





Medication-Related Osteonecrosis in Breast Cancer Patients
Medication-Related Osteonecrosis of the Jaw in Women with Breast Cancer: A Narrative Review
Alina Čebatariūnienė¹, Niyosha Rasekhi¹
- Institute of Odontology, Faculty of Medicine, Vilnius University, Vilnius, Lithuania
OPEN ACCESS
PUBLISHED: 31 December 2024
CITATION: Čebatariūnienė, A., and Rasekhi, N., 2024. Medication-Related Osteonecrosis of the Jaw in Women with Breast Cancer: A Narrative Review. Medical Research Archives, [online] 12(12).
https://doi.org/10.18103/mra.v12i2.6194
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i2.6194
ISSN 2375-1924
Abstract
Breast cancer remains a leading cause of premature death in women globally, spurring the adoption of comprehensive treatment approaches. Despite therapeutic progress, significant challenges persist for patients, especially those with advanced breast cancer prone to bone metastases. Bisphosphonates and Denosumab are key bone-modifying agents used to target bone metabolism, reduce metastatic risk, and enhance adjuvant therapy efficacy in early-stage breast cancer. However, using these agents carries risks, including adverse events such as osteonecrosis of the jaw. Due to the impact of these drugs on the jaw bone, this condition is now known as Medication-related osteonecrosis of the jaw (MRONJ). The aim is to provide a comprehensive investigation into MRONJ in the context of breast cancer treatment, with a specific focus on the effects of antiresorptive drugs such as Bisphosphonates and Denosumab. The objective of this article is to review clinical and radiographic manifestations, evaluate the pathophysiology, determine risk factors and incidence and provide guidelines to healthcare professionals for the management and treatment of MRONJ. Medication-related osteonecrosis of the jaw is a condition that occurs in breast cancer patients due to various risk factors. The treatment of MRONJ depends on the different stages of the condition. Recent research suggests that optimal management of patients prone to MRONJ necessitates a multidisciplinary approach, and the dentist is one of the team members who play a crucial role in patient care by assessing modifiable risk factors, establishing follow-up protocols, and maintaining open communication with oncologists. Preventive measures should be implemented before and during treatment with antiresorptive drugs. However, despite increased awareness, many doctors and dentists still have a limited understanding of MRONJ. Therefore, this research provides practical guidelines for preventing, managing, and treating MRONJ in breast cancer patients based on currently available literature. Dentists should follow specific protocols for patients undergoing antiresorptive therapy. The primary goals are to prevent MRONJ and maintain patients’ quality of life. Therefore, dental students and specialists must stay updated and consider this side effect.
Keywords
- Medication-related osteonecrosis of the jaw
- Breast cancer
- Bisphosphonates
- Denosumab
- Antiresorptive drugs
Introduction
Breast cancer is the primary cause of premature death among women in many countries worldwide. Multimodality treatment strategies have been advocated for the comprehensive management of breast cancer, aiming to address the disease from various angles. However, despite advancements in treatment options, many breast cancer patients continue to face significant challenges that pose threats to their lives. Advanced breast cancer often affects bones, resulting in bone metastases. The bone microenvironment plays a vital role in harbouring disseminated tumor cells and serves as a potential source of late relapse in breast cancer patients. Therefore, agents that affect bone metabolism might significantly reduce the risk of metastasis and adjuvant therapy in the early stage of the disease. Both bisphosphonates (BPs) and Denosumab (DNB) are bone-modifying agents (BMAs) because they directly affect bone structure and bone metabolism. Bone metabolism is a continuous process throughout one’s life. It involves the removal of mature bone tissue from the skeleton (bone resorption) and forming new bone tissue (ossification or new bone formation). Bisphosphonates and Denosumab are categorized as antiresorptive drugs (ARDs) because they primarily inhibit bone resorption, prevent bone loss, and reduce the risk of fractures. Despite different mechanisms of action and administration routes, both BPs and DNBs play crucial roles in the management of bone health in breast cancer patients and other conditions associated with bone loss.
Although agents such as BPs and other ARDs have been shown to complement cancer-specific treatments by improving bone structure and quality, thereby reducing the risk of skeletal morbidity, they have also been associated with an increased risk of adverse events such as atypical femur fracture, vertebral body compression fracture, and osteonecrosis of the jaw (ONJ). Among these adverse events, ONJ is the most harmful one that can seriously affect patients’ quality of life. It was first reported in association with BPs in 2003 and has been called bisphosphonate-related osteonecrosis of the jaws (BRONJ). This definition has undergone several alterations, and after marketing new ARDs such as DNB, this complication changed its name from BRONJ to medications-related osteonecrosis of the jaws (MRONJ). Oncological patients are much more at risk of developing MRONJ, and it tends to be observed more frequently in jaw bones because of their higher rate of remodelling capacity, as well as infectious agents in the oral cavity that can quickly spread to the jaw bone.
Since 2003, works of literature have been warning about the increased number of MRONJ cases, and there is currently an increasing interest in MRONJ. It is widely discussed in the scientific community, and dentists from different specialities and postgraduate and undergraduate dental students must improve and update their knowledge about patients who are at risk of developing MRONJ, such as breast cancer patients. However, despite this attention, doctors and dentists still need a better understanding of the subject or do not follow the appropriate guidelines for patients, and little progress has been made toward knowledge diffusion, education, and improvement of dental practices. Geographical regions or economic conditions are not significant factors influencing professional awareness, indicating the necessity for universal educational initiatives. Addressing the existing gaps in our understanding of MRONJ is imperative for optimizing the care and outcomes of breast cancer patients. By enhancing our knowledge of the risk factors, pathophysiology, clinical manifestations, incidence, and management strategies and treatment of MRONJ, healthcare professionals, particularly dentists, can better anticipate, prevent, and mitigate this debilitating complication. Moreover, bridging the divide between research findings and clinical practice is essential for ensuring timely and effective interventions, improving patient outcomes and enhancing the overall quality of breast cancer care.
1 Breast Cancer
Breast cancer primarily affects women and occurs when cells in the breast start growing abnormally, often beginning in the milk ducts or lobules. Various factors can increase the risk of breast cancer, such as late age for marriage and childbirth, as well as late menopause, leading to prolonged exposure to estrogen. Breast cancer can be classified based on histological types, with the most common being infiltrating duct carcinoma non-specific type (IDC-NST) and molecular characteristics based on hormonal receptors, which are essential for determining treatment options. Breast cancer is categorized into four stages based on tumor size, lymph node involvement, metastasis, and biological markers. Diagnostic methods based on imaging and molecular biotechnology have been developed for quick and accurate breast cancer screening. Breast cancer treatment aims to reduce symptoms, prolong life, and maintain quality of life. Treatment approaches, such as endocrine therapy, chemotherapy, and immunotherapy, are tailored to the specific cancer subtype. Surgical interventions or radiation may be recommended after systemic therapy to alleviate the impact of tumor burden on the patient’s quality of life. Additionally, antiresorptive therapy, such as DNB or BPs, is used as an additional treatment method.
Treatment in Early-Stage
The presence of disseminated tumour cells in the bone marrow of around 25% of patients with early-stage breast cancer is associated with an increased risk of recurrence. Recent studies suggest using selective bone-modifying agents (BMAs) as adjuvant therapy for postmenopausal women with early-stage breast cancer. Additionally, non-metastasis breast cancer patients undergoing hormonal therapy are often prescribed low doses of BMAs for the prevention and treatment of cancer treatment-induced bone loss (CTIBL). Despite these recommendations, the findings across studies have not been consistent, and there is no unanimous endorsement for universal adjuvant therapy with BMAs. Joint guidelines from Cancer Care Ontario (CCO) and the American Society of Clinical Oncology (ASCO) recommend zoledronic acid every six months for 3–to 5 years in postmenopausal women on adjuvant BP therapy. A study conducted by Michael Gnant shows a 50% reduction in fractures with DNB 60 mg every six months for three years in early-stage breast cancer patients on aromatase inhibitors. Another study by Robert Coleman’s research highlights DNB’s impact on breast cancer outcomes rather than bone health.
