





Inducible Transgenic Models for Cancer Research
Oncopigs: an inducible transgenic large animal cancer model to address pre-clinical assessments
Kyle M. Schachtsneider1, Vera Mehta1, Jessica Rege1, and Lawrence B. Schook1
- Sus Clinicals, Inc.
OPEN ACCESS
PUBLISHED: 31 March 2025
CITATION: SCHACHTSCHNEIDER, Kyle M. et al. Oncopigs: an inducible transgenic large animal cancer model to address pre-clinical assessments. Medical Research Archives, [S.l.], v. 13, n. 3, mar. 2025. . Available at: <https://esmed.org/MRA/mra/article/view/6392>. Date accessed: 24 oct. 2025.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i3.6392
ISSN 2375-1924
Abstract
Cancer research progress has been negatively hampered by the lack of reliable experimental systems in which to study the effects of nutritional interventions on cancer phenotypes. To address this, we developed an inducible transgenic large animal model, the Oncopig, which is a unique genotypically, anatomically, and immunologically relevant model that develops spontaneous tumors in response to specific genetic alterations. This allows the pigs to be bred and raised like normal animals, and why tumors can be induced at specific locations within the Oncopig to induce tumors. To date, our studies have shown that the Oncopig can be used to evaluate the efficacy of novel therapeutic agents, and the development of preclinical models for targeted therapeutic testing has the potential to significantly improve clinical HCC outcomes.
Keywords: Oncopig, cancer model, preclinical assessments, transgenic model, therapeutic testing
INTRODUCTION
BUILDING BLOCKS FOR PORCINE CANCER MODELS
The global incidence of cancer is rapidly rising, and despite an improved understanding of cancer molecular biology, immune landscapes, and advancements in cytotoxic, biologic, and immunologic anti-cancer therapeutics, cancer remains a leading cause of death worldwide. Cancer is caused by the accumulation of a series of gene mutations called driver mutations that confer selective growth advantages to tumor cells. As cancer therapies move toward personalized medicine, predictive modeling of the role driver mutations play in tumorigenesis and therapeutic susceptibility will become essential. The development of next-generation sequencing technology has made the evaluation of mutated genes possible in clinical practice, allowing for identification of driver mutations underlying cancer development in individual patients. This, combined with recent advances in gene editing technologies such as CRISPR-Cas9 enables development of personalized tumor models for prediction of treatment responses for mutational profiles observed clinically.
Pigs represent an ideal animal model for development of personalized tumor models due to their similar size, anatomy, physiology, metabolism, immunity, and genetics compared to humans. Such models would support new initiatives in precision medicine, provide approaches to create disease site tumor models with designated spatial and temporal clinical outcomes, and create standardized tumor models analogous to human tumors to enable therapeutic studies.
In this review, we discuss the process of utilizing genomic sequencing approaches, gene editing technologies, and transgenic porcine cancer models to develop clinically relevant, personalized large animal cancer models for use in co-clinical trials, improving translation into the clinic to ultimately de-risk clinical failure and potentially accelerate clinical trials.
While human clinical trials are the benchmark for testing cancer diagnostics and therapies; regulatory, enrollment, and financial challenges of trial inception are significant. Advances in cancer care are therefore dependent upon the use of preclinical in vivo model systems to test new treatments. However, currently the majority of preclinical efficacy studies are done in mice, yet 90% or more of the drugs fail in the clinic, indicating therapeutic success in rodent models does not translate to improved patient outcomes in clinical trials and underscores the deficiencies of these models to recapitulate the complexity of human tumor biology and clinical responses.
Murine models provide a critical first step in assessing a therapeutic path towards clinical utility; particularly with respect to drug toxicity. However, rodent models are not amenable to clinically relevant imaging and surgical or local regional therapeutic studies. Mice differ vastly from humans with respect to size (300x smaller), organ and tissue structures, and systemic immune physiology (only 10% overlap). In contrast to mice, pigs share many similarities with humans in terms of anatomy, physiology, immunology, and genetics, including requiring multiple genetic changes to develop cancer. In addition, both their basal metabolic rate and their xenosensor pregnane X receptor that regulates CYP3A expression—responsible for the metabolism of half of all prescription drugs—are very similar to humans. Pigs therefore represent a relevant preclinical model to study clinical imaging, surgical techniques, and therapeutic approaches.
