






Osteoporosis and Proximal Junctional Failure in Spine Surgery
Osteoporosis is a Risk Factor for Proximal Junctional Failure Following Long Spinal Fusion for Adult Spinal Deformity
Sharaf Mohanty, MD1; Amnol Gupta, MD, MBA1; Harold Fogal, MD1; Daniel Tolbert, MD1; Stuart Hershman, MD1
- Department of Orthopaedics, Massachusetts General Hospital, 55 Fruit Street, Boston MA 02114
OPEN ACCESS
PUBLISHED: 31 January 2025
CITATION: MOHANTY, Sarthak et al. Osteoporosis is a Risk Factor for Proximal Junctional Failure Following Long Spinal Fusion for Adult Spinal Deformity. Medical Research Archives,Available at: <https://esmed.org/MRA/mra/article/view/6199>.
DOI: https://doi.org/10.18103/mra.v13i1.6199
ISSN 2375-1924
Abstract
With a globally aging population, the prevalence of adult spinal deformity (ASD) is rising. Since 2005, rates as high as 63% have been reported in geriatric patients, affecting quality of life of over 28 million elderly individuals. The rate of corrective surgery for ASD, aimed at preventing progressive deformity, relieving pain, improving self-image, addressing cardiopulmonary comorbidities, and decompressing neurologic elements, increased by 141% since the early 2000s. This rise was predominantly driven by a 460% rise in the incidence of long-segment deformity correction in the elderly subsegment. Despite advancements in the safety of deformity correction, proximal junctional failure (PJF) remains a significant complication following adult spinal deformity correction. Among these complications, radiographic and clinical outcomes are particularly concerning, affecting 61% and 24% of patients, respectively. We hypothesized that osteoporosis is a significant risk factor for PJF following long spinal fusion for ASD.
Keywords
- Osteoporosis
- Proximal Junctional Failure
- Long Spinal Fusion
- Adult Spinal Deformity
Introduction
With a globally aging population, the prevalence of adult spinal deformity (ASD) is rising. Since 2005, rates as high as 63% have been reported in geriatric patients, affecting quality of life of over 28 million elderly individuals. The rate of corrective surgery for ASD, aimed at preventing progressive deformity, relieving pain, improving self-image, addressing cardiopulmonary comorbidities, and decompressing neurologic elements, increased by 141% since the early 2000s. This rise was predominantly driven by a 460% rise in the incidence of long-segment deformity correction in the elderly subsegment. Despite advancements in the safety of deformity correction, proximal junctional failure (PJF) remains a significant complication following adult spinal deformity correction. Among these complications, radiographic and clinical outcomes are particularly concerning, affecting 61% and 24% of patients, respectively. We hypothesized that osteoporosis is a significant risk factor for PJF following long spinal fusion for ASD.
Data Collection
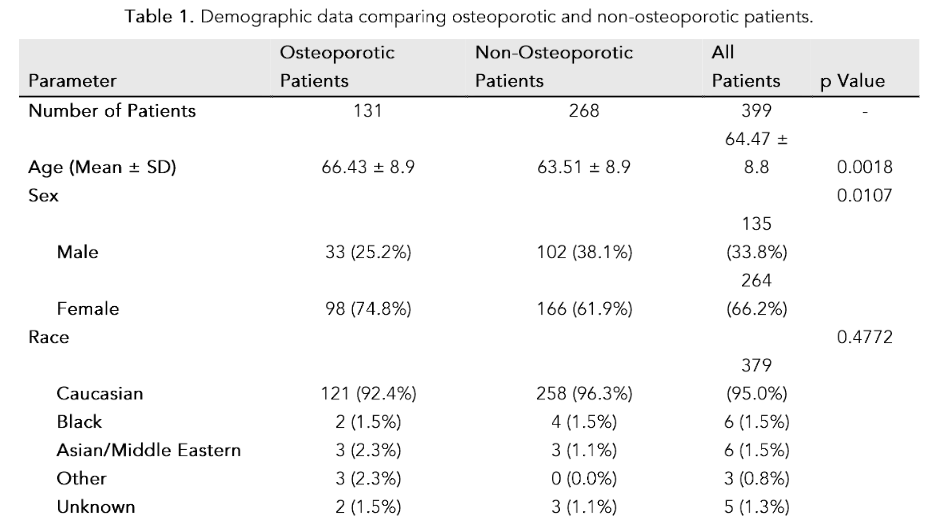
Patients with adult spinal deformity (ASD) who underwent long spinal fusion were included in the study. Eligible patients met at least one of the following radiographic and/or clinical criteria: pelvic incidence minus lumbar lordosis (PI-LL) ≥20°, T1 Pelvic Angle (TPA) ≥20°, Sagittal Vertical Axis (SVA) ≥4 cm, scoliosis ≥50°, global coronal malalignment ≥6 cm, undergoing a three-column osteotomy, or spinal fusion involving a revision surgery. Exclusion criteria included those with active spine tumors or infections, spinal deformity secondary to trauma, inflammatory or congenital conditions, and those undergoing surgery deemed inappropriate at the surgeon’s discretion.
