






Recovery from Electromagnetic Intolerance: Key Precursors
Precursors Need to be Considered to Promote Recovery from Idiopathic Environmental Intolerance–Attributed to Electromagnetic Fields
Magda Havas1
- Trent School of the Environment, Trent University, 1600 W Bank Dr, Peterborough, ON K9L 0G2, Canada
OPEN ACCESS
PUBLISHED 31 January 2025
CITATION: Havas, M., 2025. Precursors Need to be Considered to Promote Recovery from Idiopathic Environmental Intolerance–Attributed to Electromagnetic Fields. Medical Research Archives, [online] 13(1). https://doi.org/10.18103/mra.v13i1.6253
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i1.6253
ISSN 2375-1924
ABSTRACT
Exposure to radiofrequency radiation has been increasing for decades and a growing population is suffering from what has been called electrohypersensitivity. The concept of electrohypersensitivity is problematic as it implies that only those who are “hypersensitive” respond to electromagnetic fields, which is not the case. The World Health Organization recommended replacing this term with idiopathic environmental intolerance with attribution to electromagnetic fields. However, without knowing the cause of this illness medical help is reduced to alleviating symptoms and this is seldom adequate for full recovery. The aim of this report is to help people recover from electrohypersensitivity by understanding what precursors may be contributing to their symptoms. In this paper, three terms are differentiated: trigger, causal agent, and precursor–with the understanding that electromagnetic fields trigger symptoms and, while it is often difficult to identify causal agents, precursors may predispose individuals to an increased vulnerability to environmental stressors including electromagnetic pollution. Five precursor categories are identified: physical trauma to central nervous system; exposure to toxic chemicals; biological infections; acute or chronic exposure to either ionizing or non-ionizing radiation; and an impaired immune system. Recovering from electromagnetic pollution requires deactivating the trigger(s) and the precursors suggest ways this may be accomplished. The acronym R2ID3 may help physicians decide which treatments are likely to be most effective for their patients. The letters signify the following: (R1) reduce exposure to pollutants; (R2) rebalance limbic system; (I) enhance immune system; (D1) detoxify body; (D2) test DNA for patient-specific detoxification protocol; and (D3) employ dental procedures to remove infections and metals. Helping patients recover and minimizing exposure to electromagnetic pollution is of utmost importance from a public health perspective.
Keywords:
electromagnetic fields; electromagnetic radiation; non-ionizing radiation; electrohypersensitivity; idiopathic environmental intolerance; electromagnetic illness; World Health Organization; electromagnetic radiation syndrome
INTRODUCTION
ELECTROHYPERSENSITIVITY
In 2004, the World Health Organization (WHO) held a special 3-day meeting in Prague to discuss the concept of Electrohypersensitivity (EHS). This meeting, unlike most WHO meetings, was open to anyone who wished to contribute and/or attend and, consequently, individuals purporting to be intolerant of electromagnetic exposure were present.
According to the WHO, EHS is considered, … a phenomenon where individuals experience adverse health effects while using or being in the vicinity of devices emanating electric, magnetic, or electromagnetic fields (EMFs). They also stated that … EHS is a real and sometimes a disabling problem for the affected persons … Their exposures are generally several orders of magnitude under the limits in internationally accepted standards … Some individuals are so severely affected that they cease work and change their entire lifestyle, while others report mild symptoms and react by avoiding the fields as best they can.
In their attempt to include EHS people, the WHO clearly demonstrated naiveté about the topic because they did not ensure an electromagnetically clean environment for their meeting and they did not discourage the use of cell phones that trigger symptoms of those attending.
According to the WHO, the most common symptoms attributed to EHS include dermatological symptoms (redness, tingling, and burning sensations) as well as neurasthenic and vegetative symptoms (fatigue, tiredness, concentration difficulties, dizziness, nausea, heart palpitation, and digestive disturbances). WHO went on to state that, since these symptoms are not part of a recognized syndrome and since there is no known cause, the term idiopathic environmental intolerance with attribution to EMF (IEI-EMF) be used instead of electrohypersensitivity (EHS). IEI is described as an acquired disorder with multiple recurrent symptoms, that is associated with diverse environmental factors tolerated by the majority of people, and that cannot be explained by any known medical, psychiatric or psychological disorder.
WHAT’S IN A NAME?
This concept of “an intolerance to electromagnetic fields” has been referred to by various names. From the term neurasthenia at the turn of the last century to radio wave or microwave illness among radar operators during the Second World War to screen dermatitis for those working in front of computer screens in the 1980s. Then various combinations of electromagnetic sensitivity and electrohypersensitivity were used. More recently, rapid aging syndrome (RAS); electromagnetic interference/illness/injury (EMI) as well as electromagnetic radiation syndrome (EMR-S) have been introduced. This later term is an attempt to have the scientific community use just one term to describe this illness.
The term “electrohypersensitivity” has a somewhat negative connotation. It places unnecessary pressure on those who are being harmed by this pollutant, as though they are somehow at fault for reacting. Children are particularly vulnerable to lead and mercury but we don’t refer to them as lead-sensitive or mercury-intolerant. Electromagnetic illness (EMI) may be a more appropriate term implying that electromagnetic fields are triggering the symptoms and, just like with other pollutants, there are a range of reactions.
WHO RECOMMENDATIONS FOR MEDICAL DOCTORS
In 2004, the WHO recommendations to diagnose IEI-EMF (or EHS) included a three-step process and consisted of:
- a medical evaluation (to identify specific conditions that may account for the symptoms);
- an assessment of the home and workplace (for factors that may contribute to symptoms including air pollution, noise, poor lighting and ergonomic factors, stress reduction and assessment to ensure that EMF exposures were within existing guidelines); and
- a psychological evaluation.
An unusual general recommendation for physicians was that “in case of persisting symptoms, [the aim should be] focusing on reducing disability rather than searching for a specific causal factor.” How do you reduce disability without knowing the cause? Furthermore, measuring electromagnetic fields in the home was discouraged since there was no known relationship between electric or magnetic fields and symptoms unless the EMF fields exceed recommended exposure limits. The underlying and flawed assumption was that, if the guidelines are not exceeded, there are no adverse effects. Numerous government health authorities are still parroting this false narrative.
