






Nurses’ Attitudes Toward Opiophobia and Thanatophobia
Correlation of sociodemographic parameters with nurses’ attitudes about opiophobia and thanatophobia
Morana Brkljačić1, Sandra Fletko2, Ina Stašević3, Barbara Ebling4, Darko Ropac5
- Assoc.prof., MD, PhD, Morana Brkljačić, Catholic University of Croatia, Zagreb, Croatia
- Mag.med.techn., Special hospital for chronic diseases, Novi Marof, Croatia
- Assist.prof., MSc, PhD, Catholic University of Croatia, Zagreb, Croatia
- Assoc.prof., MD, PhD, University Josip Juraj Strossmayer, Osijek, Croatia
- Professor, MD, MSc, PhD, Catholic University of Croatia, Zagreb, Croatia
OPEN ACCESS
PUBLISHED: 30 June 2025
CITATION: BRKLJAČIĆ, Morana et al. Correlation of sociodemographic parameters with nurses’ attitudes about opiophobia and thanatophobia. Medical Research Archives, [S.l.], v. 13, n. 6, june 2025. Available at: <https://esmed.org/MRA/mra/article/view/6705>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i6.6705
ISSN 2375-1924
ABSTRACT
Introduction. Pain is one of the most common symptoms encountered by patients with palliative needs, and since it affects the patient’s quality of life, it is the most necessary to alleviate or eliminate it in order to improve the quality of the remaining life of the patient and his family. The basis of the treatment of any pain in palliative care is the application of non-pharmacological procedures and appropriate pharmacotherapy. Among a certain number of medical personnel, there is a fear of the consequences when using opioids, which often leads to their reduced use in practice. The term opiophobia is often associated with the term thanatophobia, which also affects the work of medical staff. In order to treat the pain as best as possible, it is necessary to examine the presence of these fears and to educate about them.
Aims. The aim of this research work was to determine the attitudes of nurses in the Department for extended treatment and palliative care Novi Marof towards opiophobia and thanatophobia.
Methods. The conducted research is of cross-sectional type. An anonymous paper-pencil survey was used in the research and was intended exclusively for nurses of the Service for extended treatment and palliative care in Novi Marof/Croatia. A total of 72 nurses participated. In the first part of the survey, the sociodemographic data of the respondents was collected, and in the second part, the expression of opiophobia and tanatophobia was examined using declarative claims to which the participants responded according to the Likert scale. Based on the collected data, appropriate statistical analyses were performed using the IBM SPSS Statistics 25 program (SPSS Inc., Chicago, IL, USA).
Results. Nurses, regardless of their workplace, years of service or level of education, have equally present thanatophobia. There is a difference with opiophobia, for those nurses who working the Department of Palliative Care, they show more affirmative attitudes towards the use opioids compared to other departments. Similarly, nurses with longer working experience show more affirmative attitudes compared to employees with shorter working experience.
Conclusion. The attitudes of nurses towards opiophobia and thanatophobia have a significant impact on patient care. Addressing these attitudes and providing education and support to nursing staff can improve the quality of care provided to patients in pain and those requiring end-of-life care.
Article Details
Introduction
The World Health Organization (WHO) defines palliative care as an approach that improves the quality of life of patients (adults and children) and their families who are facing problems associated with life-threatening illness. It prevents and relieves suffering through the early identification, correct assessment and treatment of pain and other problems, whether physical, psychosocial or spiritual.
Quality palliative care is achieved through early recognition, adequate assessment and relief of pain and other physical, emotional and spiritual problems.
Palliative medicine differs from curative medicine in that it cannot cure the patient, and therefore focuses on providing care, alleviating suffering and pain, while preserving the dignity of the patient. As the disease progresses, the curative approach is increasingly replaced by palliative medicine. While in curative medicine the primary goal is cure, and death is a failure, in palliative medicine the goal is the cessation of suffering.
The most important goal of palliative care is to provide the patient with the best possible quality of life by implementing interventions aimed at reducing suffering and pain, and controlling unpleasant symptoms. Every patient facing the end of life experiences emotional, social and spiritual pain that causes negative emotions in them and disrupts their inner peace. The priority in palliative care is to reduce the level of pain to a bearable level for the patient. Neglected or inadequately treated pain can cause unnecessary suffering and dissatisfaction for the patient. The team caring for the patient must include highly qualified professionals. The nurse spends the most time with the patient, monitors and assesses his condition and provides palliative care. She is the first to notice changes in the patient, the presence or absence of pain and discomfort. About 50% of patients still suffer from pain that is inadequately relieved. That is why proper education of nurses, knowledge of the latest guidelines and standards in pain treatment, and developed communication skills and empathy are very important, in order to ultimately help the patient, improve the quality of his remaining life.