TECHNOLOGY PLATFORM: MODELING ONCOLOGY ON DEMAND
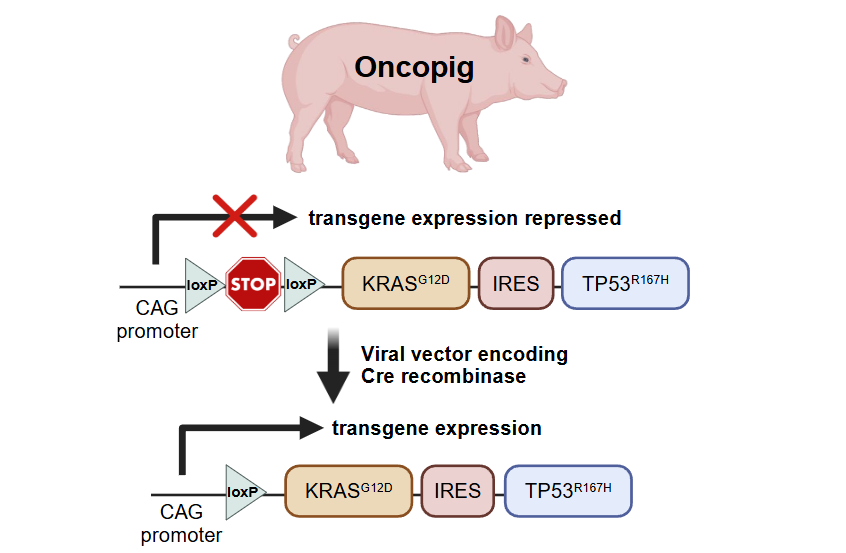
The Oncopig® is a novel, malleable, genetically defined, and highly relevant inducible cancer model that allows preclinical investigation, clinical outcome comparisons, and assessment of standard, novel, and experimental drugs, devices, and techniques unachievable with current preclinical models. Beyond these pig/human similarities described above, the Oncopig® allows for the induction of highly relevant tumors and comorbidities (i.e. cirrhosis, obesity, cardiovascular disease) which can be key to successful qualification of therapeutic safety and efficacy. Each of the Oncopig® has a transgene construct inserted into the genome that allows for expression of KRAS<sup>G12D</sup> and TP53<sup>R167H</sup> driver mutations commonly observed in human tumors (Figure 1). There is a stop sequence located upstream of the genes that prevents the genes from being expressed. This allows the pigs to be bred and raised like normal animals, and why tumors can be specifically induced in precise organs and sites on demand. The stop sequence is flanked by loxP sites so exposure to an adenoviral vector encoding for Cre recombinase (AdCre) triggers a recombination event removing the STOP sequence and allowing the driver mutations to be expressed, thus triggering oncogenesis.
BUILDING BLOCKS FOR PORCINE CANCER MODELS
All non-specific histology models are developed using one of two approaches: 1) image-guided biopsy collection of target organs; inclusion of biopsy with AdCre suspended in PBS, injection of AdCre directly mixed with gefitinib into target organ, or 2) direct injection of AdCre into the target organ. Across all organs, tumors with growth rates from 1-2 weeks and reach a size range of 0.5-3 cm in timeframe. Spontaneous tumor regression as a result of immune cell killing is observed across all models, with tumor regression rates varying from 1 week to 3 months depending on the targeted organ.
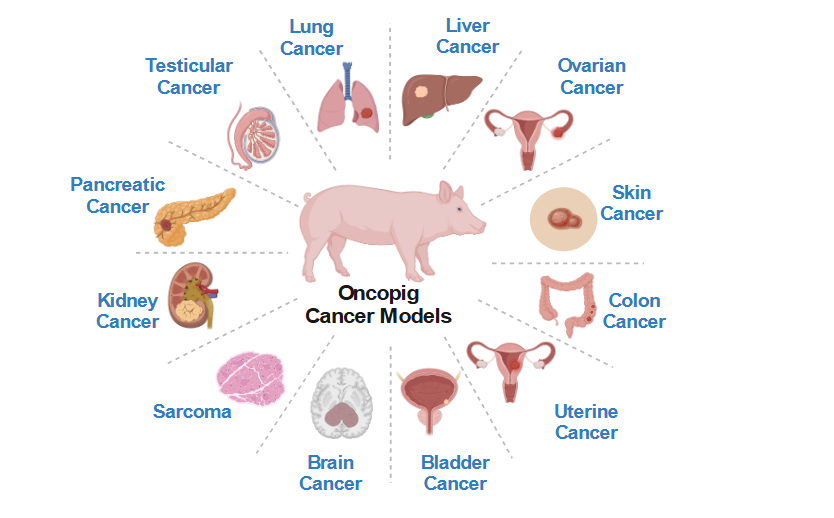 Figure 2. Oncopig Cancer Models. Figure was created using BioRender.All non-specific histology models are developed using one of two approaches: 1) image-guided biopsy collection of target organ, incubation of biopsy with AdCre suspended in PBS, injection of AdCre-biopsy mixed with gelfoam into target organ, or 2) direct injection of AdCre into the target organ. Across all organ systems, tumors form within 1-2 weeks and reach a size range of 0.5-3cm in that timeframe. Spontaneous tumor regression as a result of T-cell mediated tumor cell killing is observed across all models, with tumor regression rates varying from a few weeks to months. This spontaneous regression can be eliminated through immunosuppression to facilitate use for long-term follow-up studies.Focus has been on: 1) development of tumor induction methods through alteration of molecular pathways commonly disrupted in human cancers (precision medicine); 2) development of approaches to induce tumors at defined disease sites (spatial and temporal); and 3) creation of standardized tumor models analogous to human tumors to support preclinical therapeutic studies (translational relevance). Combined, these Sus Clinicals technology platforms permit development of: 1) clinically relevant cell lines and tumors with defined driver mutational profiles (the what); 2) tumors with precise knowledge of induction times (the when); and 3) tumors in defined locations and comorbid microenvironments (the where). These technology platforms therefore facilitate generation of consistent tumors and microenvironments for on-demand preclinical testing in a predictive large animal model, helping established medical device, diagnostic, and pharma companies optimize their innovation portfolios and move their most promising technologies to successful market launch²⁴⁻²⁷.