Some of the WHO recommendations to national authorities were appropriate but were largely disregarded and some were ill advised. For example, WHO stated that the plight of the 2-3% of the population suffering from EHS in 2004 should not be ignored, yet most countries still do not recognize this illness 20-years later. Furthermore, WHO stated that authorities should not recommend commercial products to shield EMFs and, since there was no “causal link”, they did not have to lower internationally accepted limits for EMF exposures. This does not make sense from an environmental toxicology perspective since removing the triggering agent is often the first step that needs to be taken for recovery to take place. Replacing the term EHS with IEI-EMF appeared to be politically motivated since, if the “cause” is unknown, there is no need to lower guidelines, which turned out to be one of WHO’s recommendations.
Twenty years later, much has changed regarding exposure with the rollout of WiFi, smart meters, smart appliances, wireless wearables and small cell antennas for 5G telecommunications. However, little has changed regarding the WHO recommendations despite major advances in our scientific understanding of some of the mechanisms involved. WHO still does not recognize non-thermal effects and still promotes the term idiopathic environmental intolerance attributed to electromagnetic fields. Never in the history of this planet have levels of artificial electromagnetic fields been so high. This pollutant is now virtually ubiquitous and large populations are exposed to levels of artificial radiation that are trillions of times above background levels.
INTERPRETATION OF THE WHO REPORT ON IEI-EMF
Since 2004, I have conducted several provocation and elimination studies and have worked with many people who have EHS. What I learned is that various events, exposures, conditions can contribute to EHS and these are discussed below. Before I go further, we need to differentiate between three terms: triggers, precursors and causal factors.
In my initial assessment of the WHO’s recommendation to use the term IEI-EMF I realized that I was confusing two terms: trigger and causal agent. Exposure to EMFs in their various forms can trigger the symptoms listed by the WHO and many more. While cause-effect relationships are difficult to determine, precursors (i.e., events that precede sensitivity) are more easily ascertained and may result in or contribute to EHS symptoms. These precursors need to be considered when treating someone with EHS as treatment would depend on the precursor that may also be the root cause of the reaction. The precursors fall into five categories discussed below and a person may have one or more precursors.
Five Precursors for EHS
Why are some people unable to tolerate EMF exposure? Why do they respond to levels well below internationally accepted guidelines? Why do genetically-related individuals living in the same environment differ in their sensitivity to electromagnetic pollution? These questions can be answered by knowing what previous exposures individuals have had to a variety of stressors and their health status. The common precursors experienced by those with EHS fall into one or more of the following five categories:
- Physical trauma to central nervous system;
- Chemical trauma in the form of exposure to environmental toxins;
- Biological trauma in the form of exposure to various biological agents;
- Electromagnetic trauma in the form of either high levels of acute exposure or low levels of chronic exposure to various forms of electromagnetic frequencies, both ionizing and non-ionizing;
- State of various systems in the body especially the immune and nervous systems.
Electromagnetic frequencies are known to affect the nervous system. As mentioned earlier, telephone switchboard operators were among the first occupational groups to be adversely affected by exposure to electromagnetic fields and their diagnosis was “neurasthenia” or a weakening of the nervous system. The symptoms, which were attributed largely to recurring electrical shock, were similar to those associated with severe EHS (headaches, pain, fainting, extreme nervous exhaustion).
One might expect that exposure to other neurotoxins or pre-sensitization of the nervous system could exacerbate neurological symptoms and may intensify sensitivity to electromagnetic exposure. This could include some combination of physical trauma; chemical exposure; biological toxins, especially Lyme and mold; acute or chronic electromagnetic exposure or an impaired immune function.
PRECURSOR #1: PHYSICAL TRAUMA TO CENTRAL NERVOUS SYSTEM (CNS)
Injury to the CNS that includes both traumatic brain injury (TBI) and spinal cord injury (SCI) is a serious global public health burden and a major cause of disability and mortality. It can be caused by automobile accidents; sports injuries; a fall; a stroke; and surgical injury. Symptoms can include persistent or sudden onset of a headache; a headache that changes or is different; loss of feeling or tingling in parts of the body; weakness or loss of muscle strength; loss of sight or double vision; memory loss; impaired mental ability; mood disorders; and lack of coordination. Concussions and whiplash are two of the most common forms of TBI and the incidence varies considerably across the globe.
Traumatic brain injury, as described by Ouellet et al., “… can affect multiple domains of functioning, including physical health, psychological health, cognition, and socio-occupational life. Sleep–wake disturbances are among the most common consequences of TBI. They can be present even years postinjury, and they interact with other conditions linked to the brain injury such as cognitive deficits, psychopathology, pain, and chronic fatigue. Sleep–wake disturbances thus affect recovery, the rehabilitation process, and the person’s capacity to return to premorbid functioning.”
Many of the TBI symptoms and some of the SCI overlap with EHS. There are several ways of interpreting these results. It’s possible that damage to the nervous system sensitizes individuals to electromagnetic frequencies and thus promotes or causes intolerance. Another possibility is that EMFs are exacerbating the symptoms of CNS trauma and aggravating the original symptoms. These two interpretations appear minor but are profoundly different. In the first case, the focus is on individual sensitivity and in the second case, the diagnosis would remain as SCI/TBI exacerbated by an environmental trigger (electromagnetic exposure), without any mention of sensitivity. The medical/scientific community needs to examine these interactions to determine the most appropriate explanation of what is happening.
In some cases, someone suffering from CNS damage, who is triggered by electromagnetic exposure, may recover by minimizing their exposure, while in other cases the original CNS trauma would also need to be treated to enable full recovery.
PRECURSOR #2: CHEMICAL EXPOSURE
Chemical pollutants can also be neurotoxins. Mercury, aluminum, lead, as well as some pesticides and medications can adversely affect the nervous system. Exposure to mercury can occur via several pathways including dental amalgam; food; medication; occupational exposure and environmental pollution, like coal burning for example. Organic mercury is stored in fatty tissue and is considered relatively inert until body fat is metabolized during weight loss or illness. When someone is exposed to microwave radiation from WiFi, cell phones or magnetic resonance imaging (MRI), mercury in the body is mobilized and higher levels have been measured in saliva or urine. Consequently, someone using their cell phone may be mobilizing mercury from their fillings and increasing metabolically available levels in the body.
