

Melioidosis in Western Healthcare: A Case Report
Beyond Borders: A Case Report of Melioidosis and the Urgent Need for Tropical Disease Vigilance in Western Healthcare
Alexis Demas1
- Neurology Unit, Groupe Hospitalier du Havre, Le Havre, France
OPEN ACCESS
PUBLISHED 30 September 2025
CITATION Demas, A., 2025. Beyond Borders: A Case Report of Melioidosis and the Urgent Need for Tropical Disease Vigilance in Western Healthcare. Medical Research Archives, [online] 13(9). https://doi.org/10.18103/mra.v13i9.6831
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i9.6831
ISSN 2375-1924
Abstract
Melioidosis, caused by the Gram-negative bacillus Burkholderia pseudomallei, is increasingly recognised as a threat beyond its endemic regions of Southeast Asia and Northern Australia. Globalisation, international travel, and environmental change have facilitated its emergence in Western countries, where it remains underdiagnosed due to limited clinical awareness and microbiological preparedness. We report a case of imported melioidosis in a 52-year-old French male who returned from Thailand with an initial pulmonary presentation, followed by central nervous system involvement manifesting as focal pachymeningitis. Diagnostic efforts were hindered by the pathogen’s misidentification via MALDI-TOF mass spectrometry, due to biosecurity-related database restrictions excluding B. pseudomallei. Accurate diagnosis was achieved only after relapse and referral to a national reference laboratory. This case underscores the diagnostic and therapeutic challenges posed by tropical pathogens in non-endemic settings and the need to adapt clinical protocols, microbiological platforms, and physician training in Western healthcare systems. The emergence of such infections highlights the shifting landscape of global health, shaped by travel, climate change, and evolving microbial ecologies. Greater vigilance is warranted to prevent delayed diagnoses and optimise management of imported and emerging infectious diseases.
Keywords
Melioidosis, Burkholderia pseudomallei, tropical diseases, Western healthcare, diagnostic challenges
Introduction
In an era of accelerating globalisation, climate disruption, and ecological transformation, Western countries are increasingly confronted with infectious diseases historically endemic to tropical and subtropical regions. This growing phenomenon stems not only from the intensification of international travel and tourism but also from global warming, changes in land use, and altered distributions of microbial ecosystems. Consequently, European and North American clinicians are being exposed to pathogens once considered exotic or limited to specific geographical zones.
Among these, melioidosis—caused by Burkholderia pseudomallei—represents a paradigmatic example. This Gram-negative, environmental saprophyte is endemic to Southeast Asia and northern Australia, thriving in soil and stagnant water, particularly in rice paddies and humid agricultural zones. Human infection typically occurs through inhalation, ingestion, or percutaneous inoculation, particularly during monsoon seasons or extreme weather events.
Despite its long-standing recognition in endemic areas, melioidosis remains largely unfamiliar in the West. Known as “the great mimicker,” the disease manifests in a broad spectrum of clinical forms—ranging from latent or asymptomatic colonisation to fulminant sepsis, pulmonary abscesses, or neurological involvement. The case-fatality rate can exceed 40% in septic forms without appropriate treatment.
The diagnostic complexity of melioidosis in Western countries arises from several interrelated factors. Firstly, low clinical suspicion due to unfamiliarity can lead to diagnostic delay or misdiagnosis. Secondly, many laboratories lack standardised protocols for identification of B. pseudomallei, and its classification as a potential bioterrorism agent has led to its exclusion from many MALDI-TOF reference databases used in routine diagnostics. Finally, neurological manifestations—although rare—can obfuscate diagnosis further, particularly when mimicking more prevalent entities such as tuberculosis, autoimmune encephalitis, or metastatic disease.
From an epidemiological perspective, the global burden of melioidosis is likely underestimated. A modelling study by Limmathurotsakul et al. suggested over 165,000 cases annually worldwide, with high mortality in low-resource settings. Importantly, cases are increasingly being reported in Europe and North America, especially among travellers, immigrants, and military personnel. The potential for environmental persistence and reactivation years after exposure adds another layer of complexity.
The Western medical community must adapt to these realities. Medical curricula, microbiology laboratories, and hospital infection protocols should integrate knowledge of emerging tropical diseases, particularly in the context of increasing international mobility and climate change. This includes updating diagnostic databases, improving epidemiological surveillance, and fostering clinical awareness among physicians.
In this report, we present a clinically and microbiologically challenging case of imported melioidosis in a French traveller returning from Thailand, who developed focal pachymeningitis due to B. pseudomallei. Through this case, we aim to underscore the need for greater diagnostic preparedness and strategic awareness in Western healthcare systems facing the growing influx of emerging and re-emerging infectious diseases.
