices, and techniques that may accelerate the acquisition of expert clinical SA (e.g. deliberate reflection, simulation, ergonomic environmental design etc.) could be beneficial to clinical practice. Moreover one can distinguish individual SA from ‘shared’ or ‘team’ SA, where specific communication, teamwork and leadership skills become relevant. Clinical emergencies and crises usually entail greater urgency, ambiguity, volatility and uncertainty, and impose a greater challenge on clinicians to form adequate SA in real time. Examples of SA in everyday clinical practice and the extent to which SA can be improved by adapting the clinician (through training) and/or adapting the work environment (through workplace/organisational design) are discussed.
Keywords: Situation Awareness, Neuroscience, Cognition, Human Factors, Ergonomics, Medical Education, Patient Safety
Introduction and Rationale
A key challenge for clinicians is to make sufficient sense of what is happening around them to anticipate what might happen next and take timely action, and for clinical teams similarly to function under a shared mental model. Situation awareness (SA) is an important human factors/ergonomics (HF/E) concept which arguably underpins all other non-technical skills such as perception of risk, communication, teamwork, leadership and managing automation.
This review article seeks to define SA and examine its counter-intuitively plastic and dynamic nature from several perspectives, in order to show the links between our current neuroscientific understanding of how the brain processes information and the practical aspects of the applied cognitive psychology underpinning the concept. The article will then explore more directly how SA relates to clinical practice, the factors that affect SA in healthcare environments, the differences between novice and expert SA, the extended concepts of team, shared and distributed SA, and finally the implications of SA for medical education and the design of healthcare systems more generally. Examples will be taken from anaesthetics and critical care (the author’s field of clinical expertise) however the concepts can in principle be readily extrapolated to other healthcare domains.
Definition of Situation Awareness
The roots of SA can be found in classical writings of military strategists such as Sun-Tzu (“know your enemy”)¹ and von Clausewitz (“knowledge of circumstances”)², emphasising recurrent themes of gathering intelligence and understanding/anticipating your opponent. Endsley defined SA formally as “the perception of the elements in the environment within a volume of time and space, the comprehension of their meaning, and a projection of their status in the near future”.³˒⁴ SA can be deconstructed into three levels: Perception, Comprehension and Projection.
Level I Situation Awareness – Perception
The first level of SA relates to perception of the status, attributes and dynamics of elements in an environment. It corresponds to the traditional framework of clinical assessment – reviewing a patient’s chart, taking a history, examining the patient, observing monitors, ordering investigations, consulting/conferring with colleagues etc. The ability to ask the right questions, to examine methodically and to navigate electronic medical record systems are all learned skills. Even when proficiency is gained, other factors can impair the ability to perceive key elements of a clinical situation (see below).
Level II Situation Awareness – Comprehension
Level II corresponds to the forming of a mental model that makes sense of clinical findings – a clinical impression, a working diagnosis plus differential etc. History and examination often suggest a range of likely conditions; there may be atypical presentations of less likely conditions. The ability to assign differential weight to a range of possible diagnoses and to adapt in the light of new information is learned over time through conscious reflection of aggregated experiences. Understanding how a range of contextual and environmental factors (clinical urgency, remote location, limited resources, operating in the middle of the night, interpersonal conflict etc.) can impact on human performance is part of Level II SA.