Metabolically available mercury is likely to dampen neural responses especially cognitive functions. Since both mercury and electromagnetic radiation are neurotoxin, they may be interacting additively or synergistically. Whether electromagnetic exposure also mobilizes other internal toxins is not known. Once again, we can look at this as the electromagnetic pollutant exacerbating the symptoms of chemical toxicity. Safe ways to detoxify the body may benefit those who are suffering from EHS and, indeed, this is part of the protocol used by many doctors.
PRECURSOR #3: BIOLOGICAL TOXINS
Biological trauma can be caused by exposure to bacteria, viruses, molds and other parasites by way of ingestion, inhalation or direct skin contact. Many individuals who have EHS symptoms have had previous mold exposure, especially exposure to black mold (Stachybotrys) that is a potent neurotoxin or have been diagnosed with Lyme disease, which is caused by a Borrelia bacteria that can be transmitted to humans by infected ticks or mosquitoes. Several symptoms overlap with EHS including headaches, chronic fatigue, joint stiffness, muscle pain, depression, nervous disorders, heart palpitations, skin rashes, and blurred vision. Once again, the reaction to EMF/EMR following an infection may be due to an increased sensitization cause by the pathogen resulting in greater sensitivity to EMFs or it may be due to the EMFs aggravating the original symptoms cause by the biological agent.
According to Dr. Dietrich Klinghardt (personal communication), EHS symptoms can be significantly reduced by treating the pathogenic agent. His reasoning is that the microbes are reacting to the electromagnetic exposure, releasing toxins into the body and thus making people sick. From his clinical experience, if no permanent damage has occurred, removing the microbes often eliminates the EHS symptoms.
PRECURSOR #4: ELECTROMAGNETIC TRAUMA
High levels of acute exposure or low levels of chronic exposure to various electromagnetic frequencies, including ionizing radiation, assaults the energy systems of the body. Exposure to electromagnetic pollution can cause a multitude of reactions within the body, the most prevalent seems to be oxidative stress. Oxidative stress can damage cells and tissues within the body resulting in various symptoms depending on the location and degree of damage. Common symptoms include fatigue; memory loss or brain fog; muscle and joint pain; headaches; sensitivity to noise and increased susceptibility to infection. Oxidative stress has been associated with inflammation and can lead to chronic health conditions like diabetes or cancer. Oxidative stress causes cells and organs in the body to age more rapidly, hence the term rapid aging syndrome. Diabetes as well as thyroid and pancreatic cancers are increasing as are cancers among youth. Could the rapid increase in exposure to electromagnetic pollution that causes oxidative stress be involved in the increase in these chronic and debilitating health conditions?
Oxidative stress may be caused by acute exposure to high levels of radiation, which is more common in occupational settings or with some medical treatments like x-rays or MRI. It can also be caused by chronic exposure to low levels of radiation, which is becoming increasingly common within homes due to the myriad of wireless appliances (WiFi, cordless phones, smart meters, smart appliances) combined with nearby electrical power lines and cell phone base stations mounted on or near buildings. If no other precursors exist, this may be considered an example of EHS attributed to electromagnetic exposure. Provocation and elimination studies confirm this.
PRECURSOR #5: STATE OF THE IMMUNE SYSTEM
Disturbed immune function may relate to age (young children and the elderly), previous illnesses (some of the items mentioned above); medication; and/or excessive stress. When the immune system is weakened opportunistic infections are more frequent, more severe, and last longer. There is also evidence that exposure to electromagnetic fields can amplify immune system dysfunction, including immunosuppression, autoimmunity and hyperinflammation. Oxidative stress, inflammation, and immune system disruption are common to many chronic diseases including autoimmune disease like type 1 diabetes and multiple sclerosis.
One of the early studies in the 1980s showing immune system dysregulation was associated with exposure to video display terminals. The symptoms included itchiness, pain, redness, heat sensation, papules, skin pustules and changes in mast cells. Some of the scientific findings include over-reaction of the immune system; morphological alternations of immune cells; profound increases in mast cells in the upper skin layers; increased degranulation of mast cells and larger mast cells in hypersensitive individuals; biological markers for inflammation; decreased count of natural killer (NK) cells; decreased count of T-lymphocytes; suppressed or impaired immune function and inflammatory response that can ultimately result in cellular, tissue and organ damage.
How to Promote Recovery using R2ID3
Those who develop debilitating symptoms when exposed to electromagnetic pollution find that their life choices and activities are limited. If they have a “safe home” that is electromagnetically clean, they may find themselves confined to their home since exposure in urban centres is often too high for them to tolerate and this includes schools, workplaces, public transit, stores, restaurants, coffee shops, theatres and even medical clinics and hospitals. Those who cannot escape electromagnetic exposure in their own home, from nearby cell towers or neighbours’ WiFi, may drive to a secluded area and sleep in their cars. This is no way to live and may be life-endangering during inclement winter weather.
Consequently, rapid recovery is the aim for highly sensitive people to live a fully functional life. Individuals with EHS may sometimes develop intolerance following a weakened immune system, an accident or exposure to toxicants in the environment (chemical, biological, electromagnetic). Then, the introduction of a novel source of electromagnetic pollution like a smart meter or a nearby small cell antenna or a neighbour’s WiFi may be enough to trigger symptoms of EHS.
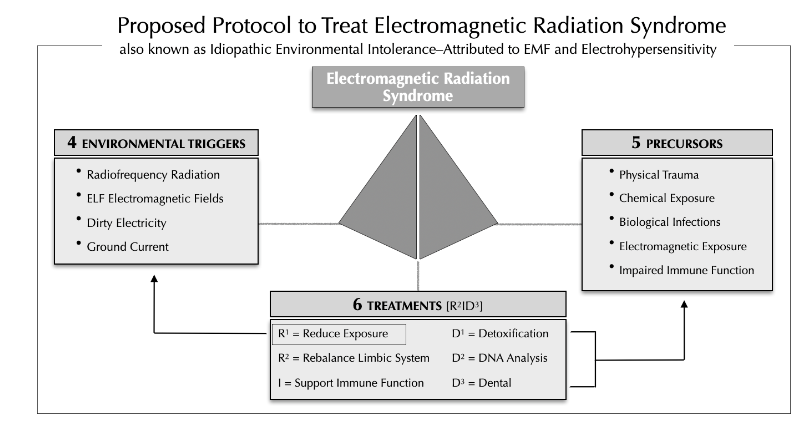
Sometimes treating the original injury or insult may lessen the symptoms and aid in recovery. For example, someone with a concussion would receive very different treatment than someone with elevated levels of mercury. The general recommendations presented here require the advice of specialists to identify the specific treatments that may benefit each patient. Sometimes more than one precursor needs to be considered and treated for full recovery to take place. These treatments, possible precursors and types of electromagnetic triggers are presented in Figure 1.