In contrast, another study by Mauceri suggests that low-dose BMAs for CTIBL prevention pose a similar MRONJ risk as osteoporosis. Clinicians, especially dentists, may not fully understand the increasing risk of MRONJ in these patients in the early stage. It can lead to overestimating or underestimating the risks and necessary preventive measures. Therefore, early-stage breast cancer patients on BMAs should undergo regular monitoring for MRONJ prevention, as they may transition to higher BMA doses in the future, increasing their risk.
Treatment in Metastasis Stage
Metastatic breast cancer can lead to skeletal-related events (SREs) in up to 80% of patients, primarily due to increased RANKL expression, which stimulates osteoclast activity and causes bone resorption. This results in complications like fractures, hypercalcemia, spinal cord compression, and pain, so bone-targeted treatments are essential. Adding BPs to standard care can reduce SRE risk by 15%, delay their occurrence, and improve bone pain. Intravenous Zoledronic acid (4mg every 3-4 weeks) is particularly effective and safe for rapid administration. Subcutaneous DNB, administered at 120 mg every four weeks, inhibits osteoclast activity and delays SRE onset compared to Zoledronic acid. The American Society of Clinical Oncology (ASCO) recommends continuing these treatments until significant declines in patient performance status. At the same time, the European Society for Medical Oncology suggests indefinite treatment under normal conditions. Current international guidelines do not favour DNB over BPs.
2 Antiresorptive Drugs
Antiresorptive drugs are crucial in preventing SERs and complications in breast cancer patients. The most commonly used ARDs are BPs and DNB. While more potent agents like zoledronic acid and DNB are effective, they carry a heightened risk of MRONJ. BPs can be taken orally or via injection to reduce cancer-related bone loss. The American Society of Clinical Oncology recommends zoledronic acid at 4 mg every 3-4 weeks for bone metastases and every six months for early-stage disease. DNB is an antiresorptive agent that exists as a fully humanized antibody against receptor activator of nuclear factor kappa-B ligand (RANKL) and inhibits osteoclast function and associated bone resorption. While BPs have been used for many years, in November 2010, the Food and Drug Administration (FDA) approved DNB (XGEVA) as a subcutaneous injection for patients with bone metastases from solid tumors. The recommended dose is 120mg every four months. Additionally, DNB (Prolia) is approved in doses of 60mg every six months for patients at high risk of fracture receiving adjuvant aromatase inhibitors or hormonal therapy for breast cancer. It has also shown direct or indirect anti-tumour effects in preclinical models and clinical applications.
Drug Effects
Bisphosphonates can help to increase bone mineral density (BMD) over time. This effect usually levels off after about 3-4 years of treatment, but it can help to prevent bone loss and reduce the risk of fractures. Out of all the BPs, zoledronic acid is especially effective in reducing the risk of adverse skeletal events, including bone loss, in women with breast cancer. In addition to these benefits, BPs can also help to relieve bone pain. This effect can benefit people with rare bone diseases like fibrous dysplasia, bone cancer, and bone metastasis. BMD responses to DNB follow a pattern similar to the BPs, although the increases are more significant and continue through 10 years. BP treatment is generally well tolerated, with benefits outweighing side effects, though issues like hypocalcemia, renal toxicity, gastrointestinal symptoms, atypical bone fractures, and ONJ can occur.
Osteonecrosis of the jaw was initially noticed in patients with disseminated malignancy undergoing monthly BP infusions to prevent skeletal-related events (SREs) and is more familiar with higher doses, prolonged treatment, or shorter intervals in metastatic disease. With newer antiresorptive drugs like DNB, distinct from BPs, this complication has shifted from BRONJ to MRONJ, indicating bone exposure in the maxillofacial and intraoral areas with delayed healing. However, it has been observed that patients with cancer who receive monthly DNB have a similar frequency as BPs. ONJ is more common in the jaw due to high bone turnover, frequent dental trauma, and vulnerability to infections, with the mandible showing a higher incidence (73%) compared to the maxilla (22.5%). Its thinner mucosa and single blood supply for the mandible increase susceptibility to necrosis and infections.
3 Medication-Related Osteonecrosis of the Jaw (MRONJ): Diagnosis and Stages
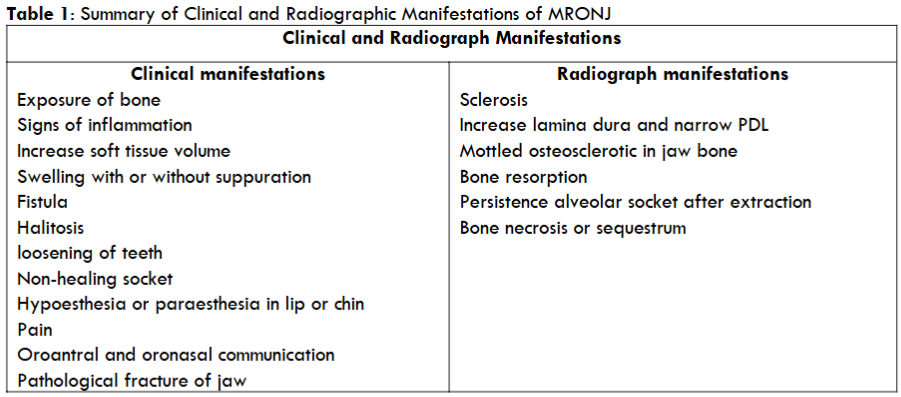
Medication-related osteonecrosis of the jaw is defined as a harmful drug reaction characterized by the gradual decay and demise of bone tissues in the mandible and maxilla of patients exposed to the treatment with medications known to increase the risk of disease in the absence of previous radiation treatment. The American Association of Oral and Maxillofacial Surgeons (AAOMS) has established specific criteria to diagnose MRONJ, which healthcare professionals commonly use and one of those criteria is bone exposure or an intraoral or extraoral fistula in the maxillofacial region through which the bone can be probed and is present for more than eight weeks; however, during the European task force on MRONJ workshop held in 2019, it was proposed that an eight-week observation period should not be a requirement to establish the diagnosis of MRONJ. So, in general, the diagnosis is based on clinical examination and radiographic findings, which help to determine the extent of necrosis and the presence of a sequestrum.
The AAOMS has proposed a classification system for MRONJ with four stages based on clinical features. The initial stage includes a group “at risk,” encompassing those who have received antiresorptive medication. Management involves close multidisciplinary observation and good oral hygiene.
Stage 0: Patients in this stage may not show any signs of necrotic bone but may experience non-specific symptoms such as dull pain in the mandible, sinus pain, unexplained tooth mobility, odontalgia without any visible cause, and gingival swelling. Other symptoms may include unexplained resorption of alveolar bone and changes in bone pattern.
Stage 1: Patients in this stage are asymptomatic, with exposed necrotic bone but no signs of infection.
Stage 2: Patients in this stage exhibit the presence of symptomatic necrotic bone and may experience pain, erythema, infection with or without purulent drainage.
Stage 3: This stage is quite severe and is characterized by severe necrosis, including symptoms like pathologic fracture, extra-oral fistula, osteolysis that extends beyond the region of alveolar bone, for example, inferior border and ramus in the mandible, and sinus floor or zygoma in the maxilla. In addition to these symptoms, this stage may include oroantral or oronasal communication, which can further complicate the condition.