Level III Situation Awareness – Projection
The “brass ring” of SA is the ability to use one’s clinical understanding of a situation to predict what will happen in the future and to act on that prognosis in a timely manner – not only to manage complications, but ideally to prevent them from happening. Pilots are taught to make sure ‘the brain is always five minutes ahead of the plane’; anaesthetists are taught to ‘think five minutes ahead of the vapour’. Examples of effective Level III SA strategies in clinical practice include the “Between The Flags” system of vital signs monitoring to alert staff to trends of patient deterioration⁵ and the evolution of Cardiac Arrest Teams to Medical Emergency Teams (MET), designed nowadays to manage not only arrested patients, but also deteriorating patients pre-arrest, thereby reducing overall mortality.⁶
The Dynamics of Situation Awareness
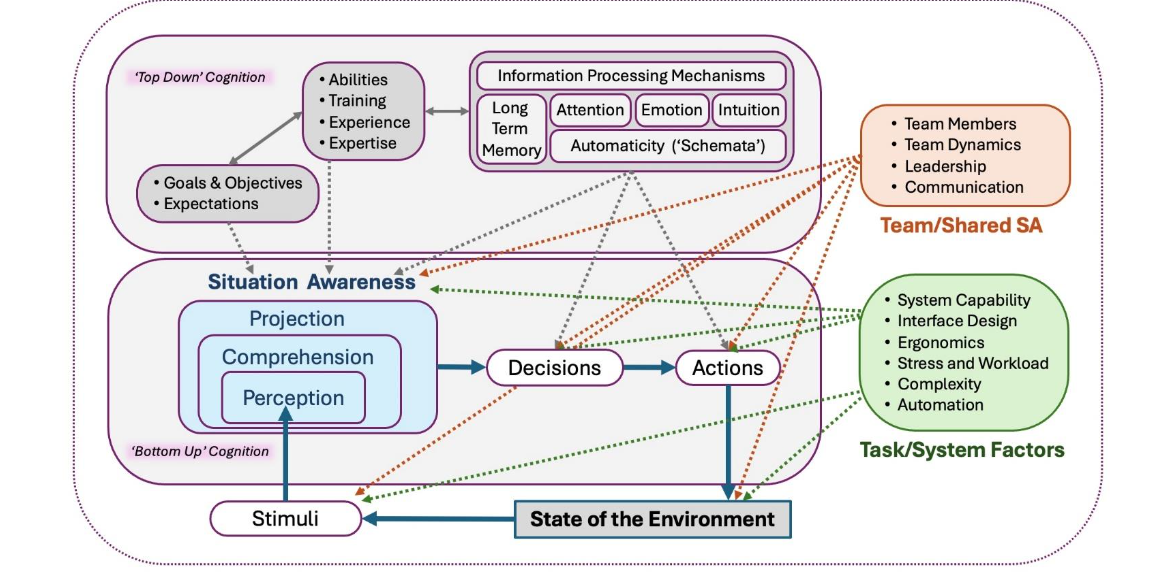
The serial logic underpinning this model (perception → comprehension → prediction) is intuitively appealing but serves only as the foundation of a network of more complex cognitive processes as observed in the real world (see Fig. 1). The next few paragraphs take a deeper dive into the neural basis of cognition seeking further insight into how SA is generated and maintained.
Figure 1. Situation Awareness
SYNAPTIC PLASTICITY
Information in biological brains is not held in binary digital packets the way it is stored in computers. Humans are born with a rudimentary ‘firmware’ of neuroanatomical connections but the ability to process, retain and recall information relies upon activation dependent synaptic plasticity (ADSP)⁷ occurring not just in infancy but throughout our lifetime. New experiences result in firing of neurons along a myriad of pathways; repeated stimulation along the same pathway within a critical timeframe results in an increase in the number of synaptic connections between activated neurons as well as a lowering of the neurotransmitter threshold for future stimulation. These make it more likely that subsequent stimulation will trigger the same pattern of firing. This biasing or synaptic weighting is fundamental to Hebbian learning, colloquially summarised as ‘neurons that fire together wire together’.⁸
Synaptic plasticity is how the brain codes information about the world. Studies of taxi drivers demonstrated that subjects trained in ‘The Knowledge’ of navigating London streets over a period of years acquired significantly larger posterior hippocampi than controls, postulated to be as a direct result of ADSP.⁹ This plasticity occurs not only in the hippocampus but wherever multipolar interneurons connect and interact throughout the brain; so most of the experiential ‘biasing’ of processed information about the world that the brain retains occurs beneath the level of consciousness. Synaptic weighting is happening all the time, even while we sleep.¹⁰ Thus
the organ we use to experience and understand the world is constantly, often imperceptibly changing. to paraphrase Heraclitus, “No person can enter the same river twice, for it is not the same river and they are not the same person”.¹¹
MENTAL MODELS AND SCHEMATA
The challenge for any brain is to discern meaning from the chaos of information about the self and the world around it in real time with only the limited processing power at its disposal. Through natural selection it appears that early neural networks acquired the ability to filter and ‘chunk’ aggregate neural activity into crude summary packets of that activity. These mental ‘models’ – precursors of ‘meaning’ – are refined by the hierarchical winnowing of information through intense competition between activated neural pathways in the midbrain, limbic system, hypothalamus, thalamus and ultimately the cerebral cortex.