The WHO guidelines for the treatment of malignant pain suggest that treatment should begin with non-opioid analgesics. Their use with opiate analgesics is justified due to their synergistic effect, allowing lower opioid doses and reducing the incidence of side effects. The lowest possible effective dose is always used, with periodic review. Opioid analgesics block the transmission of pain impulses to the brain by binding to opioid receptors. Due to their effectiveness, they are certainly the most potent pain relievers and the gold standard for the treatment of severe pain. All opioid analgesics are chemically related to morphine. Opioids are primarily intended for the treatment of moderate to severe acute and chronic malignant pain. The cause of the pain still exists, but the patient’s fear is reduced and he does not react in a panic.
Opiophobia is associated with an irrational fear of addiction and side effects when using opioids, and the moral or legal risks associated with their prescription. Although pain relief is a priority task, inadequate analgesia or oligoanalgesia still prevails in palliative care, especially in patients with initial severe acute pain or in those for whom intravenous opioid administration is the method of choice.
The WHO states that opioids used to treat pain cause physical dependence and tolerance, but that this alone is not sufficient to establish a diagnosis of addiction. Fear of addiction sometimes makes health care professionals hesitant to use opioids. Opiophobia is a major problem among professionals and is a leading reason that limits the treatment of malignant pain in patients. Insufficient knowledge is another factor that increases opiophobia among professionals. Therefore, education of medical staff on the treatment and management of pain is an important step.
Thanatophobia (Greek: thanatos – death, phobos – fear) is anxiety or a feeling of fear of death or the dying process. It appears in childhood, increases with age and is sometimes associated with nosophobia – fear of developing a disease, and many other mental disorders. Death is not seen as an integral part of life, but as something unknown that results in fear.
As medicine has advanced to the point where it can delay death, people are increasingly dying slowly behind closed doors in the hospital room. Fear of death can affect the emotional state of patients, making it difficult to make decisions about treatment or consent to certain procedures. Modern medicine makes it possible to make the end of life easier by properly treating symptoms, planning, and discussing it with the patient and family.
The personal attitudes of nursing staff towards death and dying can affect the quality of care they provide to patients in the terminal phase of life. Attitudes towards death are influenced by cultural, social and personal beliefs that then consciously or unconsciously shape the person’s behaviour. In addition to clinical skills, nurses also need skills in dealing with the dying patient and their grieving family, which requires emotional maturity. Some of them use strategies to avoid talking to patients about their emotional problems and concerns, which creates emotional distance. Therefore, nurses must face their own fears, beliefs and anxiety about mortality. It is necessary to focus on the well-being of the dying patient by focusing on their spiritual, physical, mental and social needs. It is necessary to build a positive attitude towards death and dying. Only with such an approach can a more emotionally aware and open relationship with the patient towards death and dying be achieved, and how to communicate with the family.
Aim
The aim of the research is to determine the attitudes towards opiophobia and thanatophobia of nurses at the Hospital for the Treatment of Chronic Patients with regard to their workplace (hospital department), length of service and level of education.
Participants and Methods
ETHICS
Written approval was obtained for the purposes of the study from the Ethics Committee of the Hospital. Through informed consent, all respondents were thoroughly informed about the topic and purpose of the study and the fact that participation in the study was completely anonymous and voluntary. The study was conducted in accordance with the principles of good clinical practice, ethical principles and human rights.
RESEARCH DESIGN
The research was conducted as a cross-sectional study at the Hospital for the treatment of chronic patients in Novi Marof, Croatia. The research was conducted over the 2024 year.
PARTICIPANTS
Participants included in the study were nurses. Inclusion criteria was nurses of all levels of education, with a job in different departments of the Hospital, and with different lengths of service. The exclusion criterion was an incompletely completed questionnaire. The questionnaires were completed in the presence of one of the researchers, who was available to provide clarifications for any questions at any time. Each participant could withdraw from participation at any time.
QUESTIONNAIRES AND RESEARCH INSTRUMENTS
Participants answered three groups of questions. From general data, data was collected on length of service, hospital department in which they work, and level of education. In addition, they answered 11 questions related to opiophobia and 10 questions related to thanatophobia.
