






Splenectomy for Spontaneous Rupture in Malaria Cases
Role of Splenectomy in Malaria Splenic Rupture: A Case Report
Albra Mohamed Hegazi ¹; Almuntasir Beallah Omer Mohamed Eltayb ²; Azza Fadol ³; Yusra Elhassan ¹, Tagwa Hegazi ⁴
¹ Sudan medical specialization board
² University Hospital Waterford
³ Ibn Sina Specialized Hospital
⁴ Kerry Mental Health Services
OPEN ACCESS
PUBLISHED: 31 July 2025
CITATION Hegazi, AM., and Mohamed Eltayb, ABO., 2025. Role of Splenectomy in Malaria Splenic Rupture: A Case Report. Medical Research Archives, [online] 13(7). https://doi.org/10.18103/mra.v13i7.6604
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i7.6604
ISSN 2375-1924
ABSTRACT
Background: Malaria is one of the most prevalent infectious diseases in Sudan, contributing significantly to morbidity and mortality. While most clinicians are familiar with its typical presentations, spontaneous splenic rupture is a rare but life-threatening complication that requires prompt recognition and management.
Case-Presentation: We report the case of a 51-year-old male who presented with acute left upper quadrant pain radiating to the left shoulder following recent treatment for malaria. On examination, he was hypotensive and tachycardic on arrival. Imaging revealed a sub-capsular splenic hematoma with free peritoneal fluid, consistent with a Grade III splenic rupture. Despite initial conservative measures, his condition deteriorated, necessitating emergency laparotomy and splenectomy. Postoperative recovery was uneventful, and the patient was discharged in good health with appropriate vaccinations.
Discussion: This case highlights the importance of maintaining a high index of suspicion for spontaneous splenic rupture in patients with malaria, especially in endemic regions like Sudan. Although conservative management can be considered in hemodynamically stable patients, splenectomy remains the definitive treatment in unstable cases.
Conclusion: Spontaneous splenic rupture is a rare but serious complication of malaria that necessitates prompt diagnosis and appropriate management. Early surgical intervention should be considered in unstable patients to prevent fatal outcomes.
Keywords: Malaria, Splenic rupture, Splenectomy, Sudan, Case report
INTRODUCTION
Malaria is one of the most significant parasitic diseases affecting humans worldwide, responsible for an estimated 500 million clinical cases and over 2.5 million deaths annually, with the highest burden in sub-Saharan Africa and Asia. The disease is caused by protozoan parasites of the genus Plasmodium, transmitted to humans through the bite of infected female Anopheles mosquitoes. Of the five known Plasmodium species that infect humans—P. falciparum, P. vivax, P. ovale, P. malariae, and P. knowlesi—P. falciparum and P. vivax are the most clinically relevant due to their high morbidity and mortality. P. falciparum is particularly notorious for causing severe malaria manifestations, including cerebral malaria, severe anemia, and multi-organ failure.
In Sudan, malaria remains a leading cause of morbidity and mortality. According to the World Health Organization, over 1.8 million cases were reported in 2019, accounting for 12.4% of all diseases documented by the national health sector, with a mortality rate of 13 per 10,000 cases. Historical data indicate an even higher burden, with approximately 9 million cases annually and 44,000 malaria-related deaths reported in 2007. The disease’s impact on the health system and economy is substantial, particularly in endemic regions such as Sudan, where transmission is influenced by factors like seasonal rainfall, socioeconomic status, and access to preventive measures.
The human spleen plays a critical role in the immune response against malaria. It serves as the primary site for the clearance of parasitized erythrocytes and the production of specific antibodies. During malaria infection, the spleen undergoes significant pathological changes, including hyperplasia of the lymphoid follicles, congestion, and increased phagocytic activity, often resulting in splenomegaly. Splenic enlargement is a common finding in malaria, reported in up to 80% of patients in endemic areas. However, this enlargement also renders the spleen more susceptible to complications such as infarction, subcapsular hematoma formation, and, rarely, spontaneous rupture.
