






Mortality Factors in Asthmatic ICU Patients: A Study
Variables Influencing Mortality in Asthmatic Patients Admitted to the Intensive Care Unit with Respiratory Failure
İnşa Gül Ekiz İşcanlı 1, Gökay Güngör 1, Nezihe Gökşenoğlu 2, Barış Yılmaz 1, Gül Erdal Dönmez 1, Muhammet Emin Çelik 3, Fatma Kübra Demir 4, Özlem Yazıcıoğlu Moçin 1, Tuğcan Kalkan 5, Sinem Güngör 1, Eylem Tuncay 6, Emine Aksoy 1, Huriye Berk Takır 1, Meltem Ağca 1, Beste Atabek 7, Tuğba Küççük 8, Nalan Adıgüzel 1, Zuhal Karakurt 1
- University of Health Sciences Sureyyapasa Chest Diseases and Thoracic Surgery Teaching and Research Hospital, Department of Intensive Care Unit, Istanbul -Turkiye
- University of Medeniyet Faculty Department of Intensive Care Unit, Istanbul -Turkiye
- Bilkent City Hospital, Department of Intensive Care Unit, Ankara-Turkiye
- Ankara 29 Mayıs Government Hospital, Department of Pulmonology Ankara -Turkiye
- Dörtyol Governmet Hospital Intensive Care Unit, Hatay-Türkiye
- University of Health Sciences Prof Dr İlhan Varank Sancaktepe Teaching and Research Hospital, Department of Pulmonology, Istanbul -Turkiye
- Ağrı Teaching and Research Hospital, Department of Pulmonology, Ağrı-Türkiye
- Yozgat City Hospital, Department of Pulmonology Yozgat-Türkiye
OPEN ACCESS
PUBLISHED: 31 May 2025
CITATION: İşcanlı, İGE., Güngör, G., et al., 2025. Variables Influencing Mortality in Asthmatic Patients Admitted to the Intensive Care Unit with Respiratory Failure. Medical Research Archives, [online] 13(5). https://doi.org/10.18103/mra.v13i5.6594
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i5.6594
ISSN 2375-1924
ABSTRACT
Introduction: Acute respiratory failure caused by asthma episodes has decreased significantly due to the use of anti-inflammatory and bronchodilator inhalers. Although asthmatic individuals require less intensive care units, respiratory failure can still cause intensive care unit mortality. Our study examined characteristics that define the mortality risk in asthmatic patients with respiratory failure in the intensive care unit.
Methods: A teaching diseases hospital’s intensive care units were the setting for the retrospective, observational, cross-sectional study from 2016 to 2021. Asthmatic patients in the intensive care unit with acute respiratory failure were included in the study. Causes of respiratory failure, intensive care severity score (APACHE II), type of respiratory supports (invasive and noninvasive mechanical ventilation, high flow oxygen therapy) and duration, length of intensive care unit stays, and mortality rates were recorded. A multivariate regression analysis model for mortality risk was used and analyzed by classifying mortality risk factors.
Results: The study, ICUs examined 14,575 patients. Asthma affected 438 people (3%). The study included 438 patients, 347 of whom were female (79%). Median (25%-75%), age and APACHE II score were 68 (55-78) and 17 (14-22). In asthmatics, pneumonia caused 50.5% of acute respiratory failure, sepsis 27.4%, Covid-19 14.4%, acute renal failure 8%, and acute cardiogenic edema 6.6%. The invasive mechanical ventilation was 21% (n=94), the mortality was 48 (11%). The odds ratios (confidence interval 95%, lower-upper limit) for mortality were congestive heart failure (CHF): 4.47 (1.55-12.85), APACHE II score of 20 or higher: 2.65 (1.10-6.38), invasive mechanical ventilation: 26.33 (9.80-70.70), and COVID-19: 2.84 (1.20-6.75).
Conclusions. Asthmatics requires nearly 3% ICU treatment for respiratory failure for various reasons. In asthma patients, an intensive care unit need due to APACHE II value above 20, invasive mechanical ventilation, COVID-19 and congestive heart failure increase the risk of mortality in the ICU.
Keywords
asthma; acute respiratory failure; invasive mechanical ventilation; intensive care unit; mortality
Main Points
- The need for intensive care unit (ICU) for asthma attacks is decreasing compared to the past. A higher proportion of asthma patients are followed up in ICU in the specific center for chest diseases than in general hospitals and mortality, which is very low in the literature, is even higher.
