

Mechanical Thrombectomy in Severe Cerebral Venous Thrombosis
Rescuing the Sinuses: Successful Mechanical Thrombectomy in Severe Cerebral Venous Thrombosis
Dr. M. Rathish1*, Dr. Renuka M.K.2, Dr. BabySailaja K3
- Manimohan Rathish Senior Resident, Department of Critical Care Medicine, Sri Ramachandra Institute of Higher Education and Research, Tamil Nadu, India.
- M. K. Renuka Professor, Department of Critical Care Medicine, Sri Ramachandra Institute of Higher Education and Research, Tamil Nadu, India.
- K. Baby Sailaja Associate Professor, Department of Critical Care Medicine, Sri Ramachandra Institute of Higher Education and Research, Tamil Nadu, India.
OPEN ACCESS
PUBLISHED: 31 July 2025
Main Article ContentManimohan Rathish Senior Resident, Department of Critical Care Medicine, Sri Ramachandra Institute of Higher Education and Research, Tamil Nadu, India.
M. K. Renuka Professor, Department of Critical Care Medicine, Sri Ramachandra Institute of Higher Education and Research, Tamil Nadu, India.
K. BabySailaja Associate Professor, Department of Critical Care Medicine, Sri Ramachandra Institute of Higher Education and Research, Tamil Nadu, IndiaOPEN ACCESPUBLISHED: 31 July 2025
CITATION: Rathish, M., Renuka, M.K., BabySailaja, K., 2025. Rescuing the Sinuses: Successful Mechanical Thrombectomy in Severe Cerebral Venous Thrombosis. Medical Research Archives, [online] 13(7). https://doi.org/10.18103/mra.v13i7.6736
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI:https://doi.org/10.18103/mra.v13i7.6736
ISSN 2375-1924
ABSTRACT
Cerebral venous thrombosis (CVT) is a rare but potentially life-threatening condition, often presenting with nonspecific symptoms such as headache, seizures, or focal neurological deficits. While anticoagulation remains the cornerstone of treatment, mechanical thrombectomy is increasingly being utilized for severe cases, particularly those complicated by large clot burden or clinical deterioration. This case report discusses the presentation, diagnosis, and treatment of a patient with CVT who underwent mechanical thrombectomy, with post-procedural flow restoration but eventual fatal outcome, and reviews the relevant literature.
Keywords
Cerebral venous thrombosis, mechanical thrombectomy, anticoagulation, neurological deterioration, case report.
INTRODUCTION
CVT accounts for approximately 0.5% of all strokes and typically affects young to middle-aged adults. Risk factors include hypercoagulable states, infections, malignancy, and hormonal influences such as pregnancy. Although most patients respond well to anticoagulation, some require advanced interventions like thrombectomy due to worsening neurological status or failure of medical therapy.
Cerebral venous thrombosis (CVT) is a rare but serious neurovascular condition characterized by thrombosis of the dural venous sinuses and/or cerebral veins. It accounts for approximately 0.5% to 1% of all types of stroke, affecting predominantly young adults and women of childbearing age. The pathophysiology involves impaired venous drainage, resulting in increased intracranial pressure, cerebral edema, and possibly venous infarction or hemorrhage. Risk factors include inherited or acquired thrombophilia, infections, malignancy, hormonal factors (especially oral contraceptive use and pregnancy), systemic inflammatory disorders, and recent surgeries or trauma. Clinical presentation can be variable—ranging from isolated headache to seizures, focal neurological deficits, altered sensorium, or coma. Diagnosis typically involves magnetic resonance venography (MRV) or computed tomography venography (CTV) to confirm thrombosis. Management begins with anticoagulation, usually with low-molecular-weight or unfractionated heparin. However, in severe cases or in patients not responding to medical therapy, endovascular interventions like mechanical thrombectomy are considered. This case highlights the complexities and evolving role of thrombectomy in CVT management, emphasizing the importance of early intervention in extensive clot burden and deteriorating clinical status.
CASE PRESENTATION:
An 18-year-old male presented to the emergency department with a 4-day history of progressively worsening headache, nausea, and transient episodes of right-sided weakness. He had no significant medical history.
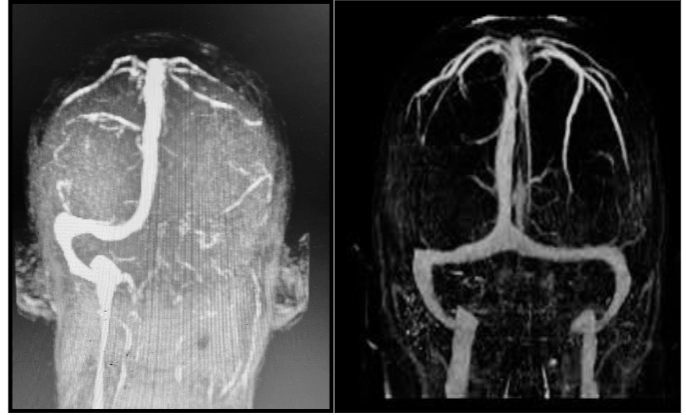
On admission, his Glasgow Coma Scale (GCS) score was 14. Neurological examination revealed mild right hemiparesis (4/5 strength). Initial blood work demonstrated elevated D-dimer levels. Non-contrast computed tomography (CT) of the head was unremarkable, but CT venography revealed extensive thrombosis of the superior sagittal sinus. Anticoagulation with intravenous heparin was initiated. Despite 48 hours of therapy, the patient experienced worsening neurological symptoms, including confusion and increased hemiparesis. Repeat imaging showed no significant recanalization and progression of clot burden. The decision was made to proceed with mechanical thrombectomy. Additional laboratory evaluations, including APLA (antiphospholipid antibody), ANA (antinuclear antibody) profiles, protein C, protein S, and homocysteine levels, were performed and were within normal limits.