Responses to questions were graded on a five-point Likert scale (from 1 = strongly disagree to 5 = strongly agree). The questions in the questionnaires were closed-ended, with only one possible answer (out of several possible answers). All data were converted from an Excel file to an SPSS file. Appropriate statistical analyses were performed from the SPSS.
STATISTICAL PROCEDURES
Descriptive methods (percentages, mean values, measures of dispersion and Spearman’s rank correlation coefficient) and inferential methods (Kolmogorov–Smirnov distribution normality test, chi-square test, t-test) were used in statistical data processing. The significance of the difference was determined at the level of p < 0.05 (95% confidence level).
Results
DESCRIPTIVE STATISTICAL ANALYSIS
The length of service of the participants in the sample varies between one and 41 years. The average length of service of all respondents is 17.6 years with increased variability (coefficient of variation is 68%). The respondents were classified into three groups according to the length of service. In the category up to 4 years: 16.7% In the category from 5 to 29 years: 63.9% More than 30 years: 19.5% of the respondents. According to the workplace (department), the participants were divided into two groups: Department for Extended Treatment (acute care department): 37 participants (51.4%) Department of Palliative Care (hospice): 35 participants (48.6%) According to the level of education, participants were divided into three categories: Secondary education: 47 participants (65.3%) Bachelor’s degree: 23 nurses (31.9%) Master’s degree: 2 participants (2.8%) Statements related to opiophobia can be divided into three groups according to their acceptance by the participants: Very little accepted statements (average below 2.00): Statements 5 and 11 with the lowest average of 1.56 and 1.64 respectively. Less accepted statements (average between 2.00 and 2.99): majority of statements. Moderately accepted statements (average above 3.00): Only statement 1 (the most acceptable of all 11 statements).
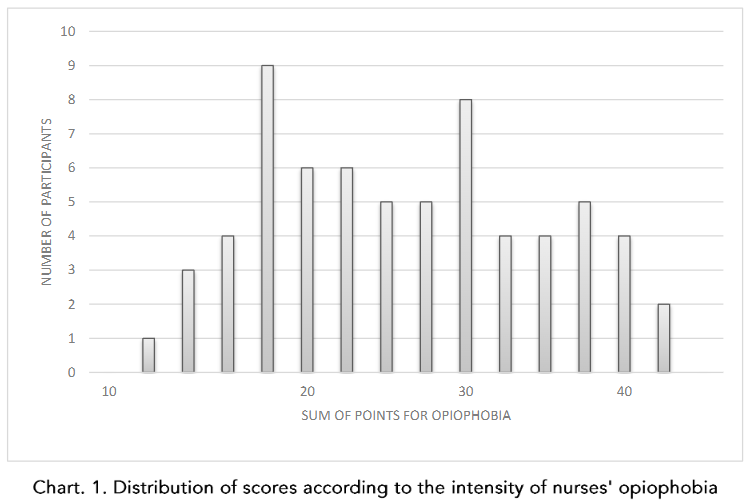
The overall average acceptance of all statements is 2.25. The variability of acceptance of individual statements by participants is moderate (coefficients of variation between 39% and 50%) or increased (coefficients of variation between 51% and 63%). (Table 1) In order to express the intensity of opiophobia with a single number (instead of 11 statements), total results were formed for 11 questions about opiophobia for each individual respondent. A lower total means less fear, and a higher total expresses greater fear of addiction, toxicity, and overdose. The theoretical sum of answers can be at least 11 (11 × 1 = 11) and at most 55 (11 × 5 = 55). Among the participants, the sum ranged between 11 and 43, with an average of 24.8 ± 7.746 and a moderate dispersion (coefficient of variation = 31%). The value of the Kolmogorov–Smirnov test (z = 0.078; p = 0.200) shows that the distribution is similar to normal. The distribution of the number of points according to the intensity of opiophobia is shown in Chart 1.
For inferential statistical analysis, participants were divided into three categories based on quartile values (Q1 = 18.25 and Q3 = 31): Minor opiophobia (1–18 points): 18 participants (25%) Medium opiophobia (19–30 points): 35 participants (49%) Higher opiophobia (31–43 points): 19 participants (26%)
Participants answered that they disagreed with most statements related to thanatophobia (except statements 5, 7, and 8). The statements can be divided into three groups with regard to their acceptance by participants: (average < 2.00): statements 1, 9, 2, and 3. Less accepted statements (average 2.00–2.99): most statements. moderate accepted statements (average > 3.00): statement 8, with an average of 3.32 (the most acceptable of all 10 statements).
