





Neuro-Rehabilitation of Soleus Muscles in Older Adults
Neuro-Rehabilitation of the Soleus Muscles: Restoring Optimal Diastolic Blood Pressure in Older Adults
Kenneth J. McLeod, Ph.D. 1
- Sonostics, Inc.
OPEN ACCESS
PUBLISHED: 31 January 2026
CITATION: McLeod, KJ., 2026. Neuro-Rehabilitation of the Soleus Muscles: Restoring Optimal Diastolic Blood Pressure in Older Adults. Medical Research Archives, [online] 14(1).
COPYRIGHT © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ISSN 2375-1924
ABSTRACT
Diastolic blood pressure declines after age 50 such that older adults commonly have a diastolic pressure well below the optimal range of 75-90mmHg, resulting in increased risk of all-cause mortality, cognitive impairment, heart disease, and cancer. The cause of the age-related diastolic pressure decline is not well understood. We propose diastolic blood pressure declines with age primarily due to decreased venous return resulting from soleus muscle atrophy. Neuro-rehabilitation of the soleus muscles in older adults has the potential to improve venous return thereby enhancing resting cardiac output, and correspondingly, optimizing diastolic blood pressure. In a repeated measures prospective clinical trial, subjects (N=25, age 75.7±7.2 years) underwent daily, non-invasive, soleus muscle neuro-rehabilitation for six months, initiated through plantar nerve modulation. Average soleus muscle fatigue strength increased more than 2x over the six months resulting in an average 0.4 L/min/m2 increase in resting cardiac index (range 0.1-0.8 L/min/m2; p=0.003). This enhanced cardiac output led to an average rise in resting diastolic blood pressure of 8mmHg, from 63.5mmHg to 71.5mmHg (p=0.001) in subjects not undergoing hypertension therapy. Extrapolation indicated that optimal (>80mmHg) diastolic blood pressure could be achieved, on average, with approximately one year of daily neuro-rehabilitation. These results provide confirmation that decreased venous return resulting from soleus muscle atrophy plays a significant role in the age-related decline in diastolic blood pressure, though overmedication and polypharmacy also play significant roles. These results provide support for neuro-rehabilitation of the soleus muscles as a convenient and non-invasive means to create substantial clinical benefits in older adults by reducing the numerous health complications arising from chronically low cardiac output and diastolic blood pressure.
Keywords
- Diastolic Blood Pressure
- Soleus Muscle
- Neuro-Rehabilitation
- Older Adults
- Cardiac Output
Introduction
Hypertension (brachial blood pressure >130/80mmHg) is widely considered a significant risk factor for cardiovascular disease in young and middle-aged adults. However, for older adults, there is growing recognition that “elevated” blood pressures can have substantial beneficial health effects. Over 25 years ago, Boshuizen, et al. reported that for adults over age 85 years, systolic blood pressures in the 140-160mmHg were associated with reduced all-cause mortality compared to “normotensive individuals.” Further, they observed that diastolic blood pressure (DBP) in the 80-95mmHg range was associated with significantly reduced risk of all-cause mortality as well as decreased rates of cognitive impairment, heart disease, and cancer, compared to those with lower DBPs. Extending these observations, Post-Hospers, et al., followed subjects aged 65 years and older for up to 16 years and observed that low DBP was strongly associated with increased all-cause mortality in the elderly. Hazard risks as high as 2x were found for individuals with low physical functioning and DBPs of 70mmHg or lower, compared to those with DBPs of 71-90mmHg. These investigators posited that DBP was more important than systolic blood pressure in determining tissue perfusion levels, and as a result, all-cause morbidity and mortality risk. This observation was confirmed by Haring, et al. who reported all-cause mortality in women over age 70 years to be significantly increased in those with DBPs below 75mmHg. Masoli, et al. addressed whether the observed increase in mortality at low blood pressure levels could be a reverse causation effect resulting from the decline in blood pressure which typically occurs in the last few years before death. They dismissed this hypothesis by showing that systolic blood pressure levels ranging from 130mmHg to 180mmHg were associated with the lowest all-cause mortality rates in both non-frail and frail adults aged 75-85 years. Lian, et al. have shown that reduced morbidity and mortality at mild hypertensive levels is not limited to the western world, but is also found in south Asian populations. Filippone, et al., in a thorough review of the clinical research addressing the issue of optimal DBP levels, identify a convergence in the literature pointing to an optimal DBP range of 75-85mmHg. Most recently, a review of mortality data for 10,000 hypertensive individuals in the National Health and Nutrition Examination Survey (1999-2018) found that all-cause mortality was significantly (p<0.001) reduced in those with diastolic blood pressures in the 80-90mmHg range compared to those with diastolic pressures of <60mmHg, or in the 60-80mmHg range.
The growing recognition that morbidity and mortality risks can be minimized in older adults by maintaining DBP levels in the elevated to mild hypertensive range (75-90mmHg) represents a critical health insight for geriatric medicine given the ubiquity of chronic low blood pressure in this population. Wright, et al. summarized blood pressure reference levels based on 2001-2008 National Health and Nutrition Examination Survey (NHANES) data. This dataset reports resting blood pressure recordings obtained per American Heart Association standards (seated for at least five minutes, arm at heart height, average of at least two measurements obtained two minutes apart, etc. DBP was found to decline continuously in both men and women after age 50, such that by age 60 mean DBP levels were less than 80mmHg, independent of whether the individual was taking hypertension medications. By the ninth decade, mean DBP levels were 65mmHg or less independent of therapeutic status. Reanalyses using the 2011-2018 NHANES data have confirmed these observations. These data demonstrate that the majority of adults over age 60 are at significantly increased risk of health complications as a result of living with below optimal resting diastolic blood pressure levels.
