





Parental Influence on Adolescent Eating Disorders and Mental Health
Relationship between Parental Behavior, Depression, Anxiety, Body Satisfaction and Eating Disorder in the Period of Adolescence
Gordana Stankovska1 Aferdita Ahmeti 2
- Faculty of Humanities and Social Sciences, International Balkan University, Skopje, Republic of North Macedonia
- Faculty of Psychology, AAB College, Republic of Kosovo
OPEN ACCESS
PUBLISHED: 31 January 2025
CITATION: STANKOVSKA, Gordana; AHMETI, Aferdita. Relationship between Parental Behavior, Depression, Anxiety, Body Satisfaction and Eating Disorder in the Period of Adolescence. Medical Research Archives Available at: <https://esmed.org/MRA/mra/article/view/6215>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i1.6215
ISSN 2375-1924
ABSTRACT
Introduction: Adolescence is a period of life in which a person grows and matures. It is a period of turbulent changes and a transition from childhood to adulthood. The changes that occur in a young person on a somatic, mental and psychological level affect the person’s anorexic or bulimic behavior.
Objective: To determine the relationship between the symptoms of eating disorders, anxiety, depression, body satisfaction, and parental behavior.
Material and methods: The study involved 240 respondents between 15 and 18 years of age, first year and third year students in two secondary schools in Skopje. During the study, we used the following measurement instruments: Eating Attitude Test, Perception of Parents Scale, Body Shape Questionnaire, Kutcher Adolescent Depressive Scale, The State – Trait Anxiety Inventory and Body Mass Index.
Results: The obtained results show the existence of interconnection between anxiety, depression, body satisfaction and family factors in relation to eating disorders and body mass index. Simultaneously, we determined that there was a difference in terms of involvement, autonomy support and parental warmth between the low-risk group and the critical group of respondents on the EAT – 26 scale. Anxiety, depression, maternal warmth and autonomy support from both parents were found to be predictors of the occurrence of eating disorders.
Conclusion: The implementation of adequate preventive programs will enable the young person to develop a healthy attitude towards nutrition, changes in personal appearance, body, and health.
Keywords
Parental Behavior, Depression, Anxiety, Body Satisfaction, Eating Disorder, Adolescence
Introduction
The nutrition process is a process that involves experiences of the external and internal world, and is therefore related to experience and emotions from the earliest stages of personality development. From the very birth of a child, the mouth is a mature and adaptive organ. Immediately after birth, it is ready to receive milk – food that creates a feeling of comfort and satisfaction. Initially, this ritual represents self-satisfaction of a biological need (hunger), however later it transforms into emotional satisfaction and interpersonal characteristics. The mother-child dyad is a source of satisfaction of all the child’s needs, biological, psychological and social. The child’s further psychological development, stability, and trust in other types of relationships with the outside world depend on the quality of this relationship. Disrupted interaction contributes to the child’s feeling of guilt, reduced self-esteem, behavioral problems or eating disorders.
When speaking of eating disorders, adolescents are a special group, and due to the various specificities of their life period (a period of intense physical, sexual, emotional, psychosocial and cognitive changes), the risk of developing symptoms of a certain type of eating disorder is increased in this age group. Obsession with weight is a mark of our time, especially among young girls, who have normal weight and still perceive themselves as fat. In recent decades, anorexia nervosa and bulimia nervosa have become particularly widespread, more so among girls than boys. Preoccupation with physical appearance and achieving socially imposed standards of physical beauty is emphasized in early adolescence, however it continues throughout all life periods. Dieting in modern society is a normal occurrence, but at the same time it is a central component for the development of eating disorders, such as anorexia nervosa and bulimia nervosa. Disturbed patterns of behavior and functioning related to food and one’s own body negatively affect the daily functioning of the person who suffers from such disorders. Eating disorders are associated with various psychological constructs, hence in attempts to discover the causes of their occurrence, various biological and genetic factors, personality factors, socio-cultural and family factors have been recognized. A young person with an eating disorder experiences changes on a psychological level, but also behavioral changes that are associated with increased dissatisfaction with their appearance and increased body weight, therefore it is necessary to develop adequate preventive programs aimed at adequate treatment and lifestyle changes.
EATING DISORDER AND DISTURBED RELATIONSHIP WITH FOOD DURING ADOLESCENCE
Adolescence is a period of life in which a person grows and matures. It is a period of turbulent changes and a transition from childhood to adulthood. This life phase is a significant, decisive period in the life of every individual. Fluctuations and changes occur during this period; therefore, the adolescent changes the role and conquers new roles – from a child the person becomes an adult. During the period of adolescence, separation occurs, identity is formed, sexuality and work responsibility are acquired.
During this period, the formation of the image of one’s own body takes place, which represents the young person’s mental image of their own physical appearance, its evaluation, the influence of perceptions and behavioral attitudes. The image of one’s own body is a multidimensional construct that contains internal (biological and psychological) and external (cultural and social) factors. Dissatisfaction with one’s own body image is developed, which represents a discrepancy between the perceived and ideal self, and the bodily experience affects the formation and maintenance of identity. Therefore, if the image of one’s own body in adolescents is negative, various negative emotions and beliefs, reduced self-esteem, depressive and anxiety symptoms, anorexia nervosa or bulimia nervosa occur.