The statistician George Box made the famous observation that “all models are wrong, but some are useful”.¹² All the models created by the brain are ‘wrong’ in so far as they are at best rough approximations; however many prove useful through the outcomes they produce. Useful models are retained, refined and become schemata,¹³ repertoires of thinking patterns and behaviour that run in the background or are activated by specific triggers. Collectively these subconscious ‘best guesses’ can be thought of as the brain’s ‘autopilot’, traditionally assigned to the basal ganglia but, like most higher order cognitive functions, now thought to be distributed across a much wider “default mode network” of brain structures.¹⁴
The increasing sophistication of information processing and modelling by central nervous systems can be tracked across species through key evolutionary steps from early metazoans to modern-day humans over hundreds of millions of years:¹⁵˒¹⁶ from the ability to focus attention by enhancing certain neural inputs while inhibiting others, to learning through physical trial and error (pavlovian conditioning), to the ability to imagine future states, abstracted learning through imagined trial and error (counterfactual or ‘what if’ learning), to modelling one’s own state of attention and that of others,¹⁷ and ultimately to the rich, ‘meaningful’ subjective experience that is human consciousness.
THE BAYESIAN BRAIN
In the traditional SA model, clinicians learn to evaluate complex clinical information from a range of sources (Level I SA) to arrive at probable diagnoses (Level II SA) and prognoses (Level III SA). This can be seen as a ‘bottom-up’ approach to cognitive processing – sensory inputs drive initial conscious perceptions, which are serially processed by higher cognitive centres. However, a wealth of research on various optical, sensory and cognitive illusions¹⁸˒¹⁹˒²⁰˒²¹ suggests that there is much more to how the brain forms conscious perceptions.
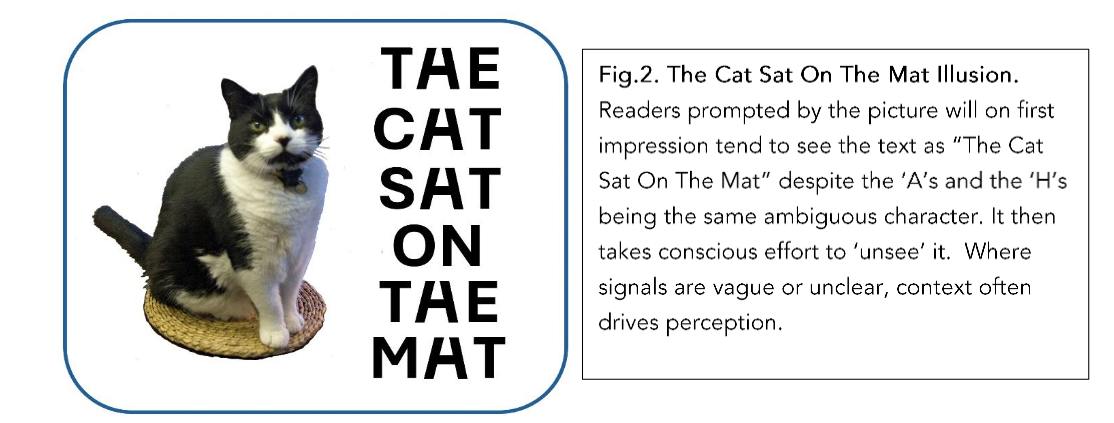
In the ‘Bayesian Brain Hypothesis’ (BBH)²²˒²³ the brain is treated as ‘statistical inference engine’²⁴ which is constantly and unconsciously trying to predict future states on the basis of past experience. Clinicians are most familiar with Bayesian theory when evaluating medical investigations and their predictive value based on specificity, sensitivity, false positives and negatives etc.²⁵ The effect of prior knowledge on probabilistic predictive power is often counterintuitive, shown most elegantly by the ‘Monte Hall Problem’²⁶ and other cognitive paradoxes. BBH is often described as a ‘top-down’ theory of cognition – our conscious perceptions of the world are to a large extent shaped by context and prior knowledge. The eyes are more than mere cameras; they ‘see’ what brain predicts they should see, calibrated as needed by salient sensory inputs (e.g. see Fig. 2).
Figure 2. The Cat Sat on the Mat
BBH has implications for more traditional models for SA predicated on ‘bottom-up’ cognitive processes. ‘Top-down’ elements better explain how with time and reflected experience, the serial hierarchy of perception-comprehension-projection becomes less distinct; prior diagnoses and prognoses shape future perceptions and perceived likelihoods, and the three levels of SA tend to coalesce into a single gestalt which form the basis of expert SA (see below).