- The identification of mortality predictors and taking measures enable to reduce mortality in ICU.
- Risk factors for mortality in ICU are clinical severity of respiratory failure at ICU admission (high APACHE II), having heart failure-acute cardiogenic edema, need of invasive mechanical ventilation, COVID-19 in pandemic.
Introduction
The prevalence of asthma was nearly 5% of adults and 7% of children 1-3. Asthmatic patients experiencing exacerbations commonly exhibit significant bronchoconstriction in their large airways, which can be triggered by environmental factors, seasonal allergies, and psychosocial factors 3-5. Asthma symptoms are managed using anti-inflammatory and bronchodilator medications. The control of asthma in childhood and young adulthood depends upon adherence to inflammatory treatment. The use of long-acting anti-inflammatory inhaler medications has resulted in a reduction in the need for intensive care unit (ICU) admissions for severe asthma attacks. Nevertheless, a small proportion of patients, ranging from 1.1% to 1.7%, required admission to the ICU due to an asthma attack 6-9. Despite the need for ICU management that has declined in asthmatic patients, those with acute respiratory failure (ARF) may still require invasive mechanical ventilation (IMV) support 10-13. Those patients may experience various rates of mortality, ranging from 16% to 19% 14,15. There has been a reported reduction in higher mortality rates in the ICU by 38% ranging from 0% to 8% with inhaled treatments that improve adherence to therapy over a period 6,10-13,16,17. There are some studies have reported the factors that increase the risk of mortality in asthma patients who require IMV in the ICU 10-13,15. Early in the pandemic, asthma as a comorbidity was defined as a risk factor for ICU mortality, especially in patients with COVID-19 18,19. Respiratory failure in asthma patients may require mechanical ventilation when caused by an asthma attack or pneumonia. Mechanical ventilation support in asthma patients is not as straightforward as in other patients, and delays in extubation may lead to steroid-induced myopathy, sepsis, and increased mortality. We aimed to evaluate asthma prevalence, and the mortality risk factors in ICU for patients with asthma comorbidity or patients admitted to ICU with asthma attack. The results of the planned study, which objective to determine asthma prevalance, mortality risk factors, and necessary precautions over the years at an expert center specializing in the management of asthma patients in the respiratory intensive care unit, will be significant.
Methods
This study was designed retrospective observational cross sectional study design. The study was approved by the local Ethics Committee of the University of Health Sciences Sureyyapasa Chest Diseases and Thoracic Surgery Teaching and Research Hospital, Noninvasive Clinical (Date, 06.04.2023 and No: 116.2017.R-292) and it was conducted in accordance with the ethical principles stated in the Declaration of Helsinki. Due to the nature of retrospective design, the signed informed consent was not obtained. The local ethics committee does not require signed informed consent for retrospective studies. The study was conducted at a chest disease teaching hospital level II and III respiratory ICUs between May 2016 and December 31, 2021. The study period was selected based on the availability of digital records for patients with asthma and the ability to obtain data from the hospital information management system. Part of the study data were collected in February 2022 and was presented as an oral presentation in May 2022 national congress. The ICU was a specialized unit especially respiratory diseases and Level II ICU had 34 beds and Level III had 26 beds and in 2016-2020. During pandemic Level III ICU beds were increased up to 60 beds and Level II 38 beds, total beds number were 98 in Pandemic. The respiratory ICU was for training purposes and a faculty team of 12 pulmonology and critical care specialist-academicians, along with 10 pulmonology residents, deliver round-the-clock patient care during medical training in the ICU. All ICU physicians and nurses follow previously well-defined ICU guidelines.
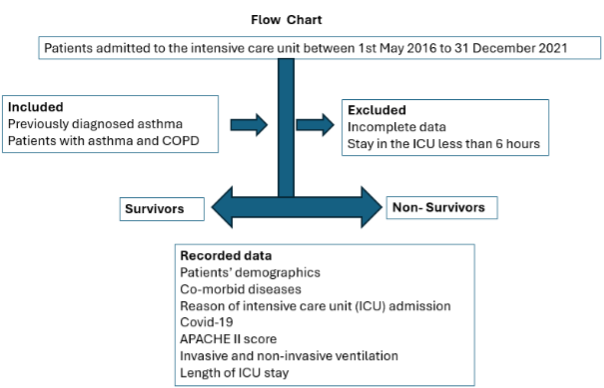
Patients: The patients who were hospitalized to the ICU due to respiratory failure and had a pre-existing diagnosis of asthma, were included in the study (Figure 1). We included all patients with asthma. Asthma patients who refuse ICU admission or stay less than 6 hours were excluded from the study.
