





Thyroid Abscess with Medullary Carcinoma: A Rare Case
The Thyroid Abscess Camoflague- A Unique Case of Thyroid Abscess with Medullary Carcinoma Thyroid
Dr Athira TS 1; Dr. Geethalakshmi Sampathkumar 2; Dr K Kala 3; Dr Rajkumar 4
- MBBS, Resident, Department of Family Medicine, Dr Kamakshi Memorial Hospital, Pallikaranai, Chennai
- MD General Medicine, DM Endocrinology, Consultant, Endocrinologist, Dr Kamakshi Memorial Hospital, Pallikaranai, Chennai
- MD DNB Pathology, Consultant, Pathologist, Dr Kamakshi Memorial Hospital, Pallikaranai, Chennai
- MCh Surgical Oncology, Consultant, Surgical Oncologist, Dr Kamakshi Memorial Hospital, Pallikaranai, Chennai
OPEN ACCESS
PUBLISHED:30 November 2024
CITATION Athira, TS., Geethalakshmi, S., et al., 2024. The Thyroid Abscess Camouflage- A Unique Case of Thyroid Abscess with Medullary Carcinoma Thyroid. Medical Research Archives, [online] 12(11). https://doi.org/10.18103/mra.v12i11.5870
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.5870
ISSN 2375-1924
ABSTRACT
Acute suppurative thyroiditis is a rare infectious disease of the thyroid gland. Its onset is generally sudden, and the clinical picture progresses very rapidly. It represents less than 1% of all thyroid diseases and if untreated, could potentially become a life-threatening endocrine emergency. Herein, we report a rare case of thyroid abscess with underlying Medullary thyroid carcinoma in an elderly male who presented with poorly controlled diabetes, chronic kidney disease, and urosepsis. During his treatment, an incidental thyroid abscess was detected, which we managed successfully with intravenous antibiotics and aspiration of pus. Upon discharge, on regular follow-up, we noted a calcified nodule adjacent to the resolved abscess. Fine Needle Aspiration suggested it was a malignant lesion and he underwent a total thyroidectomy. Histopathological Examination revealed it as Medullary thyroid carcinoma. Recognizing the significant impact of this case on clinical decisions and patient prognosis, a delay in diagnosis might have endangered our patient’s life. We believe this to be a rare presentation of such an association, reporting for the first time in literature.
Keywords: Acute suppurative thyroiditis, Medullary carcinoma thyroid, immunocompromised, elderly.
INTRODUCTION
Acute thyroid infection is a less-seen diagnosis, mostly because the gland is inherently protected by encapsulation, a rich lymphovascular supply, and iodine content. Acute Suppurative Thyroiditis (AST) comprises 0.1%-0.7 of all thyroid diseases. The age of occurrence is not always reported. It predominantly presents in childhood (80% in < 10 years and only 8% occur in adulthood with no gender preference. However, the clinical picture may differ between children and adults. The presence of anatomic aberrations like branchial arch anomalies or a piriform fistula may predispose to acute thyroid infection in the pediatric population. In adults, the commonest reasons include an immunosuppressed state (post-transplant, Acquired Immunodeficiency Syndrome), iatrogenic infections (Fine Needle Aspiration, direct trauma), or a history of underlying thyroid disease. Most cases have a bacterial etiology, among which Staphylococcus aureus is the predominant cause. Others include Streptococcus and Salmonella. Mycobacterium can rarely be involved, and fungal agents are the causative agents among immunocompromised patients. Our patient represents an extraordinary case of thyroid abscess with concomitant medullary thyroid carcinoma with uncontrolled diabetes mellitus (HbA1C-12%) in the background of chronic kidney disease and urosepsis who was diagnosed with AST at a very early stage of the disease. Despite advances in diagnostic testing and antibiotic treatments, the mortality rate is high in AST without intervention. Early diagnosis and treatment of Acute Suppurative Thyroiditis remains paramount to prevent poor outcomes. Clinicians should be cognizant of anchoring bias, which can lead to misdiagnosis and mismanagement of Acute Suppurative Thyroiditis.
