

Religiosity, Spirituality, and Mental Health in HIV Women
The Relationship between Religiosity/Spirituality and Mental Health among a Cohort of Women with HIV
Sneha Akurati¹, Katherine Ujunwa¹, Said K. Abdelrhman², Lunthita M. Duthely³*
- University of Miami Miller School of Medicine, Department of Medical Education
- University of Texas Medical Branch, School of Public & Population Sciences
- University of Miami Miller School of Medicine, Department of Obstetrics, Gynecology and Reproductive Sciences
OPEN ACCESS
PUBLISHED: 31 July 2025
CITATION: Akurati, S., Ujunwa, K., et al., 2025. The Relationship between Religiosity/Spirituality and Mental Health among a Cohort of Women with HIV. Medical Research Archives, [online] 13(7).
https://doi.org/10.18103/mra.v13i7.6616
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i7.6616
ISSN 2375-1924
Abstract
Background: Low mental health status, specifically depression, poses a significant challenge to the management of HIV, as it interferes with treatment adherence and contributes to health decline for individuals with HIV. This burden is particularly pronounced among women with HIV, who often experience a higher prevalence of depression compared to men. Several individual-level, psychosocial factors, including religiosity, spirituality and resilience, have been identified as factors that may mitigate challenges with adherence. We sought, primarily, to understand the relationship between religiosity/spirituality and mental health status, and, secondarily, the relationship between religiosity/spirituality and adherence to HIV care.
Methods: This cross-sectional study analyzed the association between self-reported religiosity/spirituality and depression and religiosity/spirituality and suppression of HIV viral load, a marker for adherence, among a cohort of (N=54) women with a recent history of HIV care non-adherence. HIV viral load and HIV visit history were extracted from the medical record. Participants receiving care from a South Florida HIV care clinic completed the PHQ-9, which assesses depressive symptoms, and the Connor-Davidson Resilience Scale (CD-RISC-25), which measures individual-level resilience. Religiosity/Spirituality was operationalized using one item of the CD-RISC-25 and dichotomized into Religious/Spiritual and Non-Religious/Spiritual groups. T-tests examined group differences. Statistical models measured the association between religiosity/spirituality and depression, as well as the relationship between religiosity/spirituality and HIV viral load suppression.
Results: Religious/Spiritual participants had significantly lower PHQ-9 scores (mean = 5.02, SD = 5.53), compared to Non-Religious/Spiritual participants (mean = 11.29, SD = 6.21; p = 0.0188). A significant, negative correlation was found between religiosity/spirituality and PHQ-9 scores (r = 0.357, p = 0.007), with religiosity/spirituality explaining 12.8% of the variance in depression severity. Among Hispanic participants, the difference in PHQ-9 scores by religiosity/spirituality approached significance (p = 0.0574).
Conclusion: Self-reported religiosity/spirituality was associated with significantly lower depressive symptoms among women with HIV, suggesting that spirituality may be a meaningful psychosocial resource. There was a trend toward HIV viral load suppression for participants who were Religious/Spiritual; the relationship, however, was not significant. Faith-based and spiritually-oriented interventions should be further explored as culturally relevant strategies to support mental health and care adherence for women with HIV; however, further study is needed.
Keywords
HIV, mental health, religiosity, spirituality, women, depression, adherence
Introduction
An estimated 39.9 million people are living with human immunodeficiency virus (HIV) worldwide with most people living with the disease being women and girls. In the United States, this number drops to 1.2 million people living with HIV, with nearly half of the new infections occurring in the South. Fortunately, the introduction of antiretroviral therapy (ART) has significantly lessened the mortality attributable to the disease. Despite the introduction of virtual wonder drugs, where the HIV virus can be driven down to undetectable levels, the morbidity associated with HIV is yet to be eliminated likely due to varying levels of access and adherence. There are several factors that contribute to poor adherence among people living with HIV. Among these are low mental health status, minority status, and low income. For many individuals, these factors overlap and compound their experience, making it especially burdensome. Low mental health status, specifically depression, may interfere significantly with treatment adherence and lead to a worsening disease state. Notably, the burden of low mental health status is especially high among women with HIV, who experience depression at a greater rate, compared to their male counterparts.