Anorexia nervosa is a syndrome that usually occurs at the beginning of puberty or in mid-adolescence, more frequently in girls, with an unclearly defined pathogenesis, however it is considered that its occurrence is the result of the action of multiple factors, from biopsychological to socio-cultural factors. Wenar speaks of a multidimensional model that leads to the emergence of anorexia nervosa. The cited factors include intrapersonal factors (female gender, lack of autonomy, fear of maturation, insecurity, feeding difficulties in early life, rigid thinking), interpersonal factors (overprotective parental attitudes, parents focused on success, parents in conflict, depressed and impulsive parents), higher-order factors (pressure to succeed), and stimulatory factors (loss of self-esteem and self-control, new and unfamiliar factors such as sexual intimacy).
In the developmental clinical perspective, emphasis is placed on the excessive control of the child, which begins in infancy. The child grows up as exemplary, obedient and attentive person at home, popular and successful at school, however with a lack of autonomy and individuality. Namely, the child lives life according to the parental image of what is considered correct behavior, there any sign of resistance on his/her part leads to an unpleasant situation. The little person believes that he/she lives through parental values and desires. Adolescence as a main developmental task leads to the formation of an independent identity, which is a particularly disturbing phase in the development of adolescent girls. A young girl tries to solve her problems by modifying her body through food intake instead of directly confronting the close adult who is responsible for the problems, which is the cause for the development of anorexia symptoms.
The fear of gaining weight now turns into a phobia of food (not-consumption of high-calorie foods), the use of medications with the sole purpose of reducing appetite, excessive exercise, and therefore the image of one’s own body in the anorexic person is not realistic. At the same time, the young person experiences changes on a somatic and psychological level, such as anxiety, depression, decreased self-esteem, and increased feelings of guilt. Binge eating disorder – purging or bulimia is a psychological disorder characterized by an obsessive preoccupation with weight. There are episodes of binge eating, accompanied by a feeling of loss of control when consuming large amounts of food rapidly, followed by a period of laxatives, diuretics, fasting, or increased physical activity. The young bulimic person is strongly focused on body shape and weight, with accompanying fear of gaining weight, as well as a negative self-assessment in relation to their body. In addition to the developmental difficulties, problems with separation, i.e. separation of the self from the object, denial and fear of separation and sexuality come to the fore, which is why bulimia is described as a disorder that occurs due to the unsuccessful adaptation to the demands of adolescence.
Psychosocial factors show that stress plays a major role as a precipitating factor in the development of bulimia nervosa. Psychological factors include disrupted family relationships, child abuse and neglect, and certain conflicts in early childhood. Psychologists and psychiatrists who support the psychodynamic theory for the development of bulimia believe that the psychological rigidity of the person is the main reason for the sadistic attack on one’s own body, which is a main characteristic associated with this disorder. Studies shows that the mental and psychological changes that occur in the young person – the adolescent – affect their bulimic behavior. The person reacts more intensely to negative events, has lower self-esteem, increased feelings of anger, rage, fear or resentment, problems related to autonomy and personality characteristics.
An individual may suffer from different types of eating disorders throughout their life, and may experience different subsequent disorders, and may not show a sufficiently pronounced clinical features for the diagnosis of anorexia nervosa and bulimia nervosa, but what is common to all eating disorders are intertwined attitudes about body weight and eating control with similar present problems such as: self-destruction of one’s own body, inadequate emotional control followed by anxiety and depression, or the presence of anger and hostility.
FAMILY RELATIONSHIPS – RISK FACTORS FOR EATING DISORDERS
Along with the biological drive, the need for offspring of each person is thought out, it is rationally, ethically and religiously grounded. A person understands the role and meaning of offspring, delights in his/her children, feels abundance of parental love, accepts each of his/her children, takes care of them, raises and educates them. The feeling of motherhood and fatherhood, the feeling of parenthood has its biological roots, but also a much deeper humanized meaning, connected with human consciousness and conscience. Therefore, we say that parenthood is a continuous process of interaction between the parents and their child, which is a process in which both parents and children undergo mutual changes. Each parent binds his desires, hopes, and visions with his/her offspring. The child needs an emotional connection with persons he/she finds dearest – his own parents. The child needs the parental smile, touch, play, meetings, conversations. Without this, a child is in a bad mood, restless, sad. From the very first contact with children, based on their reactions, we can conclude which ones were surrounded by the joyful rays of love and understanding, and which ones were surrounded by coldness in their parental home.
The lack of parental authority affects family relationships, which are characterized by anarchy and hopelessness. This certainly has consequences for the psychological structure of the young person, which can lead to mental health disorders, the emergence of antisocial behavior, or the emergence of eating disorders, which come to the fore during adolescence, when the physical appearance of adolescent changes from childish appearance to the appearance of an adult person.
A large number of studies show that in the population with eating disorders, disturbed attachment patterns are present, with the dominant pattern being insecure attachment to parents. In the etiology of eating disorders, the most important factors have been shown to be self-competence, body dissatisfaction, and dieting, all of which are based on parental actions, parental modeling of behavior, family interactions, and the child’s attachment to the parent.
Attachment styles in infancy and childhood are an important factor that continues to affect developmental characteristics in adulthood, laying the foundations for security, social acceptance, and overall satisfaction with life. Adolescence is a period in which the attachment style continues to be expressed, although the young person strives for autonomy and independence from the parent. A large number of adolescents continue to perceive their parents as sources of security and support in conditions of stress and difficulties; hence research confirms that there is a connection between the attachment style in adolescence and eating problems. This is where the connection between eating disorders and attachment style arises; therefore the insecure attachment style dominates in a young anorexic or bulimic person. In adolescence, there is an increased need for autonomy and separation from parents, and these expressed needs come into conflict with the functioning of the person with a developed insecure attachment, reduced emotional warmth and support, as well as conflicting relationships with parents which are risk factors for the emergence of body dissatisfaction and dieting, while positive relationships with parents are associated with a positive body image. Disrupted parental relationships lead to conflicting relationships and impaired communication with the young person, which is a condition for the emergence of anorexia or bulimia nervosa. Therefore, it is necessary to recognize the family as a potential resource that should be included in intervention strategies.
