





Outcomes of Rhomboid Flap for Sacrococcygeal Disease
Outcome of Rhomboid Flap for a controversial affair “The Sacrococcygeal Pilonidal disease”. An Eastern Hospital Experience
Introduction
Pilonidal sinus disease was first reported in the year 1880. Its etiology has been a debate for close to two centuries. It is perhaps the only disease condition that has evolved with multiple names in history. After many deliberations spanning decades a consensus may have been established on its etiology & pathogenesis, however the same cannot be said for an optimal modality universally accepted surgical treatment worldwide.
Ironically even today it is viewed by many surgeons as an underrated & unmerited procedure hence it continues to be as a handed down to the junior most team member among the surgical hierarchy.
In an era where Data is not mere information and information does not imply knowledge. With every great advance in surgical technology and techniques Sacral pilonidal disease will continue to ignite & flare the age old debate of the optimal surgical operative procedure that can be universally accepted as standardized worldwide. As an author we strongly feel that the disease condition merits an overhaul review among the surgical fraternity.
Pilonidal disease was first reported by Herbert Mayo a British Surgeon (1833)¹, as a congenital condition with sinus containing hair follicles located in the sacrococcygeal region of a female patient. The term pilonidal was coined by Richard Hodges which is derived from Latin pilus referring to hair and nidus nest. Hodges was a proponent of the congenital theory for pilonidal sinus disease. His belief was three factors were essential for the development of sacral Pilonidal disease, the congenital coccygeal dimple, the presence of abundant hair, and poor hygiene. Among others the proponents of neurogenic theory were Gage M² who were of the opinion that the persistence of neural canal elements were responsible for the development of this disease condition. The controversy pertaining to its name it acquired continued for decades!³˒⁴ The Neural canal theory gained grounds under the assumption that the persistence of caudal remnants of the neural tube or the dermal inclusions from sequestrated epithelial structures⁵ were responsible for this disease process. It was only the work of Patey and Scarff (1946) who demonstrated that it was in fact a granulomatous tract secondary to follicle free hair penetration, that the acquired theory gained acceptance and is the most widely held view today.
The term pilonidal cysts will continue to be shrouded as a misnomer as the cyst wall is not lined with squamous epithelium but are composed of vascular pyogenic granulation tissue¹. It is interesting to note that anal and ischiorectal abscesses although anatomically related never develop tufts or pits of hair like the pilonidal sacral disease. The most plausible explanation for this is the negative or vacuum effect created by a deep sacral natal cleft during mobility that the hair migration & lodging is exclusively restricted to sacral pilonidal disease process.
It is a disease with substantial impact on the psyche of the young adults affected socially and economically considering its high recurrence rates. Perhaps it is time to give the devil its due.
The estimated incidence is 26 per 1,00,000 people in US⁶. In the acute stage the presentation is in the form of an infected cyst, abscess with discharging active tracts or as dormant, midline natal pit openings. It is a painful condition prevalent among those aged 15-30 years, with a 3:1 male-to-female ratio⁷, it occurs after puberty, when sex hormones surge affect the apocrine bearing pilosebaceous gland and body hair growth in general. Predisposing factors to pilonidal disease include the following Obesity, Sedentary lifestyle, Smoker⁸˒⁹, Deep natal cleft, a family history of pilonidal disease, Occupational like dog & sheep shearers, barbers¹⁰˒¹¹ those with hirsute body habitus a poor personal hygiene¹²˒¹³
The most common site affected are the axilla, sacral region, the umbilicus, Intermammary breast cleft, the digits of the hands and rarely genitals both vulva and the penis¹⁴.
It uncommonly involves those over forty years of age¹⁵˒¹⁶. The term Chronic pilonidal disease is used for patients that have undergone at least one pilonidal abscess drainage procedure and continue to have a residual pilonidal sinus tract clinically seen as discharging pus. Recurrent disease is referred to disease process occurring after a period of healing & is characterised by new pit formation. Chronic Sacral Pilonidal disease has a significant impact on the individuals psyche both on the personal front & their social life. The surgical rate of recurrence for this particular disease is high 30%. The choice of the surgical procedure therefore has a definite effect on the quality of life viz Shorter hospital stay, earlier healing, shorter time off work, lower ratio of complications are the main advantages of flap techniques¹⁷ when compared to other procedures.