Figure 2. Oncopig Cancer Models. Figure was created using BioRender.All non-specific histology models are developed using one of two approaches: 1) image-guided biopsy collection of target organ, incubation of biopsy with AdCre suspended in PBS, injection of AdCre-biopsy mixed with gelfoam into target organ, or 2) direct injection of AdCre into the target organ. Across all organ systems, tumors form within 1-2 weeks and reach a size range of 0.5-3cm in that timeframe. Spontaneous tumor regression as a result of T-cell mediated tumor cell killing is observed across all models, with tumor regression rates varying from a few weeks to months. This spontaneous regression can be eliminated through immunosuppression to facilitate use for long-term follow-up studies.Focus has been on: 1) development of tumor induction methods through alteration of molecular pathways commonly disrupted in human cancers (precision medicine); 2) development of approaches to induce tumors at defined disease sites (spatial and temporal); and 3) creation of standardized tumor models analogous to human tumors to support preclinical therapeutic studies (translational relevance). Combined, these Sus Clinicals technology platforms permit development of: 1) clinically relevant cell lines and tumors with defined driver mutational profiles (the what); 2) tumors with precise knowledge of induction times (the when); and 3) tumors in defined locations and comorbid microenvironments (the where). These technology platforms therefore facilitate generation of consistent tumors and microenvironments for on-demand preclinical testing in a predictive large animal model, helping established medical device, diagnostic, and pharma companies optimize their innovation portfolios and move their most promising technologies to successful market launch²⁴⁻²⁷.
PROVIDING SOLUTIONS TO UNMET CLINICAL NEEDS
Since the Oncopig® is a highly specific and reproducible model for tumor induction, it provides a tool for multiple applications in addressing unmet clinical needs for devices, drugs and diagnostic applications. Hence, potentially drastically reducing development time, while reducing risks and improving safety for trial subjects and patients (Figure 3 and Table 1). Furthermore, the Oncopig® utilizes the same metabolic processes that result in clinical pathogenesis supporting the testing of new pharmacological and biological therapeutics. Advantages of these models include rapid formation of tumors of clinically relevant sizes for device testing. Use cases for the Oncopig® cancer models with non-specific tumor histology are broad and include use for preclinical evaluation of devices spanning interventional radiology, surgery, and endoscopy, including ablation and/or therapeutic delivery devices. Applications for interventional radiology include testing new imaging approaches for tumor detection and targeting, evaluation of new biopsy approaches, and testing arterially-directed or percutaneous device-based therapeutic approaches. Applications for the surgical field include evaluation of microdissection tools, robotic surgical equipment, laparoscopy approaches, and evaluation of new devices for tumor sampling, resection, and treatment. Applications for endoscopy fields including testing new endoscope-based imaging, biopsy, and treatment approaches. These models are also widely applicable for evaluation of novel next-generation external imaging devices, including novel CT/MRI approaches, augmented reality/virtual reality tools, and guidance software. Radiation studies are also feasible using the Oncopig® model, including both external and internally-delivered radiation therapies. Finally, these models can also be incorporated in training programs utilizing phantoms or healthy pigs to provide a more accurate “real world” experience by facilitating targeting of tumor masses in living animals.
Table 1. Applications of Oncopig® and Porcine Cancer Models
| Tumor Location | Applications |
|---|---|
| Sarcoma | In vivo induction⁹˒²⁰ and immune responses³⁶; transcriptional microenvironments³⁹; and nuclear drug targets⁵⁰ |
| Intramuscular | Histology and imaging²⁰ |
| Intratesticular | Histology and imaging²⁰ |
| Liver | autologous Oncopig® hepatocellular model⁵¹˒⁵²; genome editing³⁷; drug metabolism²⁵; hyperthermia and ultrasound treatment⁵³; local regional therapies–molecular and immune⁵⁴; microenvironments⁵⁵; precision medicine editing³⁷; genome editing tumor cells⁴⁰; drug eluting beads²⁸˒²⁹; micro-ablation³⁰; radioembolization³⁵; staging liver microenvironment⁵⁶˒⁵⁷; radiologic modalities⁵⁸; biomarkers⁵⁹; glass microsphere therapeutics⁶⁰; image guided ultrasound thermal ablation⁵³˒⁶¹˒⁶²; radiological staging⁵⁶; robotic surgery⁴³ |
| Lung | In vivo modeling via endovascular Cre induction or ex vivo biopsy Cre induction⁶⁴; microwave ablation³² |
| Bladder | Cre injection into bladder⁶⁵, drug screening⁶⁶ |
| Uterine | Histological and marker development⁶² |
| Ovarian | Histological and marker development⁶² |
| Skin | Cre-inducible melanoma model⁶⁷ |
| Kidney | Micro-ablation³⁰˒³¹˒³³, transcatheter probe development⁶⁸ |
| Colorectal | Drug delivery⁶⁹; site-specific electroporation⁷⁰; biomarkers⁷¹˒⁷²; esophageal microparticle treatment⁶⁹ |
| Pancreatic | Endovascular injection of Cre⁷³˒⁷⁴; Cre induction through duct⁷⁵; staging⁷³ |
The promise of liquid biopsies to advance precision medicine strategies requires a large animal model to support collection of adequate samples over an extended time course. One major challenge associated with translating targeted therapeutics into clinical practice is the extensive use of CT and MRI for hepatocellular carcinoma (HCC) diagnosis, which results in a lack of routine clinical biopsy collections for biological profiling²⁶˒²⁸˒²⁹. Therefore, while studies have demonstrated molecular and metabolic profiling can provide novel insights into HCC development, aggressiveness, and treatment response³⁰⁻³², the lack of routine clinical HCC biopsy collection has significantly limited our knowledge of HCC tumor biology and slowed progression of HCC precision medicine approaches³³⁻³⁵. To address this unmet clinical need, testing and validation of minimally invasive profiling techniques—such as liquid biopsy approaches to detect driver mutations in cell free DNA (cfDNA)—are critically needed. Liquid biopsy is based on the analysis of cfDNA fragments originating from cells as a result of cell death due to normal cell turnover, and as part of the immune response when tissue damage or a disease like cancer is present. Temporal profiling of cfDNA carrying cancer-specific information such as the presenceabsence of driver mutations has the potential to improve treatment stratification, prognosis, and treatment response monitoring, especially for cancers like HCC that are not routinely biopsied. Therefore, the combination of improved minimally invasive approaches to profile HCC tumor biology and development of preclinical models for targeted therapeutic testing has the potential to significantly improve clinical HCC outcomes.