Case Presentation
A 52-year-old French male was admitted to the emergency department with fever, persistent headache, and a dry cough. He had returned five days earlier from Koh Samui, Thailand, where he had been working as a construction foreman. His medical history was notable for type 2 diabetes mellitus managed with insulin.
On admission, the patient was febrile (40.2 °C) but hemodynamically stable, with an oxygen saturation of 98% on room air. Pulmonary auscultation revealed crackles in the left lower lung field. Laboratory results showed a normal leukocyte count (4.1 G/L) but elevated C-reactive protein (154 mg/L). Chest radiography demonstrated a left basal infiltrate consistent with pneumonia. Blood cultures were collected, and empirical amoxicillin therapy was initiated for presumed community-acquired pneumonia.
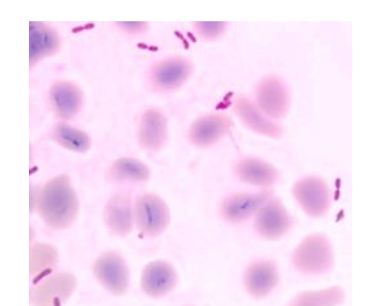
On day two, blood culture revealed Gram-negative bacilli with bipolar staining. MALDI-TOF analysis identified the organism as Burkholderia thailandensis, a rare and generally non-pathogenic relative of B. pseudomallei. Based on this result and the antibiogram, therapy was switched to oral levofloxacin, and the patient was discharged.
Five days later, the patient returned with worsening headaches and right-sided myoclonus with secondary generalised seizures. Neurological examination revealed no focal deficits. EEG was normal. CSF analysis showed mild pleocytosis (5 white blood cells), elevated protein (1.13 g/L), normal glucose, and negative cultures including 16S rRNA PCR. Brain MRI demonstrated focal frontoparietal pachymeningitis with gadolinium enhancement.

Given the persistent inflammatory syndrome, unusual neurological findings, and the rare organism initially isolated, the bacterial strain was reanalysed at a national reference laboratory. Multiplex PCR and additional testing confirmed Burkholderia pseudomallei.
A diagnosis of melioidosis with CNS involvement was established. Treatment with intravenous meropenem (6 g/day) was initiated for three weeks, followed by oral trimethoprim-sulfamethoxazole (TMP-SMX) for 10 weeks. The patient’s symptoms resolved completely. Follow-up MRI at three months showed resolution of pachymeningeal enhancement.
Discussion
This case illustrates the diagnostic complexity of melioidosis in non-endemic regions, where clinical unfamiliarity and technical limitations contribute to significant delays in appropriate management. Our patient, who returned from Thailand, initially presented with non-specific systemic and neurological symptoms that progressed to focal pachymeningitis. The causative organism, Burkholderia pseudomallei, was initially misidentified as B. thailandensis, a closely related but non-pathogenic species, due to its absence from the standard MALDI-TOF database—an exclusion stemming from its classification as a potential bioterrorism agent.
This misidentification led to inappropriate antibiotic therapy and early discharge, likely facilitating dissemination to the central nervous system (CNS). The recurrence of symptoms and neurological deterioration prompted re-analysis and accurate identification of the organism, illustrating how diagnostic setbacks in melioidosis can significantly alter the clinical trajectory. Similar diagnostic pitfalls have been reported in recent case series across Europe and North America, where imported melioidosis has led to delays in treatment and increased morbidity.
Melioidosis, although long recognised in endemic regions such as Southeast Asia and Northern Australia, remains underappreciated in Western clinical settings. It is a disease of protean manifestations: acute pulmonary infections, septicaemia, abscesses in visceral organs, osteomyelitis, and, in about 3–5% of cases, neurological involvement. The pathogenesis of neuro-melioidosis typically involves haematogenous spread across the blood-brain barrier, but may also result from direct extension or retrograde neural transmission. CNS involvement may manifest as encephalitis, brainstem syndromes, cranial neuropathies, or pachymeningitis—each mimicking other infections or inflammatory pathologies such as tuberculosis, sarcoidosis, or autoimmune encephalitis.
Our case is clinically significant due to its unusual neurological presentation and the subtlety of early systemic signs. Neurological melioidosis is particularly challenging, as initial brain imaging may be normal, and cerebrospinal fluid analysis may not yield specific findings. Thus, in returning travellers presenting with fever and unexplained neurological symptoms, especially after exposure to tropical or agricultural environments, clinicians should maintain a high index of suspicion.
Historically, melioidosis gained notoriety in the West during the Vietnam War, when American soldiers developed latent infections that reactivated years after their return. These observations underscore the bacterium’s ability to persist in a dormant state within host tissues, reactivating during periods of immune suppression. This capacity for latency and reactivation poses unique challenges to public health and clinical vigilance.
