






Oral Insulin: Advancing Diabetes Treatment Protocols
Oral Insulin – Harnessing the Natural Physiology of Glucose Control in the Body
Roger R C New, PhD1
- Middlesex University, London UK
- Diabetology Limited, London UK
OPEN ACCESS
PUBLISHED: 31 January 2025
CITATION: New, RRC., 2025. Oral Insulin – Harnessing the Natural Physiology of Glucose Control in the Body. Medical Research Archives, [online] 13(1). https://doi.org/10.18103/mra.v13i1.6180
COPYRIGHT: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i1.6180
ISSN 2375-1924
ABSTRACT
The aim of this paper is to highlight the ideal prerequisites for an oral insulin formulation to exert its maximal effect, by delivering insulin via the portal vein directly to the liver. A description is provided of the resulting differences in the way in which oral and injected insulins act, in order to treat type 2 diabetes. Key among these differences is the ability of the liver to control its activity in accord with the glucose concentration in the bloodstream, as a result of insulin entering the liver via the portal vein, and stimulating generation of glucokinase. The advantages this confers on multiple aspects of treatment of patients (safety, dosing, reproducibility etc) are outlined in detail. Separately, the way in which insulin, administered via the upper intestine, may overcome insulin resistance is discussed. Finally, a case is made for oral insulin to be employed for treatment of type 1 diabetes, gestational diabetes, and for co-administration with certain other anti-diabetes agents.
Keywords
Oral insulin, glucose control, type 2 diabetes, glucokinase, insulin resistance, type 1 diabetes, gestational diabetes.
Introduction
Insulin acts, in a healthy human, to control glucose disposal by binding to receptors in the liver and activating hepatocytes to respond to, and stabilise, blood glucose levels. The key benefit that oral insulin can deliver is to allow insulin to enter the body so that it binds to liver receptors in preference to other sites in the body, in the same way as insulin acts in a healthy individual. This is in contrast to the injected route, where insulin enters the outer circulation directly, with only 20% ever gaining access to the liver, the majority being taken up by muscle and adipose tissue, resulting in glucose being removed rapidly from the bloodstream, but in a poorly controlled fashion.
Ideally, oral insulin will enter the body via the intestine, so that, after crossing the gut wall, it can be drained into the portal vein, and absorbed by the liver before any insulin enters the outer circulation. However, not all orally-administered insulins achieve this feat.
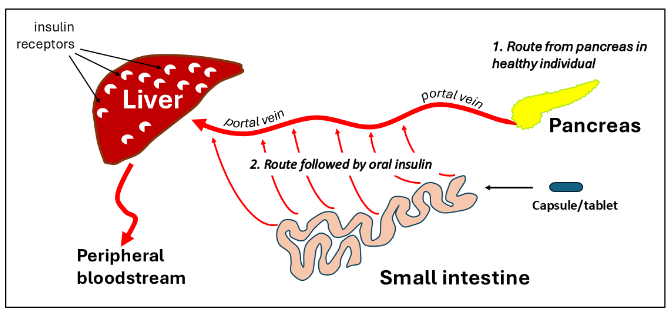
Insulin administered as a buccal spray, or a sub-lingual tablet, bypass the liver completely, entering the peripheral blood circulation in the same way as a subcutaneous injection. With insulin formulations which are swallowed, and taken up from the stomach, only a proportion may enter the portal vein, with the remainder going into the outer circulation. Even formulations which reach the intestine may not deliver insulin to the liver, since peptides associated with lipids, either covalently or non-covalently, can be shunted via the lamina propria into the intestinal lymphatics, where they are held until they flow into the outer blood circulation via the lumbar duct, avoiding contact with the liver by first pass. A schematic of the preferred route followed by insulin when administered orally is shown in Figure 1.
Importantly, a number of studies have demonstrated that, when insulin is administered to the digestive tract over long periods of time in patients with or without diabetes, the sequelae observed are entirely benign. These studies were carried out not with the aim of enhancing entry of insulin to the rest of the body, but rather of desensitising the immune system to mitigate some symptoms of diabetes. Indeed, positive outcomes were seen, but not of a magnitude sufficient to consider such an intervention a realistic treatment option.
However, the fact that daily introduction of insulin into the intestine over periods of up to two years caused no evident untoward effects in the gut has set a precedent for use of this route to act as a method of directing exogenous insulin further into the body, and in particular, towards the liver.
Comments and observations made in the passages below draw principally on data generated in studies with Diabetology’s Capsulin™ oral insulin pharmaceutical formulation, but should apply equally to other formulations meeting the criteria of an ideal oral insulin delivery vehicle as outlined above. In addition to Diabetology’s Capsulin™ formulation, specific reference is made to Biocon’s Tregopil™, and Oramed’s oral peptide platform.
1. Portal Delivery
An important first step in establishing the suitability of an oral formulation for delivery of insulin is to demonstrate that insulin is preferentially directed to the portal vein, and thence to the liver. Such a situation has been confirmed with Diabetology’s Capsulin™ formulation in a study conducted by Rheoscience AS in anaesthetised rats, where the formulation was administered in liquid form to the intestine, and insulin measured in the cannulated portal vein (see Figure 2).