Procedure:
Under general anaesthesia, a cerebral angiogram confirmed extensive thrombus in the superior sagittal sinus. Mechanical thrombectomy was performed using a combination of aspiration and stent retriever techniques. Complete recanalization was achieved with minimal residual thrombus. No immediate complications were noted.
Outcome:
Post-procedure, cerebral venous flow was successfully restored, and follow-up imaging confirmed patency of the venous sinuses. However, the patient’s neurological status did not improve. Over the subsequent 48 hours, he developed worsening cerebral oedema and herniation despite aggressive medical management. Unfortunately, the patient succumbed to his condition on day 4 post-thrombectomy.
DISCUSSION:
Mechanical thrombectomy for CVT is a promising but complex intervention, particularly in cases of extensive clot burden. While recanalization was successfully achieved in this case, the patient’s outcome highlights the challenges of managing severe CVT with secondary complications such as cerebral edema. This underscores the need for prompt diagnosis, careful patient selection, and aggressive peri-procedural management. Despite the fatal outcome, this case demonstrates the feasibility of thrombectomy in restoring venous flow in severe CVT.
Mechanical thrombectomy in cerebral venous thrombosis represents a promising but evolving therapeutic option for patients with poor response to anticoagulation or rapid neurological deterioration. The goal of endovascular treatment is to restore venous drainage, reduce intracranial pressure, and prevent further parenchymal damage. Although evidence remains limited to observational studies and case series, increasing reports suggest that thrombectomy can lead to rapid radiological and clinical improvement in selected patients. In this case, thrombectomy achieved successful recanalization, but the final outcome was unfavorable due to secondary complications like cerebral edema and herniation. This underscores the need for vigilant post-procedural management and patient selection. Several techniques are employed, including direct aspiration, stent retriever thrombectomy, or a combination of both. The decision is based on clot location, burden, and institutional expertise. Adverse events such as vessel injury, hemorrhage, or incomplete recanalization are concerns. Our patient demonstrated radiological improvement post-intervention but suffered delayed neurological worsening, highlighting that mechanical success does not guarantee clinical recovery. This case also raises questions about the timing of intervention—whether earlier thrombectomy might have averted progression. Furthermore, standardized protocols, randomized controlled trials, and registry-based data are needed to identify optimal treatment thresholds. Another consideration is the underlying cause of CVT, which may affect outcomes and recurrence risk. Our patient had no identifiable hypercoagulable state, but workup should always include screening for inherited and acquired thrombophilias. Advanced neuroimaging is essential to monitor response to therapy. Aggressive medical management, including osmotherapy and close neurocritical care, plays a vital role in minimizing secondary injury. The role of decompressive craniectomy in patients with impending herniation should also be considered when available. This report contributes to the growing evidence that mechanical thrombectomy, though complex and not devoid of risk, may benefit select patients with severe CVT. Collaboration between neurologists, intensivists, and interventional neuroradiologists is essential to maximize success. Future efforts should focus on multi-center trials to clarify indications, techniques, and long-term outcomes following thrombectomy in CVT.
CONCLUSION:
This case underscores the potential and limitations of mechanical thrombectomy in CVT management. Although the procedure restored venous flow, the patient’s outcome was determined by secondary complications. Further studies are needed to refine patient selection criteria and optimize post-procedural care to improve survival.
Conflict of Interest Statement:
None.
Funding Statement:
None.
Acknowledgements:
None.
References
1. Saposnik G, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/ American Stroke Association. Stroke. 2011;42(4): 1158-1192. doi:10.1161/STR.0b013e31820a8364
2. Coutinho JM, et al. Mechanical thrombectomy for cerebral venous thrombosis: a systematic review and meta-analysis. Stroke. 2014;45(4):1173-1179. doi:10.1161/STROKEAHA.113.004380
3. Ferro JM, et al. Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke. 2004;35(3):664-670. doi:10.1161/01.STR.0000117571.76197.26
4. Gupta R, et al. Endovascular management of cerebral venous thrombosis: current status and future directions. Interventional Neurology. 2016; 5(3-4):171-181. doi:10.1159/000447501
5. Yaghi S, et al. Cerebral venous thrombosis: a review of epidemiology, pathophysiology, and management. Frontiers in Neurology. 2020;11: 567799. doi:10.3389/fneur.2020.567799