The analysis of responses related to thanatophobia is shown in Table 2.
Table 1. Statements related to opiophobia (n = 72)
| CLAIM | AM | SD | CV |
|---|---|---|---|
| 1. Opioids should be limited to the treatment of unbearable pain | 3.22 | 1.258 | 39 |
| 2. I would never give opiates to someone who is able to work | 2.68 | 1.362 | 51 |
| 3. Opiates should be reserved for patients whose life expectancy is less than six months | 2.15 | 1.360 | 63 |
| 4. Chronic pain of unknown origin should not be treated with opiates even if this is the only way to relieve pain | 2.17 | 1.163 | 54 |
| 5. Patients who complain of excessive pain are mostly addicts | 1.56 | 0.933 | 60 |
| 6. The use of opiates for pain relief in benign diagnoses should not be practiced | 2.14 | 1.025 | 48 |
| 7. Opioids should be reserved exclusively for the treatment of pain in terminally ill patients | 2.18 | 1.304 | 60 |
| 8. Patients who fit the profile of addicts should not be given opiates | 2.40 | 1.122 | 47 |
| 9. Regardless of the severity of the pain, former addicts should not be given opiates | 2.07 | 1.053 | 51 |
| 10. When using opiates, I always have a fear of overdose | 2.54 | 0.992 | 39 |
| 11. By administering opiates, I hasten the patient’s death | 1.64 | 0.893 | 54 |
AM – arithmetic mean; SD – standard deviation; CV – coefficient of variation
AM = arithmetic mean; SD = standard deviation; CV = coefficient of variation.
Table 2. Statements related to thanatophobia (n = 72)
| CLAIM | AM | SD | CV |
|---|---|---|---|
| 1. If I knew a patient had an incurable disease, I would avoid taking care of them if possible | 1.14 | 0.564 | 49 |
| 2. The presence of dying patients in the institution where I work makes me feel uneasy | 1.86 | 1.179 | 63 |
| 3. When patients start talking about death, I feel uncomfortable | 1.93 | 1.191 | 62 |
| 4. I feel helpless when I have a terminally ill patient in the ward | 2.38 | 1.419 | 60 |
| 5. It is frustrating to talk to the families of patients who have an unfavorable diagnosis | 2.82 | 1.237 | 44 |
| 6. I am not satisfied with the way I care for dying patients | 2.44 | 1.299 | 53 |
| 7. I am not satisfied with the way I feel uncomfortable when a dying patient wants to say goodbye to me, who cares for dying patients | 2.83 | 1.404 | 50 |
| 8. Working with dying patients has had a negative impact on me | 3.32 | 1.351 | 41 |
| 9. I feel that I am not capable of caring for a dying patient as well as anyone else | 1.64 | 0.969 | 59 |
| 10. I don’t like working with patients whose disease doesn’t respond to therapy | 2.08 | 1.045 | 50 |
AM – arithmetic mean; SD – standard deviation; CV – coefficient of variation
In order to obtain a measure for each respondent that would express their lower or higher fear of the patient’s death, the answers to the 10 statements were summarized by adding them up. A lower score for the respondent means a less pronounced fear of the patient’s death, while a higher score means a more pronounced fear of his death.
The theoretical sum of the answers can be at least 10 (10 × 1 = 10) and at most 50 (10 × 5 = 50). By implementing such a system, points were determined for each respondent and the distribution of points was obtained on the basis of which descriptive indicators were calculated.
The average score for thanatophobia is 22.4 ± 6.975, with moderate dispersion (coefficient of variation = 31%). The value of the Kolmogorov–Smirnov test (z = 0.092; p = 0.200) shows that the distribution is similar to normal.
The distribution of the number of points according to the intensity of nurses’ thanatophobia is shown in Chart 2.
For the purposes of inferential statistical analysis, the participants were divided into three categories based on the quartile values (Q1 = 17 and Q3 = 27.25) according to the intensity of the patient’s fear of death:
Low fear (10–16 points) – 16 subjects (22%) Medium fear (17–27 points) – 38 subjects (53%) High fear (28–43 points) – 18 subjects (25

Chart 2. Statements related to thanatophobia (n = 72)
INFERENTIAL STATISTICAL ANALYSIS
The first group of analyses consists of t-tests of differences between arithmetic means. Six t-tests were performed comparing arithmetic means with regard to opiophobia and thanatophobia of participants with respect to their place of work in the hospital, length of service, and level of education.A significant difference was found with regard to opiophobia, with the fear of using opiates being significantly higher among nurses who do not work in the palliative care department. Similarly, significantly higher levels of fear of opioid use were found among nurses with shorter experience.The results are shown in Table 3.