CASE REPORT
A 74-year-old Indian male who is a known case of Type 2 Diabetes Mellitus and Systemic hypertension presented with 5 days of reduced oral intake and altered sensorium. On examination he was drowsy with a Glassgow Coma Scale -E3V4M5, with the rest of the vitals normal. Capillary blood glucose was very high with urine ketones negative. Arterial blood gas showed severe metabolic acidosis. Admission lab investigations are given below:
| TESTS | VALUES | REFERENCES |
|---|---|---|
| Total count | 16.9x 109/L | 4.5-11.0 x109/L |
| Serum Urea | 49.5mmol/L | 3.6-7.1 mmol/L |
| Serum Creatinine | 0.46mmol/L | 0.06-0.11mmol/L |
| Hba1c | 116mmol/L | |
| Serum Procalcitonin | 0.0066mcg/L | <0.005 mcg/L |
| TSH | 1.36 micro IU/ml | 0.27-4.2microIU/ml |
| Total T3 | 1.3nmol/L | 1.2-3.1nmol/L |
| Total T4 | 146.2nmol/L | 65.6-185.4nmol/L |
| Urine pus cells | >25pus cells | |
| Urine culture and sensitivity | E. coli growth of 1 lakh CFU/ml | |
| Blood culture sensitivity | No growth | |
| Covid RT-PCR | Negative | |
| ECHO | Concentric LVH, No RWMA, LVEF-66%, No vegetation. |
Ultrasound of the neck showed features suggestive of thyroid abscess.
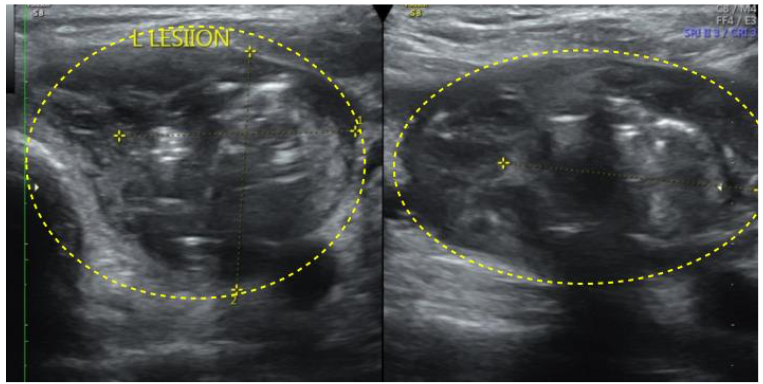
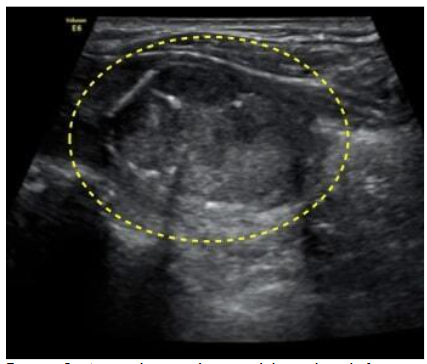
Initial Thyroid FNA biopsy showed inflammatory pathology. Pus aspirate culture and sensitivity showed heavy growth of E. coli> 1 lakh /CFU, sensitive to Imipenem, Meropenem, Ciprofloxacin, and Levofloxacin. The patient was treated with IV antibiotics (Meropenem), insulin, and hemodialysis due to progressive azotemia and oliguria. The patient improved clinically and hence was discharged on oral fluoroquinolones for a period of 6 weeks. Follow-up USG Neck showed resolution of the hypoechoic lesion, but the presence of an adjacent new lesion.
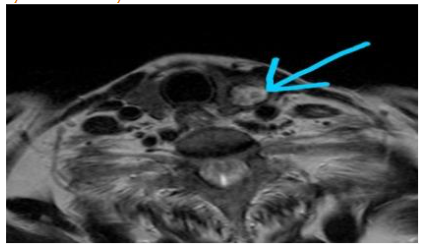
MRI Neck showed a solid ovoid nodule in the left lobe of the thyroid. Few mildly enlarged ovoid nodes in bilateral IB, II region-reactive morphology.
FNA biopsy of thyroid nodule was suggestive of malignancy.