Koteva-Mojsovska describes the family environment and dynamics as a significant factor in the emergence of an eating disorder. According to her, anorexia is the result of a protest against the attempt to express autonomy if parents show an overprotective, imposed and controlling attitude towards the young person without any possibility for self-expression. Parents who are emotionally warm towards their children, full of understanding and interest, who provide an explanation of the discipline they require and who do not use physical punishment, together with the child they build common rules, and replace the authority of power with the authority of value. Therefore, parenting is a pleasure for these parents and children grow up without traumatic experiences, with confidence, readiness for active participation and taking responsibility, they easily overcome stressful and frustrating situations.
On the other hand, parents who openly show negative feelings, have a constantly critical attitude towards the child, make a large number of demands, do not understand the motives for the child’s behavior, do not respect the child’s needs, severely punish their children, belittle them and do not pay enough attention to them, contribute to the development of neurotic disorders in the young person, including anorexia nervosa and bulimia. The family of a bulimic person is described as less cohesive and expressive, rather conflicting and insecure, which leads to the development of insecurity and fear. Due to unhealthy relationships with parents, the young person does not develop a positive self-image, as well as a reduced need for positive evaluation of the environment. Therefore, there is a threat that social pressure, high self-criticism and the desire for a thin body will come to the fore. Reduced communication and suppression of emotions lead to silent protest, the symptoms of which are manifested through anorexia or bulimia, which become a lifestyle. Identification with parents in many life situations is blocked at a healthy level; therefore, the young person experiences a feeling of rejection. Dieting or overeating is a defense against the conflict associated with separation/individualization. In this way, the adolescent expresses his/her anger, fear, anxiety, directs his/her own sadistic thoughts towards himself/herself, which results in the dependent need to overeat, purge or diet.
EATING DISORDERS AND PSYCHOLOGICAL PROBLEMS IN ADOLESCENCE
Adolescence is a period in which a young person faces numerous developmental tasks, such as fitting into the peer group, separation from the family and building a personal identity. The adolescent becomes familiar with his/her own personality, begins to be objective to oneself and his/her flaws, which is very important for personal emotional development. Integrating different views into a single homogeneous image is a difficult process and therefore a conflict arises that is experienced as stressful, which leads to conflicting relationships between parents and children – adolescents. Low self-esteem, intertwined with unfavorable relationships at home, school failure and stressful events in other social domains lead to unpleasant experiences in the young person.
Many adolescents, faced with the challenges of adolescence, internalize their problems, which become visible through anxiety, depression, loneliness, and suicidal ideation, while others will externalize them through an increased threshold for frustration, aggression, or other types of inappropriate behavior. At the same time, adolescence itself affects the quality of daily functioning of young people, it disrupts the process of growth and maturation, and leads to mental disorders, such as eating disorders.
The most problematic types of eating disorders involve starvation, dieting, binge eating, purging behavior, induced vomiting, and abuse of laxatives or diuretics, which are accompanied by severe emotional distress to the individual and to their environment. This leads to the emergence of anorexic or bulimic behavior, which is characterized by permanent and pathological changes in eating habits.
Numerous studies confirm that socio-cultural pressure from family, peers, and the media contributes to the emergence of body dissatisfaction and negative consequences, especially in vulnerable young people with a characteristic psychological profile. The psychological profile is characterized by the emergence of overestimated ideas about the meaning of physical appearance and body weight, which is the result of inadequate self-assessment (they see themselves differently than their environment sees them). This thinking style contributes to the person believing that they are fat or very thin, therefore body dissatisfaction is associated with problematic eating habits, perception, and loss of self-control when eating, dieting, or overeating. An anorexic or bulimic young person has a negative self-image, i.e. a distorted image of their own appearance. Every day the person seeks evidence to support the false mental image he/she has within himself/herself, which contributes to reduced self-esteem, increased inferiority and the emergence of certain mental disorders.
The most pronounced comorbidity with anorexia and bulimia are depressive and anxiety disorders. Weight loss is usually associated with feelings of sadness, decreased energy, sleep problems, decreased sexual interest, and increased obsessiveness, while overeating generates shame, guilt, sadness, and self-criticism. Negative emotions contribute to the young person’s withdrawal, feeling sad or angry because of their below-average or above-average body weight. At the same time, the person becomes worried and anxious, and experiences increased internal unrest and conflict, which the individual resolves by overeating or starving, thus reducing the feelings of anxiety and depression. Anxiety and depression disrupt the normal psychosocial development of the individual, leading to difficulties in the family, school, and social environment.
Methods
STUDY DESIGN AND PARTICIPANTS
According to the subject of study, the study is theoretical – empirical. The approach is analytical, because the subject matter is quite complex and encompasses several biological, psychiatric and psychological entities. The main goal of the research was to examine the relationship between the symptoms of eating disorders with anxiety, depression, body satisfaction and parental behavior.
The research was conducted on a convenient sample of 240 respondents (120 male and 120 female respondents), first and third year students in two high schools in Skopje, the capital of Republic of North Macedonia during the summer semester of the academic year of 2023/24. The entry criterion for inclusion in the study was the age of the subjects, whereby the required age was between 15 and 18 years, while the criterion for exclusion from the study referred to subjects with severe somatic disorders who are on a special diet.