OUTLOOKS AND FUTURE PERSPECTIVES FOR PORCINE BIOMEDICAL MODELS
Progress has clearly been achieved in the utility of the pig as a large animal biomedical model⁶˒⁹˒²¹˒³⁶˒³⁷. The justification for using genetically modified animals (GMO) to develop a disease on demand reflects the Principles of 3Rs (Replacement, Reduction and Refinement). The use of such a GMO animal replaces the need for intensive and painful chemical/radiation exposures to induce tumors; significantly reduces the number of pigs for large pre-clinical trials; and refines pre-clinical modeling due to the fact that the Oncopig® provides a single animal in which to conduct safety, risk and efficacy studies. The coming years yet still require focused attention with respect to full utility for drug, diagnostic and device development. Following are areas in which we have identified that require the broader research community. The amount of time and money invested into cancer therapeutic research, development, and clinical trials has continually increased over the past few decades. Despite record high cancer therapeutic approval rates, cancer remains a leading cause of death worldwide. This necessitates more effective tools to translate novel therapies into clinical practice. Current issues associated with clinical trials specifically focus on poor accrual rates and time for trial completion. In addition, preclinical studies are required before advancing to clinical trials. The translational Oncopig Cancer Model® provides a notable enhancement to current preclinical models. To address issues impacting the poor success rate of oncology clinical trials, we are incorporating the transformative Oncopig® platform into the cancer diagnostic and therapeutic approval process. Due to the Oncopig®’s high homology to humans and similar tumor phenotypes, their utility provides improved preclinical indication for both therapeutic safety and efficacy prior to investing significant time and money in human clinical trials.In addition, because treated and untreated tumors can simultaneously exist in an individual animal, each Oncopig® can feasibly serve as its own internal control, thereby allowing the Oncopig® platform to accelerate development, safety, and efficacy testing of new clinical products and procedures. The hypothesis behind the Oncopig® was that genetic alteration of pathways commonly disrupted in human cancers could provide a standardized disease site porcine tumor model, analogous to human tumors, which supports therapeutic investigation. Certainly, evidence provided in this mini review supports that hypothesis. However, further technological advances will allow exploitation of these platforms as a tool for a wide range of cancer therapies. For example, although AdCre has provided a robust induction signal more specific induction vectors with tissue-specific Cre expression should be developed. Further, utilizing viral vectors that co-express Cre recombinase and CRISPR genome editing components would support both induction of transgene expression and the ability for additional defined oncogenic mutations. Delivery of induction signals and genome editing components will require approaches for defined delivery to cells over extended time periods. This is due to the inherent need for cells to be dividing so that recombination and nuclear division and repair mechanisms are functioning. Thus, in low mitogenic tissues, delivery vehicles (loaded patches or nanoparticles with defined signal release) need to be developed.Disadvantages of these models include formation of tumors with non-specific tumor histology (due to lack of cell-specific targeting of the AdCre vector) and spontaneous regression observed over the course of several weeks to months due to T cell mediated tumor cell killing. This spontaneoustumor regression is eliminated using cyclosporine a dosing to facilitate long-term efficacy studies. The development of next-generation sequencing technology has made the evaluation of mutated genes possible in clinical practice, allowing for identification of driver mutations underlying cancer development in individual patients²⁶˒³⁸˒³⁹. This, combined with recent advances in gene editing technologies such as CRISPR-Cas9 enables development of personalized tumor models for prediction of treatment responses for mutational profiles observed clinically³⁷˒⁴⁰.While human clinical trials are the benchmark for testing cancer diagnostics and therapies, regulatory, enrollment, and financial challenges of trial inception are significant⁵˒²³. Advances in cancer care are therefore dependent upon the use of preclinical in vivo model systems to test new treatments. However, therapeutic success in preclinical rodent glioblastoma multiforme (GBM) models does not translate to improved patient outcomes in clinical trials and underscore the deficiencies of these models to recapitulate the complexity of human GBM biology and clinical responses¹³˒¹⁴. In addition, rodent models are not amenable to clinically relevant imaging, surgical, or LRT studies and differ vastly from humans with respect to brain size (300× smaller), structure (negligible white matter and gyral formation), and systemic immune physiology (only 10% overlap)¹³. Therefore, development of a large animal model that more closely reflects human brain size, structure, physiology, and systemic immunity is imperative⁴¹. In contrast to mice, the pig brain is only 5–10× smaller than humans and has extremely similar white matter composition, gyral structure, and immune systems (80% overlap)¹⁴˒⁴²˒⁴³. However, despite the increased clinical relevance compared to rodents, to date developed porcine xenografts GBM models have required immunosuppression to facilitate tumor induction⁴²˒⁴⁴˒⁴⁵. In addition, while progress has been made on porcine GBM model development using lentiviral vector-based induction of cancer driver mutations, these models have significant limitations, including need for BSL2 containment, demonstrated capability limited to spinal cord, development of motor deficits within 3-weeks, and limited control of driver mutational profiles and tumor heterogeneity⁴⁶. Therefore, generation of novel immunocompetent porcine GBM models as described in this proposal has the potential to accelerate translation of GBM diagnostic imaging and therapeutic approaches spanning surgical techniques, LRTs, and precision medicine into clinical practice, resulting in improvements in patient outcomes and quality of life not possible with current rodent models. Technological approaches to address lack of inbred breeds.Critical to the full utility of using Oncopigs® is to: (1) mitigate the inflammatory anti-tumor immune response and prevent tumor regression; (2) develop vectors to enhance in vivo somatic cell genome editing; (3) development of rare cancer models; and (4) develop strains of Oncopigs® with inherent comorbidities, e.g. obesity, diabetes, metabolic syndrome or atherosclerosis⁴⁷˒⁴⁸ or through induction via diet⁴⁷˒⁴⁸. Finally, the use of transgenic pigs requires FDA regulatory clearance for use across the United States; thus, recognition by health regulatory agencies of the Oncopig® and other transgenic pigs value as a pre-clinical model⁴⁹ is a critical next step, and building upon the foundational work with Oncopigs® to establish mini-pig lines for broader applications.
