

Mapping Biomedical Engineering Workforce in Pacific Islands
Mapping the Biomedical Engineering Workforce in 16 Pacific Island Countries and Territories to Strengthen Capacity and Health Service Delivery
Sunema Talapusi 1, Melanie Wratten 2, Si Thu Win Tin 1
- The Pacific Community (SPC), Fiji
- Alfred Health, Australia.
OPEN ACCESS
PUBLISHED 30 April 2025
CITATION: Talapusi, S., Wratten, M., et al., 2025. Mapping the Biomedical Engineering Workforce in 16 Pacific Island Countries and Territories to Strengthen Capacity and Health Service Delivery. Medical Research Archives, [online] 13(4). https://doi.org/10.18103/mra.v13i4.6455
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i4.6455
ISSN 2375-1924
ABSTRACT
Background: Biomedical engineering services play a vital role in clinical services and patient care by ensuring effectiveness and safe operation of medical devices and technology in healthcare settings. In the Pacific Island region, the biomedical engineering services has been a regional priority, particularly following the COVID-19 pandemic. However, no recent situational analysis has been carried out, with the last analysis conducted in 2014.
Aim: This study aims to assess the number and capacity of biomedical engineers and technicians currently supporting the Ministries of Health in the Pacific Island Countries and Territories (PICTs) in order to strengthen capacity and enhance biomedical services to ultimately improve health service delivery in the Pacific.
Methods: A Biomedical Situational Analysis Questionnaire and a Biomedical Workforce Profile were used for the assessment across 22 PICTs in 2023. Data were validated by key biomedical staff in each country.
Results: A total of 16 PICTs participated in the study. The findings indicate that there were 98 biomedical engineers and technicians in the region. Of these, 94% were local professionals working within their respective Ministries of Health, while 4% were expatriates from Fiji and Tonga, and 2% were from Philippines. Women represented 17% of the biomedical workforce and the majority (66%) were under the age of 40. With regards to their qualifications, 21% hold a bachelor’s degree and 62% have a certificate and/or diploma relating to biomedical engineering. A majority of the surveyed countries (80%, n=13) reported that more than 50% of biomedical services in their respective healthcare facilities were provided in-house by their local biomedical engineers and technicians.
Conclusion: This is the most up-to-date comprehensive analysis of the biomedical workforce capacity available for the Pacific countries. This study shows the gaps in biomedical services and emphasizes the urgent need for governments and development partners to continuously support and strengthen the biomedical workforce in the Pacific region. Enhancing the biomedical workforce will contribute to an improved and more efficient healthcare service delivery in the Pacific.
Keywords: Pacific Islands, workforce, capacity, biomedical engineers
Introduction
Biomedical engineering services form an integral part to the delivery of clinical care and patient safety, ensuring that medical devices and technology operate effectively and safely in healthcare settings. Biomedical Engineers and Technicians (BMETs) are responsible for the full lifecycle management of medical equipment, including procurement, installation and maintenance, in healthcare facilities. These professionals play a critical role in preventing equipment malfunction and enhancing patient safety.
Members of the Pacific Biomedical Engineering Network (PBEN) uses the medical equipment definition stated AS/NZS 3551:2012 for their roles and responsibilities in their respective Ministries of Health (MOH). In the Pacific region, where healthcare infrastructure faces unique challenges, such as geographic isolation, limited resources, and diverse environmental conditions from natural disasters and climate change, the increasing complexity of supply and maintenance of appropriate medical equipment and technologies heighten the need for skilled biomedical engineering support.
In addition, the introduction of new medical technologies, while critical for improving health outcomes, has outpaced the development of local biomedical engineering expertise. This imbalance has resulted in equipment downtime, underutilization, and increased reliance on outsourced services, affecting the quality and efficiency of care. The importance of functioning medical equipment and skilled personnel in achieving health service delivery standards has been widely recognized, particularly in the context of strengthening health systems in low- and middle-income countries.
To address these challenges, the Clinical Service Program under the Public Health Division of the Pacific Community (SPC) collaborates with Pacific Island Countries & Territories (PICTs) and partners to provide technical support and to explore regional opportunities and solutions for biomedical services, including strengthening for the PBEN.
Despite the increasing reliance on medical equipment in healthcare systems, many countries lack a sustainable biomedical workforce to support, maintain and operate these systems. The absence of up-to-date data on capacity and distribution of biomedical professionals in the Pacific hinders effective health planning and technology management. This study aims to fill the gap by assessing the number and capacity of BMETs currently supporting the MOHs in the PICTs in order to strengthen capacity and enhance biomedical services to ultimately improve health service delivery in the Pacific.