R1: REDUCE EXPOSURE TO ENVIRONMENTAL STRESSOR
The American Academy for Environmental Medicine recognizes that patients are being adversely impacted by electromagnetic frequency (EMF) and radiofrequency (RF) fields and are becoming more electromagnetically sensitive. They recommend avoiding exposure to EMF/EMR. This recommendation is in stark contrast to that provided by the WHO.
According to the WHO, “ … it is clear that there is no support or need for an intense electrical sanitation of the home and workplaces of EHS patients. A lowering of exposure levels of EMF in general could be proposed as a precautionary approach, especially for afflicted persons, but this was not seen as a remedy for a person’s symptoms. As for treatment, since EHS has symptoms similar to other environmental illnesses, clinicians would normally adopt largely psychologically based managements strategies.”
With no evidence the WHO implies that electromagnetic illness is a psychological disorder.
I classify non-ionizing electromagnetic exposure into four categories based on source, frequencies and the mode of transmission. Two of these categories are well studied, extremely low frequency electric and magnetic fields (ELF-EMF) as well as radiofrequency radiation (RFR) especially in the microwave band (300 MHz to 6 GHz). Two other categories receive much less attention but can be highly stressful and this includes dirty electricity and ground current. Dirty electricity, also referred to as high frequency voltage transients (HFVT), consists of intermediate frequencies in the kHz range. Ground current is a combination of power frequencies (50/60 Hz) and kHz frequencies as the electricity flowing along wires is the same as that flowing along the surface of the ground. The ground may also be a source of RFR in the form of reflection or reradiation from a nearby source.
Monitoring of electromagnetic exposure in all of these categories is necessary as individuals react to different frequencies. One of the problems with many provocation studies is that background levels of these four types of electromagnetic pollutants were not monitored and some of these environments could very well have been electromagnetically contaminated, which would invalidate the results.
While the WHO recommends designing double-blind, placebo-controlled provocation studies, eliminating the electromagnetic frequencies from the environment can also provide useful information. In one of our studies, we provide evidence that blood sugar among some type 1 and type 2 diabetics may be altered depending on whether they are exposed to electromagnetic fields.
In this research we refer to four case studies: a 12-year-old male recently diagnosed with type 1 diabetes; an 80-year-old female with lifetime type 1 diabetes; a 51-year-old male and a 57-year-old female both with type 2 diabetes, neither of whom were on medication for their diabetes. By reducing the dirty electricity in the home environment, both type 1 diabetics were able to significantly reduce their daily insulin injections. The female with type 2 diabetes used exercise to control her blood sugar. After a 20-minute walk her blood sugar would return to acceptable levels (7 mmol/L). However, when she exercised on a treadmill that generates dirty electricity from a variable speed transformer, her blood sugar would increase consistently to 11.6 mmol/L. The male who was recently diagnosed with type 2 diabetes, monitored his fasting plasma glucose levels as soon as he woke up each morning. The glucose content ranged from 4.2 to 9.5 mmol/L and was linearly related to the amount of dirty electricity in his home.
Reducing exposure to electromagnetic pollution is the first “R” in the acronym R2ID3. However, reducing exposure may not be enough and then additional steps need to be taken for recovery to occur.
R2: REBALANCE LIMBIC SYSTEM
R2 refers to rebalancing the limbic system. Someone living with severe EHS may experience emotional challenges, especially if their diagnosis is not accepted by family, friends, and/or co-workers. Everyday living for someone with EHS can be challenging and not being believed causes additional stress. If the situation is sufficiently severe and the patient is unable to work, or if they require in-home help as they can no longer take care of themselves or perform their normal daily activities, then additional financial challenges can add to the mounting stress. Prolonged emotional stress can be harmful to the body. Rebalancing the limbic system is vital for recovery.
Dynamic Neural Retraining System (DNRS) developed by Annie Hopper, is drug-free, self-direct program based on the principles of neuroplasticity to help reverse limbic system impairment and to regulate a maladapted stress response. In one study with 102 participants, DNRS was shown to have beneficial effects on physical function, mental health, social function, bodily pain, general health, emotional health, vitality and physical health within 3 months of following this program. Significant improvements were reported with benefits lasting for at least one year. Some of the people I’ve worked with have enrolled in this program and report that their symptoms are much reduced.
Another technique used to treat anxiety disorders, panic attacks, post-traumatic stress disorder (PTSD) and trauma is Eye Movement Desensitization and Reprocessing (EMDR). This technique, developed by psychologist Dr. Francine Shapiro, is a guided treatment that involves bilateral stimulation of the brain normally with directed eye movements, while the patient focuses on the traumatic memory. It involves temporarily slowing down the over-stimulated amygdala and helps to synchronize brain activity and has been used successfully to treat emotional disorders in more than 130 countries worldwide.
One of the newest techniques for addressing psychological trauma, designed by Dr. Daniel Asis an Argentinian physician specializing in pain management and anesthesiology, is Auricular Chromotherapy (ACT) which involves shining a yellow light on ear acupuncture points to calm and rebalance the limbic system. It has been used to successfully treat psychologic trauma, phobia and panic attacks. While the mechanism isn’t fully understood, there is evidence indicating that electrical stimulation of the earlobe activates different parts of the brain including the solitary nucleus: parabrachial nucleus; nucleus accumbens; hypothalamus; thalamus; and amygdala. This activation can help erase stressful images and disturbing thoughts. In one study with 160 patients, 93% of the patients experienced a positive outcome after just one ACT treatment.
Photobiomodulation and chromotherapy are likely to be used more frequently in western medicine once the medical community recognizes the safety and efficacy of this novel way to treat disorders and imbalances.
In 2004, the WHO recommended Cognitive Behavioral Therapy (CBT) and provided results from three studies, two of which showed improvement in symptoms following the therapy. CBT has been shown to reduce cardiovascular and neuroendocrine reactions to stress. While this therapy is still viable, it has been extended to include other techniques, some of which are mentioned above.
