





Non-Convulsive Status Epilepticus After HSV Encephalitis
Non-Convulsive Status Epilepticus Post Resolution of Herpes Simplex Virus Encephalitis: A Case Report
Shaikha Alsuwaidi1, Pournamy Sarathchandran2, Muhammad Amir Umer2, Firas Al Rawi2
- Rashid Hospital, Dubai Health, UAE
- Al Qassimi hospital, Emirates Health Services, UAE
OPEN ACCESS
PUBLISHED: 31 October 2025
CITATION: Alsuwaidi, S., Sarathchandran, P., et al., 2025. Non-Convulsive Status Epilepticus Post Resolution of Herpes Simplex Virus Encephalitis: A Case Report. Medical Research Archives, [online] 13(10). https://doi.org/10.18103/mra.v13i10.7046
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i10.7046
ISSN: 2375-1924
Abstract
Herpes simplex virus encephalitis, resulting from an infection by the herpes simplex virus, manifests with a spectrum of neurological symptoms, including altered mental status and seizures. Despite the administration of timely diagnosis and antiviral treatment, a significant number of individuals endure persistent morbidity. While the literature has documented post-acute seizures and epilepsy, reports on non-convulsive status epilepticus following the resolution of the acute phase are infrequent. This article describes a rare case presentation where a 55-year-old male presents with non-convulsive status epilepticus eight months following treatment of HSVE. The case report delineates his clinical presentation, supported by computed tomography (CT) and magnetic resonance imaging (MRI) of the brain, along with electroencephalogram (EEG) findings. Detection of nonconvulsive status early and proper optimization of antiepileptic medications helped early clinical recovery.
Keywords:
Non-convulsive status epilepticus, non-convulsive seizures, Herpes simplex virus encephalitis, post encephalitic epilepsy, herpes-simplex virus
Introduction
Herpes simplex virus (HSV) is the most common identified cause of encephalitis in developed countries, and is it mainly caused by herpes virus type-1 and occasionally by herpes virus type-2.1 A presumed mechanism for herpes simplex virus encephalitis (HSVE) involves the virus infiltrating the olfactory nerves, spreading through the olfactory pathway to the orbitofrontal and mesial temporal lobes. Moreover, the virus lays dormant in the anterior and middle cranial fossa, and may travel through cell-to-cell contact to invade the frontotemporal cortices2. The clinical presentation of HSVE is diverse, incorporating symptoms such as headache, fever, encephalopathy, seizures, and localized neurologic impairment3. Prompt diagnosis and anti-HSV therapy reduce mortality; unfortunately, neurological sequelae are still common, with an increased risk of late unprovoked seizures and epilepsy2.
Non-convulsive status epilepticus (NCSE) involves single or repeated absence or focal impaired awareness seizures lasting over 10 minutes, during which individuals are unresponsive with minimal body movement or shaking. Confirmation of the diagnosis typically requires an EEG. While literature includes descriptions of non-convulsive seizures during herpes simplex encephalitis4, there is significantly less documentation regarding NSCE post-resolution of the acute phase of the infection. In this article we describe a case of non-convulsive status epilepticus presenting 8 months following resolution of herpesvirus encephalitis. Additionally, we provide an overview of relevant literature and draw comparisons with our specific case.
Case Report
A 55-year-old male, with a medical history of hypertension and diabetes, was brought to the emergency room in March 2023 by family members due to complaints of confusion persisting for a few hours. According to family reports, he was observed speaking incoherently and making irrelevant statements. The patient had been experiencing an unexplained fever for the past three days, with no discernible focus and no accompanying headache. He has no history of smoking or illicit drug use, no recent travel, and no known sick contacts. The patient adheres to his regular medications for diabetes and hypertension and has not reported any similar complaints in the past.
During the initial examination, the patient was febrile, and while he remained alert and could follow simple commands, his speech was often irrelevant, and he only responded to certain questions. There was no neck stiffness, and the patient’s pupils, power, and reflexes were all within normal. He was also able to ambulate without support. Similarly, examinations of the skin, oral cavity, chest, and abdomen did not reveal any abnormalities.