Methods
The Biomedical Situational Analysis Questionnaire was distributed via email in April 2023 to all 22 member PICTs of SPC. The questionnaire was adapted from the 2014 survey which was developed based on the ‘Pacific Biomedical Standards: Standards for Managing Biomedical Services in the Pacific Region’ in which biomedical workforce support was one of the six components of the survey. The questionnaire consisted of a mixture of dichotomous questions and 5-point Likert scale with open ended section to support the responses.
To further capture workforce data, the Biomedical Workforce Profile as a Microsoft Excel spreadsheet was sent to member countries, requesting information on the available biomedical engineering workforce, including demographic details such as gender, age and the highest level of qualification. To resolve any discrepancies, the surveys were also distributed to key biomedical staff (managerial and technical) to verify response, with the requirement of sign-off by Directors of Clinical Services in each country.
Definitions of biomedical engineers and technicians were clearly outlined. A biomedical engineer was defined as an individual holding a bachelor’s degree in biomedical engineering or related field such as electrical, electronic and mechanical engineering. A biomedical technician was defined as an individual holding a minimum certificate level in biomedical, electrical, electronic or related engineering field and/or bachelor level degree in science and other non-biomedical related bachelor level degrees. Those without formal qualifications were defined as interns or trainees.
To assess the availability and capacity of the biomedical workforce, a related question inquired about the type of biomedical engineering services in country, specifically whether these supports were provided in-house, outsourced or a combination of both.
Data collection was followed up by SPC’s Biomedical Adviser through email, phone and/or in person communication. The collected data was analysed using Microsoft Excel.
Results
Sixteen PICTs including American Samoa, Cook Islands, Federated States of Micronesia (Kosrae and Yap States), Fiji, Kiribati, Republic of the Marshall Islands, Nauru, Niue, Palau, Papua New Guinea, Samoa, Solomon Islands, Tokelau, Tonga, Tuvalu and Vanuatu completed the questionnaire. The response rate was 73%.
Overall, 98 biomedical personnel were reported to be employed across the MOHs of the PICTs, including both local and expatriate staff. At the time of this survey, neither the Cook Islands nor Tokelau had any biomedical personnel.
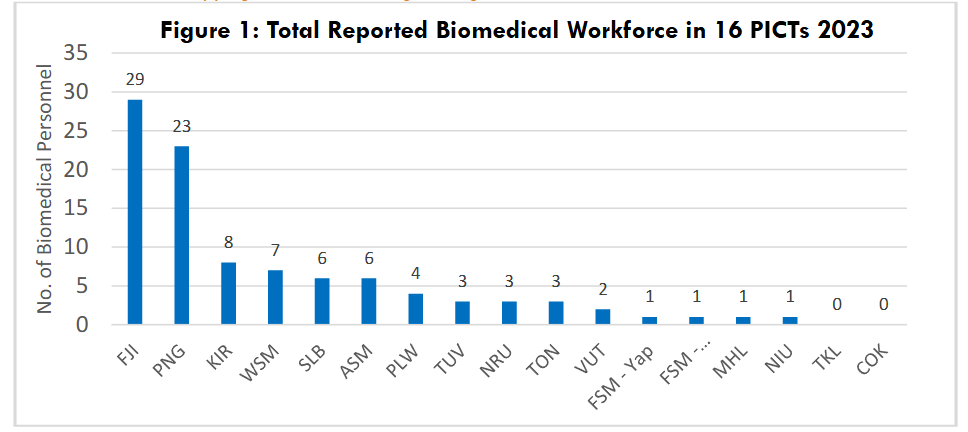
The majority of the biomedical workforce were local nationals (94%, n=92), with an additional 4% (n=4) made up of expatriates from other PICTs (from Fiji and Tonga), and 2% (n=2) of expatriates from other countries outside the region (Philippines).
