





Olfactory Groove Meningioma: Case Report & Review
OLFACTORY GROOVE MENINGIOMA: CASE REPORT AND LITERATURE REVIEW
Maria Fernanda da Silva Oliveira1, Vittoria Parisi Borlenghi1, José Augusto Camargo2*
- Medical Student. Faculdade de Medicina, Pontifícia Universidade Católica de São Paulo, Brazil
- Professor, MD, PhD. Faculdade de Medicina, Pontifícia Universidade Católica de São Paulo, Brazil
OPEN ACCESS
PUBLISHED: 31 October 2025
CITATION: Oliveira, MF., et al., 2025. OLFACTORY GROOVE MENINGIOMA: CASE REPORT AND LITERATURE REVIEW. Medical Research Archives, [online] 13(10). https://doi.org/10.18103/mra.v1 3i11.6961
DOI https://doi.org/10.18103/mra.v1 3i11.6961
ISSN 2375-1924
ABSTRACT
Background: Olfactory groove meningioma is a benign intracranial tumor that originates from the arachnoid cells of the dura mater in the region of the olfactory groove. It has an insidious onset, as it grows slowly, and symptoms appear late. Objectives: To highlight an olfactory groove meningioma through a clinical case and emphasize diagnostic and therapeutic considerations. Methods: A female patient presented with behavioral changes, recent memory deficits, right homonymous hemianopia and anosmia. Imaging revealed a large, expansile extraaxial mass with a broad dural insertion base. Etiological investigation and surgical treatment were proposed. Results: The patient underwent frontal craniotomy for complete tumor resection and had a satisfactory postoperative evolution, including reversal of neurological symptoms. Conclusion: The clinical and radiological features, along with the findings, are discussed, and the literature on the management of meningiomas in this location is reviewed.
Keywords: Olfactory groove meningioma, Frontal craniotomy, Tumor resection.
Introduction
Meningiomas are mostly benign tumors that arise from the subarachnoid layer of the meninges. Tumors involving the olfactory groove account for 5.4-13% of all intracranial meningiomas. They grow over the cribriform plate and frontosphenoidal suture, located between the crista galli and planum sphenoidale anteriorly and posteriorly, respectively. Olfactory groove meningiomas tend to show a slow, broad growth from their implantation base, causing compression and displacement of the olfactory nerve.
Although the exact causes of these tumors are not fully understood, different factors can influence the emergence of meningiomas in general, including genetic predisposition, female sex, advanced age, exposure to radiation, and environmental factors. The most common symptoms vary depending on the size and location of the tumor. Typical symptoms include anosmia, changes in behavior and mental status, recent memory deficits, hemianopia, headache, and seizures.
The diagnosis is made based on clinical evaluation, imaging examinations (magnetic resonance imaging [MRI], computed tomography [CT]), and complementary tests such as cerebral angiography and biopsy, if necessary. Treatments usually involve a surgical approach consisting of frontal craniotomy for tumor resection.
Olfactory groove meningioma represents a diagnostic challenge since its insidious growth often results in nonspecific neuropsychiatric symptoms such as behavioral changes and memory deficits, whose differential diagnoses include dementia and psychiatric disorders. In the present case, the patient initially presented with fatigue, hypersomnia, and mood alterations that were misinterpreted as depressive symptoms, leading to multiple pharmacological treatments before the correct diagnosis was established. This emphasizes the importance of maintaining a high index of suspicion for intracranial structural lesions, particularly meningiomas of the anterior cranial fossa, in patients with atypical or refractory neuropsychiatric manifestations. Early neuroimaging plays a crucial role in preventing delayed diagnosis and the associated risk of irreversible cognitive and visual impairment.
Case Report
T.G, a 49-year-old, white female patient, began experiencing fatigue and hypersomnia in November 2023. In January 2024, she presented the first episode of right homonymous hemianopia, lasting approximately three minutes. During this period, she also reported marked mood change, recurrent memory lapses, and significant difficulties with concentration and daily functioning. Several antidepressant medications were prescribed, but without clinical improvement. Two months later, she developed a second episode of right homonymous hemianopia and anosmia.