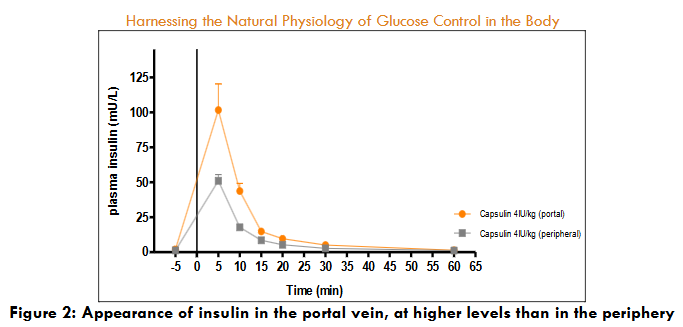
Here it is observed that the concentration in the portal vein is significantly higher than in the periphery, a situation which can only arise if the insulin enters the body first via the portal vein. In this study, the dose of insulin administered was high (4iu/kg), so it is likely that insulin appeared in the periphery after the liver was flooded with insulin and the receptors were saturated and unable to absorb all the material administered.
In a separate study using the same animal model, distribution of peptide in the body was examined with the same formulation, but containing exendin instead of insulin. Since exendin is not taken up by liver cells to any significant extent, the difference between portal and peripheral blood concentrations of peptide are easier to interpret. Table 1a shows values of Cmax in both the portal vein and periphery after administration of formulated exendin via the intestine, and of exendin in free solution via the intravenous route. As can be seen, for intravenous administration of exendin, the ratio of concentration in the outer circulation relative to the portal vein is close to 1, as is to be expected, while for the intestinal route, a ratio of greater than 3 is observed.
| Blood pool | Intravenous Exendin (2.5μg) | Intestinal Exendin (25μg) | Exendin (25μg) intestinal | Insulin (40μg) intestinal |
|---|---|---|---|---|
| Portal | 4 | 10 | 9.5 | 17.5 |
| Peripheral | 3 | 3 | 2 | 2 |
| Ratio (portal/peripheral) | 1.33 | 3.33 | 4.8 | 8.8 |
In the same study, a formulation containing both insulin and exendin at the same time was administered via the intestinal route. From the data shown in table 1b, while the concentration ratio of portal to peripheral is again greater than 1 for exendin (4.8), the ratio for insulin is significantly higher (8.8), demonstrating the effect of extraction of insulin from the bloodstream by the liver before it enters the outer circulation. Again, the insulin dose administered was relatively high – it is likely that, with lower doses, higher levels of extraction would be seen, as observed in human studies.
It is important to be aware that, in cases such as insulin, where there are many receptors in the liver, a bioavailability based on concentrations measured in the outer blood circulation is not a good reflection of the extent of delivery of this molecule, as a result of extraction by the liver when administered via the intestine. Consequently, in comparing the efficacy of different oral delivery platforms, it is important to measure parameters of insulin biopotency rather than bioavailability. For the most successful oral insulin formulation, the biopotency is probably between 10 and 20%.
2. Control mechanisms coming into play when insulin is delivered to the liver, in contrast to the periphery.
2.1 CONTROL BY MUSCLE AND ADIPOSE CELLS
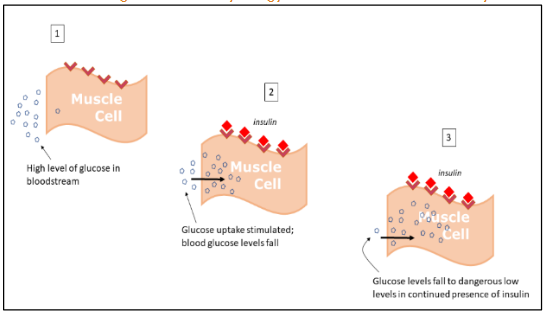
When insulin is injected, administered sublingually or inhaled, in treatment of patients with Type 2 diabetes, the insulin enters the bloodstream and binds to receptors on the surface of muscle cells and adipose tissue cells. This stimulates those cells to take up glucose to metabolise it, and in the process removes excess glucose from the bloodstream. High and prolonged exposure of these cells to insulin results in rapid glucose uptake which continues for as long as insulin is present, with the rate of glucose uptake and metabolism being determined by the size of the insulin dose. For this reason, if too high a dose of insulin is administered there is a risk of blood glucose depletion below safe levels, which can result in life-threatening hypoglycaemia. A schematic of the process of glucose uptake by muscle cells is shown in Figure 3.
2.2 CONTROL BY LIVER CELLS
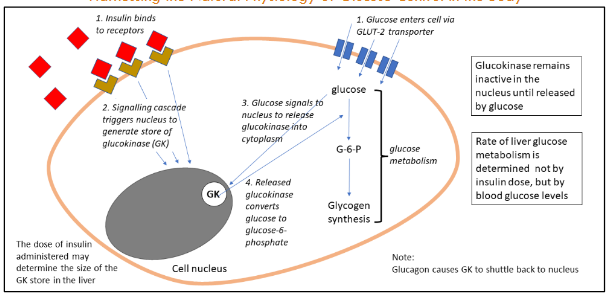
In contrast to injected insulin, control of glucose by administration of insulin orally works in a completely different way. Instead of focussing on uptake by muscle cells, oral insulin targets the liver – the organ in the body designed by Nature to control blood glucose levels, under the influence of insulin (see Figure 4 below).