Definitions: Patients who had previously been diagnosed with asthma were included in the study. Asthma diagnoses were re-confirmed by checking that they were in accordance with national and international guidelines and that they correlated with the clinics20,21. Acute respiratory distress syndrome (ARDS), can be confirmed after ruling out cardiogenic pulmonary edema and other potential causes of severe hypoxemic respiratory failure, as well as bilateral infiltrates. The diagnosis of ARDS according to the Berlin Definition necessitates the presence of all the specified criteria 22, 23. Sepsis: Sepsis is a critical medical condition characterized by the body’s widespread immune reaction to an infection, which can result in severe organ failure and mortality. COVID-19: The severe acute respiratory syndrome coronavirus 2 (SARS-CoV2) polymerase chain reaction (PCR) testing by nasal-pharynx swap was positive in patient with pneumonia is called COVID-1924. Causes of acute respiratory failure: Patients with severe low oxygen levels in the blood (partial arterial oxygen [PaO2] less than 150 mmHg compared to the amount of oxygen inhaled with or without high levels of carbon dioxide in the blood (partial arterial carbon-dioxide [PaCO2] greater than 45 mmHg) were admitted to the ICU25,26.
Medical Treatment: COVID-19 and other main reasons of ARF were treated with related guidelines. In severe hypoxemic patients with Covid-19, metilprednisolon was used mini pulse (250 mg/day) for three-day duration later 80-60 mg/day uses were completed in 5-7 days. In this study total doses of steroid use were not recorded. Antibiotic regimes were designed according to cultural results. Antifungal drugs were started after cultural fungal species and positivity for galactomannan testing. All these medications were not recorded. All ICU team followed the same medication program which were designed by international and national guidelines.
Respiratory support: Oxygen treatment was administered by nasal cannula at a flow rate of 5-6 L/min when the oxygen saturation level dropped to 92%. An oxygen mask was administered at a flow rate of 6-8 liters per minute if the pulse oxygen saturation did not reach 92% with 6 liters per minute nasal cannula. Oxygen supplementation was administered at a flow rate of 8-10 L/min using a reservoir bag. High flow oxygen (HFO) was administered when the pulse saturation level dropped below 88% while using 8-10 liters per minute of oxygen with a reservoir bag. The specific category of oxygen support number was not documented and examined as a distinct entity.
Mechanical ventilation support: ICU mechanical ventilators in pressure assist-control mode delivered the NIV via a double-tube circuit and full-face mask26. Invasive mechanical ventilation was used when non-invasive ventilation (NIV) was ineffective or contraindicated26. The Richmond agitation sedation scale (RASS) was used to assess daily sedative needs27. Patients who met weaning criteria were extubated after completing a spontaneous breathing trial28,29. After the extubating, moderate respiratory distress patients received NIV if there were no contraindications28,29.
Data: Patients demographics, co-morbid diseases (diabetes mellitus [DM], hypertension, coronary heart diseases [CHD], congestive heart failure [CHF], arrythmias [atrial fibrillation, ventricular tachycardia], dementia, Alzheimer, Parkinson, cerebrovascular accident [CVA], chronic renal failure [CRF], having tracheostomized) were recorded. Acute physiologic and chronic health evaluations (APACHE) II score30 was calculated according to ICU severe criteria, COVID-19, and pneumonia other than COVID-19, IMV and NIV, Oxygen therapy and durations; the length of ICU stay were recorded from patients’ files.
STATISTICAL ANALYSIS
The patient data were evaluated with the portable SPSS 20 software. Continuous variables (such as age, hospitalization days, and APACHE II) were recorded according to their distribution. The mean and standard deviation (SD) were used to describe data that follows a normal distribution. The individuals having distributions that deviated from normality were characterized using the median and interquartile range (25%-75%). The normality of distributions was assessed using the Shapiro-Wilk test. The dichotomous variables (such as gender, presence or absence of comorbidities, presence or absence of ventilator usage, mortality, etc.) were quantified as both a numerical value and a percentage (%). The patients with asthma were divided into two groups based on gender and mortality. The Mann-Whitney U test was employed to compare continuous nonparametric variables that do not follow a normal distribution. The student’s t-test was utilized to analyze continuous parametric variables that were normally distributed. The Chi-square test was utilized to compare dichotomous variables, and the results were presented as n (%). Mortality risk variables were assessed by logistic regression analysis. A p value of 0.05 was accepted as statistical significance.
