





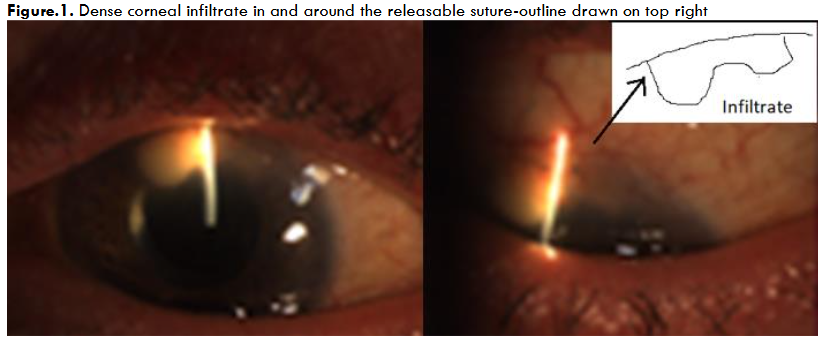
Non-infectious Endophthalmitis Post-Trabeculectomy Case Report
Non-infectious Endophthalmitis Associated with a Releasable 10-0 Monofilament Nylon Suture After a Trabeculectomy: First Case Report
Mr Bhavesh Sharma1, Ms Ellora Sharma2, Ms Monali Chakrabarti3, Mr Tarun Sharma 4
- Medical Student at University of Manchester, Manchester, UK
- Medical Student at Barts and The London School of Medicine and Dentistry, Queen Mary University of London, UK
- Consultant ophthalmologist, Ophthalmology department, Worcestershire Royal hospital, Worcester, England, UK
- Consultant Ophthalmologist, Ophthalmology department, Worcestershire Royal hospital, Worcester, England, UK
OPEN ACCESS
PUBLISHED: 31 January 2025
CITATION: Sharma, B., Sharma, E., et al., 2025. Non-infectious Endophthalmitis Associated with a Releasable 10-0 Monofilament Nylon Suture After a Trabeculectomy: First Case Report. Medical Research Archives, [online] 13(1). https://doi.org/10.18103/mra.v13i1.6216
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i1.6216
ISSN 2375-1924
Abstract
Background: Non-infectious endophthalmitis related to suture material in cataract and corneal surgery has been widely reported in Ophthalmic literature. We report a very rare case of nylon suture related non-infectious endophthalmitis in trabeculectomy surgery.
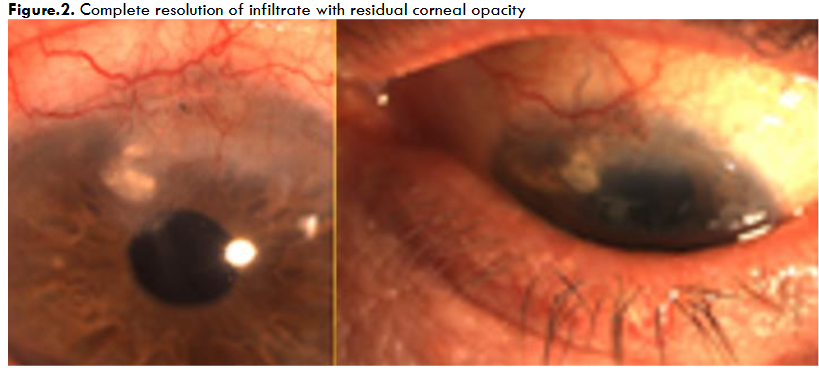
Case presentation: We present a case of acute non-infectious endophthalmitis associated with trabeculectomy surgery. After emergency vitreous biopsy and subsequent broad-spectrum antibiotic and antifungal treatment, inflammation did not settle. Following negative culture and sensitivity reports, including PCR testing for any bacteria, virus or fungus, the ocular inflammation was controlled successfully with topical and systemic steroids, with an improvement in patient’s vision. We present the photographic evidence of inflammatory exudate around the releasable suture on presentation and sequential photographs showing the resolution correlating with medications given.