Racial and ethnic minoritized women experience health-care related disparities at rates higher than their counterparts. These disparities extend into the realm of HIV care as African American women experience lower access to care and increased morbidity and mortality associated with the disease, all while being more likely to have adverse effects associated with HIV discrimination, an unfortunate experience also shared with Hispanic women living in the United States. Of note, factors like ethnic identity and religion/spirituality were found to particularly pertain to mental health status.
There are varying definitions of religiosity and spirituality. Mishra et al. describe spirituality as a relationship with a higher being and how that influences their decisions and perspectives; religiosity, specifically, guides and informs these beliefs. Literature has shown varied relationships between religiosity and mental health status. Some studies have linked higher religiosity with lower levels of depression and suggest that there is a potential benefit to religion and spirituality, especially as they pertain to medication adherence for chronic diseases, including HIV. Other studies have linked higher religiosity/spirituality to higher levels of depression. The current study sought to explore the relationship between religiosity and mental health status among a cohort of women with HIV as a continuation of mixed-methods work conducted by Duthely et al., that found, quantitatively, an inverse relationship between depressive symptomology and viral suppression and, qualitatively, that religion/spirituality was a facilitator to adherence to HIV care.
Since the onset of the COVID-19 pandemic, there has been a substantial increase in interest regarding the intersection of mental health and religiosity/spirituality, as the pandemic has acted as a major psychosocial stressor globally. Multiple studies have documented that individuals have turned to religious and spiritual practices as coping mechanisms in response to heightened psychological distress, with both positive and negative changes in religious engagement observed across diverse populations. Notably, religious beliefs and practices have been associated with lower levels of depression, anxiety, and suicidal ideation, and have served as protective factors for mental health during the pandemic, particularly among women and minority groups. These findings are especially relevant for minority ethnic women living with HIV, who face unique psychosocial and health-related challenges that may be further exacerbated by pandemic-related stressors. The increased salience of religiosity and spirituality in the context of mental health since the pandemic thus provides a compelling rationale for investigating their roles in the well-being of minority ethnic women with HIV.
Religiosity and spirituality have been shown to influence both mental health and clinical outcomes in people living with HIV. Positive religious coping is associated with greater medication adherence, lower perceived stress, and fewer depressive symptoms. Higher levels of spiritual well-being have also been linked to improved HIV-related immune functioning, including higher CD4 counts and lower viral loads. For women living with HIV, who often face compounded stigma and economic hardship, spirituality can offer a meaningful source of strength, identity, and community. However, the relationship is not uniformly beneficial. Some studies report that negative religious coping such as feelings of abandonment by God or religious guilt is associated with worsened mental health outcomes, including higher levels of depression.
These findings underscore the importance of understanding not only the presence of religiosity but also its quality and function in the context of coping with chronic illness. Despite emerging research linking religiosity and mental health, few studies have focused specifically on racially and ethnically minoritized women living with HIV in the United States, a group disproportionately affected by both structural barriers and psychosocial stressors. Given the growing interest in spirituality as a coping mechanism and its potential influence on depression and care adherence, our study examined the relationship between religiosity and mental health within this population. This study builds on prior work to examine how spirituality may promote psychological resilience and improve treatment adherence among vulnerable women living with HIV.