Results
In the study period, a total of 14,575 patients were admitted to the ICU with 438 (3%) of them being asthma patients. A total of 438 asthma patients were included in the study, with 347 of them being female (79%). Majority of asthmatic patients were elder (over 65 yar of age), 20% long term oxygen therapy (LTOT) and 10% long term home NIV (H-NIV) therapy user. Half of the patients had at least one hospitalization and one third had required ICU due to respiratory failure. Smoke history was nearly 15%, hypertension was observed by more than half of patients (58%), later diabetes (38%) and congestive heart failure (15%) (Table 1). Among 438 patients, 48 (11%) ones died in the ICU. The comparison of survivors and non-survivors for demographics and co-morbid diseases in asthma patients with respiratory failure were nearly similar (Table 1).
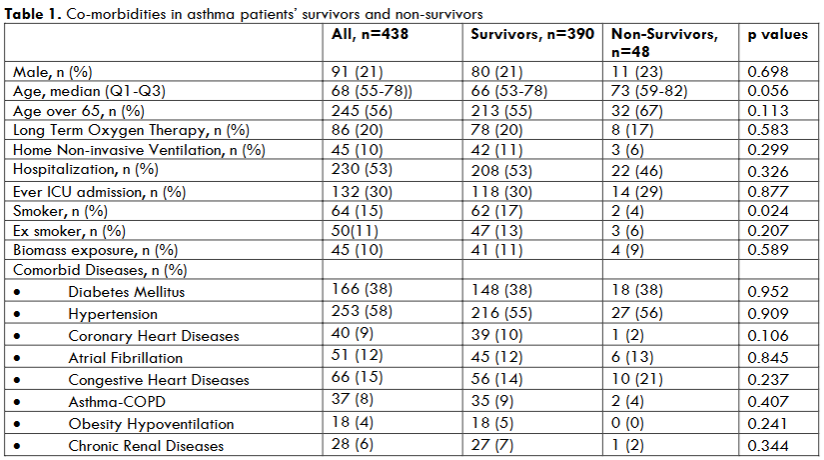
Table 2 shows a summary of the causes of acute respiratory failure; the type of respiratory support, and the duration of stay in the intensive care unit (ICU) for asthmatic patients. 50% of the patients were admitted to the hospital because of pneumonia. Acute Respiratory Distress Syndrome (ARDS) occurred in 5% of pneumonia cases and was observed in 14% of those diagnosed with COVID-19. 7% of the patients experienced acute cardiogenic edema, whereas 8% developed acute renal failure. A comparison between those who survived and those who did not survive revealed a markedly greater prevalence of ARDS, sepsis, pneumonia, COVID-19, and newborn hypoxia in the deceased group. However, none of the non-survivors had acute cardiogenic edema. The intensive care severity score, APACHE II was significantly greater in survivors than non-survivors (27 compared to 16). There was a significant increase in the utilization of invasive mechanical ventilation following unsuccessful attempts with NIV among those non-survivors. Conversely, the utilization of NIV or HFO was much lower in non-survivors.
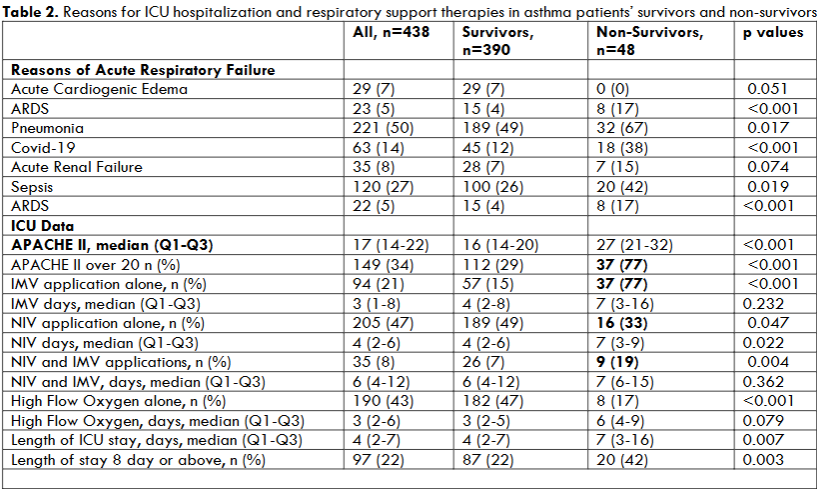
Out of the total of 22 patients diagnosed with ARDS, 10 of them were affected by the COVID-19 virus. The death rate for patients with ARDS plus COVID-19 was found to be similar mortality rate for patients without COVID-19, with rates of 50% and 40% respectively.