INSTRUMENTS
We used the following measurement instruments for the purposes of this study:
- Eating Attitude Test – EAT 26
The Eating Attitude Test – EAT 26 is a 26-item assessment scale designed to identify symptoms of eating disorders in respondents. The scale itself consists of three subscales: Bulimia and Food Preoccupation (6 items) which is indicative of food thoughts and bulimic behavior, Dieting (13 items) which refers to the pathological avoidance of high-calorie foods, and Oral Control (7 items) which refers to self-control during food intake. A score above 20 is considered critical. The scale has a Cronbach’s alpha of 0.76. - Perception of Parents Scale – POPS
The Perception of Parents Scale – POPS consists of 21 items regarding involvement, autonomy support and warmth on the part of the mother, as well as 21 items regarding involvement, autonomy support and warmth on the part of the father. Involvement refers to parental availability and interest in the child’s life; support refers to stimulating freedom of choice, the development of autonomy and independence; while warmth refers to parental display of love for the child. Cronbach’s alpha of the subscales relating to the mother ranged from 0.84 to 0.89, while for the father it ranged from 0.79 to 0.81. - Body Shape Questionnaire – BSQ
The Body Shape Questionnaire – BSQ consists of 34 items that relate to body concerns. The scale has a Cronbach’s alpha of 0.79. - Kutcher Adolescent Depressive Scale (KADS)
The Kutcher Adolescent Depressive Scale (KADS) is a self-assessment scale for depression in adolescents. It consists of 11 items, with responses scored on a 4-point scale: from 0 – never to 4 – always. The range of possible scores is from 1 to 33 points, with higher scores indicating higher levels of depression. The Cronbach’s alpha for the entire scale is 0.94. - The State – Trait Anxiety Inventory (STAI)
The State – Trait Anxiety Inventory (STAI) is a scale for measuring anxiety. It consists of 40 statements, with responses scored on a 3-point scale: from 1 – never to 3 – always. It has two subscales: Trait anxiety – STAI-T and State anxiety – STAI-S. A higher score indicates a higher level of anxiety. Cronbach’s alpha for the scale is 0.82. - Body Mass Index (BMI)
We obtain the body mass index when we divide body weight expressed in kilograms by the square of body height expressed in meters.
DATA COLLECTION PROCESS
The study was conducted during the summer semester (April – June 2024). The study itself was conducted on the school premises, the subjects participated voluntarily and the right to anonymity was respected. Before starting the study and administering the tests to the respondents, the researcher explained to them the main purpose of the study and that the data would be used for research purposes, and then they were given verbal and written instructions.
The statistical analysis of the data was performed by using the SPSS software package (Statistical Package for the Social Science, version 20). Descriptive statistics were used to analyze the data, so quantitative measures were expressed as mean ± standard deviation. Pearson correlation was used to find out the relationship between the body mass index and symptoms of eating disorders with anxiety, depression, body satisfaction and parental behavior. One-way Analysis of Variance (ANOVA) was done to determine the significance of the difference between means and standard deviations between the groups of participants on the EAT 26 questionnaire according to mother and father involvement, autonomy support and warmth. The coefficient of multiple correlations is a measure of how well a given variable can be predicted using a linear function of a set of other variables. In this study it was used to find which variables were significant predictors of eating disorder symptoms. The significance levels were accepted as .01 or .05.
Results
The study involved 240 respondents, 120 (50%) male and 120 (50%) female, from 15 to 18 years of age, students in the first and third year of high school. In our sample, most of the respondents, i.e. 138 (57.50%) had a normal body mass index (8.50-24.99 kg/m2), 26 (10.836%) had a reduced body mass index (15.00-18.49 kg/m2), 42 (17.53%) had slightly increased body mass index (25.00-29.99 kg/m2), while 34 (14.17%) has significantly increased body mass index (30.00-35.00 kg/m2).
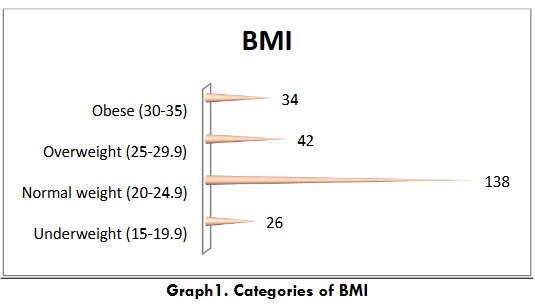
Table 1 shows the average value of the examined variables. As one can see from the presented table, the average value obtained for the symptoms of eating disorders is M=16.36 (SD=3.45), bulimia and food preoccupation M=5.24 (SD=2.67), dieting M=6.99 (SD=2.68) and oral control M=4.13 (SD=2.15). On the other hand, the mean value of anxiety is M=71.15 (SD=9.34), body satisfaction M=116.53 (SD=7.43) and depression M=19.52 (SD=9.56). At the same time, in the same table, we can see that among adolescents, in terms of parental perception, the most prevalent among the respondents is the support of autonomy by the mother and father (M=41.16, SD=9.15; M=38.16, SD=8.34), while among both parents, emotional warmth is the least prevalent (M=33.18, SD=7.34; M=28.12, SD=6.36).