Acknowledgements
The authors acknowledge support from the NIH (NCI 5R44CA268304) to partially support this work presented here. The authors also recognized the contributions from Dr. Lobena Elkhadragy, U of Illinois Medical Center, in development of the figures and tables.
Funding
DOD grant #CA150590
NIH grant #CA263034
Author Bio-sketches
Vera Mehta
Jessica Rege
Kyle Schachtsneider
Lawrence Schook
References
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. May 2021;71 (3):209-249. doi:10.3322/caac.21660
2. Honkala A, Malhotra SV, Kummar S, Junttila MR. Harnessing the predictive power of preclinical models for oncology drug development. Nature Reviews Drug Discovery. 2022/02/01 2022;21(2): 99-114. doi:10.1038/s41573-021-00301-6
3. Bryda EC. The Mighty Mouse: the impact of rodents on advances in biomedical research. Mo Med. May-Jun 2013;110(3):207-11.
4. Onaciu A, Munteanu R, Munteanu VC, et al. Spontaneous and Induced Animal Models for Cancer Research. Diagnostics (Basel). Aug 31 2020;10(9) doi:10.3390/diagnostics10090660
5. Sajjad H, Imtiaz S, Noor T, Siddiqui YH, Sajjad A, Zia M. Cancer models in preclinical research: A chronicle review of advancement in effective cancer research. Animal Model Exp Med. Jun 2021;4(2):87-103. doi:10.1002/ame2.12165
6. Schook L, Beattie C, Beever J, et al. Swine in biomedical research: creating the building blocks of animal models. Anim Biotechnol. 2005;16(2): 183-90. doi:10.1080/10495390500265034
7. Hou N, Du X, Wu S. Advances in pig models of human diseases. Animal Model Exp Med. Apr 2022;5(2):141-152. doi:10.1002/ame2.12223
8. Meyerholz DK, Burrough ER, Kirchhof N, Anderson DJ, Helke KL. Swine models in translational research and medicine. Vet Pathol. Jul 2024;61(4):512-523. doi:10.1177/03009858231222235
9. Schook LB, Collares TV, Darfour-Oduro KA, et al. Unraveling the swine genome: implications for human health. Annu Rev Anim Biosci. 2015;3: 219-44. doi:10.1146/annurev-animal-022114-110815
10. Groenen MAM, Archibald AL, Uenishi H, et al. Analyses of pig genomes provide insight into porcine demography and evolution. Nature. 2012/ 11/01 2012;491(7424):393-398. doi:10.1038/natur e11622
11. Schachtschneider KM, Schwind RM, Darfour-Oduro KA, et al. A validated, transitional and translational porcine model of hepatocellular carcinoma. Oncotarget. Sep 8 2017;8(38):63620-63634. doi:10.18632/oncotarget.18872
12. Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. Mar 10 2005;352(10):987-96. doi:10.1056/NEJMo a043330
13. de Jong M, Maina T. Of mice and humans: are they the same?–Implications in cancer translational research. J Nucl Med. Apr 2010;51(4):501-4. doi:10.2967/jnumed.109.065706
14. Hicks WH, Bird CE, Pernik MN, et al. Large Animal Models of Glioma: Current Status and Future Prospects. Anticancer Res. Nov 2021;41 (11):5343-5353. doi:10.21873/anticanres.15347
15. Integrated Genomic Characterization of Pancreatic Ductal Adenocarcinoma. Cancer Cell. Aug 14 2017;32(2):185-203.e13. doi:10.1016/j.cce ll.2017.07.007
16. Connor AA, Denroche RE, Jang GH, et al. Integration of Genomic and Transcriptional Features in Pancreatic Cancer Reveals Increased Cell Cycle Progression in Metastases. Cancer Cell. Feb 11 2019;35(2):267-282.e7. doi:10.1016/j.ccel l.2018.12.010
17. Aravalli RN, Golzarian J, Cressman EN. Animal models of cancer in interventional radiology. Eur Radiol. May 2009;19(5):1049-53. doi:10.1007/s00330-008-1263-8
18. Overgaard NH, Fan TM, Schachtschneider KM, Principe DR, Schook LB, Jungersen G. Of Mice, Dogs, Pigs, and Men: Choosing the Appropriate Model for Immuno-Oncology Research. Ilar j. Dec 31 2018;59(3):247-262. doi:10.1093/ilar/ily014
19. Pollock CB, Rogatcheva MB, Schook LB. Comparative genomics of xenobiotic metabolism: a porcine-human PXR gene comparison. Mamm Genome. Mar 2007;18(3):210-9. doi:10.1007/s00335-007-9007-7
20. Schook LB, Collares TV, Hu W, et al. A Genetic Porcine Model of Cancer. PLoS One. 2015;10(7):
e0128864. doi:10.1371/journal.pone.0128864
21. Elkhadragy L, Gaba RC, Niemeyer MM, Schook LB, Schachtschneider KM. Translational Relevance and Future Integration of the Oncopig® Cancer Model in Preclinical Applications. Annu Rev Anim Biosci. Oct 17 2024;doi:10.1146/annurev-animal-111523-102125