The concept here is NOT that the person is responding psychologically to the stressor but rather that, in addition to a physiological response, there is also a psychological stress response that can exacerbate the physical and emotional symptoms. Calming the mind allows the body to heal.
I: ENHANCE IMMUNE RESPONSE
The “I” refers to the immune system, which consists of a complex network of hormones, cells, tissues and organs that work together to defend the body against harmful pathogens. The immune system may be overactive, as in the case of asthma; underactive resulting in frequent infections and/or accelerated cancer growth; or self-destructive as in the case of autoimmune disorders like type 1 diabetes, multiple sclerosis, and rheumatoid arthritis. Immune system imbalances can happen among the very young or the elderly. The imbalance can be due to some of the precursor stressors mentioned above or to recent illness and/or to certain medications.
Exposure to low levels of radiofrequency/microwave radiation may impair the immune system with short-term exposure causing temporary stimulation and prolonged exposure causing inhibition of immune function. Furthermore, symptoms of both multiple sclerosis and diabetes (autoimmune responses) can be reduced in an electromagnetically clean environment, which would suggest that electromagnetic radiation may be exacerbating these symptoms. Although the emphasis here is on the immune system, all systems in the body work in tandem and disruption of one system, can result in compensatory actions via the other systems.
Support for the immune system requires a nutritious diet, regular exercise, sufficient sleep (which is difficult for those who suffer from EHS), stress management, good hygiene and minimizing exposure to environmental toxins including electromagnetic pollution. A compromised immune system can also result in multiple chemical sensitivity (MCS), which often accompanies EHS.
D1-3: DETOXIFICATION, DNA TESTING AND DENTAL ASPECTS
The three “Ds” are for detoxification, DNA testing and dental aspects.
D1 stands for “detoxification”. This involves removal of chemical and biological toxins from the body. Various organs (lungs, liver, skin, kidney, colon and lymph nodes) and enzymes (cytochrome P-450, glutathione S-transferases, UDP-glucurono-syltransferases, sulfotransferases and N-Acetyltransferases) promote detoxification. Saunas, chelating agents, antioxidants and nutritional supplements that promote liver health will stimulate detoxification. However, not everyone is able to detoxify at the same rate and this brings up D2, which is DNA testing.
DNA testing can provide useful evidence on how well the body can detoxify. This is critical as the rate of detoxification should be neither too rapid (to prevent a Herxheimer reaction) nor too slow and this can be determined by the status of detoxification enzymes (mentioned above) that are provided by DNA testing. By understanding an individual’s genetic variations in relevant genes, DNA testing can provide insights into their unique detoxification capabilities and potential vulnerabilities. This information can aid healthcare professionals regarding the mode and rate of detoxification and of potential risks for adverse reactions to certain toxins.
The final “D” is for dental. The mouth can be the source of multiple illnesses especially in the presence of mercury fillings, metal braces, metal posts and root-canals. Root-canals can be a source of bacterial infections; fillings are a source of mercury; and metal objects, whether they be posts or braces, can reradiate microwave radiation coming from the environment throughout the head resulting in “hot spots.” Headaches are one of the early symptoms of EHS.
Treatments for the precursor traumas may involve the skills of several different types of therapists from general practitioners, orthopedic doctors, chiropractors, physiotherapists, immunologists, neurologists, endocrinologists, naturopaths, psychologists, acupuncturists, doctors of traditional oriental medicine, dentists as well as complementary practices provided by massage therapists, energy medicine practitioners, Reiki practitioners, nutritionists, cranial/sacral therapists, yoga/meditation practices, among others.
Patients can recover if proper treatments and a safe living environment are provided. The rate of recovery will depend, to a certain degree, on the skills of the health care providers; on patient compliance; and on the amount of harm to bodily systems that need to be repaired or brought back into balance.
Medical paradigm shift: from chemicals to frequency
We have learned a great deal in the past 20 years since the WHO held their meeting on EHS in 2004. One of the lessons is the importance of knowing how various systems work within the body from an energy and frequency perspective and not just from a chemical perspective. This brings me to the final section of this paper, which provides a paradigm shift in the way we view all living creatures including humans and hence the way we assess and treat illness. This concept is based on Thomas Kuhn’s book, The Structure of Scientific Revolutions, where Kuhn argues that major advances in science occur through sudden and destabilizing changes (revolutionary rather than evolutionary) that are initially met with derision and are often ignored by the scientific/medical community, sometimes for decades. Kuhn refers to this as a paradigm shift and defines it as “a fundamental change in an individual’s or society’s view of how things work in the world.”
Schopenhauer’s quote seems particularly relevant here. All truth passes through three stages. First, it is ridiculed. Second, it is violently opposed. Third, it is accepted as being self-evident. Many examples exist. One of the most famous is Copernicus’ view of a heliocentric rather than a geocentric solar system. A medical example is Ignaz Semmelweis’ germ theory and the need for physicians to wash their hands prior to helping women in labor. The concept that organisms too small to be seen can cause death was ridiculed.
A visual example of a paradigm shift is shown in Figure 2. Is this a vase or two faces? The answer is both as it depends on the way you look at the object. There is no right or wrong answer.

In 2004, most healing relied on the chemical model. Alternative methods were not as readily available as they are today. Major advances have been made in pulsed electromagnetic field therapy and light therapy as well as ways to assess the body using electromagnetic markers and biophotons. The paradigm shift I’m referring to is the view that the human body is a “bag of chemicals consisting mostly of water” and instead seeing the body as a “being of energy and light” or consisting of electromagnetic frequencies. This concept was first described by Liboff in his paper, “Toward an electromagnetic paradigm for biology and medicine.”
Indeed, we can view various systems within the body and examine them from different perspectives. For example, the skeletal system can be examined based on physical aspects (bone density, alignment, morphology); chemical composition (calcium, phosphorus, trace minerals); or energy properties (piezoelectricity, resistance, impedance). The same reasoning can be applied to other systems in the body.
In addition to basing diagnoses on blood or urine chemistry, electromagnetic assessment tools can be used and, indeed, many are already employed by physicians like x-rays, thermography, MRI (radiofrequency and direct current magnetic field), heart rate variability, brain wave activity and there are promising new developments in biophoton research.