Age related changes in blood pressure are often attributed to arterial stiffening. Years of pulsatile arterial flow leads to fatigue and fracture of vessel wall elastin, as well as vessel diameter expansion and wall thickening, resulting in increased stiffness particularly in the aorta and its major proximal branches. This outcome can explain the rise in systolic pressure which occurs during aging, but the decline in DBP after age 50 is less well understood. That a stiffened aorta can limit volume expansion during systole can, in part, explain a portion of the DBP decline. However, DBP decline after age 50 occurs in normotensive individuals at essentially the same rate as in hypertensive individuals, pointing to an alternative process dominating the age-related decline in DBP.
An important contributing factor to the age-related decline in DBP is the concurrent decline in cardiac output (CO). Blood pressure is equal to the product of CO and peripheral vascular resistance, and so a decline in CO will lead to a drop in blood pressure in the absence of compensatory adaptation through increased vascular resistance. While the age-related decline in CO has been known to occur for almost 100 years, it was not until indicator dilution methods were developed that this decline became well quantified. Brandfonbrener, et al. first showed that CO in the supine individual declined linearly from approximately 7 L/min at age 20 to approximately 3 L/min by age 90. Katori confirmed these results, measuring CO in a semi-reclined position in male and female subjects spanning the 4-78 year old age range. Katori observed that CO peaked in the late teen years at an average level of about 7L/min, then declined at a linear rate of 0.045 L/min/year. More recently, Middlemiss, et al. utilized non-invasive techniques to assess cardiovascular hemodynamics across the adult age range. This group also found, for subjects in the supine position, CO declining by approximately 40% over the 20-70 age range, principally due to reduced stroke volume. Peripheral vascular resistance roughly doubles over this age range, resulting in the maintenance of average systolic pressure. However, they observed that even in relatively young subjects (average age of 27 years) a 20% decline in CO occurred when subjects transitioned to a seated position from supine, and an additional 10% decline when subjects transitioned from sitting to standing. This postural decline in CO results from the drop in venous return to the heart due to uncompensated gravity driven fluid pooling. The challenge of maintaining CO in the upright posture leads us to suggest that the age-related decline in cardiac output primarily reflects a progressive loss in the ability to maintain venous return during orthostasis. Our previous work has shown that older adults become progressively less able to compensate for gravity driven fluid pooling when in quiet upright posture. Specifically, CO was observed to fall by over 35% in older adults during extended quiet sitting. As venoconstriction of the leg veins does not make a significant contribution to venous return, maintenance of venous return in quiet upright posture depends primarily on skeletal muscle pumping. Correspondingly, we propose that the inability of older adults to maintain cardiac output during quiet sitting, the predominant activity for most older adults during their waking day, is due to a reduction in lower limb skeletal muscle pumping activity. During quiet sitting, the soleus muscles dominate lower limb skeletal muscle pumping. Soleus muscle activity during quiet sitting has been shown to be significantly enhanced through non-invasive neuro-modulation, resulting in increased cardiac output. Here, we investigate whether long-term, non-invasive neuro-modulation is capable of rehabilitating soleus muscles which have atrophied due to age, and produce a sustained increase in resting cardiac output and diastolic blood pressure in older adults. Such an outcome would offer a convenient means for maintaining resting blood pressure in the optimal range in older adults, substantially reducing morbidity and mortality risks in this population.
Materials and Methods
We undertook a six-month, prospective, repeated measures, clinical trial utilizing an electromechanical intervention to modulate plantar nerve activity through stimulation of the Meissner’s Corpuscles (mechano-receptive plantar nerve endings) on the soles of the feet. All procedures were performed according to the Declaration of Helsinki by personnel certified in human subject’s research standards. The protocol was approved by Pearl Pathways Institutional Review Board (ID# 2023-0306; Fishers, IN, USA), and undertaken within the Clinical Research Laboratory at Sonostics, Inc. in Endicott, NY.
SUBJECT RECRUITMENT
Older adult men and women (age 65-95 years) were recruited for the study through referral by collaborating physicians, outreach through community organizations, and word of mouth. Primary inclusion criterion was that the subjects were experiencing at least one symptom associated with chronic low cardiac output or the fluid pooling associated with insufficient venous return (swollen feet/ankles, nighttime leg cramps, chronically cold hand/feet, chronic fatigue, dizziness, or subjective cognitive impairment). Exclusion criteria were having a cardiac pacemaker (precluding CO assessment by electrical impedance plethysmography), a diastolic blood pressure above 80mmHg, a cardiac index below 1.8 L/min/m2 (indicator of potential heart failure), inability to stand without assistance, inability to utilize the study intervention for at least one hour per day, or unable to return for follow-up assessments on a monthly basis for six months. Recruited subjects were asked to report their medication schedule, specifically focusing on medications which would affect, either directly or indirectly, cardiovascular function. Subjects were not excluded from the study based on medication usage. Subjects were requested to initiate Vitamin D supplementation if they were not already supplementing their diet, as Vitamin D is a known mediator of muscle fiber regeneration.