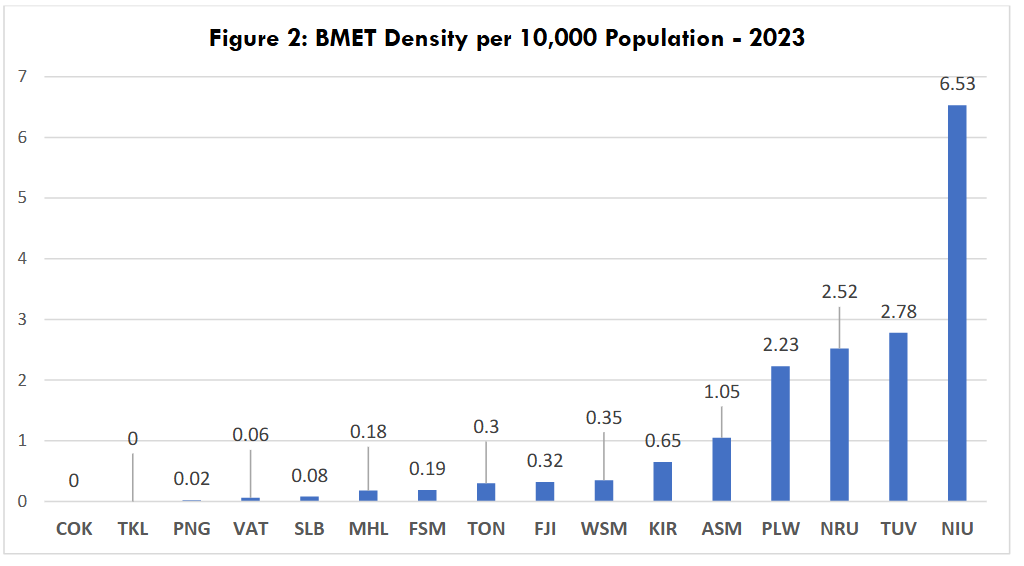
Figure 2 shows the BMET density per 10,000 population for the 16 PICTs. Countries with the youngest biomedical workforce (those aged 30 or younger) include: American Samoa (67%, n=4), Fiji (52%, n=15), Kiribati (50%, n=4), Nauru (67%, n=2), Niue (100%, n=1) and Samoa (71%, n=5). Countries with the oldest workforce include FSM – Yap (100% of staff over 50 years, n=1), Papua New Guinea (39% of staff over 50 years, n=9) and the Solomon Islands (33% staff over 60 years, n=2).
Overall, the biomedical workforce primarily consists of biomedical technicians (85%, n=83), with only 10% of the workforce being biomedical engineers (n=10) and the remaining 5% working as interns and trainees (n=5). In 2023, 21% (n=20) of biomedical staff held a bachelor-level degree, 62% (n=61) had a certificate or diploma, and 17% (n=17) had no formal qualifications. A majority of the surveyed countries (80%, n=13) recorded that more than 50% of biomedical services for their respective healthcare facilities are provided in-house by their own local biomedical engineers and technicians. The smaller islands countries (n=3) do not have local capacity and therefore outsource more than 50% of their biomedical services to private companies.
Discussion
This study provides the most comprehensive analysis to date of biomedical staff in the Pacific region, serving an important basis for ongoing monitoring of workforce development and capacity. This study found that the number of biomedical staff are low in many PICTs, highlighting a persistent lack of local human resource capacity and expertise. Although biomedical engineers and technicians are recognised as essential to health system strengthening, particularly in resource-constrained settings, there is currently no globally or regionally defined benchmark and global acceptable minimum threshold BMET density per 10,000 population as only physicians, nurses and midwives were considered by World Health Organization (WHO) in 2016.
The BMET density figures for the 16 PICTs from this study provide a baseline for future surveys. This aligns with the WHO objective of strengthening data on human resources for health by 2030 where biomedical engineers are recognized as one of the priorities in specialized service delivery.
There has been an increase in female staff represented in the biomedical field since 2014, noting that a higher number of countries were included in the 2023 data. Countries with the highest proportion of female representation are Fiji (28%, n=8) and Samoa (43%, n=3). In addition, this study has observed significant progress in female professionals attaining higher level engineering qualifications. In 2023, 40% (n=4) of Biomedical Engineers are female and all of them hold senior managerial roles leading biomedical services in their respective countries (n=4: American Samoa, Fiji, Kiribati and Samoa). These trends are consistent with the data for Australia in 2018 and in United States in 2017 that indicated that despite engineering fields being male dominated, there were increasing numbers of women entering biomedical engineering. Furthermore, the 2018 New Zealand Census reported that 20% of their biomedical workforce were female with more than 50% of those individuals working in Auckland Region.