22. Joshi K, Telugu BP, Prather RS, et al. Benefits and opportunities of the transgenic Oncopig® cancer model. Trends Cancer. Mar 2024;10(3):182-184. doi:10.1016/j.trecan.2024.01.005
23. Robertson N, Schook LB, Schachtschneider KM. Porcine cancer models: potential tools to enhance cancer drug trials. Expert Opin Drug Discov. Aug 2020;15(8):893-902. doi:10.1080/17460441.2 020.1757644
24. Schachtschneider KM, Schwind RM, Newson J, et al. The Oncopig® Cancer Model: An Innovative Large Animal Translational Oncology Platform. Front Oncol. 2017;7:190. doi:10.3389/fo nc.2017.00190
25. Lobianco F, Giurini E, Neto M, et al. 03:27 PM Abstract No. 221 Porcine and human hepatocellular carcinoma cell lines present similar drug-metabolizing enzyme expression levels and comparable sorafenib and doxorubicin cytotoxic responses. Journal of Vascular and Interventional Radiology. 2019;30 (3):S99-S100. doi:10.1016/j.jvi r.2018.12.279
26. Xu C, Wu S, Schook LB, Schachtschneider KM. Translating Human Cancer Sequences Into Personalized Porcine Cancer Models. Front Oncol. 2019;9:105. doi:10.3389/fonc.2019.00105
27. Singhal M, Khatibeghdami M, Principe DR, et al. TM4SF18 is aberrantly expressed in pancreatic cancer and regulates cell growth. PLoS One. 2019; 14(3):e0211711. doi:10.1371/journal.pone.0211711
28. Namur J, Wassef M, Millot JM, Lewis AL, Manfait M, Laurent A. Drug-eluting beads for liver embolization: concentration of doxorubicin in tissue and in beads in a pig model. J Vasc Interv Radiol. Feb 2010;21(2):259-67. doi:10.1016/j.jvir.2009.10.026
29. Isfort P, Rauen P, Na HS, et al. Does Drug-Eluting Bead TACE Enhance the Local Effect of IRE? Imaging and Histopathological Evaluation in a Porcine Model. Cardiovasc Intervent Radiol. Jun 2019;42(6):880-885. doi:10.1007/s00270-019-02181-1
30. Sommer CM, Arnegger F, Koch V, et al. Microwave ablation of porcine kidneys in vivo: effect of two different ablation modes (“temperature control” and “power control”) on procedural outcome. Cardiovasc Intervent Radiol. Jun 2012;35(3):653-60. doi:10.1007/s00270-011-0171-5
31. Laeseke PF, Lee FT, Jr., Sampson LA, van der Weide DW, Brace CL. Microwave ablation versus radiofrequency ablation in the kidney: high-power triaxial antennas create larger ablation zones than similarly sized internally cooled electrodes. J Vasc Interv Radiol. Sep 2009;20(9):1224-9. doi:10.1016/j .jvir.2009.05.029
32. Carberry GA, Nocerino E, Cristescu MM, Smolock AR, Lee FT, Jr., Brace CL. Microwave Ablation of the Lung in a Porcine Model: Vessel Diameter Predicts Pulmonary Artery Occlusion. Cardiovasc Intervent Radiol. Oct 2017;40(10): 1609-1616. doi:10.1007/s00270-017-1689-y
33. Wagstaff PG, de Bruin DM, van den Bos W, et al. Irreversible electroporation of the porcine kidney: Temperature development and distribution. Urol Oncol. Apr 2015;33(4):168.e1-7. doi:10.1016/ j.urolonc.2014.11.019
34. Swietlik JF, Mauch SC, Knott EA, et al. Noninvasive thyroid histotripsy treatment: proof of concept study in a porcine model. Int J Hyperthermia. 2021;38(1):798-804. doi:10.1080/0 2656736.2021.1922762
35. Schachtschneider K, Arepally A, Blanco D, et al. Abstract No. LBA2 Preclinical Evaluation of Yttrium-90 Radioembolization in the Oncopig® Liver Cancer Model. Journal of Vascular and Interventional Radiology. 2024;35(3):S226. doi:10.1016/j.jvir.202 4.01.016
36. Overgaard NH, Principe DR, Schachtschneider KM, et al. Genetically Induced Tumors in the Oncopig® Model Invoke an Antitumor Immune Response Dominated by Cytotoxic CD8β(+) T Cells and Differentiated γδ T Cells Alongside a Regulatory Response Mediated by FOXP3(+) T Cells and Immunoregulatory Molecules. Front Immunol. 2018;9:1301. doi:10.3389/fimmu.2018.01301
37. Elkhadragy L, Dasteh Goli K, Totura WM, et al. Effect of CRISPR Knockout of AXIN1 or ARID1A on Proliferation and Migration of Porcine Hepatocellular Carcinoma. Front Oncol. 2022;12:904031. doi:10.3389/fonc.2022.904031
38. Schachtschneider KM, Jungersen G, Schook LB, Shanmuganayagam D. Editorial: “Humanized” Large Animal Cancer Models: Accelerating Time and Effectiveness of Clinical Trials. Front Oncol. 2019;9:793. doi:10.3389/fonc.2019.00793