| Construct | Scale | N | Mean ± SD | Range of results |
|---|---|---|---|---|
| Eating disorder symptoms | EAT-26 | 240 | 16.36 ± 3.45 | 0 – 45 |
| Bulimia and food preoccupation | BFP | 240 | 5.24 ± 2.65 | 4 – 11 |
| Diet | Diet | 240 | 6.99 ± 2.68 | 3 – 15 |
| Oral control | ORC | 240 | 4.13 ± 2.15 | 2 – 7 |
| Parental perceptions | POPS | 240 | 34.12 ± 7.32 | 4 – 38 |
| Mother involvement | Mother involvement | 240 | 41.16 ± 9.15 | 6 – 57 |
| Mother autonomy support | Mother autonomy support | 240 | 33.18 ± 7.54 | 5 – 37 |
| Father involvement | Father involvement | 240 | 30.17 ± 7.05 | 4 – 35 |
| Father autonomy support | Father autonomy support | 240 | 38.16 ± 8.34 | 4 – 38 |
| Anxiety | STAI | 240 | 71.15 ± 9.34 | 31 – 115 |
| Trait Anxiety | STAI – T | 240 | 37.11 ± 6.15 | 16 – 54 |
| State Anxiety | STAI – S | 240 | 34.04 ± 6.02 | 14 – 52 |
| Body satisfaction | BSQ | 240 | 116.23 ± 7.43 | 20 – 196 |
| Depression | KADS | 240 | 19.52 ± 9.56 | 8 – 29 |
| BMI | BMI | 240 | 23.21 ± 2.15 | 17 – 27 |
Table 2 shows the interrelationships of the examined variables: anxiety, body satisfaction, and depression in relation to body mass index, bulimia and food preoccupation, dieting, and oral control. The results show that there is a significant relationship between body mass index, the total score of eating disorder symptoms, bulimia and food preoccupation, diet, and oral control in relation to anxiety, trait anxiety, state anxiety, body satisfaction and depression at the .05 and .01 levels.
| Pearson’s correlation | STAI | STAI – T | STAI – S | BSQ | KADS |
|---|---|---|---|---|---|
| BMI | -0.23* | 0.13** | 0.31* | -0.28** | 0.43* |
| EAT -26 | 0.25** | -0.57* | 0.61** | -0.67** | -0.64** |
| Bulimia | 0.35** | 0.68** | -0.42** | 0.31* | -0.45* |
| Diet | -0.12** | 0.65* | 0.43* | 0.43** | 0.64** |
| Oral control | -0.15** | 0.51** | 0.25** | 0.45* | -0.14** |
From Graph 2 we can see that in the total sample of 240 respondents, 132 (55%) belong to the low-risk group (EAT score ≤9), 65 (27.08) belong to the medium risk group (EAT-26 score ≤18) and 43 (17.92) belong to the critical group (EAT-26 score ≥19).
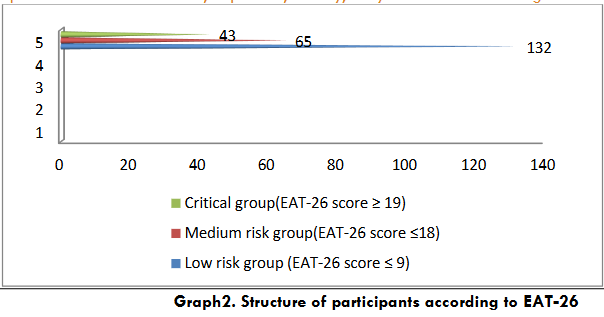
Table 3 shows the results of the three groups of respondents of the EAT-26 questionnaire in terms of perceived involvement, autonomy support and warmth from the mother. As expected, the low-risk group of respondents shows higher maternal involvement M=32.16 than the critical group M=26.15. On the other hand, the critical group of respondents has lower mean value in terms of autonomy support and warmth from the mother compared to the low-risk group.
| N | M | SD | F | df | p | |
|---|---|---|---|---|---|---|
| Mother involvement | Low risk group | 132 | 32.16 | 6.32 | 2 | 0.823 |
| Medium risk group | 65 | 30.71 | 6.86 | |||
| Critical group | 43 | 26.15 | 7.24 |
Table 4 shows the results obtained by the three groups of respondents divided according to the results of the EAT-26 questionnaire in terms of involvement, autonomy support and warmth from the father. The results show that there is no difference in involvement and warmth from the father in terms of the severity of eating disorder symptoms, however there is a difference in terms of autonomy support.
| N | M | SD | F | df | p |
|---|---|---|---|---|---|
| Father involvement | Low risk group | 132 | 30.26 | 7.31 | 0.632 |
| Medium risk group | 65 | 29.99 | 7.76 | ||
| Critical group | 43 | 27.42 | 8.34 |
From the presented data in Table 5 we can notice that the multiple correlation coefficient (R=.265) is statistically significant (F=2.134, p<.05). The predictors explained 13.2% of the variance in relation to the criterion variable ‘eating habits’, which shows a coefficient of determination R2 of .132. Anxiety, depression, maternal warmth, and autonomy support from both parents were shown to be significant predictors of eating disorder symptoms.
| Predictors | r | β | p | R | R2 | F | p |
|---|---|---|---|---|---|---|---|
| Anxiety | 0.345** | 0.216 | 0.00** | 0.265 | 0.132 | 2.134 | 0.003* |
| Body satisfaction | -0.261 | 0.156 | 0.24 | ||||
| Depression | 0.061* | -0.232 | 0.04* | ||||
| Mother involvement | -0.243 | -0.263 | 0.18 | ||||
| Mother autonomy support | 0.125 | 0.314 | 0.00** | ||||
| Mother warmth | 0.213** | 0.014 | 0.00** | ||||
| Father involvement | 0.034 | 0.231 | 0.56 | ||||
| Father autonomy support | 0.124* | 0.328 | 0.02* | ||||
| Father warmth | 0.240 | 0.251 | 0.38 |
Discussion
The current knowledge in psychiatry and psychology unequivocally indicates that the experiences that a person acquires early in life are reflected later on their functioning. A child does not have enough experience and knowledge that are important for creating a realistic image of oneself. Children build their self-image by collecting information only from the reactions of others towards them, including their parents. All messages, feelings, gestures and actions during this period are conveyed to the child by the parents; the child passively receives them and believes in them. The assessments the child receives from the parents become the child’s self-assessments that he/she retains during adolescence. The experiences the child acquires enable him/herto make certain changes in his/her self-image, which changes the most during adolescence. In a young person, the difference between the perceived and the ideal body appearance increases, which contributes to the development of body dissatisfaction, which is one of the factors for the development of anorexia or bulimia. This affects the identity of the person, whereby dieting and the desire to be thin are the basis for reducing feelings of powerlessness by disciplining one’s own body.