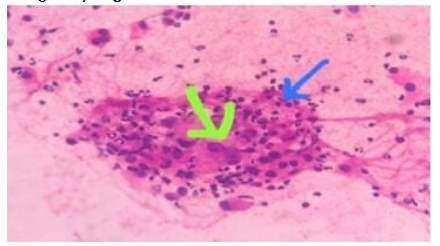
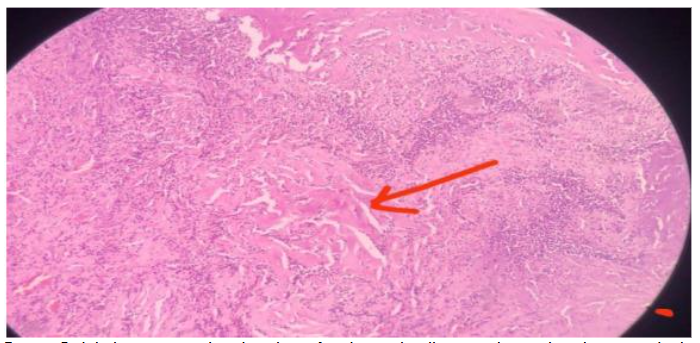
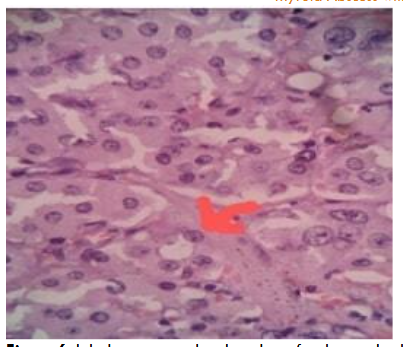
He underwent Total thyroidectomy with left paratracheal dissection. Histopathological examination showed features suggestive of Medullary Thyroid Carcinoma.
Carcinoembryonic antigen and Serum Calcitonin were normal.

Even though we couldn’t do a family screening for Medullary thyroid carcinoma, our patient didn’t have supportive features for Multiple Endocrine Neoplasia syndrome. Our patient is on regular follow-up and to date, he has had no further recurrences or metastasis.
DISCUSSION
Acute suppurative thyroiditis comprises 0.1% – 0.7 of all thyroid diseases, a rarity attributed to the gland’s inherent characteristics, which make it resistant to infection. Usually, the causative organisms are Staphylococcus and Streptococcus species(35-45%) followed by Gram-negative organisms (25%) and anaerobes(9% to 12%). Rarely the etiology being mycobacterial and fungal. In our case, E. coli was the causative organism. In general, Infections at unusual sites (eg. thyroid) are more common in diabetics than nondiabetics due to impaired immunity for example impaired neutrophilic chemotaxis and phagocytosis. In our patient, the poor glycemic state/impaired immunity could have triggered the episode of AST. In adults, proposed routes of infection for AST include lymphatic, hematogenous spread, or direct inoculum of the thyroid or surrounding anatomy, a direct extension of an abscess, and spread through a pyriform sinus fistula, usually in the setting of preexisting thyroid disease or an immunocompromised state. Our patient who was in urosepsis had grown E. coli in his urine culture. The pus culture from the thyroid abscess also showed heavy growth of E. coli which supports the possible hematogenous mode of spread from a distant infective source.
In AST the clinical spectrum is broad as even asymptomatic cases have been reported. Clinical features often include fever, sore throat, pain and swelling in the anterior midline of the neck, dermal erythema, dysphagia, hoarseness, and limitation of head movements. The left lobe is more commonly involved than the right. Tachycardia, leukocytosis, and increased ESR are seen as common with normal thyroid function tests. However exceptions have also been reported; in one study, 12% of patients were reported to have thyrotoxicosis, and 17% were reported with hypothyroidism. As shown in most of the studies, in our case also, the left lobe of the thyroid was infected and the patient was in a euthyroid state.