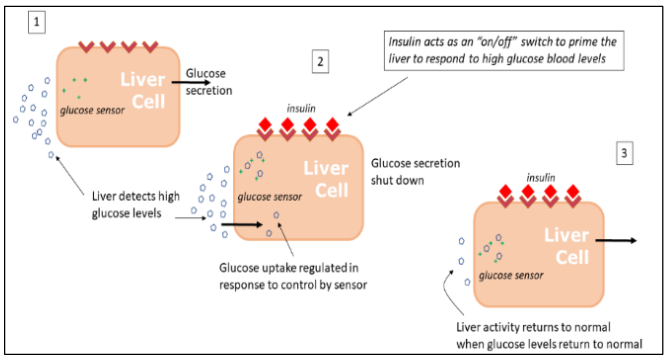
Because the majority of insulin administered in this way becomes bound to the receptors in the liver, only a small amount passes into the peripheral bloodstream. This avoids high, non-physiological, levels of insulin entering the outer circulation, which could lead to long-term vascular side effects and weight gain.
The liver regulates blood glucose levels in a safer and much more efficient way than that employed by muscle cells or adipose tissue. This is because liver cells have a sensing mechanism for glucose, which can distinguish between high and low levels of glucose in the bloodstream. It is the concentration of glucose which determines the level of glucose metabolic activity inside the liver cell, and this relationship provides a mechanism for preventing blood glucose from falling too low, and from reaching unsafe levels.
2.3 ROLE OF GLUCOKINASE IN THE LIVER
The molecule which plays a key role in the control of glucose by the liver is glucokinase (GK). GK is an enzyme which catalyses the first stage of conversion of glucose to its metabolites, eventually leading to synthesis of stored glycogen, or breakdown via pyruvate to provide energy. The role of insulin is to initiate the generation of a reservoir of GK in the nucleus of the liver cell. This GK is stored in the form of an inactive complex with a repressor molecule, and does not participate in conversion of glucose. Only when the glucose in the cytoplasm becomes elevated, and interacts with the GK/GK repressor complex, is the GK released into the cytoplasm, where it can then act on the glucose to convert it to metabolites. The rate of glucose conversion is dependent on the amount of GK in the cytoplasm, and is thus controlled not by the insulin dose, but by the concentration of glucose itself, since the more glucose is present, the more GK can be released from the store in the nucleus.
3. Impact of Glucokinase Control Mechanism on Behaviour of Portally-Transported Oral insulin
3.1 NO NEED FOR TITRATION
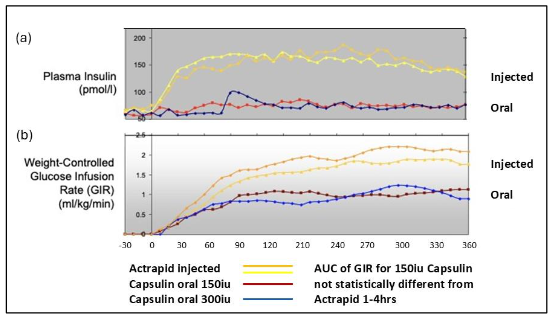
One corollary of the mechanism in liver hepatocytes outlined above is that titration on the basis of glucose intake or blood sugar levels should not be necessary. Regardless of the dose of insulin administered, the rate of response of the liver is governed by the concentration of glucose in the bloodstream, so that, within limits, the rate of hepatic glucose disposal is constant, once sufficient insulin has been administered to trigger the insulin receptors maximally. This is seen clearly in a study conducted with two doses of oral insulin (150 and 300iu) administered prior to an isoglycaemic clamp. In Figure 6b, it can be seen that glucose disposal, as measured by glucose infusion rate (GIR), is similar irrespective of the magnitude of the insulin dose administered. This is because, in this clamp study, the mean blood glucose levels at the start of the clamp were identical regardless of which group the patients were assigned to, and blood glucose levels remained constant throughout the experiment as a result of the clamp being maintained.
In healthy individuals, the normal daily insulin output of the pancreas is about 45iu. In patients with Type 2 diabetes receiving Diabetology’s Capsulin™, two capsules of 150iu each are administered per day (300iu in total). Since the biopotency of insulin in the Capsulin™ formulation is between 10 and 20%, this means the liver in patients receiving Capsulin™ will be exposed to levels of insulin very similar to those achieved in normal subjects. It is worth mentioning that, while insulin levels are close to low base-line levels in the outer circulation, after administration of oral insulin, they are not reduced to zero, and there is considered to be sufficient insulin present to enable muscle cells to use this hormone to assist in glucose uptake in exercise (in both Type 1 and type 2 diabetes patients), as in a healthy individual. In this respect, it is worth noting that glucose is taken up by muscle cells via two different membrane transporter proteins, GLUT1 and GLUT4, of which the former is insulin independent, and which contributes to a significant proportion of glucose uptake under normal conditions.