39. Schachtschneider KM, Liu Y, Mäkeläinen S, et al. Oncopig® Soft-Tissue Sarcomas Recapitulate Key Transcriptional Features of Human Sarcomas. Scientific Reports. 2017/06/01 2017;7(1):2624. doi:10.1038/s41598-017-02912-9
40. Elkhadragy L, Regan MR, W MT, et al. Generation of genetically tailored porcine liver cancer cells by CRISPR/Cas9 editing. Biotechniques. Nov 23 2020;doi:10.2144/btn-2020-0119
41. Lind NM, Moustgaard A, Jelsing J, Vajta G, Cumming P, Hansen AK. The use of pigs in neuroscience: modeling brain disorders. Neurosci Biobehav Rev. 2007;31(5):728-51. doi:10.1016/j.ne ubiorev.2007.02.003
42. Selek L, Seigneuret E, Nugue G, et al. Imaging and histological characterization of a human brain xenograft in pig: the first induced glioma model in a large animal. J Neurosci Methods. Jan 15 2014; 221:159-65. doi:10.1016/j.jneumeth.2013.10.002
43. Ho CS, Lunney JK, Lee JH, et al. Molecular characterization of swine leucocyte antigen class II genes in outbred pig populations. Anim Genet. Aug 2010;41(4):428-32. doi:10.1111/j.1365-2052.2 010.02019.x
44. Khoshnevis M, Carozzo C, Bonnefont-Rebeix C, et al. Development of induced glioblastoma by implantation of a human xenograft in Yucatan minipig as a large animal model. J Neurosci Methods. Apr 15 2017;282:61-68. doi:10.1016/j.jneumeth.20 17.03.007
45. Khoshnevis M, Carozzo C, Brown R, et al. Feasibility of intratumoral 165Holmium siloxane delivery to induced U87 glioblastoma in a large animal model, the Yucatan minipig. PLoS One. 2020; 15(6):e0234772. doi:10.1371/journal.pone.0234772
46. Tora MS, Texakalidis P, Neill S, et al. Lentiviral Vector Induced Modeling of High-Grade Spinal Cord Glioma in Minipigs. Sci Rep. Mar 24 2020;10(1):5291. doi:10.1038/s41598-020-62167-9
47. Gaba RC, Mendoza-Elias N, Regan DP, et al. Characterization of an Inducible Alcoholic Liver Fibrosis Model for Hepatocellular Carcinoma Investigation in a Transgenic Porcine Tumorigenic Platform. J Vasc Interv Radiol. Aug 2018;29(8): 1194-1202.e1. doi:10.1016/j.jvir.2018.03.007
48. Yasmin A, Regan DP, Schook LB, Gaba RC, Schachtschneider KM. Transcriptional regulation of alcohol induced liver fibrosis in a translational porcine hepatocellular carcinoma model. Biochimie. Mar 2021;182:73-84. doi:10.1016/j.biochi.2020.12.022
49. Boettcher AN, Schachtschneider KM, Schook LB, Tuggle CK. Swine models for translational oncological research: an evolving landscape and regulatory considerations. Mamm Genome. Mar 2022;33(1):230-240. doi:10.1007/s00335-021-09907-y
50. Ye M, Misra SK, De AK, et al. Design, Synthesis, and Characterization of Globular Orphan Nuclear Receptor Regulator with Biological Activity in Soft Tissue Sarcoma. J Med Chem. Dec 13 2018; 61(23):10739-10752. doi:10.1021/acs.jmedchem.8 b01387
51. Nurili F, Monette S, Michel AO, et al. Transarterial Embolization of Liver Cancer in a Transgenic Pig Model. Journal of Vascular and Interventional Radiology. 2021/04/01/ 2021;32(4): 510-517.e3. doi:https://doi.org/10.1016/j.jvir.2020.09.011
52. Gaba RC, Elkhadragy L, Boas FE, et al. Development and comprehensive characterization of porcine hepatocellular carcinoma for translational liver cancer investigation. Oncotarget. Jul 14 2020; 11(28):2686-2701. doi:10.18632/oncotarget.27647
53. Misra SK, Ghoshal G, Gartia MR, et al. Trimodal Therapy: Combining Hyperthermia with Repurposed Bexarotene and Ultrasound for Treating Liver Cancer. ACS Nano. Nov 24 2015;9(11):10 695-10718. doi:10.1021/acsnano.5b05974
54. Llovet JM, De Baere T, Kulik L, et al. Locoregional therapies in the era of molecular and immune treatments for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. May 2021;18(5): 293-313. doi:10.1038/s41575-020-00395-0
55. Patel SS, Sandur A, El-Kebir M, Gaba RC, Schook LB, Schachtschneider KM. Transcriptional Profiling of Porcine HCC Xenografts Provides Insights Into Tumor Cell Microenvironment Signaling. Front Genet. 2021;12:657330. doi:10.3389/fgen e.2021.657330
56. Pirasteh A, Periyasamy S, Meudt JJ, et al. Staging Liver Fibrosis by Fibroblast Activation Protein Inhibitor PET in a Human-Sized Swine Model. J Nucl Med. Dec 2022;63(12):1956-1961. doi:10.2967/jnumed.121.263736