ASSESSMENTS
Cardiovascular hemodynamics were assessed using the Cheetah Non-Invasive Cardiac Output Monitor (NICOM; Baxter, Inc. Vancouver, WA). NICOM provides beat-to-beat assessment of stroke volume and heart rate by electrical impedance plethysmography, with averaged cardiac output assessments reported every 30 seconds, along with cardiac index (cardiac output divided by body surface area). NICOM also provides brachial blood pressure measurements every three minutes. Impedance plethysmography was completed with the stimulation and recording electrodes attached to the upper and lower back of the subjects, with the subjects transitioning from a standing to a seated position at the start of the recording period. Subjects were seated in an electrically powered armchair, permitting adjustment to ensure the subjects feet were firmly positioned on the floor. Neuro-modulation intervention was not utilized during the recording period. Cardiovascular hemodynamics were monitored for 30 minutes. Subjects were asked to minimize speaking and movement during the recording period. Pilot study data demonstrated a coefficient of variation for the cardiac output measurements of about 10%, and correspondingly, power calculations for 95% confidence and an allowable error of 5% indicated that a minimum of 16 subjects would need to complete the study. Assuming a non-completion rate of 50%, we focused on recruiting at least 30 subjects.
Soleus muscle fatigue strength was assessed using the standard one-legged standing heel raise test on a 10o wedge. Subjects were allowed to use their fingertips to balance themselves on a wall while completing the heel raises. The assessment involved a one-second heel raise (concentric contraction), a brief pause (isometric contraction), and a one second lowering (eccentric contraction) phase, resulting in a cycle time of about 2 seconds. Heel raise cycles were continued to exhaustion, with the assessment completed for both legs. Average of left and right leg were utilized in the analysis. If injury prevented testing of both legs, results from a single leg were used in the data analysis.
INTERVENTION
Following screening and acceptance into the study, subjects were provided with an intervention device to be used in the home or workplace per subject preference. The intervention device (HeartPartner; Sonostics, Inc., Endicott, NY) provided a 45 Hz, 100 m mechanical displacement to the frontal plantar surface of the foot, sufficient to activate the Meissner’s Corpuscles, initiating a reflex response resulting in contraction of the soleus muscles (see McLeod, 2024 for a detailed description). The device induces periodic contractions to ensure sufficient time for the soleus muscles to refill with blood and lymphatic fluid between muscle contractions. Subjects were provided with an electronic power monitor to track device usage over the study period, with subjects returning the monitor at each monthly follow-up visit so that average usage time could be recorded.
PROCEDURES
After obtaining Informed consent, self-reported age, weight, height, gender, ethnicity, and educational level were collected from each subject, along with a brief health history to identify any health complications commonly associated with lower limb fluid pooling, low cardiac output, or hypotension. In addition, subjects were asked to report any medication for hypertension or which could indirectly influence the cardiovascular system through diuretic effects. Cardiac output, blood pressure, heart rate, and cardiac index, were assessed over the course of 30 minutes with the subject seated quietly. The penultimate DBP recording obtained was used to define resting DBP. The last three minutes of cardiac index recordings were averaged to define the resting cardiac index level. Soleus fatigue strength was assessed with the subjects wearing rubber-soled shoes. Subjects returned each month for follow-up assessments over the course of six months. Analysis of the relationships between age, soleus fatigue strength, resting cardiac index, and resting diastolic blood pressure, included all subjects screened for the study. Analysis of the effects of intervention were undertaken on the subjects completing the study protocol. All statistical analyses were performed using Origin 2024b (Origin Labs, Northhampton, MA). Single and multiple linear regression analyses were utilized to determine time rate of change of the physiologic measures as well as for determining relationships between measured outcome variables and demographic parameters. Missing data points were not imputed. p values < 0.05 were interpreted as reflecting significant change.
Results
Thirty-two volunteers were screened for the study. All screened subjects were from the Southern Tier region of New York, and were predominantly of European ethnicity. One potential subject was excluded from the study due to having an initial resting diastolic blood pressure exceeding 80mmHg. Of the 31 subjects enrolled, six did not complete the protocol due to relocation, health issues unrelated to the study, or time conflicts precluding follow-up appointments. No adverse effects associated with use of the intervention were reported. Eleven men and fourteen women completed the study protocol. Subject age spanned 65-92 (mean 75.7±7.1) years. The majority of subjects reported at least one cognitive health concern such as memory loss or difficulty concentrating. In addition, dizziness, cold extremities, chronic fatigue, chronic pain, nighttime leg cramps, and swollen lower extremities, were commonly reported. Fourteen of the twenty-five subjects completing the study protocol reported taking medications which influence the cardiovascular system either directly (i.e. hypertension medications) or indirectly (medications with diuretic effects).