In this study, we attempted to analyze the relationship between psychological problems present in adolescence, such as anxiety, depression, body satisfaction, perceived parental behavior, and eating disorders, which include anorexia and bulimia nervosa. The origins of anorexia and bulimia have not yet been sufficiently studied; however, it is known that they are interplay of factors that lead to the destabilization of the emotional state of the young person.
Based on the results of the EAT-26 questionnaire, we divided the respondents into three groups based on the severity of eating disorder symptoms. According to the obtained results, 65 adolescents achieved a score between 10 and 19 on the EAT-26 questionnaire, which means they are included in the medium-risk group for developing an eating disorder, while if the criticality limit is taken as a score above 19, then 43 respondents belong to the critical group for developing bulimic behavior. However, the majority of the respondents have healthy eating habits, i.e. they constitute the low-risk group for developing an eating disorder in the period of adolescence, in which various emotional and cognitive changes occur, followed by individualization, the need for autonomy, building personal identity, one’s own values and attitudes.
Studies confirm that adolescents with anorexia or bulimia are pathologically preoccupied and dissatisfied with their bodies, which affects the development of anxiety, depression, low self-esteem, withdrawal or isolation. Our obtained results confirm that anxiety, depression and body satisfaction are important predictors of the occurrence of eating disorders. The data coincide with the findings of certain studies that assume that anxiety and depression precede the occurrence of anorexia and bulimia. A history of anxiety or depressive disorders is very often found in individuals who already have anorexia and bulimia. In a young person with anorexia nervosa, ego anxiety occurs and acts as a signal that warns of internal danger that arises due to the intrapsychic conflict between the instinctive activity of the id (neurotic anxiety), the prohibition of the superego (moral anxiety) and the demands of the external environment (reality anxiety), which is an eating disorder. Depressive mood contributes to changes in the personal, academic and social aspects of the young anorexic or bulimic person.
Modern studies confirm that the family context has a certain influence on the occurrence of eating disorders. The child’s connection with his parents, especially with the mother, determines his psychosocial and biological development. Therefore, family relationships are considered risk factors for the occurrence of mental disorders, including eating disorders. The results of our research show that the low-risk and critical groups of respondents on the EAT-26 questionnaire differ in terms of the perception of involvement, support for autonomy and warmth from the mother and father. The low-risk group of respondents has a higher score on all three subscales compared to the critical group of adolescents. The emotional warmth and acceptance of adolescents by both parents contributes to the young person feeling loved, which enables the person to easily build identity and develop autonomy.
Adolescents who are accepted and receive emotional support are more successful in developing as independent individuals. By accepting their child as he or she is, parents enable the child to build a kind of protection for his/her ego against threats and disparagement in the environment. The trust that parents show towards the child is the basis for building their personal self-confidence. This contributes to the adolescent being prepared to face the negative, stressful and harmful influences of the environment. However, at the same time, a conflict arises in the adolescent between the desire for their own autonomy and the need for parents, their support and guidance in building their personality. This contributes to adolescents feeling anxious and depressed, they rarely use problem-solving strategies, cognitive restructuring and in stressful situations they do not have parental support, therefore they are a risk group for developing an eating disorder. Hence, an adolescent with anorexic or bulimic disorder needs nutritional, pharmacological and psychological treatment, which will enable the resolution of problems related to inappropriate eating habits, perception and change of thoughts that will contribute to the establishment of a new and normal, balanced eating pattern, change of personal appearance and food, body and health.
Conclusion
Eating disorders that occur during adolescence take various forms, ranging from mild dissatisfaction with one’s own body through various types of behavior where with the young person tries to achieve the ideal weight, to the appearance of symptoms of eating disorders – anorexia and bulimia. Sociocultural, psychological, biological and genetic factors are part of the genesis of the occurrence of anorexic and bulimic disorders. Difficulties with self-esteem, dissatisfaction with one’s own body image, cognitive distortion followed by dysfunctional thoughts contribute to the person being worried, anxious, depressed, and therefore overeating, vomiting or dieting. The quality and type of relationship with parents plays an important role in the psychological development of the young person and their psychological functioning. Parents reward their children for the desired forms of behavior, giving them love and attention. For every parent, parenting is a pleasure and children grow up without traumatic experiences, with confidence, readiness for active participation and overcoming stressful and frustrating situations. On the other hand, parents who do not consider the needs and rights of the young person, build a cold emotional relationship with the adolescent, contribute to the adolescent experiencing himself or herself as a worthless, empty and powerless person, they are a risk factor for the development of an eating disorder, therefore it is necessary to implement adequate preventive programs through which the person in the adolescence period will develop a healthy attitude towards food and care for their health.
Conflict of Interest Statement
There is no conflict of interest.
Acknowledgement
The authors would like to express their gratitude to all participants who participated in this research.
References
- Marcinko D. Eating Disorders-Diagnosis, Clinical Features, Occurrence, Psychodynamics and Therapeutic Characteristics. In: Marcinko D, Eating Disorders – from Understanding to Treatment. Zagreb: Medical Publishing; 2013.