57. Gaba RC, Elkhadragy L, Pennix T, et al. Magnetic Resonance Elastography for Staging Liver Fibrosis in the Oncopig®. Diagnostics (Basel). Aug 28 2024;14(17) doi:10.3390/diagnostics14171880
58. Faraji F, Gaba RC. Radiologic Modalities and Response Assessment Schemes for Clinical and Preclinical Oncology Imaging. Front Oncol. 2019; 9:471. doi:10.3389/fonc.2019.00471
59. Lin KT, Shann YJ, Chau GY, Hsu CN, Huang CY. Identification of latent biomarkers in hepatocellular carcinoma by ultra-deep whole-transcriptome sequencing. Oncogene. Sep 25 2014;33(39):4786-94. doi:10.1038/onc.2013.424
60. Jaroch DB, Liu Y, Kim AY, Katz SC, Cox BF, Hullinger TG. Intra-arterial Pressure-Enabled Drug Delivery Significantly Increases Penetration of Glass Microspheres in a Porcine Liver Tumor Model. J Vasc Interv Radiol. Oct 2024;35(10):1525-1533.e4. doi:10.1016/j.jvir.2024.06.030
61. Rund LA, Ghoshal G, Williams E, et al. Abstract 2148: Image-guided catheter-based ultrasound thermal ablation of intramuscular and retroperitoneal sarcomas in the transgenic Oncopig® cancer model. Cancer Research. 2018;78(13_Supplement):2148-2148. doi:10.1158/1538-7445.Am2018-2148
62. Rund LA, Schachtschneider KM, Gaba RC, et al. Abstract 3105: Oncopig® carcinoma cell lines: A foundation for co-clinical trials. Cancer Research. 2018;78(13 Supplement):3105-3105. doi:10.1158/1 538-7445.Am2018-3105
63. O’Connell RM, Horne S, O’Keeffe DA, et al. A novel low-cost high-fidelity porcine model of liver metastases for simulation training in robotic parenchyma-preserving liver resection. J Robot Surg. Nov 5 2024;18(1):394. doi:10.1007/s11701-024-02151-x
64. Ghosn M, Elsakka AS, Petre EN, et al. Induction and preliminary characterization of neoplastic pulmonary nodules in a transgenic pig model. Lung Cancer. Apr 2023;178:157-165. doi:10.1016/j.lungcan.2023.02.013
65. Aulitzky A VBR, Kim K, Al-Ahmadie H, Monette S, Coleman JA. MP14-02 DEVELOPMENT OF A PORCINE MODEL OF BLADDER CANCER USING THE ONCOPIG®. Journal of Urology. 2023; 209(Supplement 4):e182. doi:10.1097/JU.0000000 000003234.02
66. Segatto NV, Bender CB, Seixas FK, et al. Perspective: Humanized Pig Models of Bladder Cancer. Front Mol Biosci. 2021;8:681044. doi:10.3389/fmolb.2021.681044
67. Oh D, Hong N, Eun K, et al. Generation of a genetically engineered porcine melanoma model featuring oncogenic control through conditional Cre recombination. Sci Rep. Jan 10 2025;15(1): 1616. doi:10.1038/s41598-024-82554-w
68. Rice SL, Muñoz FG, Benjamin J, et al. Transcatheter pseudo-vascular isolation for localization and concentration of a large molecule theranostic probe into a transgenic Oncopig® kidney tumor. Nucl Med Biol. Sep-Oct 2024;136-137:108939. doi:10.1016/j.nucmedbio.2024.108939
69. Yano H, Sasaki F, Maeda H, et al. Effect of sprayable, highly adhesive hydrophobized gelatin microparticles on esophageal stenosis after endoscopic submucosal dissection: an experimental study in a swine model. Esophagus. Jan 2025;22 (1):95-104. doi:10.1007/s10388-024-01090-8
70. Rugivarodom M, Sonani H, Kamba S, Kee Song LW, Graham R, Rajan E. CREATING A PORCINE MODEL FOR COLORECTAL CANCER AND ASSESSING THE EFFICACY AND SAFETY OF ELECTROPORATION TREATMENT. Gastrointestinal Endoscopy. 2024;99(6):AB452-AB453. doi:10.1016/j.g ie.2024.04.1426
71. Ganepola GA, Nizin J, Rutledge JR, Chang DH. Use of blood-based biomarkers for early diagnosis and surveillance of colorectal cancer. World J Gastrointest Oncol. Apr 15 2014;6(4):83-97. doi:10.4251/wjgo.v6.i4.83
72. Lou J, Zhang L, Lv S, Zhang C, Jiang S. Biomarkers for Hepatocellular Carcinoma. Biomark Cancer. 2017;9:1-9. doi:10.1177/1179299×16684640
73. Boas FE, Nurili F, Bendet A, et al. Induction and characterization of pancreatic cancer in a transgenic pig model. PLoS One. 2020;15(9):e02 39391. doi:10.1371/journal.pone.0239391
74. Mondal P, Patel NS, Bailey K, et al. Induction of pancreatic neoplasia in the KRAS/TP53 Oncopig®. Dis Model Mech. Jan 1 2023;16(1) doi:10.1242/dm m.049699
75. Principe DR, Overgaard NH, Park AJ, et al. KRAS(G12D) and TP53(R167H) Cooperate to Induce Pancreatic Ductal Adenocarcinoma in Sus scrofa Pigs. Sci Rep. Aug 22 2018;8(1):12548. doi:10.1038/s41598-018-30916-6