SYNTHESIS
In summary, several relevant threads emerge. First, our picture of the world is built and maintained through patterns of synaptic weights reinforced by prior experiences which bias information processing from the perceptual level upwards. Second, parts of the brain are constantly competing with each other – some win, some lose (often for reasons not consciously apparent to us) but they all nevertheless effect plastic changes across the brain whenever they are active, even when we sleep. Third, what we understand as ‘consciousness’ represents only a fraction of the massive amount of biased information about the world that the brain has already stored and continues to process throughout our lifetime. Next, the models formed by the brain are fundamentally crude ‘executive summaries’ of complex neuronal activity whose sophistication and utility in humans are the culmination of millions of years of evolution. Finally, our sense of reality in any given moment lies somewhere between perception, memory and prediction: consciousness is not just driven from the ‘bottom up’ by our senses but also from the ‘top-down’ by our subconscious ‘schemata’ and ‘autopilot’. The world we ‘see’ is framed by an often arcane mix of what we have seen before and what we hope to see, as the Bayesian brain’s ‘best guess’ of reality. All of these elements have implications for how SA is elaborated and susceptible to a range of biological and non-biological factors.
Inattentional Blindness and Manipulating Perceptions
Under certain circumstances our senses do not render faithfully what is in front of us. Entertaining examples of ‘inattentional blindness’ are Simons and Chabris’ notorious Basketball Video²⁷˒²⁸ and Wiseman’s ‘Amazing Colour Changing Card Trick’.²⁹ These videos illustrate how perception itself can be altered and indeed misdirected by distractions or other cognitive activities such as focusing intently on a task. Medical hypnosis, a technique which allows a patient’s past memories of joyful or pleasant sensations to be experienced vividly as if they were in the present, has been shown to relieve anxiety and pain in a range of invasive procedures under local anaesthetic.³⁰˒³¹˒³² This is not only evidence of the manipulability of SA, but also an indicator of the practical benefits of understanding the plastic nature of SA in clinical environments.
Novice vs Expert Situation Awareness
Abundant research into Naturalistic Recognition Primed Decision Making (NDM or RPDM) has demonstrated that highly attuned SA is fundamental
References
1. Tzu S. The Art of War. Giles L Translation of 5th Century BCE manuscript. Available at
https://dn790006.ca.archive.org/0/items/TheArtOfWarBySunTzu/ArtOfWar.pdf 2004; 4:18
2. Von Clausewitz C. Vom Kriege (On War). Graham JJ Translation of 1874 Edition. Project Gutenberg. Available at
https://www.gutenberg.org/files/1946/1946-h/1946-h.htm retrieved 20 March 2025
3. Endsley MR. Design and evaluation for situation awareness enhancement. In Proceedings of the Human Factors Society 32nd Meeting. Santa Monica, CA: Human Factors Society. 1988; 97-101.
4. Endsley MR. Situation Awareness. In Handbook of Human Factors and Ergonomics (5th Ed.) Salvendy G, Karwowski W. Eds. 2021; Available at https://onlinelibrary.wiley.com/doi/10.1002/9781119636113.ch17.
5. Hughes C, Pain C, Braithwaite J, Hillman K. ‘Between the flags’: implementing a rapid response system at scale. BMJ Qual Saf 2013; 23(9): 714-7. doi: 10.1136/bmjqs-2014-002845
6. Tobin AE, Santamaria JD. Medical emergency teams are associated with reduced mortality across a major metropolitan health network after two years service: a retrospective study using government administrative data. Crit Care 2012; 16: R210. doi:10.1186/cc11843
7. Ganguly K, Poo M. Activity Dependent Neural Plasticity from Bench to Bedside. Neuron 2013;80: 729-41