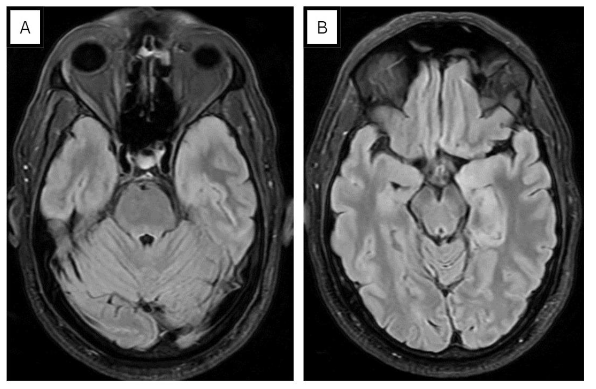
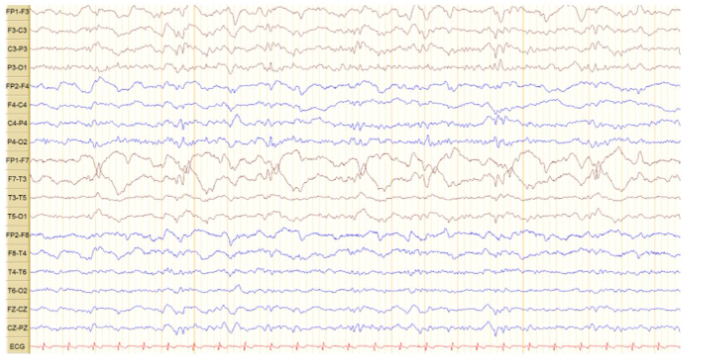
Laboratory investigations revealed neutrophilic leukocytosis in serum with a mildly elevated CRP. Bacterial cultures were negative, and both the chest X-ray (CXR) and CT head were unremarkable. However, an MRI of the brain showed T2/FLAIR hyperintensity in the left mesial temporal and temporal pole, associated with gyral edema (see Figure 1). There was with no post-contrast enhancement. Polymerase chain reaction (PCR) of cerebrospinal fluid (CSF) showed HSV-1 DNA, establishing the diagnosis of herpesvirus encephalitis and the patient was immediately started on acyclovir. Due episodic deterioration in the level of consciousness, levetiracetam 500mg BID was initiated. Subsequent EEG findings showed sub-continuous periodic lateralized discharges (PLDs) over the left hemisphere, along with bilateral independent periodic discharges (BIPDs) (see Figure 2).
With the aforementioned management, the patient promptly improved. He achieved alertness and became oriented, responding coherently to questions. Although some word-finding difficulties persisted, he was discharged on levetiracetam after completing a 14-day antiviral course.
In November 2023, the patient returned to our emergency department, accompanied by family members who reported a three-day history of confusion. According to them, he exhibited irrelevant and occasionally incoherent speech. No focal deficits or abnormal jerking movements were observed, and there were no upper respiratory or gastrointestinal symptoms, headache, fever, or known sick contacts. The patient was adhering to the prescribed medications, including antidiabetic and antihypertensive medications, as well as levetiracetam.
During the examination, he was conscious, afebrile, and vitals were within normal limits. However, he had a dull expression and a loss of awareness of his surroundings. His responses to questions were often irrelevant, with occasional moments of muteness and incomprehensibility. At times, he failed to recognize family members. Again, no focal neurologic deficits were identified during the examination, and the systemic examination revealed no notable abnormalities.
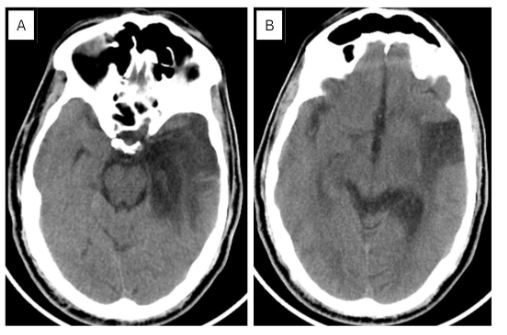
During that period, our list of potential diagnoses included herpesvirus reactivation, non-convulsive seizures, and other central nervous system infections. Consequently, acyclovir was initiated empirically. An emergency CT brain revealed a significant hypodense area in the left temporal region (see Figure 3), prompting a shift in the suspected diagnosis towards a potential ischemic stroke. The patient was admitted and started on antiplatelet therapy and statins. To detect signs of secondary CNS vasculitis due to herpesvirus a CT angiography was performed, but the results were normal. Re-analysis of cerebrospinal fluid (CSF) via PCR did not detect HSV DNA, leading to the discontinuation of acyclovir.