Methods
This cross-sectional study examined the relationship between religiosity/spirituality and mental health outcomes among women with HIV and a recent history of non-adherence to HIV care. The sample comprised 54 participants, all of whom were recruited from a single-site HIV care facility in South Florida between March 2019 and February 2020. The clinic primarily serves African American, Caribbean-American, and Hispanic American women. Inclusion criteria included: (1) being biologically female, (2) age 18 or older, (3) having a confirmed HIV diagnosis, (4) a recent history of non-adherence to HIV care (defined as sub-optimal engagement with care in the past 12 months), and (5) receiving care at the participating clinic. Exclusion criteria included cognitive impairment that would preclude informed consent or accurate survey completion, and current enrollment in an inpatient psychiatric or substance use treatment program. The study design and its implementation were informed by earlier findings and frameworks described in Duthely et al., 2021, which identified the roles of stigma, resilience, and faith in HIV care adherence.
Participants completed a series of validated, self-report assessments, available in their language of choice. Depressive symptoms were measured using the Patient Health Questionnaire-9 (PHQ-9; α = 0.89), and resilience was measured with the Connor-Davidson Resilience Scale (CD-RISC- α = 0.89). Religiosity/spirituality was operationalized using item 3 of the CD-RISC-25, which assesses the degree to which faith is a source of strength. Responses were collected and analyzed. Clinical data, including HIV viral load and HIV visit history, were abstracted from electronic medical records. T-tests compared PHQ-9 scores between religious/spiritual and non-religious participants. Linear regression assessed the relationship between CD-RISC Q3 (religious/spiritual) and PHQ-9 scores (depressive symptoms). A binary logistic regression examined the odds of HIV viral load suppression by religiosity status and demographic factors.
Ethical approval for this study was obtained from the Institutional Review Board at the University of Miami Miller School of Medicine, and all participants gave informed consent prior to participation.
Results
| Demographic and Socioeconomic Profile of Religious vs. Non-Religious Participants (N = 54) | Religious/Spiritual, (n = 47) % | Non-Religious/Spiritual, (n = 7) % |
|---|---|---|
| Race/Ethnicity | Black/African American 29 61.7 | 4 57.1 |
| Hispanic/Latin 13 27.7 | 3 42.9 | |
| White/non-Hispanic 2 4.3 | 0 0 | |
| Other 3 6.4 | 0 0 | |
| Education | Middle School or less 12 25.5 | 1 14.3 |
| High School / G.E.D. 29 61.7 | 5 71.4 | |
| Some College 3 6.4 | 0 0 | |
| Bachelor’s Degree 2 4.3 | 1 14.3 | |
| Annual Income (n=50) | $0 – $25,000 39 83.0 | 5 100.0 |
| $25,000 – $50,000 4 8.5 | 0 0 | |
| $50,000 – $100,000 1 2.1 | 0 0 | |
| More than $250,000 1 2.1 | 0 0 | |
| Employment Status | Unemployed 27 57.4 | 5 71.4 |
| Employed full-time 12 25.5 | 0 0 | |
| Employed part-time 8 17.0 | 2 28.6 | |
| Mean Age | 44.26 | 46.0 |
This table presents the demographic and socioeconomic profiles of participants stratified by religiosity/spirituality (Religious, n = 47; Non-Religious, n = 7). Variables include race/ethnicity, education level, annual income (n = 50), employment status, and mean age. The majority of participants identified as Black/African American, had a high school diploma or less, and reported low annual income (83% of religious/spiritual participants and 100% of non-religious/spiritual participants reported earning $25,000 or less). High unemployment was observed across both groups, particularly among non-religious/spiritual participants (71.4%). Few participants reported full-time employment. The mean age of participants was 44.26 years for religious and 46.0 years for non-religious individuals. This table highlights socioeconomic vulnerabilities shared across both groups, with slightly higher educational attainment and part-time employment in the religious/spiritual group.