8. Agilari E, Aquaro M, Barra A, Fachechi A, Marullo C. From Pavlov Conditioning to Hebbian Learning. Neural Comput 2023; 35(5): 930-57. doi: 10.1162/neco_a_01578
9. Maguire EA, Spiers HJ, Good CD, Hartley T, Frackwiak RS, Burgess N. Navigation expertise and the human hippocampus: a structural brain imaging study. Hippocampus 2003; 13(2): 250-9. doi: 10.1002/hipo.10087
10. Wang G, Grone B, Colas D, Applebaum L, Mourrain P. Synaptic plasticity in sleep: learning homeostasis and disease. Trends Neurosci 2011; 34(9): 452-463. Doi:10/1016/j.tins.2011.07.005
11. Heraclitus. Fragment DK B91. Hoyt R Ed. The Fragments of Heraclitus. Available at
https://heraclitusfragments.com/B91/index.html retrieved 20 Mar 2025
12. Box G. Science and Statistics. J Am Stat Ass 1976; 71(356): 791-799
13. Ghosh VE, Gilboa, A. What is a memory schema? A historical perspective on current neuroscience literature. Neuropsychologia 2014 53: 104-14. doi: 10.1016/j.neuropsychologia.2013.11.010
14. Vatansever D, Menon DK, Emmanuel A. Stamatakis EA. Default mode contributions to automated information processing. Proc Nat Acad Sci 2017; 114 (48): 12821-12826. doi: 10.1073/pna s.1710521114
15. Cisek P. Resynthesizing behavior through phylogenetic refinement. Attent Percept Psychophys. 2019; 81: 2265–2287. doi: 10.3758/s13414-019-01760-1
16. Bennett MS. What Behavioral Abilities Emerged at Key Milestones in Human Brain Evolution? 13 Hypotheses on the 600-Million-Year Phylogenetic History of Human Intelligence. Front Psychol 2021; 12:685853. doi: 10.3389/fpsyg.2021.6 85853
17. Graciano MSA. Rethinking Consciousness – A Scientific Theory of Subjective Experience. WW Norton Pubs. 2019
18. Loeb GE, Fishel JA. Bayesian Action & Perception: Representing the World in the Brain. Front Neurosci. 2014; 8. doi:10.3389/fnins.2014.00 341
19. Nour MM, Nour JM. Perception, Illusions and Bayesian Inference. Psychopathology 2015; 48(4); 217-221. doi: 10.1159/000437271
20. Born RT, Bencomo G. Illusions, Delusions and your Backwards, Bayesian Brain: A Biased Visual Perspective. Brain Behav Evol 2020; 95(5) 272-285. doi:10.1159/000514859
21. Bruckmaier G, Krauss S, Binder K, Hilbet S, Brunner B. Tversky and Kahneman’s Cognitive Illusions: Who Can Solve Them, and Why? Front Psychol 2021; 12. doi: 10.3389/fpsyg.2021.584689
22. Friston K. The history of the future of the Bayesian brain. NeuroImage 2012; 62: 1230-1233 doi:10.1016/j.neuroimage.2011.10.004
23. Hipólito I, Kirchhoff M. Breaking Boundaries: the Bayesian Brain Hypothesis for perception and prediction. Consciousness and Cognition 2023; Available at https://doi.org/10.1016/j.concog.2023.103510
24. von Helmholtz, H. Concerning the perceptions in general, 3rd Ed. Treatise on Physiological Optics, Vol. III (Translated by J. P. C. Southall 1925 of the 1866 manuscript; reprinted New York: Dover, 1962.) Opt Soc Am 1925;26:4.. Available at
https://archive.org/details/helmholtzstreati0003jame/page/338/mode/2up retrieved 27 Mar 2025
25. Sox HC Jr. Probability theory in the use of diagnostic tests. An introduction to critical study of the literature. Ann Intern Med 1986 Jan;104(1):60-6. doi: 10.7326/0003-4819-104-1-60.
26. Krauss S Wang XT. The psychology of the Monty Hall problem: discovering psychological mechanisms for solving a tenacious brain teaser J Exp Psychol Gen 2003 Mar;132(1):3-22. doi: 10.103 7/0096-3445.132.1.3.
27. Simons DJ, Chabris CF. Gorillas in our midst: sustained inattentional blindness for dynamic events. Perception 1999; 28: 1059-1074. doi:10.1068/p28 1059
28. Simons D. Selective Attention Test (video). Available at
https://www.youtube.com/watch?v=vJG698U2Mvo retrieved 16 Mar 2025
29. Quirkology. Colour Changing Card Trick (video). Available at
https://www.youtube.com/watch?v=v3iPrBrGSJM retrieved 16 Mar 2025
30. Potié A, Roelants F, Pospiech A, Momeni M, Watremez C. Hypnosis in the Perioperative Management of Breast Cancer Surgery: Clinical Benefits and Potential Implications. Anesthesiol Res Pract 2016:2942416. doi: 10.1155/2016/2942416.