Some case reports have described concomitant AST with thyroid cancer. One case developed AST after Fine Needle Aspiration of Papillary Thyroid Carcinoma, which was therefore considered as an infection secondary to needle aspiration. At times AST occurs in a background of thyroid malignancy. However, the reason remains unclear. A previous case report suggested that an abnormal blood supply from a malignant tumor could have facilitated infection, and might be in our case too. Our case was uncommon in terms of clinical presentation. Our patient presented with urosepsis in encephalopathy without any local signs or symptoms of thyroid abscess. Initially, we started treating the underlying urosepsis but despite receiving higher-end antibiotics, the patient showed no clinical improvement. It was an incidental finding in the CT Chest, which later led us to the diagnosis and gave us the reason for the patient’s deterioration.
Ultrasound of the neck region adequately demonstrates intra or extra-thyroid abscesses and solid or mixed thyroid gland lesions and adjacent inflammatory nodes. Thyroid abscess is rare and has unusual clinical features, so its diagnosis is often delayed. This results in complications and deadly outcomes if not diagnosed early and treated adequately. The USG neck showed a large heterogenous hypoechoic complex avascular cystic lesion with thick septations and multiple air pockets in our patient. Most often FNA could give us a clue to the diagnosis and is also a good means for identifying the bacteriologic source and for precise antibiotic selection. In our case, initial FNA could only demonstrate inflammatory cells, and no malignant cells were reported which made the differentiation of AST from Medullary thyroid carcinoma difficult in the early phases.
Our case became interesting as it was an absolute camouflage by the thyroid abscess as suggested in the title. We treated our case with aggressive IV antibiotics for urosepsis and superadded thyroid abscess. The patient improved clinically and was discharged. He was advised for regular follow-up with a complete hemogram and C Reactive Protein. But we didn’t know that the thyroid abscess was only the tip of the iceberg. Further, follow-up imaging of the thyroid showed complete regression of the thyroid abscess with the unmasking of an iso-hyperechoic nodule with calcification in the left thyroid lobe near the previous lesion. Fine Needle Aspiration Cytology showed malignancy features, Bethesda category 6. Our patient underwent a total thyroidectomy with left paratracheal lymph node dissection. Histopathological evaluation revealed Medullary carcinoma of the thyroid. Carcinoembryonic antigen and serum calcitonin were normal. In our case, the thyroid abscess helped to diagnose the malignancy at a very early stage. Overall AST has 3.7%-9% of reported mortality. and Medullary carcinoma accounts for 5% of all thyroid cancers with 13% of thyroid cancer-related deaths. Luckily, even though as an incidental finding, our timely intervention helped our patient to recover completely, thus preventing mortality.
CONCLUSION
In the absence of clinical evidence of thyroid abscess, and it being a rare entity, reaching a diagnosis is always a challenge. Ours was a case of thyroid abscess with concomitant Medullary thyroid carcinoma involving the left lobe of the thyroid in an elderly male which has not been documented anywhere in the literature to date. Timely diagnosis and proper source reduction along with appropriate antibiotics could reduce the mortality rate in the case of AST with concomitant thyroid carcinoma even in the elderly. Regular follow-up is mandatory in any case of AST, as in our case Medullary thyroid carcinoma was revealed later on follow-up, which helped us in prompt management and better clinical outcome. Also, any lesions in the elderly age group, should not prevent us from thinking of a malignant etiology even if it presents differently.
REFERENCES
- Al-Dajani N, Wootton SH, Cervical lymphadenitis, suppurative parotitis, thyroiditis, and infected cysts. Infect Dis Clin North Am. 2007;21(2):523-541, viii. doi:10.1016/j.idc.2007.03.004
- Ghaemi N, Sayedi J, Bagheri S. Acute suppurative thyroiditis with thyroid abscess: a case report and review of the literature. Iran J Otorhinolaryngol. 2014;26(74):51-55.