Spontaneous splenic rupture is a rare but potentially life-threatening complication of malaria, with a reported mortality rate ranging from 15% to 70% depending on the underlying cause and promptness of intervention. The pathogenesis is multifactorial and not completely understood, but proposed mechanisms include cellular hyperplasia, venous congestion, vascular occlusion, thrombosis, and increased intra-abdominal pressure from activities like coughing or vomiting. These factors may lead to subcapsular hematoma formation and eventual rupture of the splenic capsule. Although P. vivax infection has been more frequently associated with splenic complications in some studies, P. falciparum can also cause severe splenic involvement.
Clinically, patients with spontaneous splenic rupture may present with vague symptoms such as left upper quadrant pain, which may radiate to the left shoulder (Kehr’s sign), and signs of hypovolemia including tachycardia, hypotension, and pallor. Notably, up to 50% of patients may lack overt abdominal symptoms, leading to delays in diagnosis. Imaging plays a crucial role in diagnosis, with ultrasonography and computed tomography (CT) being the most useful modalities.
Management strategies for spontaneous splenic rupture include conservative management for hemodynamically stable patients and surgical intervention for those with ongoing hemorrhage or hemodynamic instability. Historically, splenectomy was the standard treatment; however, with advances in imaging and critical care, conservative management is now increasingly considered in selected cases. Nevertheless, splenectomy remains the treatment of choice in unstable patients who fail to respond to resuscitative measures.
This case report aims to highlight the clinical presentation, diagnostic approach, and management of spontaneous splenic rupture in malaria infection, emphasizing the importance of recognizing this rare but serious complication in endemic regions like Sudan. By sharing this case, we hope to raise awareness and guide clinicians in early recognition and appropriate management to improve patient outcomes.
CASE PRESENTATION
A 51-year-old man with no significant past medical history presented to the emergency department with a two-day history of dull, aching pain in the left upper quadrant radiating to the left shoulder. He denied any trauma. Five days prior, he had been diagnosed with malaria and treated with antimalarial medications. On examination, he was tachycardic and hypotensive, with tenderness and rigidity in the left upper quadrant.
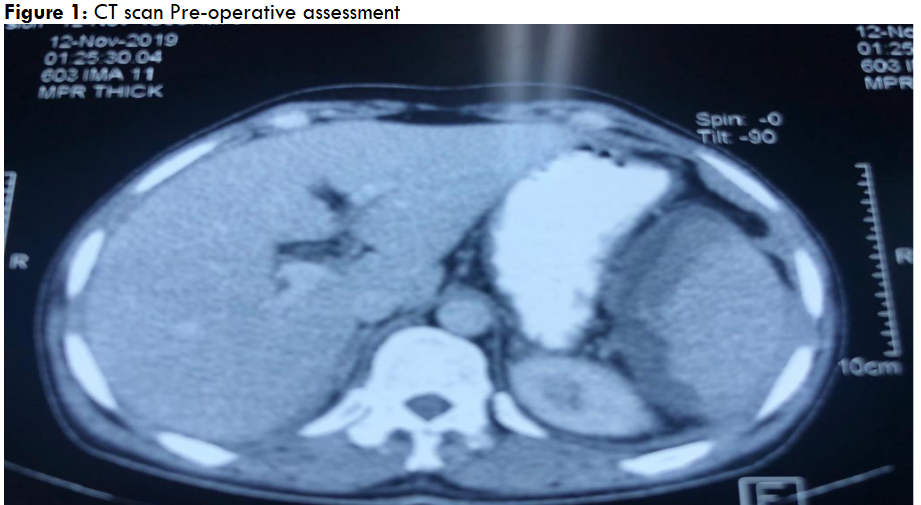
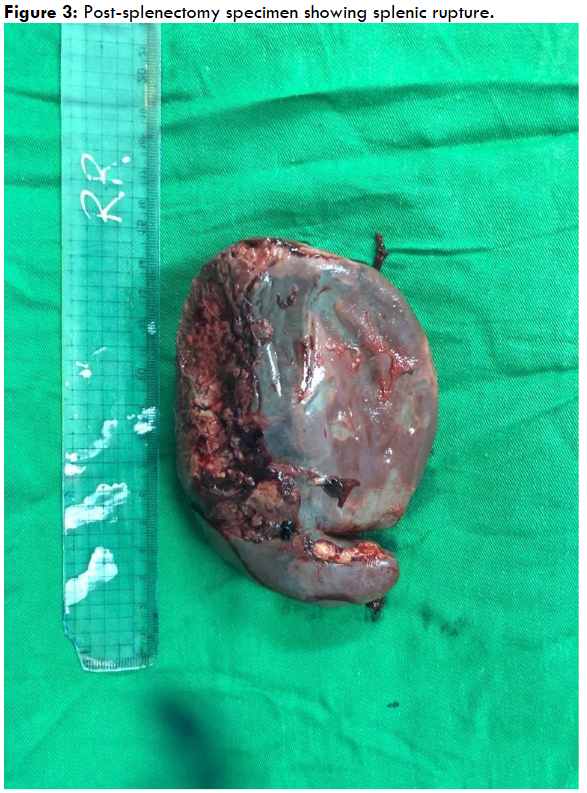
A CT scan of the abdomen revealed a 4 cm subcapsular splenic hematoma with free peritoneal fluid, consistent with a Grade III splenic rupture (Figure 1). The liver was unremarkable, and no active bleeding was noted. Initial conservative management, including intravenous fluids, blood transfusions, and antibiotics, failed to stabilize the patient. An exploratory laparotomy and splenectomy were performed (Figures 2 and 3).
The postoperative course was uneventful. At a one-month follow-up, the patient had fully recovered and received vaccinations against pneumococcus, Neisseria meningitidis, and Haemophilus influenzae.