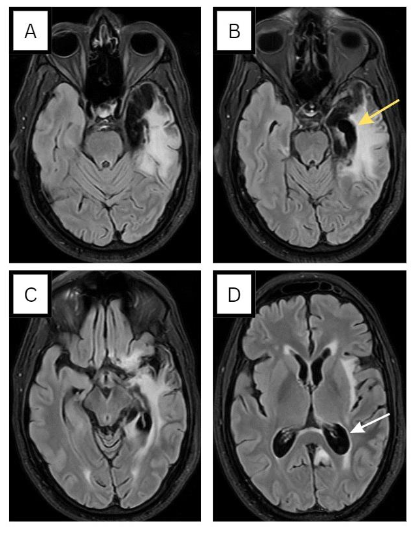
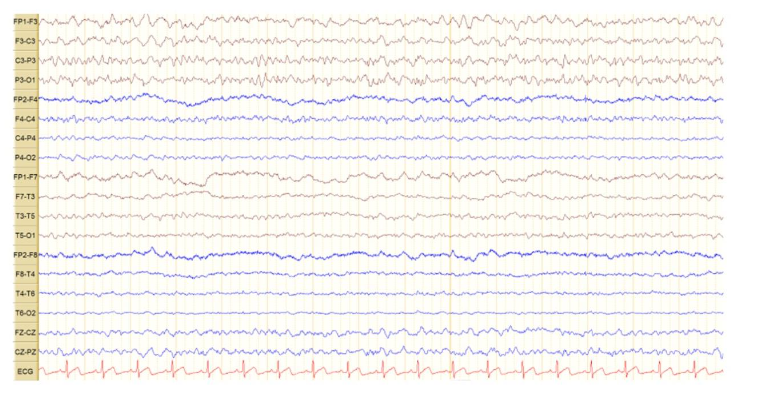
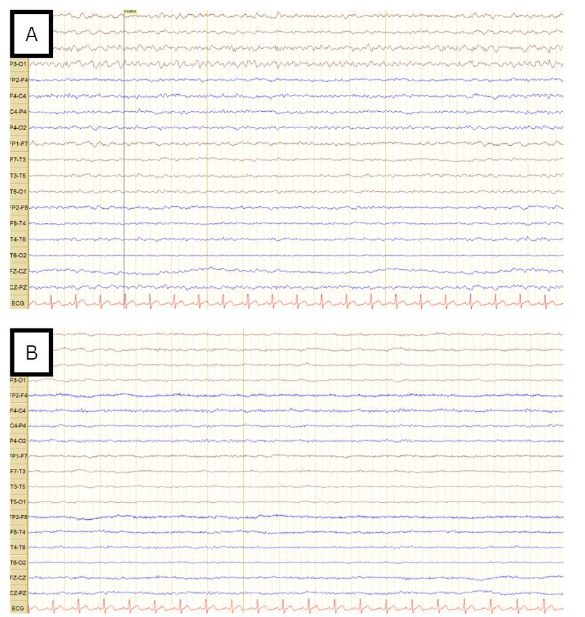
MRI was repeated and showed left temporal cortical/subcortical areas exhibiting encephalomalacia/gliosis (see Figure 4), with no evidence of restricted diffusion, thereby making stroke unlikely. An 18-channel awake EEG showed continuous focal epileptiform discharges over the left central parietal region, as quasi periodic discharges, over a background activity of moderate slowing (see Figure 5). This determination led to the diagnosis of postencephalitic non-convulsive status epilepticus. In light of this, the dosage of levetiracetam was escalated from 500mg BID to 1500mg BID. An EEG the following day showed resolution of status epilepticus but continued to display epileptiform discharges over the left fronto-central regions (Figure 6A). Consequently, lacosamide 200mg BID was introduced and EEG recorded 1 day later indicated the resolution of epileptiform discharges (Figure 6B). Upon discharge, the patient exhibited significant improvement in his clinical condition. Although he still experienced some baseline word-finding difficulty, his speech was notably more comprehensible. Additionally, he demonstrated no difficulty in responding to commands. It is important to note that the patient was an expatriate worker, and unfortunately there was loss to follow-up post-discharge.
Discussion
Seizures are a common manifestation of viral encephalitis in the acute phase, particularly with herpes simplex virus, where 75% of HSVE patients reportedly experience seizures5. The semiology of these seizures is predominantly focal (65%), followed by generalized (23%), and a combination of both (12%). Non-convulsive seizures may be subtle and missed, so the true incidence is likely underestimated. The high incidence of seizures are probably due to the fact that herpes simplex virus has an affinity to the orbitofrontal and mesial temporal lobes which are highly epileptogenic2.
The initial manifestation of fever and encephalopathy in our patient, coupled with MRI evidence showing temporal lobe FLAIR hyperintensity and a positive CSF for HSV, aligned with the diagnosis of herpes simplex virus encephalitis. Furthermore, our patient experienced episodes of escalating confusion and altered consciousness, and an EEG was crucial in diagnosing subclinical seizures. Typical EEG findings in patients with HSVE during the first 5–7 days of illness are characterized by spike and slow wave activity, often arising from the temporal lobe, and some patients (such as ours) develop PLDs5. Later, paroxysmal sharp waves or triphasic complexes with temporal predominance can be observed.