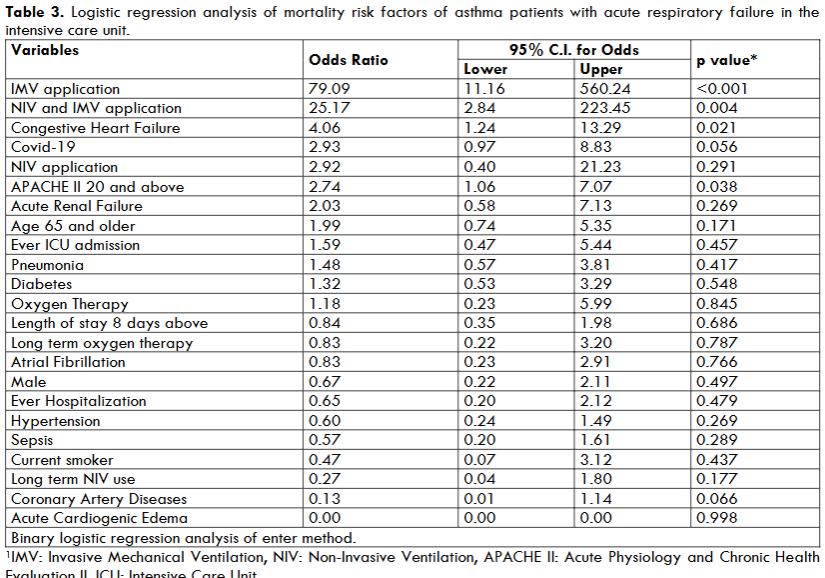
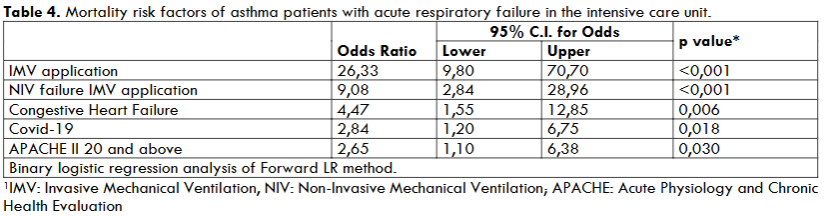
Table 3 and Table 4 summarized the logistic regression model built as mortality risk factors for asthma patient with respiratory failure due to co-morbidities, reasons of ARF, type of respiratory supports. The Logistic regression analysis was performed as enter (Table 3). The mortality risk factors were IMV, IMV after NIV failure, congestive heart failure. When the forward Likely Ratio method was applied in the Binary Logistic regression test, 5 mortality risk factors were identified for 48 deaths (Table 4).
Discussion
This study shows that in the center specific to chest patients, patients in the ICU have an asthma prevalence of 3%. Four-fifths of the patients are female. Pneumonia other than COVID-19, sepsis, COVID-19, acute renal failure, and acute cardiogenic edema are the most common reasons for acute respiratory failure. The IMV rate is 21% and the mortality rate is 11%. The 26-fold IMV and 9-fold NIV failure, 4.5-fold congestive heart failure, 2.8-fold COVID-19 and 2.7-fold APACHE II value of 20 and above are found as the risk factors for mortality in patients with asthma in the respiratory ICU.