3.2 AVOIDANCE OF LONG-TERM SYSTEMIC SIDE EFFECTS
This study showed a marked effect on glucose disposal in the absence of significant levels of insulin in the outer blood circulation, as is to be expected, if the mechanism for glucose disposal is due to insulin binding to liver receptors, rather than receptors on peripheral tissues. This is in contrast to injected insulin, where high prolonged levels of insulin were seen in the outer circulation. Preclinical studies have demonstrated that defects in glucose metabolism caused by peripheral insulin delivery can be corrected when insulin is targeted to the liver. One can expect that long-term side effects of insulinaemia in the periphery will also be reduced. Such side effects may include weight gain, retinopathy, nephropathy, neuropathy, macro-vascular disorders leading to amputation, as well as cancer and reduced life-span.
3.3 SAFETY OF ORAL INSULIN – AVOIDANCE OF HYPOGLYCAEMIA
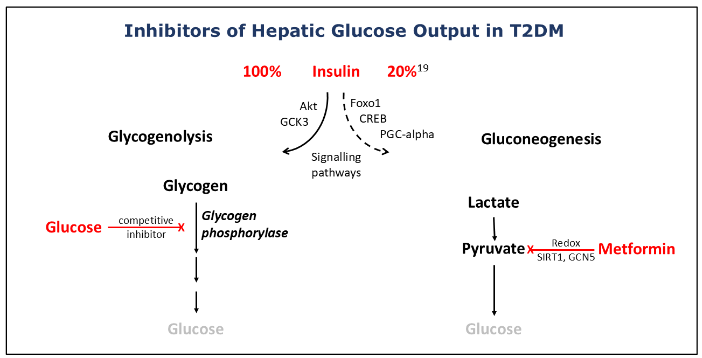
The rate of glucose uptake by the liver is a process which is determined (with the assistance of insulin) by the concentration of glucose itself in the bloodstream. The same is true for glucose output by glycogenolysis, which is mediated by the enzyme glycogen phosphorylase, for which glucose at high concentrations is a competitive inhibitor. Thus, as the concentration of glucose in the bloodstream reaches a safe level, the restrictions on glucose disposal between the bloodstream and the liver will be relaxed, the rate of reduction of glucose in the outer circulation will be reduced, and the possibility of hypoglycaemia averted. In 25,000 dosing events in Diabetology’s phase 2b study, not a single incidence of clinical hypoglycaemia was recorded. Biocon observed lower levels of clinical hypoglycaemia in their recent trial with Tregopil compared with injected insulin aspart. Oramed also noted no increase in hypoglycaemia compared with placebo in their phase 2b study with ORMD-0801.
The avoidance of hypoglycaemia with oral insulin is important, since the risk of such potentially life-threatening events is a major reason for delay in use of injected insulin in Type 2 Diabetes until later stages of the disease. This is in spite of the fact that many studies have shown that, even with injected insulin, an intensive course of insulin is beneficial when given at an early stage in the progression of the disease. With the availability of a form of insulin which does not pose a risk of hypoglycaemia, there are strong arguments for oral insulin to be employed as one of the first lines of treatments, for example alongside metformin. Type 2 diabetes patients in Diabetology’s phase 2b trial were indeed at an early stage – within two years of diagnosis, and poorly controlled on metformin – and responded well to treatment with oral insulin. Patients recruited into the trial conducted by Biocon were also at an early stage in the progression of the disease.
3.4 DURATION OF ACTION
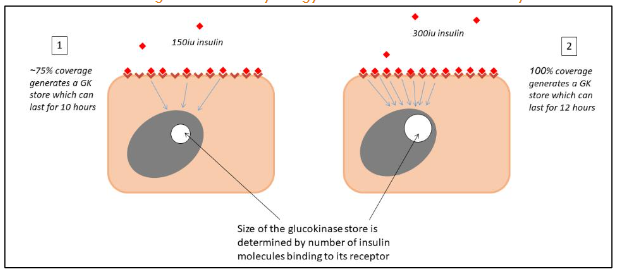
The higher the dose of insulin, the larger will be the pool of GK generated, which may explain why the duration of action of Capsulin™ in a clamp study appeared to be dependent on the insulin dose (9-10 hours for 150iu; 12-14 hours for 300iu).
3.5. REPRODUCIBILITY
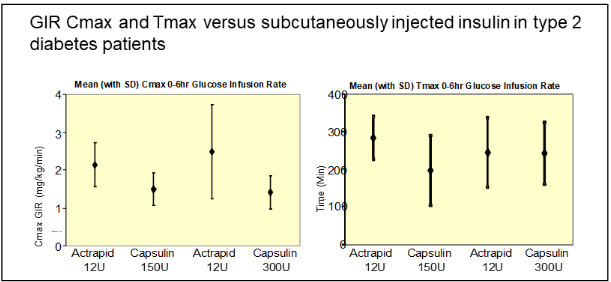
The ability of the liver to exert its effect (via glucokinase) in accord with blood glucose concentration, rather than insulin levels administered, leads to a high degree of reproducibility of response. A demonstration of the interpatient reproducibility of Capsulin™ treatment is provided by data gathered from the phase 2a clamp study described in Figure 6 above, conducted in T2DM patients poorly controlled on other oral anti-diabetes agents. Biological efficacy was determined by looking at Glucose Infusion Rates, and two measures were employed (Cmax and Tmax) to compare the variability of response between injected insulin (Actrapid) and Capsulin™. The variability is assessed not by the magnitude of the responses achieved, but by the size of the error bars associated with these responses. In Figure 9 it can be seen that the error bars are of similar magnitude for both oral and injected modes of administration, indicating that the response elicited by Diabetology’s Capsulin™ delivered via the oral route is as reproducible as that when insulin is injected.