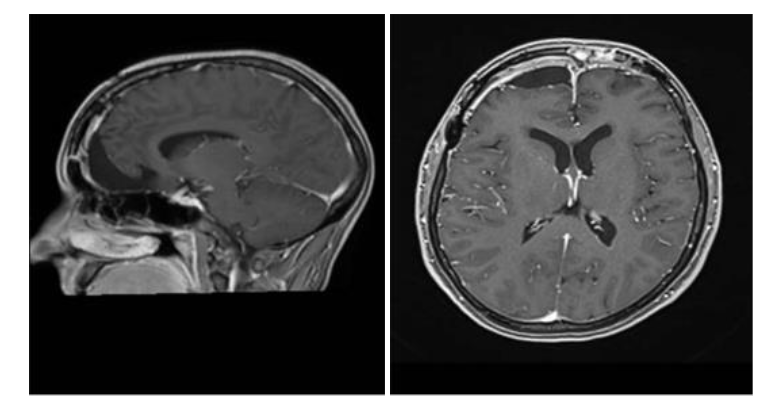
Due to these symptoms, a magnetic resonance imaging (MRI) scan of the brain was requested, which revealed a large extra-axial expansile mass with a broad dural attachment located on the floor of the anterior cranial fossa and involving the planum ethmoidale, crista galli, and olfactory groove. The mass showed a hypointense signal on both T1- and T2-weighted sequences, with intense and homogeneous enhancement after administration of gadolinium-based contrast agent. It measured approximately 5.8 × 5.0 × 4.9 cm in its largest diameters. There was compression of the anterior horns of the lateral ventricles, predominantly on the right side, in addition to a deviation of the midline structures toward the left by approximately 1.4 cm. The patient underwent a subsequent contrast-enhanced cranial MRI, which supported the diagnosis of a meningothelial lesion. Arterial and venous magnetic resonance angiography revealed a large left frontopolar vascular branch at the superior and medial margins of the lesion. Caliber asymmetry was observed between the transverse and sigmoid sinuses and cranial segments of the internal jugular veins, which were smaller on the left, probably representing hypoplasia on this side.

Surgery
A right and left frontotemporal craniotomy was performed. Using ultrasound-guided neuronavigation, the tumor was carefully dissected from the surrounding brain parenchyma, allowing for complete resection while preserving critical neurovascular structures, including the frontal lobes and optic pathways. After the 12-h CT scan, the administration of morphine was necessary because of a severe headache. The biopsy revealed grade 1 meningioma, with 90% of the tumor cells exhibiting estrogen receptor expression.
Discussion
Olfactory groove meningioma represents a diagnostic challenge since its insidious growth often results in nonspecific neuropsychiatric symptoms such as behavioral changes and memory deficits, whose differential diagnoses include dementia and psychiatric disorders. In this case, the patient initially presented with fatigue, hypersomnia, mood alterations, and recurrent memory lapses, which were misinterpreted as depressive symptoms, leading to multiple pharmacological treatments before the correct diagnosis was established. These early manifestations often mimic primary psychiatric or affective disorders, contributing to diagnostic delay. However, the later onset of anosmia and right homonymous hemianopia provided key neurological clues that indicated an underlying organic etiology. This emphasizes the importance of maintaining a high index of suspicion for structural brain lesions in patients with atypical or treatment-resistant neuropsychiatric presentations.
The compression of the frontal structures and olfactory tract explains the combination of symptoms such as anosmia, behavioral changes, recent memory deficit, right eye hemianopsia, while the right hemianopia observed in the present patient is the result of the effect of the mass on optic pathways. Due to their slow and silent growth, olfactory groove meningiomas often compress frontal structures responsible for emotional regulation, behavior, and cognition, leading to apathy, personality changes, and cognitive decline that may mimic primary mood disorders. In this case, the patient was treated for depression with no clinical improvement until neuroimaging was performed, highlighting the importance of maintaining suspicion for structural causes in atypical or treatment-resistant psychiatric presentations.
Magnetic resonance imaging (MRI) is the imaging method of choice for the identification and characterization of these tumors and is essential for surgical planning, especially in the case of large tumors with midline deviation, as in the present case. Neurosurgical treatment is aimed at complete resection of the tumor, minimizing the risk of recurrence and alleviating the compressive effect on adjacent structures. Magnetic resonance imaging also plays a central role in postoperative follow-up, enabling the evaluation of surgical success and early detection of residual or recurrent disease. In this patient, postoperative imaging confirmed complete tumor removal, correlating with marked improvement in mood, memory, and overall behavior. These findings suggest that many of the neuropsychiatric symptoms caused by olfactory groove meningiomas may be reversible once the compressive effect on the frontal and visual pathways is relieved.