Pathophysiology
The exact cause of MRONJ is not fully understood and is believed to involve multiple factors. One theory proposes that the condition may arise from the inhibition of bone remodelling or alteration of bone turnover within the jaw, which could delay and impair bone healing. Specifically, DNB has been found to reduce bone turnover more than zoledronic acid. Another hypothesis suggests that the inhibition of angiogenesis may contribute to MRONJ. It is supported by studies indicating that MRONJ is typically characterised by avascular or aseptic necrosis. BPs such as zoledronic acid can directly inhibit angiogenesis both in vitro and in vivo, and they may also indirectly block blood vessel formation by targeting macrophages, which produce matrix metalloproteinase (MMP9). Additionally, BPs and DMB decrease the arterial and venous areas and the overall vascularity of periodontal tissues during MRONJ. Inflammation and infection are crucial in the onset of osteonecrosis. Dental procedures like tooth extractions and implant placements can introduce bacteria into the bloodstream, leading to systemic inflammation. Periodontal disease can also contribute by causing temporary bacteraemia and subsequent inflammation. Bacterial lipopolysaccharides increase cytokine production and regulate RANKL, altering bone matrix through increased osteoclast activity. It disrupts regular bone maintenance, acidifying the bone environment and affecting turnover. Additionally, low pH levels from infections can release BPs from bone, inhibiting osteoclast activity and affecting nearby cells like osteoblasts and lymphocytes, contributing to MRONJ. Studies on mice with rheumatoid arthritis showed a link between systemic inflammation and more severe MRONJ. Patients with immune dysfunctions like rheumatoid arthritis, diabetes, or cancer are at higher MRONJ risk, even without antiresorptive agents. This can be confirmed by animal studies that have shown that certain medications, such as chemotherapy, steroids, disease-modifying antirheumatic drugs (DMARDs), and antiangiogenic medications when combined with antiresorptive agents, can increase the severity or prevalence of MRONJ. Several reports have identified single-nucleotide polymorphisms (SNPs) linked to genes involved in collagen formation, bone turnover, and metabolic bone diseases that may be associated with MRONJ. Sirtuin-1(SIRT1), which promotes bone formation and reduces inflammation, could offer protection against MRONJ. Other implicated genes which increase the risk of MRONJ include those related to angiogenesis and immune responses like PPAR gamma, CYP2C8 and others. Despite these findings, current research shows a weak connection between genetic factors and MRONJ risk, highlighting the need for larger, diverse studies to understand genetic predisposition better.
Risk Factors and Incidence
Medication-related osteonecrosis of the jaw is associated with several risk factors in breast cancer patients. Understanding these factors is crucial for both prevention and early intervention. Here are key MRONJ risk factors.
Drug-Related Risk Factors
The primary drug-related risk for MRONJ is exposure to DNB or BPs, with increased risk from other cancer therapies like angiogenesis inhibitors, chemotherapy, hormonal therapy, cyclophosphamide, and corticosteroids. These drugs can cause immunosuppression, increasing local inflammation and MRONJ risk. The likelihood of MRONJ rises with higher doses, longer durations, and intravenous or subcutaneous administration routes, especially in metastatic cases. And at the end, breast cancer as an underlying disease also elevates MRONJ risk.
Systemic Risk Factors
Systemic risk factors affect bone and drug metabolism, oral health, and systemic diseases. Khan et al. found that some systemic risk factors for MRONJ for cancer patients include diabetes, erythropoietin usage, smoking, hyperthyroidism, and renal disease. These factors require special attention due to their influence on bone and mucosal microcirculation. It should be considered that genetics and age can also affect the risk of MRONJ. Specific biomarkers may indicate MRONJ risk. The American Society of Bone Mineral Research suggests a threshold of carboxy-terminal cross-linking telopeptide of type I collagen (CTX) levels (> 0.150 ng/mL) for safer invasive dental procedures in patients on BPs. However, low CTX levels (< 0.150 ng/mL) could pose risks. A study by Ana Laura Soares found higher (procollagen type 1 amino-terminal propeptide) P1NP levels in patients with bone metastasis, indicating P1NP might be a better marker for metastatic bone disease and MRONJ. However, the potential use of these markers for invasive dental procedure selection in breast cancer patients remains to be determined, and more research needs to be done.
Local Risk Factors
It is essential to consider any condition that can cause inflammation or infection in the dental supporting structures as a local risk factor. Specialists must promptly recognise and treat these factors to ensure the safe initiation of medical therapy. Some factors include anatomic features such as bone exostoses and mandibular and palatal torus. Dentists should also pay attention to subclinical trauma. The elevated risk of MRONJ can be associated with periodontal disease and apical periodontitis, underscoring the role of inflammation in its pathogenesis. Denture-associated sore spots may cause permanent mucosal inflammation and make micro lesions, which facilitate the penetration of bacteria into the bone and increase susceptibility to infection and MRONJ. Dentoalveolar operations such as tooth extraction are a common predisposing factor for MRONJ. Studies show tooth extraction is cited as a predisposing event in 62% to 82% of MRONJ cases. Also, studies estimate the risk of MRONJ after tooth extraction in cancer patients exposed to IV BPs is estimated to be between 1.6% and 14.8%. Some studies suggest that tooth extraction is a significant risk factor for developing MRONJ in cancer patients receiving antiresorptive drugs. For example, in a longitudinal cohort study, Vahtsevanos et al. found that 60 out of 1621 (4.9%) patients with breast cancer, prostate cancer, or multiple myeloma treated with BPs developed MRONJ. Furthermore, tooth extraction was linked to a 33-fold increased risk of MRONJ, consistent with similar studies identifying it as a risk factor.
In contrast, others indicate that tooth extraction does not significantly influence the risk of MRONJ, instead highlighting inflammation and dental infections as the primary concerns. A non-randomised retrospective cohort study by Avishai found that tooth extraction contributes to the development of MRONJ in nearly 20% of cases. Still, inflammation or infection is the primary cause in 95% of MRONJ cases. Also, a retrospective observational study by Soutome et al. revealed that tooth extraction itself is not a risk factor for MRONJ in cancer patients on high-dose drugs; however, preserving infected teeth that require extraction increases the risk. Therefore, if local inflammation/infection is treated before extraction, MRONJ may be avoided. Studies suggest dental implants may increase the risk of MRONJ in patients treated with BPs or DNB for two reasons. First, peri-implantitis (inflammation around implants placed before antiresorptive therapy) can lead to MRONJ. Second, MRONJ is related to the insertion of implants in patients during or after taking antiresorptive medication. Moreover, the duration between implant insertion and MRONJ onset was significantly shorter in patients with cancer compared to those with osteoporosis. It is still unclear which of these two factors is more associated with the risk of MRONJ. In general, based on the works of literature, three main groups of patients are at risk of developing MRONJ: first, breast cancer patients with bone metastases receiving high doses of BMAs; second, early-stage breast cancer patients at risk of non-metastatic bone fractures due to CTIBL; and third, patients with osteoporosis or other non-malignant diseases on low-dose BMAs regimens.
Medication-Related Osteonecrosis of the Jaw Incidence in Breast Cancer
There have been several studies on the incidence of MRONJ in oncology, which refers to the number of new cases per sample or population per unit of time. However, there are limitations in studies focused on the incidence of MRONJ in breast cancer patients. Fredrik Hallmer’s study found that the incidence rate of MRONJ in metastasis breast cancer patients in the total population is 6.6%, while the incidence rate of MRONJ with zoledronic acid is 4.1%. It is to the report by Bamias et al., who found an incidence rate of 2.9% of MRONJ in patients with breast cancer treated with BPs. The incidence rate in the total population is higher than in the BP population because the risk of MRONJ from constipation DNB is three times higher than that of zoledronic acid. Recent randomised controlled trials on breast cancer patients without bone metastasis under a low dose of BMAs for CTIBL prevention reported MRONJ rates between 0% and 0.5%. Further investigation is needed to clarify the risk in these cases.
Prevention Strategy
It is essential to evaluate a patient’s MRONJ risk group, along with any additional risk factors that may be present, and then create an individualised treatment plan. A recent study involving 129 dental practitioners in the UK revealed a notable gap in knowledge, with over 90% exhibiting poor awareness of medications associated with MRONJ. Furthermore, only 40% expressed comfort in treating patients with antiresorptive-related MRONJ. Therefore, educating healthcare professionals and patients about the risk of MRONJ following certain medications is crucial for prevention. Furthermore, recent research suggests optimal management of patients prone to MRONJ necessitates a multidisciplinary approach. In light of these findings, a collaborative effort involving dentists, OMFSs, primary care physicians (family doctors), and oncologists, alongside active patient participation and oncology nurses, is essential to achieve optimal outcomes for individuals affected by MRONJ.