- Krleza A. Anorexia Nervosa: Etiology, Common Comorbid Disorders and Therapy. Psyche: Journal of Psychology Students.2020; 3(1): 7-14. https://hrcak.srce.hr/266931. Accessed June 15, 2023.
- Ambrosi-Randic N. Development of Eating Disorders. Jastrebarsko: Naklada Slap; 2004.
- Batista M. Psychological Adaptation and Sociocultural Attitudes in Adolescents with Anorexia Nervosa. University of Zagreb: Faculty of Medicine; 2019.dBack EA. Effects of parental relations and upbringing in troubled adolescent eating behaviors. Eating Disorders. 2011; 19:1-22.
- Furham A, Badnin N, Sneade I. Body image dissatisfaction: Gender differences in eating attitudes, self-esteem, and reasons for exercise. Journal of Psychology: Interdisciplinary and Applied. 2012; 136(6): 581-596. doi: 10.1080/00223980209604820.
- Smolak L. Body image developmental children. In: Cash TF, Pruzinsky T, eds. Body image: A handbook of theory, research and clinical practice. New York: The Guilford Press; 2002:65-74.
- Sander J, Moessner M, Bauer S. Depression, anxiety and eating disorder – related impairment: Moderators in female adolescents and young adults. International Journal of Environmental Research and Public Health. 2021; 18: 2775. https://doi.org/10.3390/ijeroh18052779.
- Levine MP, Smolak L. Body image developmental children. In: Cash TF, Pruzinsky T, eds. Body image: A handbook of theory, research and clinical practice. New York: The Guilford Press; 2002:74-83.
- Keski-Rahkonen A, Mustelin L. Epidemiology of eating disorders in Europe: prevalence, incidence, comorbidity, course, consequences, and risk factors. Current Opinion in Psychiatry. 2016; 29(6): 340-345.
- Dzielska A, Kelly C, Ojala K. Weight reduction behaviors among European adolescents – Changes from 2001/2002 to 2017/2018. Journal of Adolescent Health. 2020; 66(6): 70-80. https://www.eatingdisorderhope.com Accessed April 27, 2023.
- Wenar C. Developmental psychopathology: From infancy through adolescence. New York: McGravi-Hill; 2014.
- Rada K, Vukomanovic A, Panjkota Krbavcic I. Body Perception and the Incidence of Anorexia Nervosa in Young People in Croatia. Croatian Journal of Food Technology, Biotechnology and Nutrition. 2022; 17(1-2):34-39. https://www.researchgate.net/profile/lnes.
- Herpetz-Dahimann B. Adolescent eating disorders: update on definitions, symptomatology, epidemiology, and comorbidity. Child and Adolescent Psychiatric Clinical Research. 2015; 24(1): 177-196.
- Christian C, Perko VL, Vanzhula IA, Tregarthen JP, Forbush KT, Levinson C. Eating disorder core symptoms and symptom pathways across developmental stages: A network analysis. Journal of Abnormal Psychology. 2020; 129(2): 177-190. https://doi.org/10.1037/abn0000477.
- Qian J, Wu Y, Liu F, et al. An update on the prevalence of eating disorders in the general population: A systematic review and meta-analysis. Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity. 2022; 27(2): 415-428. https://doi.org/10.1007/s40519-021-01162-z
- Dale Grave R, Calugi S, Marchesisi G. Self-induced vomiting in eating disorders: Associated features and treatment outcome. Behavior Research and Therapy. 2009; 47: 680-684.
- Stavrou P. How does a woman experience bulimia nervosa? The link between bulimia nervosa, low self-esteem and insecure attachment: a phenomenological approach. Journal of Psychology Clinical Psychiatry. 2018; 9(5): 502-506.
- Polivy P, Gape SH. Changes in millennial adolescent mental health and health-related behaviors over 10 years: A population cohort comparison study. International Journal of Epidemiology. 2021; 48: 1650-1660. doi: 10.1093/ije/dyz006.
- Riviere J, Doulliez C. Perfectionism, rumination and gender are related to symptoms of eating disorders: A moderated mediation model. Personality and Individual Differences. 2017; 4(1): 116-168.
- Mendelson BK, McLaren L, Gauvin L, et al. The relationship of self-esteem and body esteem in women with and without eating disorders. Journal of Psychology. 2002; 133(4): 357-368.
- Palmer B. Concepts of eating disorders. In: Treasure J, Schmidt U, Furth E, eds. Handbook of eating disorders. Chichester: John Wiley and Sons; 2003:1-11.
- López-Gil JF, García-Hermoso A, Smith L, et al. Global Proportion of Disordered Eating in Children and Adolescents: A Systematic Review and Meta-Analysis. JAMA Pediatrics. 2023, 177: 363–372.
- Steinberg L, Silk JS. Parenting adolescents. In: Bornstein MH, ed. Handbook of parenting. Mahwah, New Jersey: Erbaum; 2001: 103-104.
- Ward A, Gowers S. Attachment and childhood development. In: Treasure J, Schmidt U, Furth E, eds. Chichester: John Wiley and Sons; 2003: 89-103.
- Back EA. Effects of parental relations and upbringing in troubled adolescents’ eating behaviors. Eating Disorders. 2006; 19: 1-22.
- Berk L. Development through the Lifespan. Jastrebarsko: Slap Publishing House; 2006.
- Leonidas C. Social support networks and eating disorders: An integrative review of the literature. Eating Disorders. 2014; 10: 915-927.
- Koteva-Mojsovska T. Family Upbringing and Social Behavior of Children. Skopje:Academic Press; 2021.