4. Overcoming insulin resistance
Most studies conducted with various forms of oral insulin to date have not reported any reductions in cholesterol or triglycerides. This is an important parameter in patients with diabetes, since this group often has high levels of triglycerides, and recently, a high ratio of triglycerides (TG) to high-density lipoprotein (HDL) cholesterol has been proposed as an indicator of insulin resistance, with a value of 3.5 acting as a cut-off point. In the phase 2b trial carried out by Diabetology, The TG:HDL ratio decreased from 3.8 to 3.45, indicating a possible influence of treatment on insulin resistance. This is important, firstly because insulin resistance is one of the primary factors implicated in onset of Type 2 diabetes, but also because use of insulin to treat patients with diabetes is going to be less than optimal if their resistance to insulin is high.
Insulin resistance is initiated and/or perpetuated by three different factors:
- High levels of glucose in the bloodstream
- High levels of plasma insulin, and
- High levels of plasma triglyceride
As treatment with oral insulin progresses, these factors can be mitigated in the following ways.
- Both fasting plasma glucose and post-prandial glucose concentrations are generally reduced as treatment progresses. In Diabetology’s phase 2b study, fasting plasma glucose levels decreased to those corresponding to the prediabetes threshold (126mg/dL) in a large number of patients, after twelve weeks of treatment.
- More importantly, high levels of insulin in the outer circulation are avoided, because oral insulin directed via the portal vein delivers insulin directly to the liver, where it is absorbed before it can enter the peripheral bloodstream. This has been demonstrated in Diabetology’s phase 2a clamp study. In so doing, the need for excessive secretion of insulin from the pancreas is reduced, raising the possibility of sparing this organ from potential exhaustion, which can manifest later as the disease progresses.
- Finally, as has also been seen in Diabetology’s phase 2b study, triglyceride levels are markedly reduced after 12 weeks. This is significant, since the breakdown products of triglycerides – diacyl glycerides and certain free fatty acids – are instrumental in promoting insulin resistance in a range of different tissues.
The proposed mechanism of lipid reduction is as follows: elevated blood triglycerides are thought to derive in large part from overproduction and secretion of chylomicrons from enterocytes. This process is usually held in check by homeostatic mechanisms involving insulin and GLP-1 signalling, but is dysregulated in patients with insulin resistance. It has recently become apparent that the duodenum is an important focus of insulin resistance, and that insulin resistance is brought about through stimulation of inflammatory and oxidative processes at this site. Insulin itself is known to have both anti-inflammatory and anti-oxidative properties, independent of its role in control of glucose metabolism, and it is possible that, because of these actions, administration of insulin via the duodenum may be able to reverse insulin resistance at this site, and lower secretion of triglyceride-containing chylomicrons by enterocytes, leading to lowering of triglycerides in the bloodstream.
It is to be expected that blood levels of triglycerides and low-density lipoprotein (LDL) cholesterol will continue to fall as treatment continues beyond twelve weeks, and to reach normal levels typical of healthy individuals. In some cases (particularly triglycerides with the 150iu dose) this target has already been attained in Diabetology’s study. As a result, all three factors perpetuating insulin resistance, as listed above, will start decreasing after onset of treatment, leading to the expectation of an increase in sensitivity to insulin over time, resulting in ever greater efficacy of oral insulin as treatment continues, and particularly a progressive lowering of glycated haemoglobin HbA1c.
5. Next Steps
5.1 TREATMENT OF TYPE 1 DIABETES AND GESTATIONAL DIABETES
The majority of the discourse above has been directed towards, and exemplified by, the treatment of type 2 diabetes. This does not mean that oral insulin does not have a role to play in type 1 diabetes as well. The concern regarding the possibility of inducing hypoglycaemia with injected insulin is as present with Type 1 diabetes as with Type 2 diabetes, if not more so, even when patients are being treated with insulin administered via a pump. As outlined above, oral insulin will be able to eliminate this concern, through the safety mechanisms intrinsic in liver control of glucose disposal, while at the same time providing the requirements for insulin (perhaps through administration of two or three capsules per day), both in response to glucose peaks during meals, and to maintenance of glucose at basal levels in between mealtimes. Oral insulin should be superior to injected insulin in terms of mitigating the risk of hypoglycaemia due to insulin overdosing. The main question would be the extent to which oral insulin could react to a sudden spike in blood glucose. Injected insulin will provide a more rapid response than oral, although it is doubtful whether such a rapid response will be necessary in such cases. Experience shows that, even with oral insulin, a capsule can pass through an empty stomach into the intestine within ten minutes, and enter the body shortly thereafter, showing rises in the blood stream in type 1 diabetes patients within 30 minutes. Further studies to investigate this approach are merited, to determine whether oral insulin can be used as either a partial or complete replacement for injected insulin, and under what conditions.