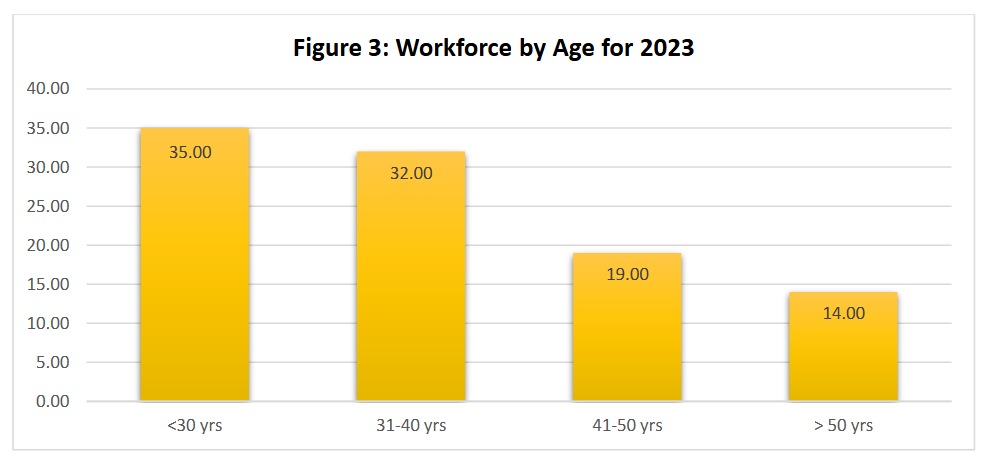
There has been a significant shift in the age demographic of BMETs in PICTs, as younger personnel have increasingly entered the biomedical engineering field. In 2014, only 35% of the biomedical workforce in PICTs was reported to be under the age of 40, however by 2023 the figure has almost doubled to 66%. With a younger biomedical workforce in the Pacific region, ongoing investment in mentorship, leadership and managerial skill development, along with a clear career pathway and succession planning will be essential to ensure this cadre of young professionals are appropriately supported in career progression. The increasing number of younger professionals entering the field presents both an opportunity and a challenge. While a youthful workforce offers long-term sustainability, it also requires structured professional development pathways, mentoring, and leadership training through a regionally harmonized career progression pathways, supported by national policies.
A limited biomedical workforce constrains countries’ ability to manage equipment inventories, implement preventative maintenance, and respond to technological failures. Investing in formal education, regional training hubs, and standardizing competencies will be critical in addressing this capacity gap. Additionally, ongoing recruitment, training and retention policies will be required to continue to build and maintain the human resource capacity required for the growing demands for the biomedical support across the region and to establish a sustainable regional biomedical workforce.
Despite an increase in the number of biomedical staff with formal qualifications, there remains a significant gap in the access to formal training in the region, and limited opportunities for biomedical staff to obtain university-level qualifications (undergraduate and postgraduate). Biomedical staff continue to undertake certification training for equipment, as well as on-the-job training to strengthen core skillsets. Though PICTs reported that 80% of biomedical engineering services were conducted in-house, these formal and informal training opportunities are essential for strengthening the workforce’s skill and further reducing dependence on outsourced biomedical support. The registration and accreditation of biomedical engineers and technicians at both the national and regional level could play an essential role in formalising the profession and ensuring consistency in skills and knowledge across the BMET professional cohort.
It is important to acknowledge a key limitation of the 2023 workforce data: it was based on self-reporting. Discrepancies between responses from administrators and biomed professionals remain a challenge, and variations in data across different years may be influenced by the knowledge, experience, and roles of the individuals tasked with completing the surveys. Additionally, sample sizes between the 2014 and 2023 surveys varied, making direct comparisons inappropriate. This study also lacked data on years of service as well as in-service training, which is crucial to obtaining a more accurate understanding of the workforce capacity and development in each country. Future biomedical workforce analysis studies should address these gaps. Despite the limitations, this study provides more detailed findings, as the questions were specific and clearly defined to capture an overall updated situation of the biomedical engineering workforce and services in the Pacific.
Conclusion
In conclusion, retaining qualified and experienced biomedical staff continues to be a significant challenge across all PICTs. This highlights the need to continuously develop the capacity of the biomedical workforce to keep up with the constant advancement in technology, ensuring that comprehensive biomedical support is available to health systems throughout the Pacific region. This study also highlights the importance of improving health workforce information systems and the need for more research in biomedical field. Future studies should consider collecting longitudinal data, capturing in-service training and retention rates to support more targeted interventions.
Global and regional collaboration, through networks such as the PBEN, plays a critical role in knowledge exchange, peer support, and collective advocacy. Sustained support for the networks can help smaller island states overcome workforce isolation and promote sustainable, scalable biomedical solutions to achieving the Health Islands Vision and the Blue Pacific 2050 Strategy on health, which emphasize resilient health systems. It also supports SDG 3 (Good Health and Well-being) by ensuring health systems have the skilled professionals needed for quality care. Sustained investment in education, training and workforce retention, alongside strong regional collaboration, will be key to addressing these challenges and enhancing healthcare services in the Pacific.