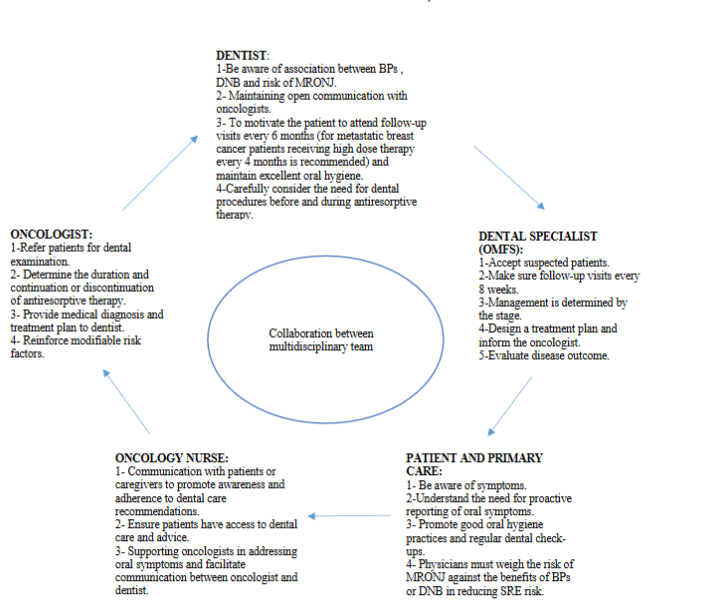
Additionally, developing and implementing educational programs become imperative to enhance interdisciplinary collaboration and deepen healthcare professionals’ understanding of bone-modifying agents’ benefits and potential side effects across dental and medical specialities. Due to limited studies on MRONJ in women with breast cancer, all healthcare professionals must pay special attention to those who are using or planning to use antiresorptive drugs. Mitigating potential risks and ensuring comprehensive care is necessary.
Clinical Practice Guidelines for Dental Treatment According to Timing. Preventive Measures
In the context of MRONJ prevention, it is essential to note that there was no standard and comprehensive protocol. The literature presents various protocols, from antibiotic regimens to autologous platelet concentrates and innovative approaches such as laser therapy. However, due to the need for a complete protocol, this study aimed to create a comprehensive guide for healthcare professionals, especially dentists. The guide addresses dental care for women with breast cancer or those starting anti-resorptive medications. The protocol also aims to instruct on what and how dental treatments should be performed when breast cancer patients are under these medications. The goal of the prevention of MRONJ is to eliminate dental risk factors and maintain a healthy oral environment. Patients are divided into two groups based on their history with ARDs. The first group, the pretreatment phase, includes patients who have never taken ARDs and are scheduled to start antiresorptive treatment. Their oral health must be assessed precisely through clinical and radiographic examinations, particularly for cancer patients. The second group, the in-treatment phase, consists of patients already exposed to ARDs. These patients will participate in an oral health assessment program to minimise local risk factors for MRONJ. To gain a better understanding of this topic, all recommendations are listed in the following tables.
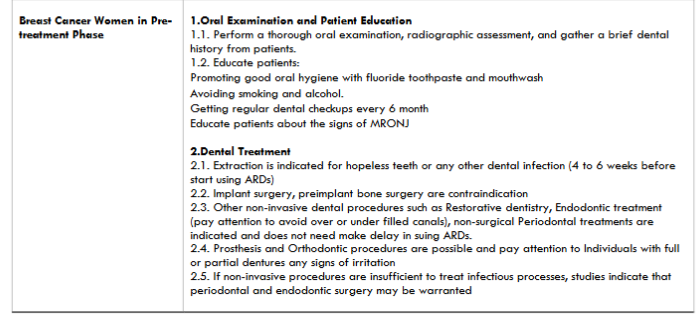
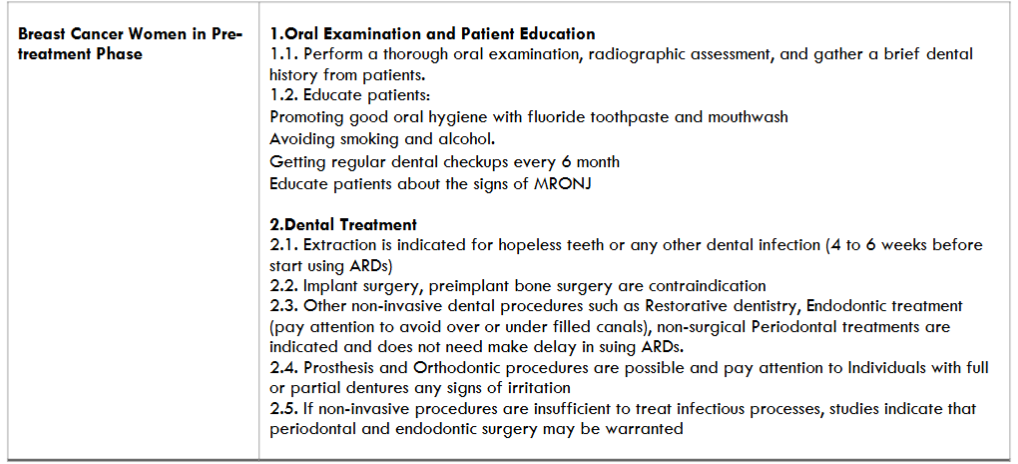
Cancer Patients in the Pre-Treatment Phase
Preventing MRONJ requires a multidisciplinary approach and active patient involvement. Healthcare professionals should educate cancer patients treated with DNB or BP about MRONJ risks. Patients must maintain good oral hygiene with fluoride products, avoid smoking and alcohol, and attend regular dental checkups. They should also be aware of MRONJ symptoms like exposed bone, jaw pain, loose teeth, pus, and non-healing sores for early detection and management.
Dental Treatments in the Pre-Treatment Phase
In the pretreatment phase, non-restorable teeth and those with poor prognosis should be extracted, along with any necessary elective dentoalveolar surgery. Antibiotics and antimicrobial rinses are recommended pre- and post-operatively. In cancer patients with hopeless teeth or any other dental infection, if systemic conditions permit, initial antiresorptive therapy should be delayed for 45-60 days after dental surgeries to allow soft tissue healing before starting the medications. In another study, Singh concluded that when a pretreatment extraction is completed, the tooth should be removed traumatically, and osseous healing should be complete, usually requiring 4 to 6 weeks before antiresorptive medication is started. This study emphasises the importance of avoiding tooth extractions in patients undergoing high-dose drug therapy for cancer. Invasive procedures like implants or bone surgery are contraindicated due to their potential risk of MRONJ. However, non-invasive dental procedures such as restorative dentistry and endodontic treatment can proceed without delaying antiresorptive therapy.
Medical oncologists play a crucial role in educating patients about the importance of dental health and preventive measures to reduce the risk of MRONJ. They should check for exposed bone during chemotherapy while assessing oral mucositis. Dentists must perform oral examinations, radiographic assessments, and review dental histories for local infections before starting antiresorptive therapy. Necessary treatments like endodontics, dental cleanings, and restorative and non-surgical periodontal procedures should be done to remove infection sources. Poorly performed root canals can increase MRONJ risk, so evaluating the tooth and clinician’s skill is vital. Other considerations, such as denture wearers, should also be checked for irritation or trauma, particularly from ill-fitting dentures, as these can lead to mucosal injury and infection. These assessments should be integrated into the treatment plan to minimise MRONJ risks.
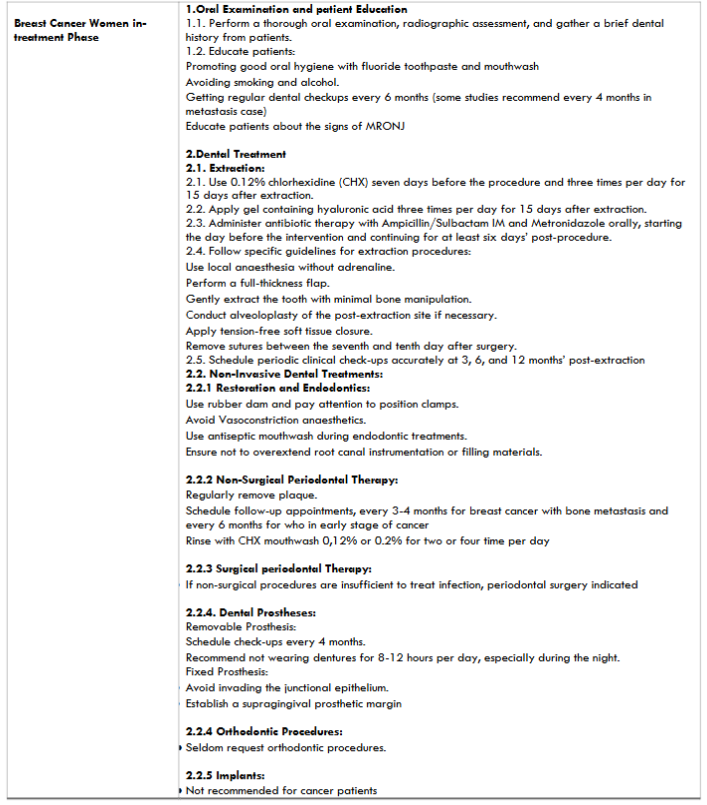
Cancer Patients in the Treatment Phase
Cancer patients treated with drugs related to MRONJ are considered at high risk of developing MRONJ due to the presence of multiple known risk factors. Teeth extractions or procedures that impact the bone are considered risk factors for developing MRONJ in patients. Literature reports that following a tooth extraction, there is a 2.9% incidence of MRONJ in cancer patients and 0.15% in osteoporosis patients. However, surgical procedures are considered necessary to eliminate infective outbreaks of MRONJ in cancer patients during the treatment when dental diseases cannot be resolved through other means. Spontaneous development of MRONJ without any invasive dental treatment has also been reported.