| Summary Statistics of PHQ-9 scores by Religious vs. Non-Religious Participants | Group | Count | Min PHQ9 | Median PHQ9 | SD PHQ9 | Max PHQ9 |
|---|---|---|---|---|---|---|
| Religious/Spiritual | 47 | 0 | 3 | 5.53 | 20 | |
| Non-Religious/Spiritual | 7 | 4 | 9 | 6.21 | 20 |
Table 2 summarizes the distribution of PHQ-9 depression scores among participants categorized as Religious/Spiritual (n = 47) versus Non-Religious/Spiritual (n = 7). Reported values include the minimum, mean, median, standard deviation, and maximum scores within each group. Participants identifying as Religious/Spiritual demonstrated notably lower depressive symptom severity, with a mean PHQ-9 score of 5.02 (SD = 5.53) compared to 11.3 (SD = 6.21) in the Non-Religious/Spiritual group. These findings suggest a potential inverse association between self-identified religiosity and depression severity in this cohort.
| Mean PHQ-9 Depression Scores in Religious vs. Non-Religious Participants (N = 54) | Group | Mean PHQ9 | p-value |
|---|---|---|---|
| Religious/Spiritual | 5.021277 | 0.0018 | |
| Non-Religious/Spiritual | 11.285714 |
Table 3 reports the mean PHQ-9 scores and corresponding p-value from a statistical comparison between participants who self-identified as Religious/Spiritual (n = 47) and Non-Religious/Spiritual (n = 7). The Religious/Spiritual group exhibited a significantly lower mean PHQ-9 score (M = 5.02) compared to the Non-Religious/Spiritual group (M = 11.29), with the difference reaching statistical significance (p = 0.0018). These results suggest a meaningful association between religious/spiritual identification and reduced depressive symptom burden within this cohort.
| By PHQ-9 Scores and Resilience by Ethnicity | Ethnicity | Count | Mean PHQ9 | Std Dev PHQ9 | Mean Resilience | Std Dev Resilience |
|---|---|---|---|---|---|---|
| White/non-Hispanic | 2 | 4.50 | 4.95 | 91.00 | 18.38 | |
| Hispanic/Latin | 16 | 4.94 | 5.28 | 82.75 | 19.85 | |
| Black/African American | 33 | 6.76 | 6.43 | 80.55 | 23.85 | |
| Other | 3 | 1.33 | 1.53 | 79.33 | 18.5 |
Table 4 presents the mean and standard deviation of PHQ-9 depression scores and CD-RISC-25 resilience scores, stratified by participant-reported race/ethnicity. Black/African American participants exhibited the highest mean PHQ-9 scores, indicating greater depressive symptom severity, followed by Hispanic/Latin participants. In contrast, White/non-Hispanic participants had the highest average resilience scores. These findings highlight variation in mental health and psychological resilience across racial and ethnic subgroups within the sample.
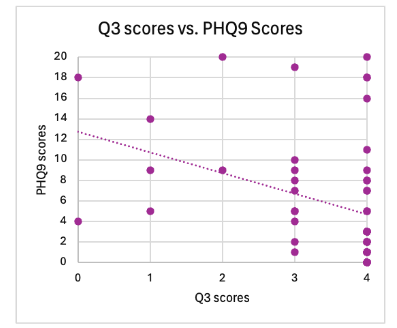
Figure 1 presents the results of a Pearson correlation analysis examining the relationship between religiosity/spirituality (CD-RISC Q3 score) and depression severity (PHQ-9 score). The analysis revealed a statistically significant inverse correlation (r = 0.357, p = 0.007), indicating that higher levels of religiosity/spirituality self-reported religiosity were associated with lower depressive symptoms. Religiosity accounted for approximately 12.78% of the variance in PHQ-9 scores.