It is worth noting that insulin is the treatment of choice for gestational diabetes, even in preference to common medications such as metformin, and an oral insulin will be highly advantageous as a safer alternative to injected insulin.
5.2 CO-ADMINISTRATION WITH OTHER PEPTIDES – EG GLUCAGON-LIKE PEPTIDE 1 RECEPTOR AGONISTS (GLP-1 RAS)
In the field of diabetes and obesity, the current trend is to combine two or more different peptide therapies to achieve an additive, or even synergistic enhancement in efficacy. The same is possible with insulin. Indeed, there is a strong rationale for combining insulin with other agents which act on or in the intestine, since oral insulin is already being delivered via the intestinal route. In this context, one obvious candidate for combination with insulin is a glucagon-like peptide-1 receptor agonist (GLP-1 RA). Data from treatment modalities combining these two agents in injected form have already suggested that there is an advantage in putting them together. However, the benefit is likely to be much greater if they are both administered orally via the gut.
| GLP-1 | Insulin |
|---|---|
| Activates glucose sensor in the portal vein | Helps liver respond to glucose gradient across liver |
| Inhibits gluconeogenesis in liver (reducing glucose output) | Inhibits glycogenolysis in liver (reducing glucose output) |
| Normalises glucagon levels | Works in combination with glucagon to maintain glucose within safe range (no hypos) |
| Generates glucokinase stores in the liver to control glucose uptake – eliminating the need for titration |
6. Discussion and conclusions
From the discussion above, it is clear that there are important differences between insulin administered orally and injected insulin, arising from the fact that oral insulin follows more closely the natural physiology of glucose control, and behaves in a similar fashion to endogenous insulin. This behaviour needs to be taken into account when evaluating the results of preclinical and clinical studies. Because insulin is absorbed by the liver, when delivered via the portal vein, concentrations in the bloodstream are kept at a low level (comparable to baseline physiological levels) so that estimation of the efficacy of oral insulin on the basis of blood levels is a mistake. Whether an oral insulin formulation is effective or not can only be determined by looking at blood glucose levels and change in HbA1c.
Because oral insulin is targeting the liver, the kinetics of glucose change are different from injected, both in the short and the long term. Muscle tissue reacts very rapidly to an increase in insulin levels, resulting in dramatic falls in glucose within minutes. In contrast, the liver reacts more slowly, and in humans may take several hours to bring about the same degree of change. Furthermore, control of glucose uptake into the liver by glucokinase ensures that precipitous falls in blood glucose levels do not occur even when relatively high doses of insulin are administered, in contrast to injected insulin where the possibility of inducing life-threatening hypoglycaemia is always a worry, even in patients using insulin pumps.
In the long term, for reasons outlined above, there is the possibility that avoidance of high levels of insulin in the outer circulation, coupled with falls in triglycerides, will lead to a reduction in insulin resistance, so that the efficacy of insulin will increase over time. However, this will be a slow process, and it is likely that, in order to see maximal effects of oral insulin, studies beyond the standard three months time period will need to be conducted. The potential for reduction of side effects of insulin (avoidance of hypoglycaemia, reduction of micro- and macrovascular issues) leads to the possibility, in contrast to injected insulin, of administering oral insulin not just at the later stages, but also at an early stage in the progression of type 2 diabetes. This is supported by observations that early intensive courses even of injected insulin can improve prognosis in diabetes patients.
| Parameters for Insulin Treatment | Oral Insulin | Injected Insulin |
|---|---|---|
| Biopotency | ✓ | ✓ |
| Cost of goods low* | ✓ | ✓ |
| Patient friendly | ✓ | ✗ |
| Avoids high insulin blood levels | ✓ | ✗ |
| No hypoglycaemic events* | ✓ | ✗ |
| Can avoid side effects of insulinaemia | ✓ | ✗ |
| Absence of cardiovascular implications | ✓ | ✗ |
| No need for titration | ✓ | ✗ |
| Weight neutral | ✓ | ✗ |
| Stability at room temperature* | At least 6 months | 1 month |
* Specifically for Diabetology’s Capsulin™ oral insulin formulation
7. Methodology
7.1 STUDIES IN RODENTS
In a collaboration with Synovo GmbH, adult Wistar rats, average weight 380g, employed in groups of five for each test article, were acclimatised for seven days, and maintained on a restricted diet for one day prior to anaesthesia. Each animal was then surgically manipulated to allow cannulation of the portal and tail veins, and peptides at doses of 25μg per animal (exendin) and 40μg (insulin) dissolved in a solution of Diabetology’s oral delivery formulation components were instilled via a syringe into the intestine. In a separate group of animals exendin was administered via intravenous injection at a dose of 2.5μg per animal. At timed intervals after administration of peptides, blood samples were taken, and peptide concentrations measured by ELISA. Further details can be found in the publication by New et al.