Dental Treatments in the Treatment Phase
Atraumatic surgical procedures (extraction): The Italian Society of Oral and Maxillofacial Surgery and the Italian Society of Oral Pathology and Medicine advocates a protocol for dental extractions in at-risk cancer patients. This protocol includes a combination of medical prophylaxis and specific surgical procedures; a standardized example of this protocol entails the following steps:
Pre and post-procedure Medical Prophylaxis: Patients are instructed to use a 0.12% chlorhexidine (CHX) antiseptic mouthwash at home thrice daily, starting seven days before the dental procedure. Postoperatively, they should continue using CHX mouthwash thrice daily for 15 days. Patients are also advised to apply a hyaluronic acid gel thrice daily for 15 days.
Antibiotic Therapy Administration: Concurrently, antibiotic therapy (e.g., Ampicillin/ Sulbactam intramuscular and Metronidazole orally) is administered, starting the day before the intervention and continuing for at least six days post-procedure.
Surgical Procedure Guidelines: During the surgical extraction, specific recommendations include the use of local anaesthesia without adrenaline, performing a full-thickness flap, gently extracting the tooth with less bone manipulation, conducting alveoloplasty of the post-extraction site, if necessary, and applying a tension-free soft tissue closure. These measures aim to facilitate healing through first intention. It is also advisable to proceed with one tooth extraction at a time, especially when multiple extractions are necessary. Sutures should be removed between the seventh and tenth day after surgery and during the first year of follow-up; it is essential to have periodic clinical checkups scheduled accurately at 3, 6, and 12 months. If the extraction socket has not healed after eight weeks, MRONJ should be suspected. Recent advancements in surgical techniques have introduced autologous platelet concentrates (APCs) and lasers for MRONJ presentation. In clinical studies, both Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) have demonstrated effectiveness in reducing the onset of MRONJ and expediting epithelisation, particularly in patients undergoing BPs therapy. PRP, rich in growth factors, and PRF, a second-generation autologous product, play pivotal roles in modulating inflammation and enhancing immune responses mediated by chemotactic molecules. The evidence suggests that PRF may intervene with bisphosphonate-induced effects on osteoclasts and mucosal cells. Also, the high level of leukocyte content serves to combat emerging infections in sites with challenging healing processes. It appears to be a favourable material in oral surgery; Plasma Rich in Growth Factor (PRGF) is another APC that contains various growth factors and shows the potential to induce mitosis of target cells, leading to favourable outcomes. Clinical observations reveal that adjunctive therapy with leukocyte–PRF (L-PRF) during tooth extraction in oncologic patients reduces MRONJ incidence. For those reasons, it should be considered a dentist-friendly material in oral surgery where patients show a high risk of developing complications that can lead to infections. In patients with a BP history, laser use after dentoalveolar surgery showed no signs of MRONJ after six months post-surgery. The combination of L-PRF and laser in patients cured with BPs showed physiological wound healing after one month, and none experienced MRONJ.
The clinician must adhere to consistent guidelines when dealing with inflammatory-infective issues that can be resolved through endodontic or periodontal surgical procedures. It includes applying the same protocols relevant to dental extractions. The guidelines should cover critical aspects such as medical prophylaxis and surgical procedure guidelines.
Non-Invasive Dental Treatments
To prevent the spread of infectious processes, it is highly recommended that non-invasive dental treatments like restoration and root canal treatment be undertaken. During those treatments, the dentist should always work with rubber dam isolation and avoid trauma to oral mucosa due to wrong-position clamps. It is recommended not to use Vasoconstriction anaesthetics and to provide antiseptic mouthwash to reduce the bacterial load in the oral cavity during endodontic treatments, as well as to avoid exceeding the limits of the root canal with endodontic instruments and root canal filling material.
Non-Surgical Periodontal Therapy
Recent studies suggest that cancer patients who are at risk of MRONJ should receive professional oral hygiene and is indicated. Non-surgical periodontal therapy that is non-invasive should be carried out cautiously to ensure regular plaque removal. It is also important to periodically screen patients undergoing treatment to monitor their oral and periodontal health. As a result, it is essential to schedule a follow-up period of 3-4 months for patients undergoing high doses of treatment with ARDs and every six months for those who have early-stage breast cancer for CTIBL prevention. For the management, it is recommended to use chlorhexidine rinses with concentrations between 0.12% and 0.2% and administered 2 to 4 times a day, depending on the severity. Educating individuals on proper home oral hygiene practices is also essential, as it should cover both the oral cavity and dentures. These measures can help reduce the risk of periodontal infection.
Dental Implants
It is a contraindication and is not recommended for in-treatment cancer patients to get dental implants due to the extensive bone manipulation that is required for placing the implant fixtures. Additionally, cancer patients’ systemic health conditions can increase the risk of developing peri-implantitis, which is also a significant risk factor for MRONJ.
Dental Prostheses
Cancer patients with removable dental prostheses should have checkups every four months. These checkups aim to assess denture fit, prevent pressure ulcers, and enhance stability. Patients should avoid wearing dentures for about 8–12 hours daily, especially at night. For fixed prostheses like crowns and bridges, it is crucial to consider the biological width and avoid infringing on the junctional epithelium. Supragingival prosthetic margins should be established to minimise trauma to the surrounding soft tissues and support periodontal health.
Considerations for Orthodontics
Orthodontic treatment is viewed as an elective option. While concerns exist about potential drug accumulation in the jawbone, cancer patients undergoing ONJ-related drug treatment seldom request orthodontic procedures.
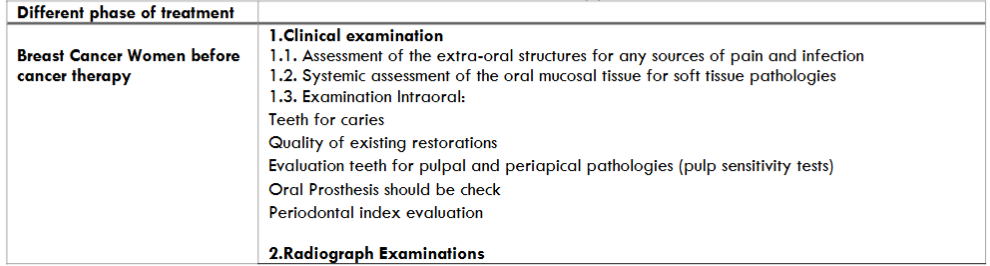
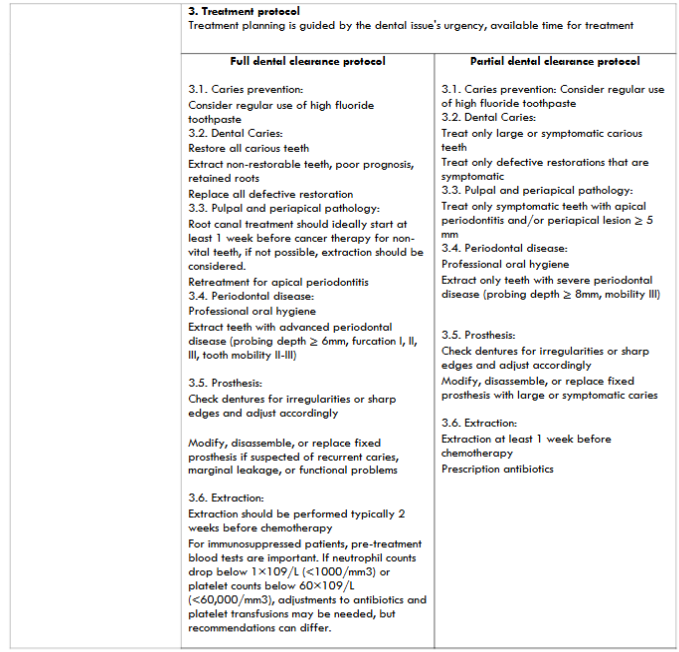
Table 2: The instructions for Breast Cancer Women before cancer therapy.