Table 3. Comparisons of arithmetic means of the number of points (t test)
| PHOBIA | VARIABLE | No | AM | t | P |
|---|---|---|---|---|---|
| Opiophobia | Acute Care | 37 | 27.46 | 3.251 | 0.002 |
| Palliative Care | 35 | 21.89 | |||
| Thanatophobia | Acute Care | 37 | 23.16 | 0.897 | 0.373 |
| Palliative Care | 35 | 21.69 | |||
| Opiophobia | Shorter work experience | 12 | 21.00 | 2.985 | 0.006 |
| Longer work experience | 14 | 29.29 | |||
| Thanatophobia | Shorter work experience | 12 | 20.00 | 1.117 | 0.275 |
| Longer work experience | 14 | 23.50 | |||
| Opiophobia | Middle school | 47 | 24.91 | 0.109 | 0.913 |
| Higher education * | 23 | 25.13 | |||
| Thanatophobia | Middle school | 47 | 22.98 | 0.643 | 0.522 |
| Higher education * | 23 | 21.83 |
* Two Master of Nursing participants were excluded from this analysis.
Chi-Square Test
The Chi-square test was used to determine the significance of the relationship between the level of opiophobia and thanatophobia and the workplace of the participants. There is a statistically significant relationship (p = 0.007) between the hospital departments (acute care, palliative care) in which the participants are employed and the level of opiophobia (minor, medium, higher), which is very strong (coefficient Φ = 0.37; Cramer’s V = 0.37).
Participants in acute care departments show stronger opiophobia (79%) compared to participants in palliative care departments.
There is no statistically significant relationship (p = 0.316) between the hospital departments (acute care, palliative care) in which the participants are employed and the level of thanatophobia (minor, medium, higher).
Table 4. Comparisons of proportions of participants with a positive attitude towards opiophobia and thanatophobia (n = 72)
| PHOBIA | VARIABLE | No | Proportion | t | P |
|---|---|---|---|---|---|
| Opiophobia | Acute Care | 37 | 5/37 = 0.233 | ||
| Palliative Care | 35 | 13/35 = 0.355 | 2.38 | 0.020 | |
| Thanatophobia | Acute Care | 37 | 7/37 = 0.189 | 0.69 | 0.490 |
| Palliative Care | 35 | 9/35 = 0.257 | |||
| Opiophobia | Shorter work experience | 12 | 6/12 = 0.500 | 2.68 | 0.013 |
| Longer work experience | 14 | 1/14 = 0.071 | |||
| Thanatophobia | Shorter work experience | 12 | 6/12 = 0.500 | 1.58 | 0.128 |
| Longer work experience | 14 | 3/14 = 0.214 |
Applying Spearman’s correlation coefficient, a weak but statistically significant connection was established between attitudes towards opiophobia and those towards thanatophobia (correlation coefficient = 0.37).
Discussion
The approach to treating malignant pain varies, but opioids remain the gold standard. Due to potentially unwanted side effects and lack of knowledge of the basic principles of treatment, opioid phobia develops.
This study shows that opioid phobia is present among medical staff, but less among those working in palliative care units. Similarly, a larger number of nurses in palliative care units express a more affirmative attitude towards the use of opioids compared to those in acute care units. Medical staff caring for patients with palliative needs are more likely to encounter severe pain in patients and use opioid analgesics more often, which is why it is understandable that the level of opioid phobia is lower than in other units.
A 2018 study in China showed similar results, indicating that the environment in which staff work affects the level of knowledge of nurses about pain management. Weaker knowledge of pain management is associated with negative attitudes about the use of opioids and it was It has been emphasized that education and increasing the level of knowledge of nurses have a more positive impact on attitudes towards pain management.
A study in Turkey shows that nurses are afraid of using opioids, mostly because of side effects. 68.6% of them are afraid of using opioids, and as many as 47.7% consider them dangerous. In that 2022 study, there was a fear of using opioids in patients with previous addiction (64% of participants expressed fear), while this study did not confirm this, but rather the opposite. When asked whether, regardless of the severity of the pain, former addicts should not be given opiates, the largest proportion of participants (38.8%) stated that they did not agree with this statement at all. The aforementioned study also did not find a link between length of work experience and fear of using opioids.