| Logistic Regression, examining the relationship between Demographic Characteristics, Religiosity/Spirituality and HIV Viral Load Suppression | Effect | Point Estimate | 95% Wald Confidence Limits (Lower) | 95% Wald Confidence Limits (Upper) |
|---|---|---|---|---|
| Non-Religious/Spiritual | 0.349 | 0.065 | 1.892 | |
| Age | 1.013 | 0.960 | 1.068 | |
| Black/African American | 2.623 | 0.142 | 48.443 | |
| Hispanic/Latina | 4.030 | 0.174 | 93.477 | |
| Other Racial/Ethnic Group | 6.138 | 0.074 | 511.761 |
This logistic regression model using Firth’s penalized likelihood method examined associations between selected covariates and the odds of being virally suppressed (< 200 copies/mL vs >= 200 copies/mL). Compared to religious/spiritual participants, participants categorized as non-religious/spiritual had lower odds of being suppressed (OR = 0.35; 95% CI: 0.07 1.89; p = 0.222), though the confidence interval was wide. Age was not significantly associated with suppression (OR = 1.01; 95% CI: 0.96 1.07; p = 0.638), however increasing age trended towards HIV VL suppression. In summary, none of the predictors were statistically significant at the 0.05 level. Compared to White, non-Hispanic participants, Black participants had more than twice the odds of being suppressed (OR = 2.62; 95% CI: 0.14 48.44), and Hispanic and other racial/ethnic groups had even higher estimated odds (Hispanic OR = 4.03; 95% CI: 0.17 93.48; Other OR = 6.14; 95% CI: 0.07 511.76) of being unsuppressed.
Discussion
In this study of women with HIV and a recent history of care non-adherence, higher self-reported religiosity/spirituality was significantly associated with lower depressive symptom severity, as measured by the PHQ-9. Specifically, those who endorsed religion or spirituality as a source of strength had PHQ-9 scores that were, on average, more than six points lower than those who did not. This finding aligns with a growing body of literature suggesting that spirituality and religious engagement may offer psychological benefits, particularly for individuals navigating chronic illnesses such as HIV.
Our correlation analysis revealed a modest but statistically significant, inverse relationship between religiosity and depressive symptoms (r = 0.357, p = 0.007), supporting prior work identifying faith and spirituality as potential protective factors against psychological distress. The mechanisms proposed in earlier studies such as increased hope, resilience, perceived social support, and meaning-making are also plausible mediators in our sample, all of which have been found to mitigate depressive symptoms among people with HIV.
Importantly, our cohort was composed primarily of women from historically marginalized backgrounds, with 61.1% identifying as Black/African American and 29.6% as Hispanic/Latina. Historically marginalized populations frequently encounter intersecting structural barriers including poverty, systemic racism, stigma, and healthcare access inequities that elevate risk for poor mental health and treatment disengagement. Despite these elevated risks, participants who identified as religious/spiritual reported lower depressive symptom scores, and resilience scores were generally high across racial and ethnic groups.
Among Hispanic/Latin participants, the mean PHQ-9 score was 4.94 (n = 16), which was lower than that of Black/African American participants (mean = 6.76, n = 33), and slightly higher than that of the small White/non-Hispanic (mean = 4.5, n = 2) and Other (mean = 1.33, n = 3) subgroups. Although not statistically significant among Black participants, the observed trends mirror findings in the literature, suggesting that religious coping may confer cross-cultural benefits, though these may manifest differently based on sociocultural context and denominational traditions.
Our statistical model (logistic regression) identified several relationships between demographic variables (race/ethnicity, low religiosity/spirituality) and HIV viral load suppression. However, estimates were imprecise and not statistically significant, likely due to the limited sample size. Findings suggest possible trends in the relationship between race, spirituality, and suppression outcomes, but further investigation in larger samples is warranted.
Beyond depressive symptoms, emerging research has also linked religiosity to improved HIV-related clinical outcomes, such as higher rates of viral suppression, improved ART adherence, and more consistent engagement in care. For example, studies have found that individuals with strong spiritual beliefs are more likely to maintain regular clinical appointments and report fewer missed doses of antiretroviral therapy. One longitudinal study reported that increased spirituality was independently associated with improved viral suppression over time, even after adjusting for psychosocial confounders such as depression and substance use.