Soleus muscle fatigue strength of the screened individuals (N=32;
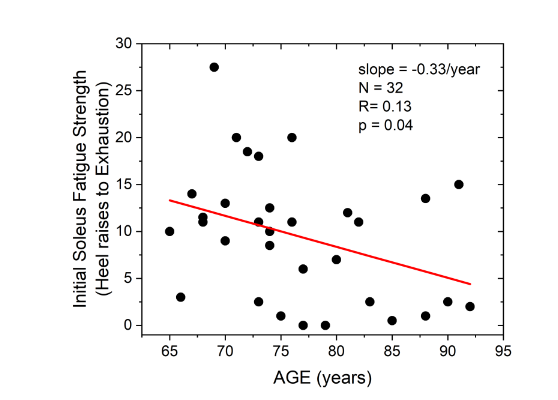
) ranged from zero (two subjects) to 27.5 (one subject) one-legged standing heel raises, with an average of 9.2. Age was a significant (p=0.04) predictor of soleus muscle fatigue strength, with fatigue strength declining at a rate of 0.33 heel raises per year of age, such that fatigue strength declined from an average of 13 heel raises at age 65 to an average of 5 heel raises at age 90 years. Stepwise elimination multiple regression analysis of soleus fatigue strength against age, weight, height, gender, and education, demonstrated that age was the only significant predictor of soleus fatigue strength.
Cardiac index (CI) levels in the screened population ranged from 1.8 to 3.4 L/min/m2, with an average of 2.47±0.35 L/min/m2. Multiple linear regression analysis of CI against age, body mass, body height, gender and education showed that only soleus fatigue strength was a significant predictor of CI with a regression coefficient of 0.024 (S.E. 0.008) L/min/m2/Heel raise; p=0.004 (
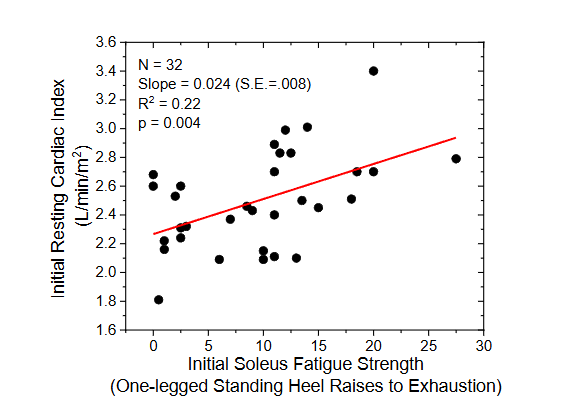
). Correspondingly, over the range of soleus fatigue strengths observed among the screened individuals (i.e. 0-30), CI increased, on average, approximately 36%, from 2.2 L/min/m2 to about 3.0 L/min/m2.
Initial resting diastolic blood pressure (DBP) of screened individuals ranged from 55mmHg to 84mmHg, with an average of 67.8±7.7mmHg. Resting DBP was significantly correlated to resting cardiac index (regression coefficient of 9.69 (s.e. 3.75) mmHg/L/min/m2; p=0.01;
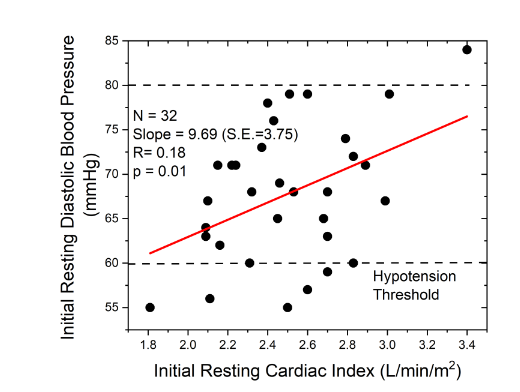
). Following 30 minutes of quiet sitting, seven screened individuals had a resting diastolic pressure of 60mmHg or less, a level commonly defined as clinically hypotensive. Only one screened subject had a resting DBP over 80mmHg, and as well, had the highest resting CI level. Stepwise elimination multiple linear regression analysis of resting DBP against age, body height, body weight, gender, education, soleus fatigue strength, and cardiac index, demonstrated that cardiac index was the only significant predictor of DBP.
Univariate regression analysis of DBP against CI indicated that for older adults, a CI of 3-4 L/min/m2 would be necessary, on average, to support a resting DBP of 80mmHg. Correspondingly, per the data presented in Figure 2, to achieve a CI of 3-4 L/min/m2 would require, on average, that the subjects be capable of completing at least 30 one-legged heel raises.
All subjects participating in the study utilized the intervention device in their home, usually while watching television. Several subjects were employed and used their device at their workplace as well. Seven of the enrolled subjects opted not to use the electronic power monitor, and so device usage times were available for only 19 subjects. Averaged over the six-month study duration, device usage time ranged from 0.95 hours/day to 5.34 hours per day, with an average of 3.07 (±1.30) hours per day (
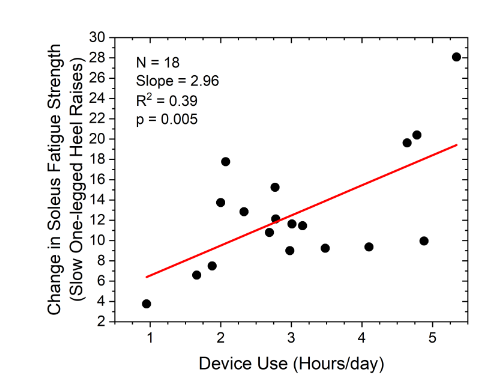
).