Furthermore, electromagnetic tools to treat illness are increasingly being used in western medical practice. This would include blue light/UV radiation for treating neonatal jaundice; visible light for seasonal affective disorder (SAD); infrared sauna for infections and detoxification; pulsed electromagnetic fields and light therapy for improving circulation, reducing inflammation, alleviating pain and promoting healing of non-union bone fractures in humans and animals alike; and transcranial magnetic stimulation (TMS) to temporarily relieve symptoms of depression.
A few years ago, at a medical meeting, an elderly doctor said that he asks three questions of his patients.
- Does the body have all the essential nutrients it requires? [vitamin C, amino acid, etc.]
- Is the body exposed to toxins that need to be removed? [mercury, lead, DDT, asbestos]
- Are their cells communicating with each other? [neurological & hormonal]
This last question took me off guard but is essential for optimal functioning of all types of systems including socio-economic ones. These three questions form the chemical model used in current western medicine. However, the human body consists of 50 trillion cells and their need to communicate instantaneously cannot be done by chemical messengers alone. There needs to be another system also in operation and Ross Adey identified that as electromagnetic energy when he stated that, cells are “whispering to each other” electromagnetically.
Fritz Popp elaborated on this concept and brought quantum coherence into the realm of medicine. “We know today that man, essentially, is a being of light. And the modern science of photobiology … is presently proving this. In terms of healing, the implications are immense. We now know, for example, that quanta of light can initiate, or arrest, cascade-like reactions in the cells, and that genetic cellular damage can be virtually repaired, within hours, by faint beams of light. We are still on the threshold of fully understanding the complex relationship between light and life, but we can now say emphatically, that the function of our entire metabolism is dependent on light.”
The concept of biophotons as neural communication signals is gaining popularity and is likely to advance our understanding of biological systems and enhance our ability to diagnose and cure disorders that have so far eluded us.
As research on the biological effects of exogenous (external) electromagnetic frequencies progressed, it became increasingly clear that these exogenous frequencies can interfere with endogenous (internal) electromagnetic activities within the body and these small disruptions could have serious consequences.
What if we used the same chemical model mentioned above but converted it into an electromagnetic frequency model and asked the following three questions:
- Does the body have all the essential frequencies it requires? [sunlight, UV radiation, Schumann Resonance, pulsed electromagnetic fields, light therapy, chromotherapy];
- Is the body exposed to toxic frequencies? [extremely low frequency electromagnetic fields, radiofrequency radiation, microwaves, dirty electricity, ground current];
- Are the cells in the body communicating with each other electromagnetically? [electromagnetic fields, biophotons].
The essential frequencies are those coming from the natural environment. They include sunlight that controls photosynthesis, circadian rhythm, reproductive cycles in various species, emergence of leaves, germination of seeds, navigation; Schuman Resonance that has various regulatory properties; and the earth’s geomagnetic field that plays a role in orientation, navigation and in ion cyclotron resonance as described by Liboff. Liboff demonstrates that direct current (DC) magnetic fields can interact in a resonant manner with endogenous alternating current (AC) electric fields in biological systems. Consequently, subtle changes in biological systems can be brought about by altering the DC magnetic field.
Clearly any system, and the body consists of multiple systems, needs to be communicating effectively with both the internal and the external environment to maintain homeostasis.
Normally we look for biochemical markers for some illness, perhaps we should consider electromagnetic markers like heart rate variability (HRV), brain wave activity, skin conductance, thermal regulation, meridians and acupuncture points and chakras instead of endocrine glands. This concept is not that novel as we already use EMFs to diagnose (CT scans, MRI, x-rays, heart rate, temperature etc.) and treat (UV radiation, bright light, infrared saunas) various illnesses (neonatal jaundice, seasonal affective disorder, endogenous toxicants).
Furthermore, the concept of “death” or the absence of a “life force” is based on the absence of a heartbeat (no electromagnetic frequency); brain death is based on the absence of brain wave activity; and cell death occurs when the electrical potential across the cell membrane drops below a critical level. Even our concept of life is governed by the absence of electromagnetic frequencies rather than chemical changes in the body.
Conclusions
Idiopathic environmental intolerance attributed to electromagnetic fields (IEI-EMF) is the label recommended in 2004 by the World Health Organization (WHO) to replace electrohypersensitivity (EHS) and to explain the symptoms experienced by 2-3% of the population when they are exposed to electromagnetic fields at levels well below international guidelines. By labelling this “idiopathic” (i.e., with no known cause), the WHO circumvented the need to change guidelines or to reduce exposure. IEI-EMF is a politically expedient term that has retarded medical advances in this field by insisting that exposures do not need to be reduced. At the same time, it encouraged the scientific community to ask the question, “What is causing intolerance to electromagnetic exposure?”
While cause-effect relationships are difficult to determine especially when it comes to the complex workings of the human body, precursors to electrohypersensitivity (EHS) are more easily ascertained and are worth examination. The most common precursors to EHS include: (1) physical trauma to the central nervous system; (2) exposure to chemical toxins; (3) exposure to biological toxins; (4) acute or chronic exposure to EMFs; and (5) an impaired immune system. These precursors may be contributing to (or causing) electromagnetic sensitivity or the electromagnetic fields in the environment may be aggravating the symptoms of the earlier trauma(s). In either case, reducing exposure to the trigger seems a reasonable recommendation, since it would be the same recommendation for a chemical toxicant or a biological irritant.
If reducing exposure isn’t enough to promote full recovery, treating one or more of the precursors may be considered. The acronym R2ID3 identifies six actions that may promote recovery: (R1) reduce exposure and this includes chemical and electromagnetic pollution as well as biological irritants; (R2) rebalance limbic system; (I) support the immune system; (D1) detoxify the body from both chemical and biological toxins; (D2) test DNA for patient-specific detoxification protocol; (D3) dental work to remove infections and metals in the mouth.
Research in this field has highlighted the importance of viewing the human body from an energy/frequency perspective as it reacts to exogenous electromagnetic fields. Endogenous electromagnetic activity can be disrupted and even minor disruptions can result in serious health effects. This paradigm shift from the role chemicals play in the body to the role electromagnetic frequencies play provides novel tools for both assessment and treatment of an illness and gives physicians more options and a novel way of looking at the body.