These findings suggest a potential mediating effect of spirituality on the mental health HIV care cascade, wherein reduced depressive symptoms may facilitate better treatment adherence, leading to improved virologic outcomes. This is particularly relevant in high-risk populations, where comorbid depression has been repeatedly shown to negatively impact ART adherence, CD4 count, and viral load. As such, interventions that strengthen coping and psychological resilience through culturally salient means such as faith-based practices may represent a valuable and underutilized avenue for optimizing both mental and physical health outcomes.
Given these observations in prior literature, our findings point to the potential utility of integrating faith-based interventions into HIV clinical care, especially for populations where religion is a central element of identity. Faith-based partnerships have been successfully leveraged in prior public health efforts, including diabetes prevention, cancer screening, and maternal health in African American and Latinx communities. Tailored interventions such as church-based mental health workshops, peer-led spirituality groups, and chaplain integration into HIV clinics could facilitate culturally competent outreach, reduce mental health stigma, and enhance engagement in both psychiatric and HIV care.
Moreover, training faith (spiritual/religious) leaders to serve as mental health liaisons or adherence counselors may be a particularly cost-effective and community-driven approach to intervention. These leaders help foster trust within their communities, and with appropriate training, could serve as bridges between biomedical and psychosocial models of care. Of note, in our study, White, non-Hispanics are a minority and this parallels the general population of women with HIV in the clinic. White/non-Hispanics often have worse HIV-related clinical outcomes in the clinic.
Nevertheless, several limitations warrant discussion. Our relatively small sample size, especially for the non-religious subgroup (n = 7), limits generalizability and increases susceptibility to type II error. Our use of a single-item measure of religiosity (Q3 from CD-RISC-25) may not fully capture the complex, multidimensional nature of religious and spiritual life. Multidimensional instruments such as the Brief Multidimensional Measure of Religiousness/Spirituality (BMMRS) or the Spiritual Well-Being Scale may offer greater sensitivity in future studies. Additionally, as our data were collected cross-sectionally, we cannot infer causality or temporal sequence. It remains possible that individuals experiencing fewer depressive symptoms are more inclined to identify with religious beliefs, or that a third variable such as social support mediates the observed associations.
Despite these caveats, the consistency of our findings with prior literature and the strength of observed effects suggest that spirituality may represent a valuable psychosocial asset in HIV care. It remains crucial for future work to explore these associations longitudinally and within larger, more demographically diverse cohorts.
Conclusion
This study adds to a growing body of evidence highlighting a significant association between self-reported religiosity/spirituality and reduced depressive symptoms among women with HIV, particularly those with histories of care non-adherence. Participants who identified their faith as a source of strength consistently demonstrated lower PHQ-9 scores, suggesting that spirituality may serve as a protective factor against psychological distress in high-risk populations. Beyond mental health, our findings align with emerging research indicating that religiosity may also support improved clinical outcomes, including greater ART adherence and viral suppression. These dual mental and physical health benefits reinforce the importance of viewing spirituality not as peripheral, but as integral to culturally sensitive, holistic HIV care. For Black and Hispanic women groups disproportionately affected by HIV, faith-informed interventions may offer a meaningful way to enhance engagement, adherence, and overall well-being.
To better understand these effects, future research should explore the mechanisms through which spirituality confers resilience such as emotion regulation, social support, meaning-making, or behavioral activation. Larger, prospective studies using multidimensional measures of both religiosity and depression are needed. As healthcare systems advance toward integrative, patient-centered models, acknowledging spiritual dimensions of care may be key to addressing disparities and improving long-term outcomes for people living with HIV.
Conflict of Interest Statement:
The authors declare no conflicts of interest related to this study.
Funding Statement:
This study received external funding from the NIH National Institute of Drug Abuse. Research activities also received institutional support from the University of Miami Miller School of Medicine.
Acknowledgements:
The authors would like to thank the staff and patients at the participating HIV care clinic in South Florida for their time and invaluable contributions to this research. We also extend our gratitude to the University of Miami Miller School of Medicine for providing the resources necessary to complete this study.