Subjects completing the study all experienced an increase in soleus muscle fatigue strength, with fatigue strength improvements ranging from 4 to 28 heel raises over the six month study period. Average soleus fatigue strength increased with increased device usage time (coefficient=2.96; p=0.005). One hour per day of device usage was associated, on average, with a 6 count improvement in number of heel raises over six months, while those using the device for 5 hours/day achieved, on average, an 18 count increase in number of heel raises completed during an assessment. Average rate of increase was 1.9 heel raises per month, so for the average starting soleus fatigue strength of 9.2 heel raises, about 12 months of intervention would be required to achieve the minimum of 30 heel raises estimated to be necessary to support a cardiac index of 3-4 L/min/m2 and a DBP of 80mmHg. The change in soleus strength intercept was not significantly different from zero, consistent with learning effects being a non-significant contributor to this assessment.
Cardiac index (CI) increased in each subject over the course of the study (
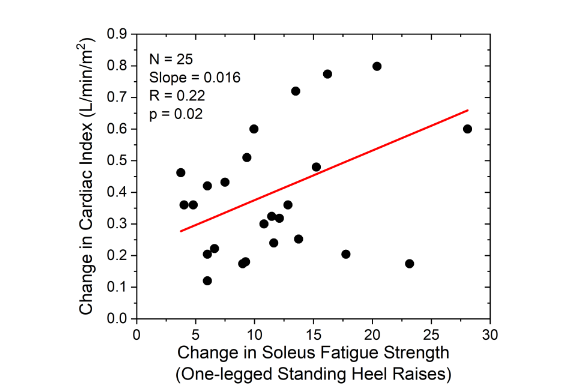
). The CI increase ranged from less 0.1 L/min/m2 to over 0.8 L/min/m2 (average of 0.39 L/min/m2). The average change in CI was significantly related to the change in soleus fatigue strength (regression coefficient of 0.016 L/min/m2; p=0.02). The CI intercept of 0.22 L/min/m2 (p = 0.01) indicates that the CI increase was the result of one or more additional factors beyond improvement in soleus fatigue strength. Multiple regression analysis identified no significant demographic factor capable of explaining the increase in CI in the absence of increased soleus fatigue strength, and learning effects were not considered a plausible explanation for this non-zero intercept. Average rate of CI increase was 0.064 L/min/m2/month indicating that about 13 months of intervention would be required to increase average cardiac index the starting level of 2.2 L/min/m2 to a level of 3 L/min/m2 or higher.
Average DBP levels increased significantly in response to increased CI (16.1 mmHg/L/min/m2; N = 25; p = 0.002) (
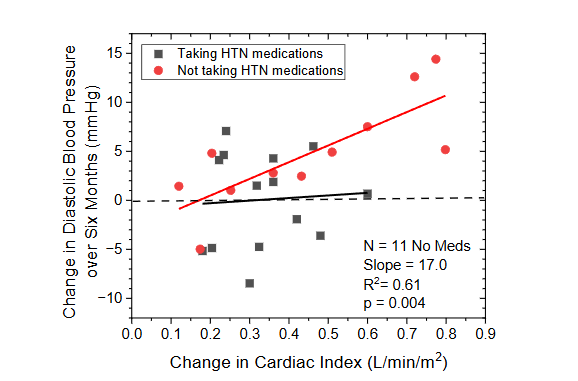
). However, declines in DBP over the six month study period were observed in seven subjects. Medication review showed that of the subjects experiencing declines in DBP, six were taking medications which directly, or indirectly, affect the cardiovascular system (CVS). Separating the DBP response into subgroups reflecting those taking hypertension medication, or other medications known to influence the CVS, and those not taking such medications, identified two distinct responses. Those subjects not taking CVS affecting medications demonstrated a robust linear response to changes in CI, with DBP rising 17mmHg for each 1L/min/m2 increase in CI (p=0.004), with an intercept not significantly different from zero. Conversely, subjects taking CVS affecting medication showed no improvement in average DBP, and no change in DBP related to changes in CI.
Analysis of temporal trend data illustrates the magnitude of DBP change achieved through neuro-rehabilitation of the soleus muscles. DBP in the non-medicated subgroup increased at a rate of 1.27 mmHg per month (p = 0.001;
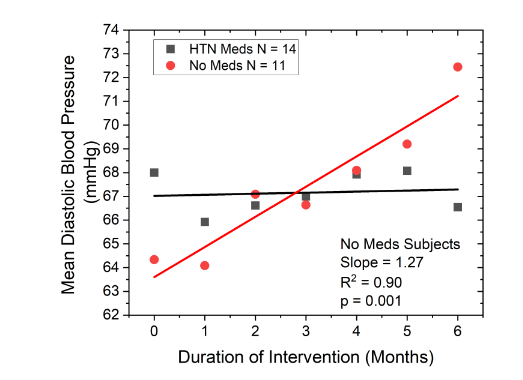
). Starting at an average of about 63mmHg, average DBP for this group increased to over 71 mmHg over the six month study period. Extrapolating over time, this rate of increase suggests that 14 months of intervention would be required to restore DBP into the optimal range (>80mmHg) presuming soleus muscle function and cardiac output continued to improve at the rate observed during the first six months of intervention.