Anatomopathological examination confirmed grade I meningioma, a finding that correlates with a favorable prognosis and low recurrence rate. The expression of hormone receptors in 90% of tumor cells reinforces the hypothesis of a hormonal influence on the pathophysiology of meningiomas, underscoring the importance of long-term clinical and radiological follow-up. Early diagnosis and surgical intervention are fundamental for optimizing neurological recovery and preventing irreversible cognitive decline. This case illustrates how timely neuroimaging and multidisciplinary management can significantly improve outcomes and quality of life in patients with atypical neuropsychiatric presentations secondary to olfactory groove meningioma.
Conclusion
This case report highlights the importance of early diagnosis and neurosurgical intervention for the management of olfactory groove meningiomas, whose initial presentation often involves nonspecific neuropsychiatric and cognitive symptoms that can delay diagnostic suspicion. Complete surgical resection, performed with the aid of neuronavigation and advanced microsurgical techniques, was found to be effective in reversing neurological deficits, confirming its use as the treatment of choice. Although grade I meningiomas have a low recurrence rate, prolonged clinical and radiological monitoring is essential, especially in cases with hormone receptor expression given the possible influence of sex steroids on tumor pathogenesis.
Declaration Ethical Approval and Consent to Participate
Not applicable.
PATIENT CONSENT
The patient’s consent to report this case was obtained on the condition that all details that would allow any reader to identify the person be omitted.
DATA AVAILABILITY
All data supporting the findings of this case are available within the article and referenced literature.
FUNDING
None.
AUTHOR CONTRIBUTIONS
All authors contributed equally to the conception, drafting, revision, and final approval of the manuscript.
COMPETING INTERESTS
The authors declare no competing interests.
ACKNOWLEDGEMENTS
None.
References:
- Candy NG, Hinder D, Jukes AK, Wormald PJ, Psaltis AJ: Olfaction preservation in olfactory groove meningiomas: a systematic review. Neurosurg Rev, 46:186, 2023.
- Moura FFM, Kochi S, Ferreira PJTM, Domingues RAD, Pinto CCA, Mota CAS, Silva GMR, Andrade IS: Meningiomas: ensaio pictórico dos principais locais de ocorrência do tumor primário mais comum do sistema nervoso central. Rev Foco, 17(9):e5922, 2024.
- Guimarães MLB, Nunes LAFA, Cruz NMRA, Dias GPF, Martins DANP, Baptista MAFB, Aguiar HF: Anosmia: meningioma de goteira olfatória. Anais do Hospital de Reabilitação de Anomalias Craniofaciais, Universidade de São Paulo, 2017.
- Miyagishima DF, Sundaresan V, Gutierrez AG, Barak T, Yeung J, Moliterno J, McGuone D, Claus EB, Günel M: A systematic review and individual participant data meta-analysis of gonadal steroid hormone receptors in meningioma. J Neurosurg, 139:1638-1647, 2023.
- Agopiantz M, Carnot M, Denis C, Martin E, Gauchotte G: Hormone receptor expression in meningiomas: a systematic review. Cancers (Basel), 15:980, 2023.
- Pashkov A, Filimonova E, Poptsova A, et al: Cognitive, affective and behavioral functioning in patients with olfactory groove meningiomas: a systematic review. Neurosurg Rev, 48:457, 2025.
- Alkhatib M, Hua L, Beyer F, et al: Molecular landscape and clinical correlates of olfactory groove meningiomas: a multi-institutional study. J Neurosurg, 1-9, 2025.
- Maiuri F, Corazzelli G, Berardinelli J, et al: Risk factors and surgical maneuvers to decrease recurrences of olfactory groove meningiomas: institutional case series and systematic literature review. Neurosurg Rev, 48:562, 2025.
- Fountas KN, Hadjigeorgiou GF, Kapsalaki EZ, et al: Surgical and functional outcome of olfactory groove meningiomas: lessons from the past experience and strategy development. Clin Neurol Neurosurg, 171:46-52, 2018.
- Revuelta Barbero JM, Gutierrez J, Newman S, et al: Keyhole supraorbital-eyebrow approach for resection of an olfactory groove meningioma with intraoperative endoscopic assistance. World Neurosurg, 157:160-161, 2022.
- Zenga F, Penner F, Cofano F, et al: Trans-frontal sinus approach for olfactory groove meningiomas: a 19-year experience. Clin Neurol Neurosurg, 196:106041, 2020.