31. Fusco N, Bernard F, Roelants F, Watremez C, Musellec H, Laviolle B, Beloeil H. Hypnosis and communication reduce pain and anxiety in peripheral intravenous cannulation: Effect of Language and Confusion on Pain During Peripheral Intravenous Catheterization (KTHYPE), a multicentre randomised trial. BJA 2020;124(3):292-298. doi: 10.1016/j.bja.2 019.11.020
32. Slater P, Van-Manen A, Cyna AM. Clinical hypnosis and the anaesthetist: a practical approach. BJA Education 2024; 24(4): 121e128. doi: 10.1016/j.b jae.2024.01.005
33. Klein G. Naturalistic decision making. Hum Factors 2008; 50(3): 456–60. doi:10.1518/0018720 08X288385
34. Klein GA. A recognition-primed decision (RPD) model of rapid decision making. In: Klein GA, Orasanu J, Calderwood R, Zsambok CE, editors. Decision making in action: models and methods. Norwood, NJ: Ablex Publishing; 1993; 138–47.
35. Klein G. Sources of Power: How people make decisions. Cambridge (Mass.): MIT Press. 1998
36. Engel PJH Tacit knowledge and visual expertise in medical diagnostic reasoning: Implications for medical education. Medical Teacher 2008; 30: e184-e188 doi:10.1080/0142159080214 4260
37. Waag WL, Bell HH. Situation assessment and decision making in skilled fighter pilots. In Zsambok, CE, Klein, G. Naturalistic decision making. Mahwah, NJ: Lawrence Erlbaum Associates, Publishers. 1997: 247–54.
38. Dominguez CO. Expertise and metacognition in laparoscopic surgery: a field study. In: Proceedings of the Human Factors and Ergonomic Society 45th Annual Meeting, Minneapolis/St. Paul; 2001:1298–303.
39. Gladwell M. Outliers: The Story of Success. New York, NY: Little Brown and Company Pubs. 2008
40. Ericsson KA, Charness N, Feltovich P, et al., editors. The Cambridge Handbook of Expertise and Expert Performance. New York (NY): Cambridge University Press; 2006Nakayama
41. Gao Q, Hartwig MG. Commentary: Are 10000 hours really the key to adult learning? Perhaps not. JTCVS Open 2021;8: 688-9. doi: 10.1016/j.xjon.20 21.09.009
42. Wong NC. The 10000-hour rule. Can Urol Assoc J 2015; 9(9-10):299. doi:10.5489/cuaj.3267
43. Ericsson KA. Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad Med 2004; 79(10 Suppl): S70-81.
44. Ericsson KA. Deliberate practice and acquisition of expert performance: a general overview. Acad Emerg Med 2008;15(11):988-94.
45. Eriksson KA, Harwell KW. Deliberate Practice and Proposed Limits on the Effects of Practice on the Acquisition of Expert Performance: Why the Original Definition Matters and Recommendations for Future Research. Front Psychol 2019; 10: 2386. doi: 10.3389/fpsyg.2019.02396
46. Flack J. Situation Awareness: Proceed With Caution. Human Factors 1995; 37(1) : 149-57. doi: 10.1518/001872095779049480
47. Endsley MR. A taxonomy of Situation Awareness Errors. In: Fuller R, Johnston N, McDonald N, Eds. Human Factors in Aviation Operations. Aldershot: Ashgate Publishing. 1995; 287–92.
48. Schulz CM, Krautheim V, Hackemann A, Kreuzer M, Kochs EF, Wagner KJ. Situation awareness errors in anesthesia and critical care in 200 cases of a critical incident reporting system. BMC Anesthesiol 2016;16:4 doi: 10.1186/s12871-016-0172-7
49. Prineas S, Mosier, K, Mirko C, Giuccardi S. Non-Technical Skills in Healthcare. Donaldson L, Riccardi W, Sheridan S, Tartaglia R Eds. In: Textbook of Patient Safety and Clinical Risk Management. Cham (CH): Springer; 2021. Chapter 30. 2020.
50. Killgore WDS. Effects of sleep deprivation on cognition. Prog Brain Res 2010; 185:105-29
51. Rogers AE. The Effects of Fatigue and Sleepiness on Nurse Performance and Patient Safety. Chapter in Patient Safety and Quality: An Evidence Based Handbook for Nurses. Rockville (MD): Agency for Healthcare Research and Quality (US); 2008. Available at https://www.ncbi.nlm.nih.gov/books/NBK2651/ retrieved 16 Mar 2025
52. Tawfik DS, Profit J, Morgenthaler TI, Tutty MA, West CP, Shanfelt TD. Physician Burnout, Wellbeing, and Work Unit Safety Grades in Relationship to Reported Medical Errors. Mayo Clin Proc 2018; 93(11): 1571–80.