Results
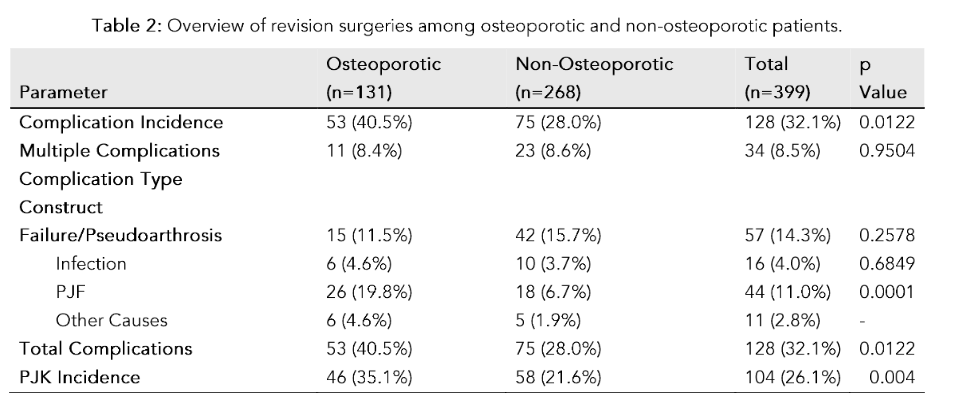
Similarly, osteoporotic patients exhibited higher rates of construct failure (PJF) (18.9% vs. 6.5%, p < 0.0001). However, the incidence of construct failure/pseudarthrosis and infection did not differ significantly between groups (11.5% vs. 15.7%, p = 0.578; 4.6% vs. 3.7%, p = 0.684, respectively). Complications attributed to other causes were rare in both groups, accounting for 4.6% in osteoporotic and 1.9% in non-osteoporotic patients.
Limitations
Our study controlled for demographic and clinical differences between osteoporotic and non-osteoporotic cohorts. Early complications are predominantly considered in this study, while long-term outcomes remain to be evaluated. Future studies should aim to evaluate PJF in the context of osteoporosis treatment.

| Parameter | Osteoporotic Patients (n=268) | Non-Osteoporotic Patients (n=399) | P-Value |
|---|---|---|---|
| Construct Failure/Pseudarthrosis | 15 | 8 | 0.458 |
| Infection | 6 | 7 | 0.773 |
References
- Safe MM, Ames CP, Smith JS. Perioperative Hounsfield Units at the Planned Upper Instrumented Vertebra May Predict Proximal Junctional Kyphosis in Adult Spinal Deformity. Neurosurgery. 2020;87:275-283.
- Schwab F, Dubey A, Gamez L, et al. Adult scoliosis: prevalence, SF-36, and anatomical parameters in an elderly volunteer population. Spine (Phila Pa 1976). 2005;30(9):1082-1085. doi:10.1097/01.brs.0000160242.34824.c2.
- Koller H, Franz C, Meier O, et al. Factors influencing radiographic and clinical outcomes in adult scoliosis surgery: a study of 448 European centers. Eur Spine J. 2016;25(2):532-548. doi:10.1007/s00586-013-2810-4.
- Yagid M, Ohno H, Konomi T, et al. Teriparatide improves volumetric bone mineral density and fine bone structure in the UIV-1 vertebra, and reduces bone failure type PJK after surgery for adult spinal deformity. Osteoporos Int. 2017;26(12):3495-3502. doi:10.1007/s00198-016-3778-0.