Discussion
Low resting diastolic blood pressure (DBP) remains a commonly occurring, yet poorly understood, aspect of aging even though it is associated with a wide range of severe health complications in older adults, up to and including increased risk of all-cause mortality. As a major goal of healthcare is to increase quality adjusted life years of the population, understanding and preventing the age related decline in DBP has the potential to significantly improve the healthcare of older adults. Here, we have addressed the question of whether a principal cause of low DBP in older adults is soleus muscle atrophy. Soleus atrophy arises from disuse, and results in reduced venous return, and as a direct consequence, reduced cardiac output. Chronically low cardiac output can lead to declining blood pressure in older adults, particularly during quiet upright posture, limiting the blood perfusion necessary to prevent tissue and organ failure. The results obtained here lend substantial support to this hypothesis.
In our older adult subject group, average soleus fatigue strength (9.2 one-legged standing heel raises) was remarkably similar to values reported by others. For example, Whyte, et al. observed that healthy 65-80 year olds could complete an average of 9.5 slow heel raises. In comparison, Hebert-Losier reported that 20-year-old men and women could complete an average of 37 heel raises before exhaustion, suggesting a four-fold decrease in soleus muscle fatigue strength occurring over the adult life span. We observed a significant, 0.33 heel raises/year decline in soleus fatigue strength, with the average at age 90 years being less than 5 heel raises. Extrapolating back in time predicted that a 20 year old would have a soleus fatigue strength of about 28 heel raises, similar to the value reported by Hebert-Losier. This seems to indicate that the decline in soleus fatigue strength continues at roughly a constant rate from age 20 onward. This observation is consistent with the rapid decline in vigorous physical activity levels which has been shown to begin in young adulthood.
Average initial cardiac index in our study population (2.2 L/min/m2) was on the low end of normative values for healthy older adults (2.1-3.2 L/min/m2). However, our cardiac index recordings were obtained in an upright seated position, and our subjects were specifically selected based on having at least one health symptom related to lower body fluid pooling, low resting cardiac output, or low blood pressure. A lower average cardiac index level, therefore, would be expected. Cardiac index was found to be strongly correlated to soleus fatigue strength (p=0.004) consistent with the fact that cardiac output is critically dependent on venous return, and soleus muscle pumping is essential for maintaining venous return in quiet upright posture.
While a study exclusion criterion was having a diastolic blood pressure (DBP) above 80mmHg, only one screened subject was excluded on this basis. Subject selection for this trial included the fact that the individuals were experiencing one or more symptoms of hypotension, which may have biased the study population. However, if our study group is at all representative of the older adult demographic, the vast majority of those aged 65 years and old would appear to living with below optimal diastolic blood pressure (DBP). Further, seven of the 32 screened subjects had a resting DBP below 60mmHg; a level considered to be clinically hypotensive. This leads us to suggest that 20% or more of the older adult population may be at greatly increased risk of falls and injury in addition to the longer term consequences of chronically low DBP.
The correlation between DBP and cardiac index indicates that a cardiac index in the 3-4 L/min/m2 range is necessary to maintain a DBP of 80mmHg in this age group. That this is the typical cardiac index of a young adult adds confirmation to the validity of this estimate. As well, these values indicate that the relationship between cardiac index and diastolic blood pressure does not change substantially over the adult life span. In addition, the relationship we observed between soleus fatigue strength and cardiac index leads us to estimate that the ability to complete 30, or more, one-legged standing heel raises is necessary to support a cardiac output of 3 L/min/m2. This is also remarkably consistent with the fact that young adults, who typically maintain a cardiac index in the range of 3.5 L/min/m2 have an average soleus fatigue strength of about 37.
Daily neuro-modulation of the plantar nerves resulted in a dose-dependent rehabilitation of the soleus muscles, and correspondingly, improved soleus muscle function resulted in significant increases in resting cardiac output. Regression analysis on these data indicate a non-zero intercept, such that in the case of no improvement in soleus fatigue strength, cardiac output appeared to increase significantly, by 0.22 L/min/m2. We interpret this outcome to be a reflection of the fact that daily soleus muscle activation, leading to increased venous return for several hours per day, was sufficient to significantly improve cardiac ejection fraction through the Frank-Starling mechanism. Forced increases in venous return, for example through sequential pneumatic compression, has previously been shown to improve ejection fraction over time and it is possible that this same phenomenon has occurred in our study.
Consistent with our working hypothesis, initial resting DBP in the non-medicated subgroup was significantly correlated with resting cardiac index levels, and similar to cardiac index and soleus fatigue strength, DBP demonstrated a continuous increase over time. In addition, the temporal relationships between these three parameters were remarkably consistent. That is, we estimate it would require about 12 months of intervention for the average study subject to achieve a soleus fatigue strength permitting 30 or more heel raises in a single bout. Similarly, the time to achieve a 3 L/min/m2 cardiac index was estimated to be about 13 months, and the time to achieve a resting DBP of 80mmHg was estimated at about 14 months. This pattern of recovery times supports the causal mechanism we have hypothesized, and as well, suggests the presence of a short physiologic delay time in the adaptation process as the body adjusts to the changes initiated by neuro-rehabilitation of the soleus muscles.