We need to prevent radiation damage by reducing our exposure as much as possible. This could be achieved if all stationary sources of microwave radiation (smart meters, smart appliances, WiFi) were wired and if wireless was limited primarily to mobile technology (cell phones). Convenience of wireless at the cost of wellness is short-term thinking and this type of thinking is affecting future generations. Educating health care providers, the public, and policy makers is of upmost urgency.
Funding:
This research received no external funding.
Conflict of Interest:
The author declares no conflict of interest.
References
- Mild, K.H.; Repacholi, M; van Deventer, E; Ravazzani, P. (Ed). Electromagnetic Hypersensitivity, Proceedings: International Workshop on EMF Hypersensitivity Prague, Czech Republic, 25-27 October 2004, published 2006. https://apps.who.int/iris/handle/10665/43435
- Pope, J. Report of the Royal Commission on A Dispute Respecting Hours of Employment between The Bell Telephone Company of Canada, Ltd. And Operators at Toronto, Ont., Issued by the Department of Labour, Canada, Ottawa, Government Printing Bureau, 1907. https://publications.gc.ca/site/eng/472922/publication.html
- Bevington, MJ. Electromagnetic-Sensitivity and Electromagnetic-Hypersensitivity: A Summary, Capability Books, London, UK. 2010; 43 pp. https://books.google.ca/books/about/Electromagnetic_Sensitivity_and_Electrom.html?id=Er3ntgAACAAJ&redir_esc=y
- Havas, M. Electrohypersensitivity (EHS) is an Environmentally-Induced disability that requires Immediate Attention. J Sci Discov. 2019, 3(1): 20 pp. http://www.e-discoverypublication.com/wp-content/uploads/2019/03/JSD18020-final.pdf
- Havas, M. When Theory and Observation Collide: Can non-ionizing radiation cause cancer? Environ Pollut 2017, 221:501-505. https://www.sciencedirect.com/science/article/abs/pii/S0269749116309526
- Havas, M. Electromagnetic Hypersensitivity: Biological Effects of Dirty Electricity with Emphasis on Diabetes and Multiple Sclerosis. Electromagn Biol Med 2006, 25:259–268. https://pubmed.ncbi.nlm.nih.gov/17178585/
- Havas, M. Dirty Electricity elevated blood sugar among electrically sensitive diabetics and ay explain brittle diabetes. Electromagn Biol Med 2008, 27:135–146. https://pubmed.ncbi.nlm.nih.gov/18568931/
- Havas, M. Radiation from wireless technology affects the blood, the heart, and the autonomic nervous system. Rev Environ Health 2013, 28(2-3):75–84. https://pubmed.ncbi.nlm.nih.gov/24192494/
- Havas, M. The Role of Electrosmog and Electrotherapy in Diagnosing and Treating Diabetics with Electrical Hypersensitivity. BAOJ Diabet 2016, 2: 014.
- Lai, H. Neurological effects of Radiofrequency Electromagnetic Radiation. In: Advances in Electromagnetic fields in Living Systems, 1994, Vol. 1. pp 27–80. https://link.springer.com/chapter/10.1007/978-1-4615-2542-4_2
- Rea, W.J.; Pan, Y.; Fenyves, E.J.; Sunisawa, I.; Suyama, H.; Samadi, N.; Ross, G.H. Electromagnetic field sensitivity. J. Bioelectr. 1991. 10: 241–256. https://www.tandfonline.com/doi/abs/10.3109/15368379109031410
- Johns Hopkins Medicine. Overview of Nervous System Disorders. 2023, https://www.hopkinsmedicine.org/health/conditions-and-diseases/overview-of-nervous-system-disorders
- Ouellet, M-C.; Beaulieu-Bonneau, S.; Morin, C.M. Chapter 10 – Traumatic Brain Injury. In: Handbook of Sleep Disorders in Medical Conditions. Science Direct. 2019, https://www.sciencedirect.com/science/article/abs/pii/B978012813014800010X?via%3Dihub
- Mortazavi, G; Mortazavi, S.M. Increased Mercury Release from Dental Amalgam Restorations after Exposure to Electromagnetic Fields as a Potential Hazard for Hypersensitive People and Pregnant Women. Rev Environ Health. 2015;30(4):287–92. doi: 10.1515/reveh-2015-0017. https://pubmed.ncbi.nlm.nih.gov/26544100/
- Paknahad, M.; Mortazavi, S.M.J.; Shahidi, S.; Mortazavi, G.; Haghani, M. Effect of radiofrequency radiation from Wi-Fi devices on mercury release from amalgam restorations. J Environmental Health Science and Engineering 2016, 14: 12 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4944481/
- CDC. Lyme Disease. Centers for Disease Control and Prevention, 2022, https://www.cdc.gov/lyme/index.html
- Anttila, K. Mycotoxins, fungus and ‘electrohypersensitivity’. Med. Hypotheses 2000 55(3):208-214. https://www.sciencedirect.com/science/article/abs/pii/S0306987799910459?via%3Dihub
- Belpomme, D.; Campagnac, C.; Irigaray, P. Reliable disease biomarkers characterizing and identifying electrohypersensitivity and multiple chemical sensitivity as two etiopathogenic aspects of a unique pathological disorder. Rev Environ Health 2015, 30(4):251–271. https://pubmed.ncbi.nlm.nih.gov/26613326/
- Yakymenko, I.; Tsybulin, O.; Sidorik, E.; Henshel, D.; Kyrylenko, O.; Kyrylenko, S. Oxidative mechanisms of biological activity of low-intensity radiofrequency radiation. Electromagn Biol Med 2016 35(2):186–202. https://pubmed.ncbi.nlm.nih.gov/26151230/
- Belyaev, I.; Dean, A.; Eger, H; Hubmann, G.; Jandrisovits, R.; Kern, M. et al. EUROPAEM EMF guideline 2016 for the prevention, diagnosis and treatment of EMF-related health problems and illnesses. Rev Environ Health 2016, 31:363–97. https://pubmed.ncbi.nlm.nih.gov/27454111/