- Hampshire C, Mahoney B, Davis SK. Parenting Styles and Disordered Eating among Youths: A Rapid Scoping Review. Front Psychol. 2022; 12:802567.
- Suldo S, Sandberg D. Relationship between attachment styles and eating disorder symptomatology among college women. Journal of College Student Psychopathology. 2000; 15: 59-73.
- Gila A, Castro J, Toro J, et al. Subjective body image dimension in normal female population: Evolution through adolescence and early adulthood. International Journal of Psychology and Psychological Therapy. 2004; 4: 1-10.
- Mendelson BK, McLaren L, Gauvin L, et al. The relationship of self-esteem and body esteem in women with and without eating disorders. Journal of Psychology. 2002; 133(4): 357-368.
- Schaumberg K, Reilly EE, Gorrell S, et al. Conceptualizing eating disorder psychopathology using an anxiety disorders framework: evidence and implications for exposure-based clinical research. Clinical Psychology Review 2021; 83:101952. https://doi.org/10.1016/j.cpr.2020.101952
- Solmi M, Radua J, Olivola M, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry. 2021; 12(3): 134-154. https://doi.org/10.1038/s41380-021-01161-7.
- Micali N, Horton NJ, Crosby RD, et al. Eating disorder behaviors amongst adolescents: investigating classification, persistence and prospective associations with adverse outcomes using latent class models. European Child and Adolescence Psychiatry. 2017; 26(2):231–240. https://doi.org/10.1007/s00787-016-0877-7.
- Prefit AB, Candea DM, Szentagotai-Tatar A. Emotion regulation across eating pathology: A meta-analysis. Appetite. 2019; 143: 104438. doi: 10.1016/j.appet.2019.104438.
- McCarthy M. The thin ideal, depression and eating disorders in women. Behavior Research and Therapy. 2019; 28:205-215.
- Raphael FJ, Lacey JH. Socio-cultural aspects of eating disorders. Annals of Medicine. 2002; 24: 293-298.
- Pesa JA, Syre TR, Jones E. Psycho-social differences associated with body weight among female adolescents: The importance of body image. Journal of Adolescent Health. 2000; 26: 330-337.
- Bufferd SJ, Levinson CA, Olino TM, et al. Temperament and psychopathology in early childhood predict body dissatisfaction and eating disorder symptoms in adolescence. Behavior Research Therapy. 2022; 151:104039. https://doi.org/10.1016/j.brat.2022.104039
- Vidovic V. Feeding and Eating Disorders in Early Infancy, Childhood and Adolescence. Medicus. 2009; 18(2): 185-191.
- Penate W, Gonzales-Loyola M, Oyanadel C. The predictive role of affectivity, self-esteem and social support in depression and anxiety in children and adolescents. International Journal of Environmental Research Public Health. 2020; 17: 6948. doi: 10.3390/ijerph17196984.
- Ambrosi-Randic N, Pokrajac-Bulian A. Psychometric properties of the eating attitude test. Eating Weight Disorders. 2005; 76-82.
- Grolnick WS, Ryan RM, Deci EL. The inner resources for school performance: Motivational mediators of children’s perceptions of their parents. Journal of Education Psychology. 1991; 83: 508-517.
- Cooper PJ, Taylor MJ, Cooper M, Fairburn CG. The development and validation of the Body Shape Questionnaire. International Journal of Eating Disorders. 1987; 6: 485-494.
- LeBlanck JC, Alnudevar A, Brooks SJ, et al. Screening for adolescent depression: Comparison of the Kutcher Adolescent Depression Scale with the Beck Depression Inventory. Journal of Child and Adolescent Psychopharmacology. 2002; 1292): 113-126.
- Spielberger CD, Gorsuch R, Lushene R. Manual for the State-Trait Anxiety Inventory. Consulting Psychologist Press, Palo Alto, CA, USA; 1970.
- Potterton R, Richards K, Allen K, et al. Eating disorders during emerging Adulthood: a systematic scoping review. Front Psychol. 2020; 10:3062.
- Couturier J, Isserlin L, Norris M, et al. Canadian practice guidelines for the treatment of children and adolescents with eating disorders. Journal of Eating Disorder. 2020; 8(1):4.
- Klump KL, Culbert KM, Slane JD, et al. The effects of puberty on genetic risk for disordered eating: Evidence for a sex difference. Psychological Medicine. 2012; 56:124-135. doi: 10.1017/S0033291711001541.
- Garcia SC, Mikhail ME, Keel PK, et al. Increased rates of eating disorders and their symptoms in women with major depressive disorder and anxiety disorders. International Journal of Eating Disorder. 2020; 53: 1844–1854.
- Smith KE, Mason TB, Leonard RC, et al. Affective predictors of the severity and change in eating psychopathology in residential eating disorder treatment: The role of social anxiety. Eating Disorder. 2018; 26: 66–78. doi: 10.1002/eat.23366.
- Keyes KM, Gary D, O’Malley PM, et al. Recent increases in depressive symptoms among US adolescents: Trends from 1991 to 2018. Social Psychiatry and Psychiatric Epidemiology. 2019; 54: 987–996.
- Prefit AB, Candea DM, Szentagotai-Tatar A. Emotion regulation across eating pathology: A meta-analysis. Appetite. 2019; 143: 104438.
- Polanczyk GV, Salum GA, Sugaya LS, et al. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychological Psychiatry, 2015; 56: 345–365.
- Criscuolo M, Laghi F, Mazzoni S, et al. How do families of adolescents with anorexia nervosa coordinate parenting? Journal of Child Family Studies. 2020; 29: 2542–2551.