DISCUSSION
Spontaneous splenic rupture (SSR) is a rare but potentially life-threatening complication of malaria that demands a high index of suspicion and prompt intervention. It has been reported in both Plasmodium falciparum and Plasmodium vivax infections, with P. vivax historically considered more frequently associated with splenic complications due to repeated cycles of infection leading to chronic congestion and fibrosis. However, more recent studies have confirmed that P. falciparum infection can also result in severe splenic involvement, including SSR.
The exact pathogenesis of SSR in malaria is multifactorial and incompletely understood. Proposed mechanisms include marked reticuloendothelial hyperplasia leading to increased intrasplenic tension, venous congestion caused by sequestration of parasitized erythrocytes, and vascular occlusion resulting in infarction and subcapsular hematoma formation. Additional triggers—such as sudden increases in intra-abdominal pressure from coughing, sneezing, or vomiting—can precipitate capsule rupture in an already enlarged and fragile spleen.
Clinical presentation of SSR can be highly variable. Patients typically present with left upper quadrant pain that may radiate to the left shoulder (Kehr’s sign) and symptoms of hypovolemia, including tachycardia, hypotension, and pallor. However, as reported by Yagmur et al, up to 50% of cases may initially lack classic abdominal symptoms, contributing to diagnostic delays and increasing the risk of fatal outcomes. Imaging is indispensable for diagnosis: ultrasonography is a readily available, non-invasive modality that can detect splenic enlargement, subcapsular hematomas, and free intraperitoneal fluid. Computed tomography (CT) offers superior sensitivity and specificity, allowing precise grading of splenic injuries, detection of small hematomas, and assessment of active bleeding.
Management strategies for SSR hinge on the patient’s hemodynamic status and the extent of the rupture. In hemodynamically stable patients with contained hematomas, conservative management—including strict bed rest, antimalarial therapy, blood transfusions, and close monitoring—has been successfully employed. Osman et al reported successful non-operative management in select patients, though they emphasized the need for intensive monitoring and appropriate imaging follow-up. Nonetheless, conservative management carries a risk of delayed rupture and sudden decompensation, especially in settings with limited resources for close observation.
For patients with ongoing hemorrhage or hemodynamic instability, splenectomy remains the gold standard treatment. This approach rapidly controls bleeding, preventing fatal outcomes. In our case, despite initial conservative measures, the patient’s continued hemodynamic deterioration mandated surgical intervention. Embolization of the splenic artery has been described as an alternative to splenectomy in selected patients, but it requires interventional radiology expertise and equipment that may not be available in many malaria-endemic regions.