53. Rivera AJ, Tarsh B-T. Interruptions and Distractions in Healthcare: Review and Reappraisal. Qual Saf Health Care . 2010 August ; 19(4): 304–312. doi:10.1136/qshc.2009.033282.
54. Young JQ, Ranji SR, Wachter RM, Lee CM, Niehaus B. “July Effect”: Impact of the Academic Year-End Changeover on Patient Outcomes – A Systematic Review. Ann Int Med 2011; 155(5):309-15. doi: 10.7326/0003-4819-155-5-201109060-00354
55. Jane Ferguson J, Stringer G, Walshe K, Allen T, Grigoroglou Ashcroft DM, Kontopantelis E. Locum doctor working and quality and safety: a qualitative study in English primary and secondary care. BMJ Qual Saf 2024; 33: 354–362. doi:10.113 6/bmjqs-2023-016699
56. Baverstock A, Finlay F. Take a break: HALT—are you Hungry, Angry, Late or Tired? ADC Ed Prac 2019;104:200. doi: 10.1136/archdischild-2019-317209
57. Gaba DM, Fish KJ Howard SK. Crisis management in Anesthesiology. New York: Churchill Livingstone. 1994; 24-33
58. Yentis S. Of humans, factors, failings and fixations. Anaesthesia 2009;65(1):1-3. doi: 10.1111/j.1 365-2044.2009.06018.x
59. Harmer M. The Case of Elaine Bromiley: Independent Review of the care given to Mrs Elaine Bromiley on 29 March 2005. Available at
https://emcrit.org/wp-content/uploads/ElaineBromileyAnonymousReport.pdf retrieved 22 March 2025.
60. Matthews WJ, Meck WH. Time perception: the bad news and the good. WIREs Cogn Sci 2014,
5:429–446. doi: 10.1002/wcs.1298
61. Schonger M, Sele D. Intuition and exponential growth: bias and the roles of parameterization and complexity. Math Semesterber (2021) 68:221–235. doi:10.1007/s00591-021-00306-7
62. Kuhlenschmidt KM, Choi E, Moonmoon K, Blackwell J, Comish PB, Balentine C, Grant J, Park C, Dultz LA, Shoultz, Cripps MW, Dumas Ryan P. Provider Perception of Time During Trauma Resuscitation: A Prospective Quantitative Trauma Video Review Analysis. J Surg Res 2022 Jun:274: 207-212. doi: 10.1016/j.jss.2021.12.048. Epub 2022 Feb 18
63. Kaber DB, Endsley MR. Out-of-the-loop performance problems and the use of intermediate levels of automation for improved control system functioning and safety. Proc Safety Progress 1997; 16(3): 126-31. doi:10.1002/prs.608160304
64. Gouraud J, Delrome A, Berberian B. Autopilot, Mind Wandering, and the Out of the Loop Performance Problem. Front Neurosci 2017; 11. doi: 10.3389/fnins.2017.00541
65. Ruskin KJ, Ruskin AC, O’Connor M. Automation failures and patient safety. Curr Opin Anaesthesiol 2020; 33(6): 788-92. DOI: 10.1097/AC O.0000000000000935
66. Endsley MR, Jones WM. A model of inter and intra-team situation awareness: implications for design, training and measurement. In: McNeese M, Salas E, Endsley MR Eds. New trends in cooperative activities: understanding system dynamics in complex environments. Santa Monica: Human Factors and Ergonomics Society. 2001;1–24.