- Williams J, Abdul Wahab AH, Leman WI. Successful Treatment of a Thyroid Abscess in a Pediatric Patient: A Case Report. Cureus. 16(4):e57428. doi:10.7759/cureus.57428
- Madana J, Yolmo D, Saxena SK, Gopalakrishnan S. Thyroid abscess with branchial anomaly. International Journal of Pediatric Otorhinolaryngology Extra. 2010;5(4):170-173. doi:10.1016/j.pedex.2009.09.004
- Engineer D, Prakash S, Yadav A, et al. Acute thyroid swelling in renal transplant recipient. Indian J Nephrol. 2017;27(6):462. doi:10.4103/ijn.IJN_335_16
- Yedla N, Pirela D, Manzano A, Tuda C, Lo Presti S. Thyroid Abscess: Challenges in Diagnosis and Management. J Investig Med High Impact Case Rep. 2018;6:2324709618778709. doi:10.1177/2324709618778709
- Htet ZW, Tai ES, Yang SP. Acute Bacterial Suppurative Thyroiditis following Fine Needle Aspiration: A Case Report and Review of the Literature. Case Reports in Endocrinology. 2020;2020:e7104806. doi:10.1155/2020/7104806
- Sanker V, Mohamed A, Jadhav C. Acute Suppurative Thyroiditis (AST) With Thyroid Abscess: A Rare and Potentially Fatal Neck Infection. Cureus. 2022;14(9):e29062. doi:10.7759/cureus.29062
- Igarashi H, Yoshino H, Hijikata M, et al. Acute suppurative thyroiditis in infected thyroid cyst in an adult patient under hemodialysis. Clinical Case Reports. 2017;5(5):570-573. doi:10.1002/ccr3.861
- Chainchel Singh MK, Vijayanathan A. Idiopathic Thyroid Abscess – A Rare Occurrence. Eur Endocrinol. 2019;15(1):42-43. doi:10.17925/EE.2019.15.1.42
- Thada ND, Prasad SC, Alva B, Pokharel M, Prasad KC. A Rare Case of Suppurative Aspergillosis of the Thyroid. Case Reports in Otolaryngology. 2013;2013. doi:10.1155/2013/956236
- Sharma RK, McManus C, Kuo JH. Idiopathic thyroid abscess in a healthy 22-year old female – A case of anchoring bias. Journal of Clinical and Translational Endocrinology: Case Reports. 2021;19:100073. doi:10.1016/j.jecr.2020.100073
- Baba HO, Salih AM, Hammood ZD, et al. Acute suppurative thyroiditis progressing to a thyroid abscess; a case report with review of literature. International Journal of Surgery Open. 2022;38:100433. doi:10.1016/j.ijso.2021.100433
- Brook I. Microbiology and management of acute suppurative thyroiditis in children. International Journal of Pediatric Otorhinolaryngology. 2003;67(5):447-451. doi:10.1016/S0165-5876(03)00010-7
- Haddad FH, Malkawi OM, Omari AA, et al. Diabetes and infarcted papillary thyroid cancer.
- Sen S, Ramakant P, Paul MJ, Jennifer A. Case Report: Acute suppurative thyroiditis secondary to urinary tract infection by E. coli: a rare clinical scenario. BMJ Case Reports. 2016;2016. doi:10.1136/bcr-2015-213231
- Falhammar H, Wallin G, Calissendorff J. Acute suppurative thyroiditis with thyroid abscess in adults: clinical presentation, treatment and outcomes. BMC Endocr Disord. 2019;19:130. doi:10.1186/s12902-019-0458-0
- Panda SK, Patro B, Samantaroy MR, Mishra J, Mohapatra KC, Meher RK. Unusual presentation of follicular carcinoma thyroid with special emphasis on their management. Int J Surg Case Rep. 2014;5(7):408-411. doi:10.1016/j.ijscr.2014.03.006
- Otani H, Notsu M, Koike S, et al. Acute suppurative thyroiditis caused by thyroid papillary carcinoma in the right thyroid lobe of a healthy woman. Thyroid Res. 2018;11:4. doi:10.1186/s13044-018-0049-6
- Priya R, Virmani N, Dabholkar JP. Medullary Carcinoma of Thyroid: Case Report and a Review of Literature. Journal of Head & Neck Physicians and Surgeons. 2016;4(2):80. doi:10.4103/2347-8128.196232
- Lafontaine N, Learoyd D, Farrel S, Wong R. Suppurative thyroiditis: Systematic review and clinical guidance. Clin Endocrinol (Oxf). 2021;95(2):253-264. doi:10.1111/cen.14440