Post-splenectomy care is crucial to reduce the risk of overwhelming post-splenectomy infection (OPSI), primarily caused by encapsulated bacteria such as Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis. Vaccination against these organisms is recommended preoperatively (if possible) or in the early postoperative period, along with patient education regarding prompt medical attention for febrile illnesses.
CONCLUSION
In conclusion, Spontaneous splenic rupture in malaria is a rare but serious complication of malaria that requires a high index of suspicion, especially in endemic areas. While conservative management is an option in stable patients, splenectomy remains the definitive treatment in unstable patients. Early recognition, appropriate imaging, and timely surgical intervention in unstable patients are critical for improving outcomes. Preventive measures, including vaccination, should always be part of comprehensive patient care post-splenectomy.
DECLARATION:
ETHICAL APPROVAL: Ethical approval for this case report was obtained from the Department of Surgery, Omdurman Teaching Hospital.
PATIENT CONSENT: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the signed consent is available for review by the Editor-in-Chief of this journal.
DATA AVAILABILITY: All data supporting the findings of this case are available within the article and referenced literature.
COMPETING INTERESTS: The authors declare no competing interests.
FUNDING: No financial support was received for this study.
AUTHOR CONTRIBUTIONS: Both authors contributed equally to the conception, drafting, revision, and final approval of the manuscript.
ACKNOWLEDGMENTS: The authors would like to thank the surgical and radiology teams at Omdurman Teaching Hospital for their clinical support and collaboration.
REFERENCES
- Alani AM, Kolleri JJ, Ekeer A, Ibrahim ZAA. Spontaneous splenic rupture in malaria patients: two case reports. Cureus. 2021;13(12):e20344. doi:10.7759/cureus.20344
- Joshi SV, Nichat PD, Ansari K, et al. Spontaneous splenic rupture in a case of P. vivax infection: a rare case report. Glob J Res Anal. 2022;11(10):138-139. doi:10.36106/gjra/9509530
- Odeh A, et al. Spontaneous splenic rupture as a complication of malaria and incidental acute appendicitis: a case report. Cureus. 2021;13(10):e19028. doi:10.7759/cureus.19028
- Keller M. Malaria in Sudan. Sudan Health Report. 2020;9.3M 1.1M:1-6.
- Saad E, Elsamani E, Abdelrahman W. Spontaneous splenic rupture complicating severe P. falciparum infection: a case report and literature review. Case Rep Infect Dis. 2019;2019:2781647. doi:10.1155/2019/2781647
- Yagmur Y, Kara IH, Aldemir M, et al. Spontaneous rupture of malarial spleen: two case reports and a review of the literature. Crit Care. 2000;4(5):309-313. doi:10.1186/cc713
- Nyada SR, Voundi EV, Messi SE, Ebune JL. Per operatory finding of spontaneous rupture of the spleen: a case report. World J Adv Res Rev. 2022;15(3):328-330. doi:10.30574/wjarr.2022.15.3.0945
- Osman MF, Elkhidir IM, Rogers SO, Williams M. Non-operative management of malarial splenic rupture: the Khartoum experience and an international review. Int J Surg. 2012;10(9):410-414. doi:10.1016/j.ijsu.2012.06.001
- Mebius RE, Kraal G. Structure and function of the spleen. Nat Rev Immunol. 2005;5(8):606-616. doi:10.1038/nri1669
- Ferraioli G, Brunetti E, Gulizia R, et al. Sonographic assessment of splenic involvement in malaria patients. J Ultrasound Med. 1999;18(9):639-643. doi:10.7863/jum.1999.18.9.639
- Hofman FN, Kluin PM, van de Wiel A. Splenic artery embolization in patients with spontaneous splenic rupture: a systematic review. J Vasc Interv Radiol. 2007;18(11):1477-1483. doi:10.1016/j.jvir.2007.07.015
- Davidson RN. Non-immune travellers and malaria. J Infect. 1998;37(2):153-160. doi:10.1016/S0163-4453(98)90119-2