The large suppressive effect of hypertension medications, and other medications which affect body hydration, on DBP was not anticipated. While the objective of hypertension therapy is to reduce blood pressure, we did not expect the ability of such medications to prevent any rise in DBP in the presence of significant increases in cardiac output, without a change in medication dosage. Inhibiting the change in blood pressure means that vascular resistance must have dropped in direct proportion to the increase in cardiac output. Over 250 medications are known to lead to hypotension, commonly through reduction in body hydration. This can occur as a result of increased urine volume, increased sweat production, decreased thirst sensation, decreased appetite, or combinations of these outcomes due to polypharmacy. While we only asked our subjects about the use of cardiovascular and anxiety/depression medications, several did provide us with their complete medication list and we found that these subjects were taking 12 or more medications and supplements daily, so polypharmacy effects are a possibility. That many medications reduce body hydration provides a possible explanation for the decrease in vascular resistance which occurred in direct proportion to the increase in cardiac output. With the shift of fluid from lower body soft tissues into the vascular system, due to increased skeletal muscle pumping, interstitial tissue pressures would drop. Decreased hydrostatic tissue pressure would permit passive expansion of the arterioles and capillary beds in the lower body, significant contributors to vascular resistance.
Limitations of this study include the relatively small sample size, in particular after the study group was separated into the medicated and non-medicated subgroups. Nonetheless, regression coefficients for many of the critical relationships (e.g. DBP vs cardiac index; DBP vs time) are relatively robust. In addition, the medication regimen for each subject was self-reported and so possibly inaccurate. Requiring subjects to bring in all of their medications when enrolling in such a study would likely be worthwhile to reduce reporting errors. Finally, the six-month study duration was relatively short. While the duration permitted testing of our underlying hypothesis, a longer study would have permitted addressing additional sub-hypotheses such as whether medicated subjects experience the benefits of soleus rehabilitation, but with a slower recovery rate. Features of this study include the repeated measures design, which allowed each subject to serve as their own control, thereby improving sensitivity, and the use of monthly follow-up assessments, which permitted more accurate determination of the physiologic changes over time despite the presence of large natural variations.
Conclusions
In summary, soleus muscle pumping plays a critical role in maintaining resting cardiac output in older adults, and correspondingly, diastolic blood pressure (DBP). However, soleus fatigue strength declines throughout adulthood, leading to declines in both cardiac output and DBP in a large fraction of the older adult population. Plantar nerve modulation is capable of rejuvenating the soleus muscles, resulting in full rehabilitation in an estimated 12 months. Soleus rehabilitation leads directly to a sustained increase in resting cardiac output and DBP, at least in individuals who are not taking hypertension medications, or other medications with diuretic action. Returning DBP to optimal levels (75-90mmHg range) in the older adult is estimated to require just over one year of neuro-rehabilitation therapy. Neuro-rehabilitation of the soleus, combined with limiting, whenever possible, medications, or polypharmacy, which can dehydrate the older patient, could become a convenient and effective strategy for eliminating chronic diastolic hypotension in older adults, and result in substantially reduced mortality and morbidity in this population.
Conflict of Interest
The author serves as Chief Science Officer for Sonostics, is a patent holder on neuro-modulation technologies, and holds an equity interest in Sonostics, Inc.
Funding
This study was supported by Sonostics, Inc.
Acknowledgements
The author would like to acknowledge the assistance of Drs. E. Dohner, M.E. Hoffman, and J. Perry in the recruitment of subjects for this study, as well as Mr. K. Washington who played an active role in recruitment of subjects in the community and undertook the vast majority of the subject assessments.
References
- Satoh M, Ohkubo T, Miura K, et al. Long-term risk of cardiovascular mortality according to age group and blood pressure categories of the latest guideline. Hypertens Res. 2025;48(4):1428-1433. doi:10.1038/s41440-025-02151-w.
- Boshuizen HC, Izaks GJ, van Buuren S, Ligthart GJ. Blood pressure and mortality in elderly people aged 85 and older: community based study. BMJ. 1998;316(7147):1780-1784. doi:10.1136/bmj.316.7147.1780.
- Post Hospers G, Smulders YM, Maier AB, Deeg DJ, Muller M. Relation between blood pressure and mortality risk in an older population: role of chronological and biological age. J Intern Med. 2015;277(4):488-497. doi:10.1111/joim.12284.
- Haring B, McGinn AP, Kamensky V, et al. Low Diastolic Blood Pressure and Mortality in Older Women. Results From the Women’s Health Initiative Long Life Study. Am J Hypertens. 2022;35(9):795-802. doi:10.1093/ajh/hpac056.
- Masoli JAH, Delgado J, Pilling L, Strain D, Melzer D. Blood pressure in frail older adults: associations with cardiovascular outcomes and all-cause mortality. Age Ageing. 2020;49(5):807-813. doi:10.1093/ageing/afaa028.
- Lian Q, Jafar TH, Allen JC, Ma S, Malhotra R. Association of Systolic and Diastolic Blood Pressure With All-Cause Mortality Among Community-Dwelling Older Adults: A Prospective Observational Study. J Aging Health. 2022;34(4-5):674-683. doi:10.1177/08982643211055245.
- Filippone EJ, Foy AJ, Naccarelli GV. The diastolic blood pressure J-curve revisited: An update. Am Heart J Plus. 2021;12:100065. Published 2021 Oct 28. doi:10.1016/j.ahjo.2021.100065.
- Hou W, Zheng B, Gong Y. Association between isolated low or high diastolic blood pressure with all-cause and cardiovascular mortality: evidence from NHANES (1999–2018); Journal of Hypertension 2025; 43(Suppl 1):p e202-e203, May. doi: 10.1097/01.hjh.0001117276.60303.32.