A recent Swedish study reported the cost of a conventional wide excision and closure for a pilonidal sinus to be EUR 6222 per patient with a recurrence rate of 32% at 5 years¹⁸ perhaps it is time to finally give sacral pilonidal disease its merit sans reservation.
Endoanal pilonidal sinus is a rare variety of pilonidal disease that affects the perianal skin directly or may occur circumferentially around the anus, involving the skin of the anal verge first, this pilonidal sinus may tract down caudally, creating a perianal fissure or fistula communicating with the anal canal.
This disease condition is prevalent in different regions of Saudi Arabia. This study was therefore undertaken to report the regional prevalence of Sacral Pilonidal disease in the Eastern regional Hospital of the province and highlight the myriad of treatment options that currently available in its management.
Material and Methods
This retrospective study was undertaken at Al Omran General Hospital following an Ethical and IRB approval. A total of 35 patients were recruited following fulfilment of inclusion criteria. All subjects were operated on by the same surgical team, from 2019 – 2023.
PRIMARY OBJECTIVE: The Rhomboid flap is the ideal Flap Surgical Procedure for Sacral Pilonidal disease
SECONDARY OBJECTIVE: To ensure a dressing free for adults with Sacral PNS disease.
Data analysis
The collected data was entered & computer analysed using SPSS software, version 17 (SPSS Inc, Chicago). Descriptive data has been presented as percentage for qualitative variables, whereas the quantitative data were presented as graphs with tables.
Procedure
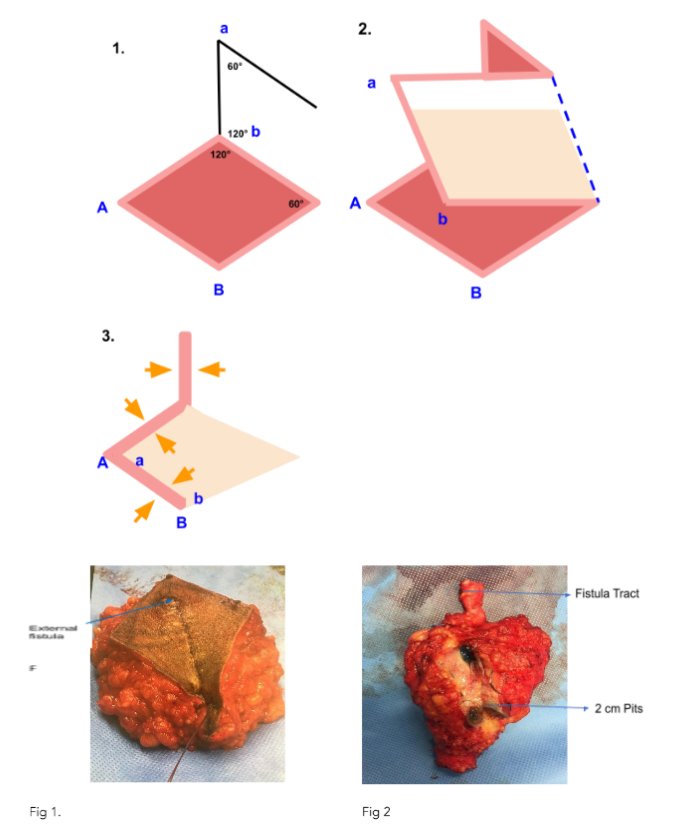
The patient was placed prone after spinal or GA. A rhombus was marked over the sacral pilonidal sinus disease in such a way that all midline pits and lateral tracts are covered with the long axis of the rhombus¹⁹ The gluteal region were strapped apart with adhesive tape. The reference point A was placed in such that the lateral diseased tissue tracts are palpated and included with the line of excision of the rhomboid flap. All sides of the Rhombus are of equal length. The opposite angles however are 120 degree and 60 degree respectively. Methylene blue dye was injected through the external opening of the sinus tracks to outline the intracutaneous tracts and all sinus tracks were excised using both visual and palpation technique of fibrous tracts by the digit of the operating surgeon. The use of Intraoperative methylene blue decreased recurrence rate from 16% to 30%²⁰ The skin and subcutaneous fat is then incised down to deep sacral fascia. Once the diseased tissue is excised in a rhomboid shape manner the subsequent flap raised from the opposite side should include the skin, subcutaneous fat, and the fascia overlying gluteus maximus. This flap is then trans positioned to cover the midline rhomboid defect in such a way that the point a is inset to point A (Figs. 1 and 2), and the point b to B. Deep absorbable sutures are then placed in a two layered fashion over a vacuum drain directed cephalad with a negative suction the edges of the skin are approximated using 3-0 non absorbable sutures. The final shape of this flap should appear as the figure 3 in the diagram. The drains were removed after 48 hrs provided the output was less than 30 ml/day. Sutures were removed on 9-10th postoperative day. A Surgical OPD follow up examination was scheduled at the end of the first month, then the three month, at the end of six months and finally end of one year. The mean hospital stay in days, wound infection, seroma formation, hypoesthesia, the days to return back to work & recurrence if any were recorded at each follow up in Clinic.