ASTHMA PREVALENCE IN THE ICU, PATIENTS’ CHARACTERISTICS, AGE, SEX AND CO-MORBIDITIES
Very recently, in a bi-national study (Australia-New Zealand and USA) conducted by Abdelkarim et al12. in asthmatic patients hospitalized in the ICU in 2014-2015, it was shared that asthma patients were found at a very low rate of 0.73-0.46% in the ICU, were young (42-43 years old) and mostly women (69%)6. In the same study, it was reported that there was no information about the comorbidities of the patients and their pre-ICU period. Again, very recently, in a study conducted by Younan et al31 in asthmatic patients hospitalized in ICUs in the Paris region in a 20-year period (1997-2016), the rates of asthma patients in 5-year periods were 2.84%, 1.76%, 1.05%, 1.05%, respectively, and the median age was 46 years, and 55.4% female patients were reported31. Nanchal and et al32, a total of 2,476,955 hospitalizations with the principal diagnosis of AE in adults over 18 years of age from 2000 to 2008 in the USA and approximately 10% of hospitalizations include an ICU stay, and study results showed an increase in adults hospitalized for asthma attack in 2008 were older and had more comorbid diseases. Binoachon reported that the rate of IMV patients with asthma was 0.05%, the median age was 49 years and 64% were women. In the same study, comorbidity records were also obtained, and 58% of patients had no comorbidity, while the most common comorbidities were diabetes (26%), COPD (10%), presence of immunosuppression (6%), renal failure (5%), cirrhosis (3%), and cancer (1%)33. Sunjaya and coworkers were done a metanalysis of 51 studies conducted between December 1, 2019, and July 11, 2021, they reported the association of COVID-19 and asthma as 8.08%34. The mean age was 52 years (SD 12) and 57.3% were female. Hypertension (10-25%), diabetes (10-20%), and COPD (5-10%) were reported as comorbidities in 40 studies. In our study, we had a higher prevalence of asthmatic patients (3%), this result was possibly the study hospital which is a center for chest diseases. And our asthmatic patients were older (mean age 68) and the female predominance (79%) was higher compared to other studies. We attribute these differences due to our center, which receives asthmatic patients from other centers. The present study center is a reference chest disease-specific intensive care unit. The predominance of women in our center, which manages elderly asthmatic patients with comorbidities, which are more difficult to manage, may be explained by the fact that the severity of attacks may increase in some postmenopausal asthma patients. In a meta-analysis conducted by Zemp et al35 on this subject, it was reported that there were studies showing that the incidence of asthma would increase with menopause, while a large cohort study showed no difference. Although there are conflicting studies on the incidence of asthma in menopause, we can say that the severity of asthmatic women’s attacks may increase with age because of comorbidities. In our study, hypertension was the most common comorbidity, followed by diabetes. However, the prevalence of hypertension and diabetes was approximately 2 times higher than in the other studies, while the rates of COPD-Asthma (ACO) were similar. This may be since our patients were approximately 20 years older than in the other studies. The other co-morbid diseases such as cardiac arrhythmia and heart failure, which were not reported in previous studies, were also reported.
CIGARETTE SMOKE AND ASTHMA
Binachon et al33 reported that 41% (n=33) of all 80 patients with severe asthma who underwent IMV were active smokers, 43% (n=29) of those who lived and 33% (n=4) of those who died. In Sunjuva et al study34, 5.4% were current smokers (n=38 672 from 23 out of 51 studies) and 9.8% were former smokers (n=43 622 from 10 out of 51 studies) in patients with COVID-19 and asthma. In the same study, no statistically significant association for current smokers (five out of 10 studies; p=0.09) and former smokers were found (two out of 10 studies; p=0.94). In present study, smoking history was 30% (n=132), smoking history was similar in survivors and non-survivors in the ICU (30% vs 29%), and active smokers were significantly more in those survivors (17% vs 4%, p=0.024). We can explain that the patients quit active smoking as their general condition worsened, it was thought that active smokers were less in the non-survivors. In studies, 30%-40% smoking may be considered among the risks that make asthma attacks difficult to control and lead to ICU hospitalizations.
INVASIVE MECHANICAL VENTILATION AND MORTALITY IN THE INTENSIVE CARE UNIT
In recent studies, Abdelkerim et al.12 reported intubation rates of 24.4% and 24.7% for patients with asthma in the USA and Australia-NewZelland, respectively, and ICU mortality of those intubated was similar in the USA and Australia-NewZelland (0.54% vs. 2.0%, p=0.31). In the same study, overall mortality in patients with asthma in the ICU was similar, 0.79% in the USA and 0.79% in Australia-NewZelland (p=0.81). In France in the French overseas territory of Reunion Island, Binoachon et al.33 reported an intubation rate of 42%, while intubation was 57% in the study by Gupta et al6 In 2014, Nanchal et al32 reported that intubation rates in mechanical ventilation in the treatment of asthma exacerbations in the 2000-2008 period decreased over time (1.4% in 2000 to 0.73% in 2008) and NIV applications increased (0.34% to 1.9%)32. Nanchal et al published the mortality of asthmatic patients in the first 3 days of follow-up and reported that the odds of in-patient mortality were significantly lower in 2008 than in 2000 (OR 0.64, 95% CI 0.51- 0.81)32. In our study, the intubation rate was 29.5% and mortality was 11%, higher than in other studies. The high rates may be explained by the fact that the study center was a reference hospital specific to chest diseases. In the present study, IMV has also been reported as a very important risk factor for mortality.