A 2009 survey in Kansas found that 78.5% of nurses who are in constant contact with opioids feel more comfortable using them. Nurses who used opioids more often showed greater concern about the impact on the patient. In contrast, a 2017 survey showed that 84% of nurses were not afraid of using opioids, while 87.5% did not consider opioids to be dangerous drugs but helpful in relieving pain. This is consistent with the present study, where the fewest participants agreed with the statement that the use of opiates accelerates the patient’s death. That research also showed that nurses mostly learn from experience.
When examining fear of overdose, in this study most participants were undecided — neither agreeing nor disagreeing — but more participants indicated that they were not afraid of overdose. A survey from Rwanda showed that 63% of nurses stated they are afraid of using opioids, and 56.8% are afraid of overdose when using them. In that research, lack of knowledge was identified as the main factor of opiophobia.
In this study, participants disagreed with the statement that opioids should be reserved exclusively for the treatment of terminally ill patients. A 2019 survey in Ankara showed that 67.6% of participants thought the opposite — that opioids should only be used in cancer patients. This result was attributed to lack of knowledge and prejudice.
The majority of participants in this study disagreed with the statement that chronic pain of unknown origin should not be treated with opioids if it is the only way to relieve pain, and that the use of opioids for pain relief in benign diagnoses should not be practiced. On the other hand, in a survey conducted in Greece, the majority of participants (55%) believed that opioids should not be used when the source of pain is unknown, because such pain relief can make it more difficult to make a diagnosis.
This study shows that opioid phobia is more prevalent among nurses with higher education than among those with secondary education, which does not confirm previous claims that higher education necessarily leads to more positive attitudes. However, taking into account that a large number of staff with higher education are also younger and have less work experience, this is understandable. This confirms the result that nurses with longer work experience have a more affirmative attitude towards the use of opioids.
Research conducted in Switzerland indicates that fear of side effects and the development of addiction are the main causes of opioid phobia among healthcare providers, and that opioid phobia is associated with their personality traits, with fears being more pronounced among caregivers with shorter work experience. Years of experience are also an important factor influencing the formation of attitudes towards the use of opioids, along with additional education of nurses. Other studies also point to a lack of knowledge as a major factor in the development of opiophobia.
Opiophobia is most often associated with thanatophobia, and this study confirmed a statistically significant, albeit weak, association between these phobias. This means that subjects with lower levels of opiophobia have, on average, lower levels of thanatophobia, and vice versa.
Opiophobia is more pronounced in acute care unit staff. This is also indicated by a study conducted in China, where oncology nurses showed a positive attitude towards death and were inclined to accept death as an integral part of life, not showing a strong fear of death when faced with it. However, thanatophobia is more pronounced in employees with longer working experience, which supports the fact that nurses who care for dying patients for a longer period of time also become aware of their own mortality, which causes anxiety in them.
In this study, 50% of participants with shorter working experience and 21.4% of participants with longer working experience expressed an affirmative attitude towards thanatophobia, which is in line with the results of the aforementioned study in China. The fact that working with dying patients is difficult is also indicated by the fact from this study, where the majority of participants confirmed the claim that working with dying patients had negative consequences.
The level of education of nursing staff does not indicate the level of thanatophobia. This is confirmed by a study conducted in the United Kingdom.
Fear of death is universal and present in every individual. Nurses in this study generally had a positive attitude towards death and dying. This is shown by the attitude towards the statement that they do not feel capable of caring for a dying patient, which was not accepted by the majority of participants. This is confirmed by a study conducted in Australia. The Cooper-Barnett study found that end-of-life care represents a significant stress and source of anxiety for nursing. This is also confirmed by a study from the United States. Nurses (especially in intensive care) were less prepared for the feelings and reactions that they encounter during end-of-life care. Therefore, they state that preparation for the feelings and reactions that staff encounter during their work is essential in nursing education.
In this study, we can conclude that years of experience and the work environment greatly contribute to the formation of the attitudes of medical staff. Since attitudes affect the work of nurses, it is necessary to change negative ones into positive ones in order to provide the patient with the highest quality health care. Patients facing the end of life encounter pain, one of the most difficult symptoms and a trigger for other unpleasant feelings. Therefore, the involvement of nurses in the treatment of pain and the formation of a positive attitude towards the use of opioids is important. Research indicates that one of the causes of thanatophobia and opiophobia is (still) the lack of education of medical staff.
Research Shortcomings
The research was limited to a small number of participants and was conducted in one institution, so the conclusions of this research cannot be generalized. In order to gain better insight into the factors that influence the attitudes of healthcare workers, especially nurses, in relation to opiophobia and thanatophobia, it is strongly suggested that research be continued with a larger number of respondents, in a larger number of healthcare institutions that provide palliative care for terminally ill patients, and simultaneously in several European Union countries.