- Editorial. Cause for concern: The rising incidence of early-onset pancreatic cancer. The Lancet, Gastroenterology & Hepatology 2023, 8(4): 287. https://www.thelancet.com/journals/langas/article/PIIS2468-1253(23)00039-0/fulltext
- Kim, J.; Gosnell, J.E.; Roman, S.A. Geographic influence in the global rise of thyroid cancer. Nat Rev Endocrinol 2020, 16, 17–29. https://doi.org/10.1038/s41574-019-0263-x
- Lin, X.; Xu, Y., Pan, X.; Xu, J.; Ding, Y.; et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: An analysis from 1990 to 2025. Scientific Reports, Nature Research 2020, (10):14790. https://www.nature.com/articles/s41598-020-71908-9
- Johansson, O. Disturbance of the immune system by electromagnetic fields—A potentially underlying cause for cellular damage and tissue repair reduction which could lead to disease and impairment. Pathophysiology 2009, 16(2-3):157–177. https://pubmed.ncbi.nlm.nih.gov/19398310/
- Rubik, B.; Brown, R. Evidence for a connection between coronavirus disease-19 and exposure to radiofrequency radiation from wireless communications including 5G. J Clini Trans Res 2021, 7(5):666–681. https://pubmed.ncbi.nlm.nih.gov/34778597/
- Dean, A.L.; Rea, W.J. 2012. Recommendations regarding Electromagnetic and Radiofrequency Exposure. American Academy of Environmental Medicine, https://www.aaemonline.org/recommendations-regarding-electromagnetic-radiofrequency-exposure/
- Guenter, D.; Delleman, B.; Parascandaio, F.; Dragos, S.M.; Freeman, K. Neuroplasticity-based treatment for fibromyalgia, chronic fatigue and multiple chemical sensitivity: feasibility and outcomes. McMaster University, 2019 (unpublished). https://retrainingthebrain.com/research/
- Menon, S.B.; Jayan, C. Eye movement desensitization and reprocessing: A conceptual Framework, Indian J Pschol Med 2010, 32(2):136–140. https://pubmed.ncbi.nlm.nih.gov/21716864/
- Yoshizumi, A.M.; Asis, D.G.; Luz, F.A. Auricular Chromotherapy in the Treatment, of Psychologic Trauma, Phobias, and Panic Disorder. Medical Acupuncture 2018, 30(3):151–154. https://pubmed.ncbi.nlm.nih.gov/29937969/
- Szmigielski, S. Reaction of the immune system to low-level RF/MW exposures. Sci Total Environ 2013, 454-455:393–400. https://pubmed.ncbi.nlm.nih.gov/23562692/
- Kuhn, T. Structure of the Scientific Revolution, The University of Chicago Press, Chicago, 1962.
- Liboff, A. Toward an Electromagnetic Paradigm for Biology and Medicine. J Alterative Complementary Med. 2004, 10(1):41–47. https://pubmed.ncbi.nlm.nih.gov/15025877/
- Stokowski, LA. Fundamentals of phototherapy for neonatal jaundice, Adv Neonatal Care 2006, 6(6):303–312, DOI: 10.1016/j.adnc.2006.08.004
- Partonen, T. Lonnqvist, J. Seasonal affective disorder, Lancet 1998, 352(9137):1369–1374. https://pubmed.ncbi.nlm.nih.gov/9802288/
- Vatansever, F.; Hamblin, M.R. Far infrared radiation (FIR): its biological effects and medical applications, Photonics Lasers Med 2012, 1(4):255–266. https://pubmed.ncbi.nlm.nih.gov/23833705/
- Yamauchi, N.; Einagawa, E.; Imai, K.; Kobuchi, K.; Li, R.; Taguchi, Y.; Umeda, M. High-Intensity Red Light-Emitting Diode Irradiation Suppresses the Inflammatory Response of Human Periodontal Ligament Stem Cells by Promoting Intracellular ATP Synthesis. Life (Basel) 2022, 12(5):736 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9144579/
- Shaw, K.; Symington, S.; Havas, M. Pilot Study: Pulsed Electromagnetic Field Therapy (PEMFT) Alleviates Symptoms of Osteoarthritis, Nov Tech Arthritis Bone Res 2017, 1(5):8 pp. https://juniperpublishers.com/ntab/pdf/NTAB.MS.ID555571.pdf
- Varani K.; Vincenzi, F.; Pasquini, S.; Blo, I.; Salati, S.; Cadossi, M.; De Mattei, M. Pulsed Electromagnetic Field Stimulation in Osteogenesis and Chondrogenesis: Signaling Pathways and Therapeutic Implications, Int. J Mol Sci 2021, 22(2):809 https://pubmed.ncbi.nlm.nih.gov/33467447/
- CamH. Repetitive Transcranial Magnetic Stimulation (rTMS). Centre for Addition and Mental Health, Toronto, 2003, https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/repetitive-transcranial-magnetic-stimulation
- Adey, WR. Electromagnetic fields, the modulation of brain tissue functions — A possible paradigm shift in biology, International Encyclopedia of Neuroscience, Third Edition; Adelman, G, Smith, B.H., Eds. Elsevier, New York, 2004, 21 pp. https://citeseerx.ist.psu.edu/document?repid=rep1&type=pdf&doi=0d38908cece9fe99d0079606c445d51d126069cd
- Popp, FA. Properties of biophotons and their theoretical implications, Indian J Exp Biol 2003 41(5):391–402. https://pubmed.ncbi.nlm.nih.gov/15244259/
- PRL Staff. Biophotons: Humans are “Beings of Light”, Premier Research Labs, 2022, https://prlabs.com/blog/biophoton-fritz-albert-popp.html
- Prasad, A.; Rossi, C.; Lamponi, S.; Pospisil, P.; Foletti, A. New perspective in cell communication: potential role of ultra-weak photon emission. J Photochem Photobiol B 2014, 139:47–53. https://pubmed.ncbi.nlm.nih.gov/24703082/
- Sun, Y.; Wang, C.; Dai, J. Biophotons as neural communication signals demonstrated by in situ biophoton autography. Photochem Photobiol 2010, 9(3):315–322. https://pubmed.ncbi.nlm.nih.gov/20221457/
- Tang, R.; Dai, J. Biophoton signal transmission and processing in the brain. J Photochem Photobiol B 2014, 139:71–75. https://pubmed.ncbi.nlm.nih.gov/24461927/
- Liboff, A. Electric-field ion cyclotron resonance. Bioelectromagnetics 1997, 17:85–87. https://pubmed.ncbi.nlm.nih.gov/9125238/