LIMITATIONS
There are some limitations in present study. The first one is a retrospective design. However, all patients’ files obtained from ICU statistic data were reliable and missing values were acceptably low. The second one was the study conducted in a single center so it may not be correct to generalize our results. Meanwhile, the study center is the biggest training chest hospital in the country so the hospitalized patients with asthma can represent the other centers.
Conclusions
This study results revealed that asthma prevalence is less than 3 percent in the respiratory ICU. Asthma control is getting better after dual treatment of inhaling steroid and bronchodilators via new technique devices. Our study revealed a high prevalence of middle-aged female asthma patients at ICU, which led us to conclude that we should place greater emphasis on asthma control and the management of comorbidities, particularly in postmenopausal women. Asthma patients may require intensive care unit admission due to the risk of lung infections, particularly in viral diseases such as SARS-CoV-2 and acute renal failure, and acute cardiogenic edema that cause widespread pulmonary involvement. Therefore, hospitalization and close monitoring are recommended for these asthma patients. Our study revealed that one in five patients with asthma as a comorbid condition admitted to the ICU with respiratory failure required intubation, and one in ten patients died. Our study showed that in patients with asthma having higher APACHE II scores, congestive heart failure and respiratory failure requiring invasive mechanical ventilation, and COVID-19 pneumonia are associated with an increased risk of death in the ICU. Patients with asthma and those with risk factors should be closely monitored when admitted to the intensive care unit.
Conflict of Interest Statement
There is no support or financial support that occurred in the previous three years. Additionally, there are no non-financial relationships that could potentially influence the writing of the article. The authors have no conflict of interest to declare.
Funding
This article is unfunded and has “No Funding”.
Data Availability Statement
All data are presented in the paper. All data and other material are available from the corresponding author on reasonable request.
Author Contributions
I.G.E.I., Z.K, G.G. were involved in planning and supervised the work, Z.K., G.E.D, T.K, M.E.Ç. F.K.D., O.Y.M., and S.G. processed the experimental data, performed the analysis, Z., K, E.A.T. and E.A. drafted the manuscript and designed the figures. Z.K., I.G.E.I and N.A. aided in interpreting the results and worked on the manuscript. All authors discussed the results and commented on the manuscript.
Acknowledgements
We would like to thank the doctors, nurses, and staff at the ICU who closely monitored patients throughout the pandemic and worked with dedication.
References
- Aaron SD, Boulet LP, Reddel HK, Gershon AS. Underdiagnosis and Overdiagnosis of Asthma. Am J Respir Crit Care Med. 2018;198(8):1012-1020. doi:10.1164/rccm.201804-0682CI
- Mortimer K, Lesosky M, García-Marcos L, et al. The burden of asthma, hay fever and eczema in adults in 17 countries: GAN Phase I study. Eur Respir J. 2022;60(3):2102865. Published 2022 Sep 15. doi:10.1183/13993003.02865-2021
- Murphy KR, Solis J. National Asthma Education and Prevention Program 2020 Guidelines: What’s Important for Primary Care. J Fam Pract. 2021;70(6S):S19-S28. doi:10.12788/jfp.0219.
- Reddel HK, Bacharier LB, Bateman ED, et al. Global Initiative for Asthma Strategy 2021: Executive Summary and Rationale for Key Changes. Am J Respir Crit Care Med. 2022;205(1):17-35. doi:10.1164/rccm.202109-2205PP
- Bloom CI, Palmer T, Feary J, Quint JK, Cullinan P. Exacerbation Patterns in Adults with Asthma in England. A Population-based Study. Am J Respir Crit Care Med. 2019;199(4):446-453. doi:10.1164/rccm.201808-1516OC.
- Gupta D, Keogh B, Chung KF, et al. Characteristics and outcome for admissions to adult, general critical care units with acute severe asthma: a secondary analysis of the ICNARC Case Mix Programme Database. Crit Care. 2004;8(2):R112-R121. doi:10.1186/cc2835.
- Gibbison B, Griggs K, Mukherjee M, Sheikh A. Ten years of asthma admissions to adult critical care units in England and Wales. BMJ Open. 2013;3(9):e003420. Published 2013 Sep 19. doi:10.1136/bmjopen-2013-003420.
- Stow PJ, Pilcher D, Wilson J, et al. Improved outcomes from acute severe asthma in Australian intensive care units (1996 2003). Thorax. 2007;62(10):842-847. doi:10.1136/thx.2006.075317The Global Burden of Disease. The Global Asthma Report 2018: Asthma Mortality.