Treatment
The main goals of treating patients who are at risk of developing or have established MRONJ are to prevent MRONJ and preserve the quality of life, and this can be achieved through patient education and comforting, infections and pain control, as well as preventing the spread of the lesion and the development of new areas of necrosis. Additionally, for oncology patients, it is essential to prioritise and support continued oncologic treatment for those receiving antiresorptive therapy to control bone pain and reduce the incidence of SREs. The therapy of MRONJ is based on disease stage and can be either conservative (non-operative) or surgical, and decisions regarding surgical versus non-operative treatment should be personalized to each patient and adapted to their unique requirements. Evaluating the risk-to-benefit ratio is crucial in this process.
The effectiveness of conservative therapies in managing MRONJ is discussed in many kinds of literature. This treatment method is based on the use of drugs to control symptoms such as pain and infection. Infections are common complications of MRONJ and can contribute to its development. Therefore, non-operative treatment is mainly recommended, particularly in the early stage of MRONJ. However, according to the AAOMS classification update 2022, it can be helpful in all stages. Conservative therapy includes systemic antibiotic therapy in combination with antimicrobial therapy and oral hygiene. Sometimes, the removal of movable bony sequestrum segments and the extraction of symptomatic teeth from the exposed necrotic bone are also part of the treatment. The main goal of these treatments is the stabilisation of lesions. In the past, guidelines for managing MRONJ discouraged surgical intervention due to inconsistent evidence of favourable results in cancer patients. However, as experience has grown over the years, more evidence has emerged to support the use of surgery in treating MRONJ for patients who have not responded to conservative treatment or are not suitable for them. Surgery procedures can be used even in earlier stages of MRONJ.
Additionally, the necrotic bone removed during surgery should be sent for histopathological processing, as it may uncover metastases in the jaw specimen. However, this occurs in only a minority of cases. Surgical procedures for MRONJ include debridement, sequestrectomy, segmental and marginal resection. However, Davide De Cicco’s study states that debridement and sequestrectomy procedures should not be considered surgical interventions but rather conservative therapies. Surgical interventions are primarily categorised based on the extent of necrotic bone resection. However, other studies categorise those procedures as surgical interventions. Antibiotics are commonly prescribed before and after surgery, and perioperative antibiotic treatment should be administered to help prevent infection. There are also several additional possible treatments for MRONJ, including ozone therapy, laser therapy, growth factors combined with antibiotics, and vitamin D supplements for patients with vitamin D deficiency.
4 Enhancing Annotation Sheet Recommendations
Incomplete prescribing information about BPs and DNB, written in the annotation sheet by the FDA, it was mentioned that “cancer patients should maintain good oral hygiene and should have a dental examination with preventive dentistry before treatment with BPs.” Or “A dental examination with appropriate preventive dentistry should be considered before treatment with DNB in patients with risk factors of CONJ such as invasive dental procedures and diagnosis of cancer”³². Using words such as “should” in the annotation sheet of DNB and BPs related to the treatment of breast cancer are non-committal words. According to clinical guidelines in the pretreatment phase expressed by Sven Otto⁴⁰, they are inappropriate. Nita Singh⁴⁸ strongly recommends that physicians conduct oral examinations and take a brief dental history. It is most important to educate the patients about the risk of MRONJ and discuss the importance of oral hygiene and dental treatments. The word “essential” indicates that this particular action is fundamental and necessary and cannot be omitted without compromising the desired outcome or objective; however, using a word such as “should” conveys the sense to the reader that this is a recommendation or preferred under the circumstances and is not imply absolute necessity or obligation and there may be some flexibility or discretion in adhering to it. So, stronger terms like “must” are recommended to emphasise the critical role of dental care in preventing MRONJ and minimising the adverse effects of these medications.
Conclusion
Medication-related osteonecrosis of the jaw is a serious condition that can affect women with breast cancer, presenting through various stages that range from asymptomatic to severe bone exposure and pathological fractures. Its pathophysiology remains poorly understood but may involve factors such as inhibited bone remodelling, inflammation, immune dysfunction, and genetic predisposition. Additionally, systemic and local risk factors, including invasive dental procedures, anatomical issues, and periodontal disease, contribute to the disease’s development and severity. The incidence of MRONJ varies with different antiresorptive medications, showing higher rates associated with Denosumab compared to Zoledronic acid. Therefore, it is crucial for both dental students and specialists to stay informed about MRONJ, especially regarding its implications for patients with early-stage and metastatic breast cancer. Adhering to established management guidelines is essential for providing appropriate care to those affected by this condition.
References
1. Slepicka PF, Cyrill SL, dos Santos CO. Pregnancy and Breast Cancer: Pathways to Understand Risk and Prevention. Trends Mol Med. 2019;25(10):866-881. doi:10.1016/j.molmed.2019.06.003
2. Van Acker HH, Anguille S, Willemen Y, Smits EL, Van Tendeloo VF. Bisphosphonates for cancer treatment: Mechanisms of action and lessons from clinical trials. Pharmacol Ther. 2016;158:24-40. doi:10.1016/j.pharmthera.2015.11.008
3. Hallmer F, Bjarnadottir O, Götrick B, Malmström P, Andersson G. Incidence of and risk factors for medication-related osteonecrosis of the jaw in women with breast cancer with bone metastasis: a population-based study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020;130(3):252-257. doi:10.1016/j.oooo.2020.04.808
4. Shapiro CL. Bone-modifying Agents (BMAs) in Breast Cancer. Clin Breast Cancer. 2021;21(5):e618-e630. doi:10.1016/j.clbc.2021.04.009
5. Goldvaser H, Amir E. Role of Bisphosphonates in Breast Cancer Therapy. Curr Treat Options Oncol. 2019;20(4). doi:10.1007/s11864-019-0623-8
6. Reyes C, Hitz M, Prieto-Alhambra D, Abrahamsen B. Risks and Benefits of Bisphosphonate Therapies. J Cell Biochem. 2016;117(1):20-28. doi:10.1002/jcb.25266
7. Mirelli C, Marino S, Bovio A, et al. Medication-Related Osteonecrosis of the Jaw in Dental Practice: A Retrospective Analysis of Data from the Milan Cohort. Dent J (Basel). 2022;10(5). doi:10.3390/dj10050089
8. Mauceri R, Coppini M, Attanasio M, et al. MRONJ in breast cancer patients under bone modifying agents for cancer treatment-induced bone loss (CTIBL): a multi-hospital-based case series. BMC Oral Health. 2023;23(1). doi:10.1186/s12903-023-02732-6
9. Boston B, Ipe D, Capitanescu B, et al. Medication-related osteonecrosis of the jaw: A disease of significant importance for older patients. J Am Geriatr Soc. 2023;71(8):2640-2652. doi:10.1111/jgs.18414
10. Soares AL, Simon S, Gebrim LH, Nazário ACP, Lazaretti-Castro M. Prevalence and risk factors of medication-related osteonecrosis of the jaw in osteoporotic and breast cancer patients: a cross-sectional study. Supportive Care in Cancer. 2020;28(5):2265-2271. doi:10.1007/s00520-019-05044-0
11. Kashyap D, Pal D, Sharma R, et al. Global Increase in Breast Cancer Incidence: Risk Factors and Preventive Measures. Biomed Res Int. 2022;2022. doi:10.1155/2022/9605439
12. Dall GV, Britt KL. Estrogen effects on the mammary gland in early and late life and breast cancer risk. Front Oncol. 2017;7(MAY). doi:10.3389/fonc.2017.00110
13. Sinn HP, Kreipe H. A brief overview of the WHO classification of breast tumors, 4th edition, focusing on issues and updates from the 3rd edition. Breast Care. 2013;8(2):149-154. doi:10.1159/000350774
14. Barzaman K, Karami J, Zarei Z, et al. Breast cancer: Biology, biomarkers, and treatments. Int Immunopharmacol. 2020;84. doi:10.1016/j.intimp.2020.106535
15. 14. Otto S ASFRESROBETMPCEMM (Kaunas).. Infection as an Important Factor in Medication-Related Osteonecrosis of the Jaw (MRONJ). Published online May 2021.