Conclusion
In palliative care, patient care is provided comprehensively and according to the principles of a holistic and interdisciplinary approach. The most important goal in working with patients in palliative care is to maintain the best possible quality of life and alleviate suffering until the end of life.
In palliative care, the priority in patient care shifts from curative to palliative, and the focus is primarily on satisfying some of the patient’s most important needs, such as pain relief. This requires knowledge of good and correct pain assessment, the choice of analgesics and non-pharmacological methods of pain treatment, and finally the evaluation of care.
Patients with malignant pain require adequate therapy, which often requires the use of opioid analgesics. In our society in general, including among medical staff, there is very often a fear of developing addiction or overdose with opioids. Poor education, stigmatization.
Fear of side effects often leads to patients not receiving adequate pain therapy. Despite the presence of opiophobia, medical staff in this study demonstrated adequate knowledge about the use of opioids compared to other studies. Medical staff in palliative care departments are more likely to encounter the use of opioids, which is why they have more positive attitudes about this form of therapy.
In palliative care departments, staff also encounter dying patients more often and therefore have greater experience and different, more positive attitudes towards dying and death. The main conclusion of this study is that the cause of thanatophobia and opiophobia mainly lies in the insufficient education of medical staff, which indicates the need for greater education of staff in palliative care and pain management.
Conflicts of Interest Statement:
The authors have no conflicts of interest to declare
References
1. WHO. Palliative care. 2020. Available:
https://www.who.int/news-room/fact-sheets/detail/palliative-care
2. Demuro M, Bratzu E, Lorrai S, Preti A. Quality of Life in Palliative Care: A Systematic Meta-Review of Reviews and Meta-Analyses . Clin Pract Epidemiol Ment Health, 2024;20:e17450179183857.
doi. http://dx.doi.org/10.2174/0117450179183857240226094258
3. McCaffrey N, Bradley S, Ratcliffe J, Currow DC. What aspects of quality of life are important from palliative care patients’ perspectives? A systematic review of qualitative research. J Pain Symptom Manage. 2016;52(2):318-328.e5.
4. Wang CW, Chow AYM, Chan CLW. The effects of life review interventions on spiritual well-being, psychological distress, and quality of life in patients with terminal or advanced cancer: A systematic review and meta-analysis of randomized controlled trials. Palliat Med. 2017;31(10):883-94.
5. Kassianos AP, Ioannou M, Koutsantoni M, Charalambous H. The impact of specialized palliative care on cancer patients’ health-related quality of life: A systematic review and meta-analysis. Support Care Cancer. 2018;26(1):61-79.
6. Gaertner J, Siemens W, Meerpohl JJ, et al. Effect of specialist palliative care services on quality of life in adults with advanced incurable illness in hospital, hospice, or community settings: systematic review and meta-analysis. BMJ. 2017;357:j2925.
7. Schüchen RH, Mücke M, Marinova M, et al. Systematic review and meta‐analysis on non‐opioid analgesics in palliative medicine. J Cachexia Sarcopenia Muscle. 2018;9(7):1235-54.
8. Jamison RN, Mao J. Opioid Analgesics. Mayo Clin Proc. 2015;90(7):957-68.
9. Cohen B, Ruth LJ, Preuss CV. Opioid Analgesics. [Updated 2023]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available: https://www.ncbi.nlm.nih.gov/books/NBK459161/
10. Trujillo KA. Opiophobia and the tragedy of needless pain: A call for education and balance.
Pharmacol Biochem Behav, 2023;230:173616
11. CDC Guideline for Prescribing Opioids for Chronic Pain. MMWR. 2016; 65(1): 1–49.
12. Dowell D, Haegerich T, Chou R. No shortcuts to safer opioid prescribing. N. Engl. J. Med. 2019; 380:2285-2287.
13. Webster F, Bremner S, Oosenbrug E, Durant S, McCartney CJ, Katz J. From Opiophobia to Overprescribing: A Critical Scoping Review of Medical Education Training for Chronic Pain. Pain Med. 2017;18(8):1467-1475. doi: 10.1093/pm/pnw 352. PMID: 28371881; PMCID: PMC5914373.
14. Balasubramanian C, Subramanian M, Balasubramanian S, Agrawal A, Raveendran S, Kaliaperumal C. “Thanatophobia”: Physician’s perspective of dealing with patients with fear of death. J Nat Sci Biol Med. 2018;9(1):103-104.