- McFadden ER Jr. Acute severe asthma. Am J Respir Crit Care Med. 2003;168(7):740-759. doi:10.1164/rccm.200208-902SO.
- Althoff MD, Holguin F, Yang F, et al. Noninvasive Ventilation Use in Critically Ill Patients with Acute Asthma Exacerbations. Am J Respir Crit Care Med. 2020;202(11):1520-1530. doi:10.1164/rccm.201910-2021OC.
- Abdelkarim H, Durie M, Bellomo R, et al. A comparison of characteristics and outcomes of patients admitted to the ICU with asthma in Australia and New Zealand and United states. J Asthma. 2020;57(4):398-404. doi:10.1080/02770903.2019.1571082.
- Al-Dorzi HM, Al-Shammary HA, Al-Shareef SY, et al. Risk factors, management and outcomes of patients admitted with near fatal asthma to a tertiary care hospital in Riyadh. Ann Thorac Med. 2014;9(1):33-38. doi:10.4103/1817-1737.124441.
- Burns KE, Adhikari NK, Keenan SP, Meade MO. Noninvasive positive pressure ventilation as a weaning strategy for intubated adults with respiratory failure. Cochrane Database Syst Rev. 2010;(8):CD004127. Published 2010 Aug 4. doi:10.1002/14651858.CD004127.pub2.
- Shapiro JM. Intensive care management of status asthmaticus. Chest. 2001;120(5):1439-1441. doi:10.1378/chest.120.5.1439.
- Expert Panel Working Group of the National Heart, Lung, and Blood Institute (NHLBI) administered and coordinated National Asthma Education and Prevention Program Coordinating Committee (NAEPPCC), Cloutier MM, Baptist AP, et al. 2020 Focused Updates to the Asthma Management Guidelines: A Report from the National Asthma Education and Prevention Program Coordinating Committee Expert Panel Working Group [published correction appears in J Allergy Clin Immunol. 2021 Apr;147(4):1528-1530. Doi: 10.1016/j.jaci.2021.02.010.]. J Allergy Clin Immunol. 2020;146(6):1217-1270. doi:10.1016/j.jaci.2020.10.003
- Kao CC, Jain S, Guntupalli KK, Bandi V. Mechanical ventilation for asthma: a 10-year experience. J Asthma. 2008;45(7):552-556. doi:10.1080/02770900801999090.
- Mahdavinia M, Foster KJ, Jauregui E, et al. Asthma prolongs intubation in COVID-19. J Allergy Clin Immunol Pract. 2020;8(7):2388-2391. doi:10.1016/j.jaip.2020.05.006.
- Dolby T, Nafilyan V, Morgan A, Kallis C, Sheikh A, Quint JK. Relationship between asthma and severe COVID-19: a national cohort study. Thorax. 2023;78(2):120-127. doi:10.1136/thoraxjnl-2021-218629
- Venkatesan P. 2023 GINA report for asthma. Lancet Respir Med. 2023;11(7):589. doi:10.1016/S2213-2600(23)00230-8
- Yıldız F, Oğuzülgen IK, Dursun B, et al. Turkish Thoracic Society asthma management and prevention guideline: key points. Tuberk Toraks. 2011;59(3):291-311.
- Wu F, Zhao S, Yu B, et al. A new coronavirus associated with human respiratory disease in China [published correction appears in Nature. 2020 Apr;580(7803):E7. doi: 10.1038/s41586-020-2202-3.]. Nature. 2020;579(7798):265-269. doi:10.1038/s41586-020-2008-3
- Lu R, Zhao X, Li J, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395(10224):565-574. doi:10.1016/S0140-6736(20)30251-8
- Lodeserto FJ, Lettich TM, Rezaie SR. High-flow Nasal Cannula: Mechanisms of Action and Adult and Pediatric Indications. Cureus. 2018;10(11):e3639. Published 2018 Nov 26. doi:10.7759/cureus.3639
- ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526-2533. doi:10.1001/jama.2012.5669
- Nava S, Hill N. Non-invasive ventilation in acute respiratory failure. Lancet. 2009;374(9685):250-259. doi:10.1016/S0140-6736(09)60496-7
- Sessler CN, Gosnell MS, Grap MJ, et al. The Richmond Agitation-Sedation Scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166(10):1338-1344. doi:10.1164/rccm.2107138