16. Tsang JYS, Tse GM. Molecular Classification of Breast Cancer.; 2019. http://journals.lww.com/anatomicpathology
17. Trayes KP, Cokenakes SEH. Breast Cancer Treatment. Am Fam Physician. 2021;104(2):171-178.
18. He Z, Chen Z, Tan M, et al. A review on methods for diagnosis of breast cancer cells and tissues. Cell Prolif. 2020;53(7). doi:10.1111/cpr.12822
19. Gradishar WJ, Anderson BO, Abraham J, et al. Breast cancer, version 3.2020. JNCCN Journal of the National Comprehensive Cancer Network. 2020;18(4):452-478. doi:10.6004/jnccn.2020.0016
20. Suarez-Almazor ME, Herrera R, Lei X, Chavez-MacGregor M, Zhao H, Giordano SH. Survival in older women with early stage breast cancer receiving low-dose bisphosphonates or denosumab. Cancer. 2020;126(17):3929-3938. doi:10.1002/cncr.33035
21. Gnant M, Pfeiler G, Dubsky PC, et al. Adjuvant denosumab in breast cancer (ABCSG-18): A multicentre, randomised, double-blind, placebo-controlled trial. The Lancet. 2015;386(9992):433-443. doi:10.1016/S0140-6736(15)60995-3
22. Coleman R, Finkelstein DM, Barrios C, et al. Adjuvant denosumab in early breast cancer (D-CARE): an international, multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2020;21(1):60-72. doi:10.1016/S1470-2045(19)30687-4
23. Fu PA, Shen CY, Yang S R, et al. Long-term use of denosumab and its association with skeletal-related events and osteonecrosis of the jaw. Sci Rep. 2023;13(1). doi:10.1038/s41598-023-35308-z
24. O’Carrigan B, Wong MHF, Willson ML, Stockler MR, Pavlakis N, Goodwin A. Bisphosphonates and other bone agents for breast cancer. Cochrane Database of Systematic Reviews. 2017;2017(10). doi:10.1002/14651858.CD003474.pub4
25. Poon M, Zeng L, Zhang L, et al. Incidence of Skeletal-related Events Over Time from Solid Tumour Bone Metastases Reported in Randomised Trials Using Bone-modifying Agents. Clin Oncol. 2013;25(7):435-444. doi:10.1016/j.clon.2013.03.003
26. Coleman R, Hadji P, Body JJ, et al. Bone health in cancer: ESMO Clinical Practice Guidelines †. Annals of Oncology. 2020;31(12):1650-1663. doi:10.1016/j.annonc.2020.07.019
27. Poznak C Van, Somerfield MR, Barlow WE, et al. JOURNAL OF CLINICAL ONCOLOGY Role of Bone-Modifying Agents in Metastatic Breast Cancer: An American Society of Clinical Oncology-Cancer Care Ontario Focused Guideline Update. J Clin Oncol. 2017;35:3978-3986. doi:10.1200/JCO
28. Anastasilakis AD, Pepe J, Napoli N, et al. Osteonecrosis of the Jaw and Antiresorptive Agents in Benign and Malignant Diseases: A Critical Review Organized by the ECTS. Journal of Clinical Endocrinology and Metabolism. 2022;107(5):1441-1460. doi:10.1210/clinem/dgab888
29. Dalle Carbonare L, Mottes M, Valenti MT. Medication-related osteonecrosis of the jaw (MRONJ): Are antiresorptive drugs the main culprits or only accomplices? the triggering role of vitamin d deficiency. Nutrients. 2021;13(2):1-14. doi:10.3390/nu13020561
30. Ruggiero SL, Dodson TB, Aghaloo T, Carlson ER, Ward BB, Kademani D. American Association of Oral and Maxillofacial Surgeons’ Position Paper on Medication-Related Osteonecrosis of the Jaws—2022 Update. Journal of Oral and Maxillofacial Surgery. 2022;80(5):920-943. doi:10.1016/j.joms.2022.02.008
31. Dunphy L, Salzano G, Gerber B, Graystone J. Medication-related osteonecrosis (MRONJ) of the mandible and maxilla. BMJ Case Rep. 2020;13(1). doi:10.1136/bcr-2018-224455
32. Fda. HIGHLIGHTS OF PRESCRIBING INFORMATION. www.fda.gov/medwatch.
33. Lu J, Hu D, Zhang Y, Ma C, Shen L, Shuai B. Current comprehensive understanding of denosumab (the RANKL neutralizing antibody) in the treatment of bone metastasis of malignant tumors, including pharmacological mechanism and clinical trials. Front Oncol. 2023;13. doi:10.3389/fonc.2023.1133828
34. Reid IR, Billington EO. Drug therapy for osteoporosis in older adults. The Lancet. 2022;399(10329):1080-1092. doi:10.1016/S0140-6736(21)02646-5
35. Kuehn S, Scariot R, Elsalanty M. Medication-Related Osteonecrosis: Why the Jawbone? Dent J (Basel). 2023;11(5). doi:10.3390/dj11050109
36. AlDhalaan NA, BaQais A, Al-Omar A. Medication-related Osteonecrosis of the Jaw: A Review. Cureus. Published online February 11, 2020. doi:10.7759/cureus.6944
37. Schiodt M, Otto S, Fedele S, et al. Workshop of European task force on medication-related osteonecrosis of the jaw—Current challenges. In: Oral Diseases. Vol 25. Blackwell Publishing Ltd; 2019:1815-1821. doi:10.1111/odi.13160
38. Hadaya D, Soundia A, Freymiller E, et al. Nonsurgical Management of Medication-Related Osteonecrosis of the Jaws Using Local Wound Care. Journal of Oral and Maxillofacial Surgery. 2018;76(11):2332-2339. doi:10.1016/j.joms.2018.05.025
39. Lončar Brzak B, Horvat Aleksijević L, Vindiš E, et al. Osteonecrosis of the Jaw. Dent J (Basel). 2023;11(1). doi:10.3390/dj11010023
40. Otto S, Pautke C, Van den Wyngaert T, Niepel D, Schiødt M. Medication-related osteonecrosis of the jaw: Prevention, diagnosis and management in patients with cancer and bone metastases. Cancer Treat Rev. 2018;69:177-187. doi:10.1016/j.ctrv.2018.06.007
41. Deepigaa M, Arvind M. Clinical Practice Guidelines in Dental Management of Medication Related Osteonecrosis of Jaw (MRONJ). Journal of Research in Medical and Dental Science 2021. 2021;9(1):128-133. www.jrmds.in
42. Kim JE, Yoo S, Choi SC. Several issues regarding the diagnostic imaging of medication-related osteonecrosis of the jaw. Imaging Sci Dent. 2020;50(4):273-279. doi:10.5624/ISD.2020.50.4.273
43. Kuchuk I, Mazzarello S, Butterfield K, Appleton A, Addison CL, Clemons M. Oral care and the use of bone-targeted agents in patients with metastatic cancers: A practical guide for dental surgeons and oncologists. J Bone Oncol. 2013;2(1):38-46. doi:10.1016/j.jbo.2012.12.001
44. Kün-Darbois JD, Fauvel F. Medication-related osteonecrosis and osteoradionecrosis of the jaws: Update and current management. Morphologie. 2021;105(349):170-187. doi:10.1016/j.morpho.2020.11.008
45. Kuroshima S, Sasaki M, Sawase T. Medication-related osteonecrosis of the jaw: A literature review. J Oral Biosci. 2019;61(2):99-104. doi:10.1016/j.job.2019.03.005
46. Kün-Darbois JD, Libouban H, Mabilleau G, Pascaretti-Grizon F, Chappard D. Bone mineralization and vascularization in bisphosphonate-related osteonecrosis of the jaw: an experimental study in the rat. Clin Oral Investig. 2018;22(9):2997-3006. doi:10.1007/s00784-018-2385-2
47. Lorenzo‐pouso AI, Bagán J, Bagán L, et al. Medication‐related osteonecrosis of the jaw: A critical narrative review. J Clin Med. 2021;10(19). doi:10.3390/jcm10194367
48. Gkouveris I, Hadaya D, Soundia A, et al. Vasculature submucosal changes at early stages of osteonecrosis of the jaw (ONJ). Bone. 2019;123:234-245. doi:10.1016/j.bone.2019.03.031
49. Basso FG, Pansani TN, Soares DG, Cardoso LM, Hebling J, de Souza Costa CA. Influence of bisphosphonates on the adherence and metabolism of epithelial cells and gingival fibroblasts to titanium surfaces. Clin Oral Investig. 2018;22(2):893-900. doi:10.1007/s00784-017-2167-2
50. de Molon RS, Hsu C, Bezouglaia O, et al. Rheumatoid Arthritis Exacerbates the Severity of Osteonecrosis of the Jaws (ONJ) in Mice. A Randomized, Prospective, Controlled Animal Study. Journal of Bone and Mineral Research. 2016;31(8):1596-1607. doi:10.1002/jbmr.2827
51. Wick A, Bankosegger P, Otto S, et al. Risk factors associated with onset of medication-related osteonecrosis of the jaw in patients treated with denosumab. Clin Oral Investig. 2022;26(3):2839-2852. doi:10.1007/s00784-021-04261-4
52. Khan AA, Morrison A, Hanley DA, et al. Diagnosis and management of osteonecrosis of the jaw: A systematic review and international consensus. Journal of Bone and Mineral Research. 2015;30(1):3-23. doi:10.1002/jbmr.2405
53. De Cicco D BCSMCGSSGABGVRDS. Medication-Related Osteonecrosis of the Jaws: A Comparison of SICMF-SIPMO and AAOMS Guidelines. Diagnostics (Basel). Published online June 2023.