15. Fulton JJ, Newins AR, Porter LS, Ramos K. Psychotherapy targeting depression and anxiety for use in palliative care: A meta-analysis. J Palliat Med. 2018;21(7):1024-37.
16. Kavalieratos D, Corbelli J, Zhang D, et al. Association between palliative care and patient and caregiver outcomes. JAMA. 2016;316(20): 2104-14.
17. Guerrero-Torrelles M, Monforte-Royo C, Rodríguez-Prat A, Porta-Sales J, Balaguer A. Understanding meaning in life interventions in patients with advanced disease: A systematic review and realist synthesis. Palliat Med. 2017;31(9):798-813.
18. Lau J, Mazzotta P, Fazelzad R, Ryan S, Tedesco A, Smith AJ, Sud A, Furlan AD, Zimmermann C. Assessment tools for problematic opioid use in palliative care: A scoping review. Palliat Med. 2021;35:1295-1322. doi: 10.1177/0269216321101 5567. Epub 2021 May 17. PMID: 34000897; PMCID: PMC8267087.
19. Guo Q, Zheng R. Assessing oncology nurses’ attitudes towards death and the prevalence of burnout: A cross-sectional study. Eur J Oncol Nurs. 2019;42:69-75. doi: 10.1016/j.ejon.2019.08.002. Epub 2019 Aug 5. PMID: 31446266.
20. Yılmaz İ, Akansel N. The Turkish form of psychometric properties of opioids questionnaire. Agri. 2022;34(2):117-130.
21. Barnett M, Mulvenon C, Dalrymple PA. Nurses’ knowledge, attitudes, and practice patterns regarding titration of opioid infusions at the end of life. JHPN. 2010;12(2):81-88.
22. Guest C, Sobotka F, Karavasopoulou A, Ward S, Bantel C. Nurses and opioids: results of a bi-national survey on mental models regarding opioid administration in hospitals. J Pain Res. 2017;10: 481-493.
23. Uwera N. Nurses’ barriers and facilitators to management of pain in children in two selected referral hospitals in Rwanda [Doctoral dissertation, University of Rwanda]. 2022. www.ur.ac.rw
24. Baldemir R, Akçaboy EY, Noyan Ö, Çelik Ş, Akçaboy ZN. Nurses Attitudes Toward Opioid Using. Bozok Med J. 2019;9(4):6-14.
25. Theodosopoulou P, Moutafi M, Kalogridaki M, Tsiamis C, Rekatsina M, Pikoulis E. Acute Pain Management and Perceptions among Emergency Healthcare Workers: Feedback from Greece. Rom J Anaesth Intensive Care. 2023;29(1):22-31. doi: 10.2478/rjaic-2022-0004. PMID: 36844961; PMCID: PMC9949016.
26. Nguyen T, et al. Impact of a pharmacist-led palliative care education program focused on the appropriate use of opioids in Vietnam. Pharm Sci Asia. 2024;49(4): 340-348.
27. Salim NA, Joshua R, AbuBaker NA, Chehab F, Jose A. Effect of a nursing in-service education program on nurses’ knowledge and attitudes towards pain management in a governmental hospital in the United Arab Emirates: Experimental random assignment study. Dubai Med J. 2019;2:146–152.
28. Wells G, Llewellyn C, Hiersche A, Minton O, Wright J. Medical student anxiety in caring for dying patients and their family: a cross-sectional study. BMJ Support Palliat Care. 2023;7;13(e2): e278-e281. doi: 10.1136/bmjspcare-2021-003331. PMID: 34518284.
29. Peters L, et al. Emergency and palliative care nurses’ levels of anxiety about death and coping with death: a questionnaire survey. Australas Emerg Nurs J. 2013;16(4):152-9. doi: 10.1016/j.aenj.201 3.08.001. Epub 2013 Sep 26. PMID: 24199900.
30. Cooper J, Barnett M. Aspectsofcaring for dyingpatientswhichcauseanxiety to firstyear student nurses. Int J Palliat Nurs. 2005;11(8):423-430.
31. Arbour RB, Wiegand DL. Self-described nursing responses experienced during care of dying patients and their families: A phenomenological study. JHPN. 2023;25(2):E49-E56.
32. Yazkan G, Ugurlu N, Birgili F. Investigation of nomophobia levels of nursing department students. EJONS Journal. 2022;6(21),118–128. doi. https://doi.org/10.38063/ejons.