7.2 HUMAN GLUCOSE CLAMP STUDY
The study comprised sixteen male patients with type 2 diabetes poorly controlled on oral antidiabetic medications, including metformin. Patients were randomly allocated, in cross-over fashion, to groups receiving, on two occasions separated by eleven days, injected insulin (12 iu Actrapid) on one day, and either 150iu or 300iu of Capsulin™ on the other day. Patients fasted overnight for ten hours, and all medications were withheld, prior to conduct of the 6 hour isoglycaemic clamp, during which glucose infusion rate and plasma insulin levels were measured at regular intervals. Patients had an average weight BMI of 28.3, age 60.2 years and HbA1c of 7.4%. Further details can be found in the publication by Luzio et al.
References
- Ergun-Longmire B, Marker J, Zeidler A, Rapaport R, Raskin P, Bode B, Schatz D, Vargas, A, Rogers D, Schwartz S, Malone J, Krischer J, Maclaren NK. Oral Insulin Therapy to Prevent Progression of Immune-Mediated (Type 1) Diabetes. Ann. N.Y. Acad. Sci. 2004; 1029: 260–277.
- The Diabetes Prevention Trial – Type 1. Effects of Oral Insulin in Relatives of Patients With Type 1 Diabetes. Diabetes Care. 2005;28:5 1068-1076.
- New RRC, Bogus M, Travers GN, Hahn U, Vaiceliunaite A, Burnet M, Wang JH and Wen H. Glucagon-like peptide-1 receptor agonists for treatment of diabetes and obesity: advantage of oral delivery. Front. Drug Deliv. 2024;4:1456654. doi: 10.3389/fddev.2024.1456654.
- Massa ML, Gagliardino JJ, Francini F. Liver Glucokinase: An Overview on the Regulatory Mechanisms of its Activity. IUBMB Life. 2011;63(1): 1–6.
- Kaminski MT, Schultz J, Waterstradt R, Tiedge M, Lenzen S, Baltrusch S. Glucose-induced dissociation of glucokinase from its regulatory protein in the nucleus of hepatocytes prior to nuclear export. Biochimica et Biophysica Acta. 2014;1843:554–564.
- Matschinsky FM, Wilson DF. The Central Role of Glucokinase in Glucose Homeostasis: A Perspective 50 Years After Demonstrating the Presence of the Enzyme in Islets of Langerhans. Front. Physiol. 2019;10:148.doi: 10.3389/fphys.2019.00148.
- Luzio SD, Dunseath G, Lockett A, Broke-Smith TP, New RR, Owens DR. The glucose lowering effect of an oral insulin (Capsulin) during an isoglycaemic clamp study in persons with type 2 diabetes Diabetes, Obesity and Metabolism. 2009 doi: 10.1111/j.1463-1326.2009.01146.x.
- Zhang AMY, Wellberg EA, Kopp JL, Johnson JD. Hyperinsulinemia in Obesity, Inflammation, and Cancer. Diabetes Metab J. 2021;45:285-311. doi.org/10.4093/dmj.2020.0250.
- Edgerton DS, Scott M, Farmer B, Williams PE, Madsen P, Kjeldsen T, Brand CL, Fledelius C, Nishimura N, Cherrington AD. Targeting insulin to the liver corrects defects in glucose metabolism caused by peripheral insulin delivery. JCI Insight. 2019; 5: e126974.
- Kolb H, Kempf K, Röhling M, Martin S. Insulin: too much of a good thing is bad. BMC Medicine. 2020;18:224. doi.org/10.1186/s12916-020-01688-6.
- New RRC, Ramanujam S, Chaudhari V, Bogus M, Travers GN. Namjoshi G. Safety and Efficacy of an Oral Insulin (Capsulin) in Patients with Early-Stage Type 2 Diabetes: A Dose-Ranging Phase IIb Study. Diabetes Obes Metab. 2022;1–8.
- Lebovitz HE, Fleming A, Cherrington AD, Joshi S, Athalye SN, Loganathan S, Vishweswaramurthy A, Panda J, Marwah A. Efficacy and Safety of Tregopil, a Novel, Ultra-Rapid Acting Oral Prandial Insulin Analog, as Part of a Basal-Bolus Regimen in Type 2 Diabetes: A Randomized, Active Controlled Phase 2/3 Study. Expert Opinion on Pharmacotherapy. 2022; doi: 10.1080/14656566.2022.2141569.
- Eldor R, Francis BH, Fleming A, Neutel J, Homer K, Kidron M, Rosenstock J. Oral Insulin (ORMD-0801) in Type 2 Diabetes Mellitus: Dose-Finding 12-Week Randomized Placebo-Controlled Study. Diabetes, Obesity and Metabolism 2022 doi.org/10.1111/dom.14901
- Weng JP, Li YB, Xu W, Shi LX, Zhang Q, Zhu DL, Hu Y, Zhou ZG, Yan X, Tian HM, Ran XW, Luo ZJ, Xian J, Yan L, Li FP, Zeng LY, Chen YM, Yang LY, Yan SJ, Liu J, Li M, Fu ZZ, Cheng H. Effect of intensive insulin therapy on β-cell function and glycaemic control in patients with newly diagnosed type 2 diabetes: a multicentre randomised parallel-group trial. Lancet. 2008;371: 1753–60.