54. şahin O, Odabaşı O, Aliyev T, Tatar B. Risk factors of medication-related osteonecrosis of the jaw: A retrospective study in a Turkish subpopulation. J Korean Assoc Oral Maxillofac Surg. 2019;45(2):108-115. doi:10.5125/jkaoms.2019.45.2.108
55. Soutome S, Otsuru M, Hayashida S, et al. Relationship between tooth extraction and development of medication-related osteonecrosis of the jaw in cancer patients. Sci Rep. 2021;11(1). doi:10.1038/s41598-021-96480-8
56. Avishai G, Muchnik D, Masri D, Zlotogorski-Hurvitz A, Chaushu L. Minimizing MRONJ after Tooth Extraction in Cancer Patients Receiving Bone-Modifying Agents. J Clin Med. 2022;11(7). doi:10.3390/jcm11071807
57. Pichardo SEC, van der Hee JG, Fiocco M, Appelman-Dijkstra NM, van Merkesteyn JPR. Dental implants as risk factors for patients with medication-related osteonecrosis of the jaws (MRONJ). British Journal of Oral and Maxillofacial Surgery. 2020;58(7):771-776. doi:10.1016/j.bjoms.2020.03.022
58. He L, Sun X, Liu Z, Qiu Y, Niu Y. Pathogenesis and multidisciplinary management of medication-related osteonecrosis of the jaw. Int J Oral Sci. 2020;12(1). doi:10.1038/s41368-020-00093-2
59. Singh N, Surface L. Dental Management of Medication-Related OSTEONECROSIS of the JAW: WHILE RARE, THIS PATHOLOGY HAS DEVASTATING EFFECTS ON PATIENT HEALTH AND QUALITY OF LIFE.
60. Nicolatou-Galitis O, Schiødt M, Mendes RA, et al. Medication-related osteonecrosis of the jaw: definition and best practice for prevention, diagnosis, and treatment. Oral Surg Oral Med Oral Pathol Oral Radiol. 2019;127(2):117-135. doi:10.1016/j.oooo.2018.09.008
61. Scribante A, Ghizzoni M, Pellegrini M, Pulicari F, Spadari F. Laser Devices and Autologous Platelet Concentrates in Prevention and Treatment of Medication-Related Osteonecrosis of the Jaws: A Systematic Review. Medicina (Lithuania). 2023;59(5). doi:10.3390/medicina59050972
62. Ottesen C, Schiodt M, Gotfredsen K. Efficacy of a high-dose antiresorptive drug holiday to reduce the risk of medication-related osteonecrosis of the jaw (MRONJ): A systematic review. Heliyon. 2020;6(4). doi:10.1016/j.heliyon.2020.e03795
63. Di Fede O, Panzarella V, Mauceri R, et al. The dental management of patients at risk of medication-related osteonecrosis of the jaw: New paradigm of primary prevention. Biomed Res Int. 2018;2018. doi:10.1155/2018/2684924
64. Yong CW, Robinson A, Hong C. Dental Evaluation Prior to Cancer Therapy. Frontiers in Oral Health. 2022;3. doi:10.3389/froh.2022.876941
65. Prof. G. Campisi – Professore Straordinario – Dirigente Medico I Livello Dott. O. Di Fede – Ricercatore-. PROMaF protocol: Prevention and research on Medication relate Osteonecrosis of the Jaws, . Published online December 2014.
66. A. Bedogni GCVF and AA. Raccomandazioni clinico-terapeutiche sull’osteonecrosi delle ossamascellari associata a bisfosfonati e sua prevenzione,” SICMF – SIPMO. Published online 2013.
67. Mauceri R, Panzarella V, Pizzo G, et al. Platelet-Rich Plasma (PRP) in dental extraction of patients at risk of bisphosphonate-related osteonecrosis of the jaws: A two-year longitudinal study. Applied Sciences (Switzerland). 2020;10(13). doi:10.3390/app10134487
68. Parise GK, Costa BN, Nogueira ML, Sassi LM, Schussel JL. Efficacy of fibrin-rich platelets and leukocytes (L-PRF) in tissue repair in surgical oral procedures in patients using zoledronic acid—case–control study. Oral Maxillofac Surg. 2023;27(3):507-512. doi:10.1007/s10006-022-01094-7
69. Moinzadeh AT, Shemesh H, Neirynck NAM, Aubert C, Wesselink PR. Bisphosphonates and their clinical implications in endodontic therapy. Int Endod J. 2013;46(5):391-398. doi:10.1111/iej.12018
70. Mosaico G, Casu C. Management and maintenance of oral health: Personalized primary prevention strategies and protocols in patients at risk of developing medication-related osteonecrosis of the jaw. INNOSC Theranostics and Pharmacological Sciences. 2024;0(0):1419. doi:10.36922/itps.1419
71. Ministero della Salute “Dipartimento della sanit`a pubblica e dell’innovazione. Raccomandazioni per la promozione della salute orale, la prevenzione delle patologie orali e la terapia odontostomatologica nei pazienti adulti con malattia neoplastica. Published online January 2014.
72. Hadaya D, Soundia A, Freymiller E, et al. Nonsurgical Management of Medication-Related Osteonecrosis of the Jaws Using Local Wound Care. Journal of Oral and Maxillofacial Surgery. 2018;76(11):2332-2339. doi:10.1016/j.joms.2018.05.025
73. Inchingolo AM, Malcangi G, Ferrara I, et al. MRONJ Treatment Strategies: A Systematic Review and Two Case Reports. Applied Sciences (Switzerland). 2023;13(7). doi:10.3390/app13074370
74. Kaibuchi N, Hoshi K, Yamazaki A, Miyamoto-Sangu N, Akagi Y, Okamoto T. The progress of medication-related osteonecrosis of the jaw with conservative initial treatment: A 12-year retrospective study of 129 patients. Bone Rep. 2021;14. doi:10.1016/j.bonr.2021.101072
Most read articles by the same author(s)
- Alina Čebatariūnienė, Teodora Gerliakaitė, Reuse of Implant Healing Abutments: A Narrative Review , Medical Research Archives: Vol 13 No 10 (2025): Vol.13, Issue 10, October 2025