Conclusions: This case highlights the importance of being vigilant against post-procedural infectious endophthalmitis. However, the possibility of non-infectious causes of intraocular inflammation should also be considered in any culture negative cases and managed appropriately with topical and systemic steroids.
Keywords
Endophthalmitis, Trabeculectomy, Non-infectious, Suture, Ophthalmology
Introduction
Trabeculectomy surgery has been the most reliable surgical procedure for glaucoma over last 50 years. The advent of releasable suture allowed postoperative bleb manipulation and improved aqueous flow leading to improved success rate. The most common suture material used in glaucoma surgery for releasable suture is 10 O monofilament Nylon. Any suture is known to increase the risk of Intraocular infection and any exposed suture-end might provide a wick for entry of potential infectious organisms in the eye. Any significant inflammation in the postoperative period is almost always considered as infectious endophthalmitis as Non-infectious endophthalmitis is very rare. Non-infectious endophthalmitis is an intraocular severe inflammation in the postoperative period. It is always culture negative and will usually respond to topical steroids. It is usually related to a non-infectious substance that enters the eye or its surrounding tissues. As per our literature review, non-infectious endophthalmitis has not been previously reported in trabeculectomy surgery.
We report the first-ever case of non-infectious endophthalmitis associated with a releasable 10-0 monofilament nylon suture after a trabeculectomy.
Case Summary
A 67-year-old Caucasian male with a history of advanced glaucoma underwent left trabeculectomy surgery on the 22nd November 2017. He had past ocular history of high myopia, iritis, and was bilaterally pseudophakic. He was under regular clinical review as per the departmental protocol. Three months after his trabeculectomy surgery, he presented to the emergency eye clinic on 27/2/18 with a week long history of a sore and sticky left eye, with intermittent foreign body sensation. Ocular examination showed mild congestion of the eye with a good, functioning bleb. No bleb tenderness or leak was noted. Intraocular pressure at this point was 11mmHg (Right) and 7mmHg (Left eye).
Initially broad-spectrum antibiotics and cycloplegics (ofloxacin and cyclopentolate) were prescribed for suspected blebitis. Though the patient developed blurred vision in the Left eye a week later, he came for next review a few weeks later on 11/4/2018.
The emergency Ophthalmology team assessed and diagnosed Left keratitis, and requested urgent Glaucoma team opinion. The offending releasable Suture was removed. A vitreous biopsy was sent for and intravitreal antibiotics injected. The patient was reviewed by the Glaucoma consultant who noted two sub-epithelial infiltrates along the track of releasable suture and a significant anterior chamber inflammatory reaction.
Second opinions were then sought from two other Consultants. A provisional diagnosis of fungal endophthalmitis in the eye was arrived at. Thus, it was treated as endophthalmitis using intravitreal antibiotics and antifungal agents. However, the vitreous biopsy results showed no organisms or fungal elements, but just scanty pus cells were noted. As the PCR tests were negative as well, the possibility of fungal, viral or bacterial endophthalmitis was ruled out. The ocular inflammation expert opined the infiltrate to be largely inflammatory as opposed to infectious. Hence, oral Prednisolone and topical Dexamethasone drops were prescribed, in addition to the ongoing antibiotic and antifungal regimen. This treatment regime resulted in a gradual resolution of the corneal infiltrate in a few days. Thus, all except the Dexamethasone drops were discontinued. Oral prednisolone and Omeprazole were continued. Over the next few months, the ocular symptoms improved. The best-corrected vision returned to 6/9 (Snellen). The Goldmann intraocular pressure stabilised at 14mmHg with Ganfort (Bimatoprost/Timolol) eye drops in the left eye. A corneal residual scar in the area of the infiltrate remained.