Therapeutically, melioidosis requires a two-phase antibiotic strategy. The intensive phase consists of intravenous administration of ceftazidime or meropenem for a minimum of 10–14 days. The eradication phase involves oral trimethoprim-sulfamethoxazole (TMP-SMX) for at least 12 weeks, and often longer in the case of deep-seated infections or neurological involvement. In our patient, delayed initiation of appropriate therapy may have prolonged disease duration and increased the risk of complications. Early, pathogen-specific treatment remains the cornerstone of successful management.
This case also raises broader issues related to global health and preparedness. With increasing global mobility and climatic shifts, European healthcare systems are likely to encounter more cases of melioidosis and other emerging infections. There is an urgent need to adapt diagnostic tools, such as expanding MALDI-TOF databases to include pathogens of tropical relevance, even those listed as potential biothreat agents. At the policy level, guidelines must be updated to reflect the epidemiological realities of a connected world.
Finally, public health surveillance systems and travel medicine protocols should integrate risk stratification for melioidosis in individuals returning from endemic areas, particularly if they present with fever of unknown origin or neurological symptoms. Education and training for clinicians, especially those in emergency medicine, infectious diseases, and neurology, must include recognition of diseases like melioidosis that challenge Western diagnostic norms.
Conclusion
The case of imported melioidosis we describe not only reflects the challenges of diagnosing a rare and unfamiliar disease in a non-endemic setting, but also exemplifies the broader impact of globalisation and ecological disruption on clinical practice. The failure to initially identify Burkholderia pseudomallei due to database limitations and insufficient awareness highlights systemic vulnerabilities in Western diagnostic infrastructures.
As international travel continues to rise and climate change reshapes microbial geographies, diseases like melioidosis will become increasingly relevant in Western medicine. It is imperative that clinicians adopt a broader, globally-informed diagnostic mindset, particularly in the evaluation of fever and neurological syndromes in returning travellers. Laboratory capacities must also evolve, with updated reference libraries and training to recognise previously unfamiliar pathogens.
Improving awareness, refining diagnostic tools, and strengthening global surveillance are no longer optional measures but vital components of infectious disease preparedness. Melioidosis serves as a sentinel condition in this regard—a reminder that the microbial world is interconnected, and that vigilance, adaptability, and education are key to managing tomorrow’s infections today.
References
- Jones KE, Patel NG, Levy MA, et al. Global trends in emerging infectious diseases. Nature. 2008;451(7181):990–993.
- Carlson CJ, Albery GF, Merow C, et al. Climate change increases cross-species viral transmission risk. Nature. 2022;607(7919):555–562.
- Wu X, Lu Y, Zhou S, Chen L, Xu B. Impact of climate change on human infectious diseases: Empirical evidence and human adaptation. Environ Int. 2016;86:14–23.
- Cheng AC, Currie BJ. Melioidosis: epidemiology, pathophysiology, and management. Clin Microbiol Rev. 2005;18(2):383–409.
- Currie BJ. Melioidosis: evolving concepts in epidemiology, pathogenesis, and treatment. Semin Respir Crit Care Med. 2015;36(1):111–125.
- Dance DA. Melioidosis: the tip of the iceberg? Clin Microbiol Rev. 1991;4(1):52–60.
- Limmathurotsakul D, Golding N, Dance DA, et al. Predicted global distribution of Burkholderia pseudomallei and burden of melioidosis. Nat Microbiol. 2016;1:15008.
- Howard K, Inglis TJ. The effects of Burkholderia pseudomallei biosecurity requirements on microbiological diagnosis and research. Med J Aust. 2003;178(5):242–244.
- Yung AP, McDonald MI. Neurological melioidosis: a review of cases from tropical northern Australia. Clin Infect Dis. 2003;36(3):392–397.
- Limmathurotsakul D, et al. Predicted global distribution of B. pseudomallei. Nat Microbiol. 2016;1(1):15008.
- Biggs BA, et al. Melioidosis in returning travellers: review of cases in Victoria, Australia. Med J Aust. 2014;200(2):136–138.
- Allworth AM. Melioidosis: An imported infection seen in military personnel. Aust N Z J Med. 1986;16(5):803–807.
- Sanford JP. Melioidosis: a persistent problem. J Infect Dis. 1980;142(3):386–389.
- Wiersinga WJ, Currie BJ, Peacock SJ. Melioidosis. N Engl J Med. 2012;367(11):1035–1044.
- Currie BJ, Ward L, Cheng AC. The epidemiology and clinical spectrum of melioidosis: 540 cases from the 20-year Darwin prospective study. PLoS Negl Trop Dis. 2010;4(11):e900.
- Meumann EM, et al. Neuromelioidosis: neurological manifestations of melioidosis. Trop Med Infect Dis. 2019;4(1):38.
- Lipsitz R, et al. Workshop on treatment of and postexposure prophylaxis for Burkholderia pseudomallei and B. mallei infection, 2010. Emerg Infect Dis. 2012;18(12):e2.