- Meneghini LF. Early Insulin Treatment in Type 2 Diabetes: What are the pros? Diabetes Care. 2009;32:S226-269.
- Owens DR. Clinical Evidence for the Earlier Initiation of Insulin Therapy in Type 2 Diabetes. Diabetes Technology and Therapeutics. 2013; 15: 776-785 DOI: 10.1089/dia.2013.0081
- Kramer CK, Zinman B, Retnakaran R. Short-term intensive insulin therapy in type 2 diabetes mellitus: a systematic review and meta-analysis. The Lancet, Diabetes & Endocrinology. 2013;1:28-34.
- Zhang W, Wang HD, Liu FC, Ye X, Tang WJ, Zhang PZ, Gu TW, Zhu DL, Bi Y. Effects of Early Intensive Insulin Therapy on Endothelial Progenitor Cells in patients with Newly Diagnosed Type 2 Diabetes. Diabetes Ther. 2021; https://doi.org/10.1007/s13300-021-01185-w.
- Gastaldelli A, Toschi E, Pettiti M, Frascerra S, Quiñones-Galvan A, Sironi AM, Natali A, Ferrannini E. Effect of Physiological Hyperinsulinemia on Gluconeogenesis in Nondiabetic Subjects and in Type 2 Diabetic Patients. Diabetes 2001;50:1807-12
- Bertsch RA, Merchant MA. Study of the use of lipid panels as a marker of insulin resistance to determine cardiovascular risk. Perm J. 2015;19:4-10.
- Pantoja-Torres B, Toro-Huamanchumo CJ, Urrunaga-Pastor D, Guarnizo-Poma M, Lazaro-Alcantara H, Paico-Palacios S, Ranilla-Seguin VDC, Benites-Zapata VA. High triglycerides to HDL-cholesterol ratio is associated with insulin resistance in normal-weight healthy adults. Diabetes Metab Syndr Clin Res Rev. 2019;13:382-388.
- Petersen MC, Shulman GI. Mechanisms of insulin action and insulin resistance. Physiol Rev. 2018; 98:2133–223.
- Mary Sugden M, Holness M Pathophysiology of diabetic dyslipidemia: implications for atherogenesis and treatment. Clinical Lipidology, 2011;6:4, 401-411, DOI: 10.2217/clp.11.32.
- Stahel P, Xiao C, Nahmias A and Lewis GF. Role of the Gut in Diabetic Dyslipidemia. Front. Endocrinol. 2020;11:116. doi: 10.3389/fendo.2020.00116.
- Sun Q, Li J, Gao F. New insights into insulin: The anti-inflammatory effect and its clinical relevance. World J Diabetes. 2014;April 15; 5(2): 89-96.
- Song Y, Ding W, Bei Y, Xiao Y, Tong HD, Wang LB, Ai LY. Insulin is a potential antioxidant for diabetes-associated cognitive decline via regulating Nrf2 dependent antioxidant enzymes. Biomed Pharmacother. 2018;Aug;104:474-484. doi: 10.1016/j.biopha.2018.04.097.
- Rademaker D, de Wit L, Duijnhoven RG, Voormolen DN, Mol BW, Franx A, DeVries JH, Painter RC, van Rijn BB, SUGAR-DIP Study Group. Oral Glucose-Lowering Agent vs insulin for Gestational Diabetes: A Randomized Clinical Trial. JAMA 2024; doi:10.1001/jama.2024.23410.
- Whitelaw DC, Kelly CA, Ironmonger W, Cunliffe C, New R, Phillips JN. Absorption of orally ingested insulin in human type 1 diabetic subjects: proof of concept study. Diabetes. 2005;54(suppl 1):5-LB.
- Balena R, Hensley IE, Miller S, Barnett AH. Combination therapy with GLP-1 receptor agonists and basal insulin: a systematic review of the literature. Diabetes, Obesity and Metabolism, 2013;15: 485–502.
- Risovic I, Sumarac Dumanovic MS, Bojic M, Djekic D. Direct comparison two fixed-ratio combination glucagon-like peptide receptor agonist and basal insulin on glycemic and non glycemic parameters in type 2 diabetes. BMC Endocrine Disorders. 2023;23:28. https://doi.org/10.1186/s12902-023-01282-w.
- Aroda VR, Aberle J, Bardtrum L, Christiansen E, Knop FK, Gabery S, Pedersen SD, Buse JB. Efficacy and safety of once-daily oral semaglutide 25 mg and 50 mg compared with 14 mg in adults with type 2 diabetes (PIONEER PLUS):a multicentre, randomised, phase 3b trial. The Lancet. 2023;402, Issue 10403P693-704August 26.
- Eldor R, Kidron M, Greenberg-Shushlav Y, Arbit E. Novel Glucagon-Like Peptide-1 Analog Delivered Orally Reduces Postprandial Glucose Excursions in Porcine and Canine Models. J Diabetes Sci Technol. 2010;4(6):1516-1523.