67. Wright MC, Ensley MR. Building Shared Situation Awareness in Healthcare Settings. In Nemeth CP Ed. Improving Healthcare Team Communication. London: Routledge. 2017. doi: 10.1201/9781315588056
68. Skog A, Peyre SE, Pozner CN, Thorndike M, Hicks G, Dellaripa PF. Assessing Physician Leadership Styles: Application of the Situational Leadership Model to Transitions in Patient Acuity. Teach Learn Med 2012; 24(3): 225-30. doi: 10.1080/10401334.2 012.692269
69. Cooper S, Wakelam A. Leadership of resuscitation teams: “Lighthouse Leadership”. Resuscitation 1999; 42:27–45. doi: 10.1016/s0300-9572(99)00080-5
70. Weller JM, Mahajan R, Fahey-Williams K, Webster CS. Teamwork matters: team situation awareness to build high-performing healthcare teams, a narrative review. BJA 2024; 132(4): 771-778. doi: 10/1016/j.bja.2023.12.035
71. Fioratou E, Flin R, Glavin R, Patey R. Beyond monitoring: distributed situation awareness in anaesthesia. BJA 2010; 105(1): 83-90. doi: 10.1093/b ja/aeq137
72. Carayon P, Wooldridge A, Hoonakker P, Schoofs-Hundt A, Kelly MM. SEIPS 3.0: Human-Centered Design of the Patient Journey for Patient Safety. App Ergon 2020; 84: 103033. doi:10.1016/j.a pergo.2019.103033
73. Youssef SC, Haram K, Noel J, Patel V, Porter J, Dagupta P. Evolution of the digital operating room: the place of video technology in surgery. Langenbeck’s Arch Surg 2023; 408: 95. doi:10.100 7/s00423-023-02830-7
74. Stichler JF, Feiler JL. Ergonomics in Healthcare Facility Design, Part 1: Patient Care Areas. JONA 2011; 41(2): 49-51. doi:10.1097/NNA.0b013e3182 0592e6
75. Feiler JL, Stichler JF. Ergonomics in Healthcare Facility Design, Part 2: Support Areas. JONA 2011; 41(3): 97-99. doi: 10.1097/NNA.0b013e31820c72a1
76. Martin JL, Norris BJ, Murphy E, Crowe JA. Medical device development: the challenge for ergonomics. Appl Ergon 2008; 39(3): 271-83. doi: 10.1016/j.apergo.2007.10.002
77. Ward M, Sujan M, Pool R, Preston K, Huang H, Carrington A, Chozos N. Integrating Human-Centred AI into Clinical Practice. Available at https://ergonomics.org.uk/resource/integrating-human-centred-ai-in-clinical-practice.html retrieved 16 Mar 2025
78. Leong KBMSL,Hanskamp-Sebregts M, van der Wal RA, Wolff AP. Effects of perioperative briefing and debriefing on patient safety: a prospective intervention study. BMJ Open 2017; 7: e018367. doi:10.1136/bmjopen-2017-018367
79. Burgess A, van Diggele C, Roberts C, Mellis C. Teaching clinical handover with ISBAR. BMC Medical Education 2020; 20(Suppl 2):459. doi: 10.1186/s12909-020-02285-0
80. Skegg E, McElroy C, Mudgway M, Hamill J. Debriefing to improve interprofessional teamwork in the operating room: A systematic review. J Nurs Scholarship 2023; 55: 1179-88. doi: 10.1111/jnu.1 2924
81. Mitchell SA, Boyer TJ. Deliberate Practice in Medical Simulation. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from
https://www.ncbi.nlm.nih.gov/books/NBK554558/ retrieved 26 Mar 2025
82. Endsley MR. A Systematic Review and Meta-Analysis of Direct Objective Measures of Situation Awareness: A Comparison of SAGAT and SPAM. Human Factors 2021; 63(1): 124-50. doi: 10.1177/0 018720819875376
83. Coolen E, Draaisma J, Loeffen J. Measuring situation awareness and team effectiveness in pediatric acute care by using the situation global assessment technique. Eur J Paed 2019; 178: 837-850. doi: 10.1007/s00431-019-03358-z
84. Jonsson K, Brulin C, Härgestam M, Lindkvist M, Hultin M. Do team and task performance improve after training situation awareness? A randomized controlled study of interprofessional intensive care teams. Scand J Trauma Res Em Med 2021; 29:73. doi: 10.1186/s13049-021-00878-2
85. Hunter J, Porter M, Williams B. A novel study of situational awareness among out-of-hospital providers during an online clinical simulation. Australas Emerg Care 2023; 26: 96-103
86. Hogan MP, Pace DE, Hapgood J, Boone DC. Use of Human Patient Simulation and the Situation Awareness Global Assessment Technique in Practical Trauma Skills Assessment. J Trauma Acute Care Surg 2006; 61(5): 1047-1052. doi: 10.1097/01.t a.0000238687.23622.89
87. Zimmermann C, Fridrich A, Schwappach DL. Training Situational Awareness for Patient Safety in a Room of Horrors: An Evaluation of a Low-Fidelity Simulation Method. J Pat Safety 2021; 17 (8): e1026-e1033. doi: 10.1097/PTS.000000000 0000806
88. Jaffe, R, Zavodnick, J, Papanagnou, D, Zhang, XC, Diemer, G. Patient Safety Escape Room: A Team Simulation in Recognizing and Reporting Patient Safety Hazards. Am J Med Qual 2022; 37 (2):166-172 doi:10.1097/01.JMQ.0000753252.299 33.8d