Discussion
This patient presented as severe postoperative inflammation including significant anterior chamber activity three months after the surgery. It was treated as a case of intraocular fungal infection due to its delayed presentation. Two independent Ophthalmology consultants agreed with the diagnosis and the planned course of action. Usually, postoperative endophthalmitis presents within first few days to 2 weeks post-operative. This case had a severe inflammatory reaction only after 3 months post-operative. As there were corneal infiltrates and anterior chamber inflammation, it was treated as fungal endophthalmitis. Further, it was noted that the infiltrate was in the same shape as the loop of the releasable suture placed in the trabeculectomy flap. No improvement in either symptoms or clinical signs was noted following treatment with the intravitreal antibiotics and the antifungals. After the vitreous biopsy was reported, an ocular inflammation expert opinion was sought. The ocular inflammation consultant considered this as Non-infectious inflammatory reaction and advised to start topical and oral steroids. A significant improvement in patient’s condition both in symptoms and signs was noticed within the next few days. Ultimately, the steroid treatment led to a complete resolution of inflammation and also a restoration of visual acuity. As the inflammatory exudate at presentation was densest around the site of releasable suture and the residual scar after resolution of inflammation was also very pronounced around the site of releasable suture, this was considered reasonable evidence that the severe inflammation was related to the releasable suture which was a 10-0 Monofilament nylon. As the vitreous biopsy and conjunctival suture did not grow any organism on culture and the PCR (Polymerase chain reaction) was negative for any infectious agent, this case was considered to be non-infectious in origin. Suture related endophthalmitis are usually infectious in origin due to some exposed externalised part or a slow leak leading to a track through which bacteria travel and cause infection. A literature review shows six reported cases, where sterile inflammation occurred to monofilament material in corneal and cataract surgery. Our search did not reveal any report in the literature of a similar case of non-infectious endophthalmitis after trabeculectomy surgery and possibly related to the releasable suture.
This case highlights that while ophthalmologists should remain vigilant for post-procedural infectious endophthalmitis, non-infectious causes of intraocular inflammation should also be considered and managed appropriately with the use of steroids.
References
- King AJ, Hudson J, Fernie G, Kernohan A, Azuara-Blanco A, Burr J, Homer T, Shabaninejad H, Sparrow JM, Garway-Heath D, Barton K, Norrie J, McDonald A, Vale L, MacLennan G; TAGS Study Group. Primary trabeculectomy for advanced glaucoma: pragmatic multicentre randomised controlled trial (TAGS). BMJ. 2021 May 12;373:n1014. doi: 10.1136/bmj.n1014.
- Cohen J, Osher RH. Releasable suture in filtering and combined surgery. Ophthalmol Clin North Am. 1988; 1:187-197.
- Kolker AE, Kass MA, Ratt JL. Trabeculectomy with releasable sutures. Arch Ophthalmol 112:62–66, 1994.
- Rosenberg LF, Siegfried CJ. Endophthalmitis Associated with a Releasable Suture. Arch Ophthalmol. 1996;114(6):767.
- Jackson H, Bosanquet R: Should nylon corneal sutures be routinely removed? Br J Ophthalmol 1991, 75: 663–664. 10.1136
- Henry, C.R., Flynn Jr, H.W., Miller, D. et al. Delayed-onset endophthalmitis associated with corneal suture infections. J Ophthal Inflamm Infect 3, 51 (2013).
- Mowatt L, Butler L: Hazard of redundant corneal sutures: a safety message. J Cataract Refract Surg 2004, 30: 1152.
- Confino J, Brown SI: Bacterial endophthalmitis associated with exposed monofilament sutures following corneal transplantation. Am J Ophthalmol 1985, 99: 111–113.
- Henry CR, Flynn HW Jr, Miller D, Forster RK, Alfonso EC: Infectious keratitis progressing to endophthalmitis: a 15-year-study of microbiology, associated factors, and clinical outcomes. Ophthalmology 2012, 119: 2443–2449. 10.1016
- Christo CG, van Rooij J, Geerards AJM, Remeijer L, Beekhuis WH: Suture-related complications following keratoplasty: a 5-year retrospective study. Cornea 2001, 20: 816–819.
- Moore TE, Aronson SB. Suture reaction in the human cornea. Arch Ophthalmol 1969; 82:575-579.
- Sullivan LJ, Su C, Snibson G, Taylor HR. Sterile ocular inflammatory reactions to monofilament suture material. Aust N Z J Ophthalmol. 1994 Aug;22(3):175-81.