While herpes simplex virus encephalitis (HSVE) typically follows a monophasic course, it can manifest as chronic persistent or relapsing forms2. Post-acute seizures in HSVE can be attributed to various causes, including relapse, postinfectious autoimmune disease, and unprovoked seizures leading to postinfectious epilepsy. Relapses occur in 5-26% of cases, typically manifesting shortly after completing acyclovir therapy2. With regards to our patient, who re-presented 8 months following the acute phase HSVE with confusion, a relapse of HSE was high among the differentials. However, a repeat CSF PCR was negative for HSV, and an EEG showed non-convulsive status epilepticus.
In a retrospective review of patients with prior HSVE, postencephalitic epilepsy was noted in 45.5 % of the patients3. The predominant seizure patterns in postencephalitic epilepsy were unilateral temporal, bilateral temporal and multifocal or generalized with the majority of patients reporting an aura5. The high incidence of late unprovoked seizures following HSE may be due to the necrotizing nature of HSV-1 infection and involvement of the highly epileptogenic mesial temporal and basi-frontal cortices2. For example our patient’s repeat MRI scan showed the devastating impacts HSV can have on the brain including the profound atrophy of the left mesial temporal regions.
A case series of 23 patients identified risk factors for the development of postencephalitic epilepsy included younger age and acute symptomatic seizures during HSVE6. Brain imaging, CSF analysis, and EEG were not associated with the development of epilepsy following herpes simplex virus encephalitis. Autoimmune phenomena is another cause of delayed neurological deterioration and may be associated with the development of anti N-methyl-D-aspartate (NMDA) antibodies6. Although sending for autoantibodies would have been interesting, our patient’s lumbar puncture did not show any protein elevation or lymphocytic pleocytosis indicative of autoimmune etiology. Additionally, he responded well to antiepileptic escalation alone, so we did not pursue further autoimmune testing at that time.
Concerning seizure control in postencephalitic epilepsy, there are no randomized controlled trials on the efficacy of antiepileptic drugs and their combinations, and current recommendations are based on expert opinion5. At the time of early seizure recurrence, many of the patients will be on phenytoin, valproate or levetiracetam if seizures presented during the acute phase of HSVE. Our patient was on levetiracetam when he presented with non-convulsive status epilepticus months following the acute phase of HSVE. Despite increasing levetiracetam dose our patient’s EEG showed some epileptiform discharges (Figure 6A) and therefore lacosamide was added with good effect on patient’s clinical status and resolution of epileptiform discharges (Figure 6B). Regrettably, epilepsy following HSVE typically proves resistant to treatment with antiepileptic drugs5, therefore follow up is very important in such cases. A pre-surgical evaluation with special consideration of neuropsychological performance can be done to define the subgroup of patients with a chance for favorable outcome.
In conclusion, this case highlights the importance of considering non-convulsive status epilepticus in individuals exhibiting prolonged altered mental states following the resolution of acute HSVE. An EEG is paramount in confirming the diagnosis.
References
- Stahl, J. P., & Mailles, A. (2019). Herpes simplex virus encephalitis update. Current Opinion in Infectious Diseases, 32(3), 239–243. https://doi.org/10.1097/QCO.000000000000055
- Misra, U. K., Tan, C. T., & Kalita, J. (2008). Viral encephalitis and epilepsy. Epilepsia, 49(Suppl. 6), 13-18. https://doi.org/10.1111/j.1528-1167.2008.01751.x
- Singh, T. D., Fugate, J. E., Hocker, S., Wijdicks, E. F. M., Aksamit, A. J., & Rabinstein, A. A. (2016). Predictors of outcome in HSV encephalitis. Journal of Neurology, 263(2), 277-289.
- Jeremić, M., Arsenijević, M., Jovanović, D., & Berisavac, I. (2021). Non-convulsive status epilepticus as an initial manifestation of herpes simplex virus encephalitis. Epileptic Disorders, 23(5), 749-753. https://doi.org/10.1684/epd.2021.1320
- Sellner, J., & Trinka, E. (2012). Seizures and epilepsy in herpes simplex virus encephalitis: current concepts and future directions of pathogenesis and management. Journal of Neurology, 259, 2019–2030. https://doi.org/10.1007/s00415-012-6494-6
- Hersh, N., Ben Zvi, H., Goldstein, L., Steiner, I., & Benninger, F. (2023). Epilepsy following herpes simplex encephalitis – A case series. Epilepsy Research, 192, 107137. https://doi.org/10.1016/j.eplepsyres.2023.107137