Conflict of interest:
The authors have no conflicts of interest to declare.
Funding Statement:
The authors received no funding for the work discussed in the manuscript.
Acknowledgements:
This study was conducted in partnership between the Ministries of Health in 16 PICTs and the Pacific Community (SPC), with support from Australia’s Department of Foreign Affairs and Trade (DFAT).
References
- World Health Organization. Human Resources for Medical Devices: The Role of Biomedical Engineers. Geneva: WHO; 2017. Accessed September 2, 2023. https://iris.who.int/bitstream/handle/10665/255261/9789241565479-eng.pdf
- World Health Organization. Medical Device Donations: Considerations for Solicitation and Provision. 2nd ed. Geneva: WHO; 2011. Accessed September 5, 2023. https://www.who.int/publications/i/item/9789240093621
- Murtaza NM, Imtiyaz A, Seema C. Integration of healthcare system with its experts for improving the life expectancy of medical devices: a review. Int J Sci Res Sci Technol. 2016;2(2):223-231. Accessed January 23, 2025. https://ijsrst.com/paper/249.pdf
- World Health Organization, Organisation for Economic Co-operation and Development. Delivering Quality Health Services: A Global Imperative for Universal Health Coverage, 2018. Accessed April 6, 2025. https://iris.who.int/handle/10665/272465
- Malkin RA. Design of health care technologies for the developing world. Annu Rev Biomed Eng. 2007;9:567-587. doi:10.1146/annurev.bioeng.9.060906.151913
- World Health Organization. The Global Health Observatory: Biomedical engineers density (per 10,000 population). August 29, 2018. Accessed February 10, 2024. https://www.who.int/data/gho/data/indicators/indicator-details/GHO/biomedical-engineers-density-(per-10-000-population)
- Strengthening Specialised Clinical Services Program. Biomedical Situational Analysis Questionnaire. Revised Situational 2014. Noumea: SPC; 2014.
- World Health Organization. Health Workforce Requirements for Universal Health Coverage and the Sustainable Development Goals. Human Resources for Health Observer Series No. 17. Geneva: WHO; 2016. Accessed February 13, 2025. https://iris.who.int/handle/10665/250330
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030. Geneva: WHO; 2016. Accessed September 9, 2024. https://iris.who.int/bitstream/handle/10665/250368/9789241511131-eng.pdf
- Strengthening Specialised Clinical Services Program. Biomedical Meeting Report: 3rd Meeting/Workshop for Biomedical Technicians of the Pacific Region. Denarau, Fiji; 2014.
- L T, R P, W P. Biomedical engineering – a critical workforce in healthcare delivery: an Evidence Check rapid review brokered by the Sax Institute for the NSW Ministry of Health. Sax Institute. January 2020. Accessed February 10, 2025. https://www.saxinstitute.org.au/wp-content/uploads/20.06_Evidence-Check_Biomedical-engineering-a-critical-workforce-in-healthcare-delivery.pdf
- American Society for Engineering Education. Engineering & Engineering Technology by the Numbers 2023. ASEE; 2023. Accessed February 2, 2025. https://ira.asee.org/wp-content/uploads/2024/12/Engineering-Engineering-Technology-By-the-Numbers-2023-1-combined.pdf
- Statistics New Zealand. New Zealand Census 2018. Wellington: Stats NZ; 2018. Accessed February 10, 2025. https://www.stats.govt.nz/tools/aotearoa-data-explorer
- World Health Organization and the Pacific Community. Outcomes of the Fifth Health Ministers Meeting, WHO-SPC 2023, Tonga. Accessed April 7, 2025. WPR-2024-DPS-001-eng.pdf
- World Health Organization. 2015 Yanuca Island Declaration on Health in Pacific Island Countries and Territories. WHO; 2015. Accessed February 9, 2025. https://iris.who.int/bitstream/handle/10665/208257/PHMM_declaration_2015_eng.pdf
- Pacific Islands Forum. 2050 Strategy for the Blue Pacific Continent. Suva, Fiji: PIF Secretariat; 2022. Accessed February 9, 2025. https://forumsec.org/sites/default/files/2023-11/PIFS-2050-Strategy-Blue-Pacific-Continent-WEB-5Aug2022-1.pdf
- United Nations. Sustainable Development Goals. United Nations; 2015. Accessed January 18, 2025. https://www.un.org/sustainabledevelopment/health/