- Wright JD, Hughes JP, Ostchega Y, Yoon SS, Nwankwo T. Mean systolic and diastolic blood pressure in adults aged 18 and over in the United States, 2001-2008. Natl Health Stat Report. 2011;(35):1-24.
- Muntner P, Shimbo D, Carey RM, et al. Measurement of Blood Pressure in Humans: A Scientific Statement From the American Heart Association. Hypertension. 2019;73(5):e35-e66. doi:10.1161/HYP.0000000000000087.
- Muntner P, Jaeger BC, Hardy ST, et al. Age-Specific Prevalence and Factors Associated With Normal Blood Pressure Among US Adults. Am J Hypertens. 2022;35(4):319-327. doi:10.1093/ajh/hpab154.
- Chen FY, Lee CW, Chen YJ, et al. Pathophysiology and blood pressure measurements of hypertension in the elderly. J Formos Med Assoc. 2025;124 Suppl 1:S10-S16. doi:10.1016/j.jfma.2025.03.027.
- Franklin SS, Gustin W 4th, Wong ND, et al. Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study. Circulation. 1997;96(1):308-315. doi:10.1161/01.cir.96.1.308.
- Brandfonbrener M, Landowne M, Shock NW. Changes in cardiac output with age. Circulation. 1955;12(4):557-566. doi:10.1161/01.cir.12.4.557.
- Katori R. Normal cardiac output in relation to age and body size. Tohoku J Exp Med. 1979;128(4):377-387. doi:10.1620/tjem.128.377.
- Middlemiss JE, Cocks A, Paapstel K, et al. Evaluation of inert gas rebreathing for determination of cardiac output: influence of age, gender and body size. Hypertens Res. 2019;42(6):834-844. doi:10.1038/s41440-018-0179-1.
- Williams KJ, Ayekoloye O, Moore HM, Davies AH. The calf muscle pump revisited. J Vasc Surg Venous Lymphat Disord. 2014;2(3):329-334. doi:10.1016/j.jvsv.2013.10.053.
- McLeod KJ. Reversal of Soleus Muscle Atrophy in Older Adults: A Non-Volitional Exercise Intervention for a Changing Climate. Clin Interv Aging. 2024;19:795-806. Published 2024 May 10. doi:10.2147/CIA.S447665.
- Hainsworth R, Drinkhill MJ. Counterpoint: active venoconstriction is not important in maintaining or raising end-diastolic volume and stroke volume during exercise and orthostasis. J Appl Physiol (1985). 2006;101(4):1264-1270. doi:10.1152/japplphysiol.00561a.2006.
- Drees JA, Rothe CF. Reflex venoconstriction and capacity vessel pressure-volume relationships in dogs. Circ Res. 1974;34(3):360-373. doi:10.1161/01.res.34.3.360
- Harvey JA, Chastin SF, Skelton DA. Prevalence of sedentary behavior in older adults: a systematic review. Int J Environ Res Public Health. 2013;10(12):6645-6661. Published 2013 Dec 2. doi:10.3390/ijerph10126645
- McLeod KJ. Characterizing Soleus Muscle Response to Targeted Plantar Nerve Modulation Using Mechanomyography. Neuromodulation. 2025;28(8):1248-1254. doi:10.1016/j.neurom.2024.11.003.
- Latham CM, Brightwell CR, Keeble AR, et al. Vitamin D Promotes Skeletal Muscle Regeneration and Mitochondrial Health. Front Physiol. 2021;12:660498. Published 2021 Apr 14. doi:10.3389/fphys.2021.660498.
- Puga AM, Lopez-Oliva S, Trives C, Partearroyo T, Varela-Moreiras G. Effects of Drugs and Excipients on Hydration Status. Nutrients. 2019;11(3):669. Published 2019 Mar 20. doi:10.3390/nu11030669.
- Whyte S, Lavender H, Elam, Svantesson U. Tests of muscle function and health related quality of life in healthy older adults in Sweden. Isokinetics and Exercise Science. 2021;29. 1-7. doi:10.3233/IES-202126.
- Hébert-Losier K, Wessman C, Alricsson M, Svantesson U. Updated reliability and normative values for the standing heel-rise test in healthy adults. Physiotherapy. 2017;103(4):446-452. doi:10.1016/j.physio.2017.03.002.
- Lu Y, Yu K, Zhai M, Ma P. Age and school-segment difference in daily sedentary behavior and physical activity among student (9-23 years): a cross-sectional accelerometer-based survey. Front Pediatr. 2023;11:1202427. Published 2023 Jul 17. doi:10.3389/fped.2023.1202427.
- Cioccari L, Luethi N, Glassford NJ, Bellomo R. The normal cardiac index in older healthy individuals: a scoping review. Crit Care Resusc. 2019;21(1):9-17.
- Bickel A, Shturman A, Sergeiev M, Ivry S, Eitan A, Atar S. Hemodynamic effect and safety of intermittent sequential pneumatic compression leg sleeves in patients with congestive heart failure. J Card Fail. 2014;20(10):739-746. doi:10.1016/j.cardfail.2014.07.004.
- Bhanu C, Petersen I, Orlu M, et al. Drug-induced orthostatic hypotension: Cluster analysis of co-prescription patterns in older people in UK primary care. Pharmacoepidemiol Drug Saf. 2024;33(1):e5730. doi:10.1002/pds.5730.