Results
In this study of 35 patients 28 were males and 7 were females. Mean age was 24 years (range 15–29 years). Of the 35 patients, 19 had primary disease, 6 had recurrent disease, and 10 subjects had previous incision and drainage procedure for sacral pilonidal abscess. Average age was 24 years—the oldest was 45 years and the youngest was 14 years. The males out numbered the females 28 vs 7. Fifty four percent had the disease process in the second decade of their life. Only six among the males were smokers. Eighty three percent of the patients were obese.
Three female subjects had complications—one had flap necrosis and the other two had persistent serous discharge from the wound. It took 3 weeks for both to heal completely. Three patients had flap Oedema, which resolved by 10 days. One had persistent discharge at the tip which took 4 weeks to heal. The time taken to ambulate post operatively was 2-4 days.The average hospital stay for our patients was 3-5 days, the reason was post operative pain and drain output more than 30cc. The postoperative pain score was 5-6 out of 10 on a Universal Pain Score tool Chart. The time taken to return to work was 4 weeks.
Hypoaesthesia was common in the majority of the subjects. The most common organism isolated from wound swabs was staphylococcus. No recurrence was reported at the end of a year follow up. None needed readmission due to recurrent pilonidal disease. All patients had a dressing free life by the fourth postoperative week.
Although recurrence are common²⁰, the disease condition can be reduced worldwide by performing a flap procedure either a Limbergs flap, Karydakis flap or a Bascome procedure. On an average for flap based procedures worldwide the length of stay ranged from three to six days²¹. The shorter the hospital duration with earlier return to work the more likely the surgical procedure may be regarded a success. The Limbergs flap procedure has been reported to have lower infection & recurrence rates, a shorter hospital stay and better aesthetic results when compared to other procedures²⁰–²² The reported recurrence rate for Limberg flap is 2.5%²³˒²⁴ Advancement flaps like V-Y plasty the reported recurrence rate are less than 10 % whereas for Z-flaps 2-10% and for W-flaps anywhere from 0–16%²¹–²⁴.
QUANTITATIVE DATA
Fig 8
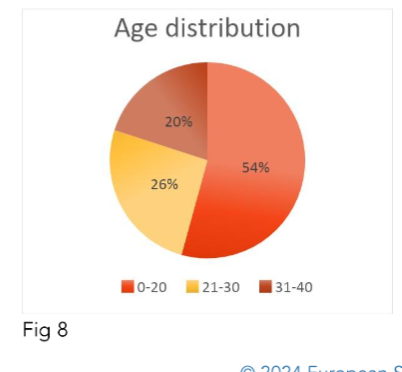
Fig 9
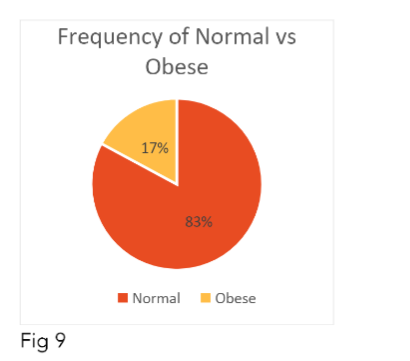
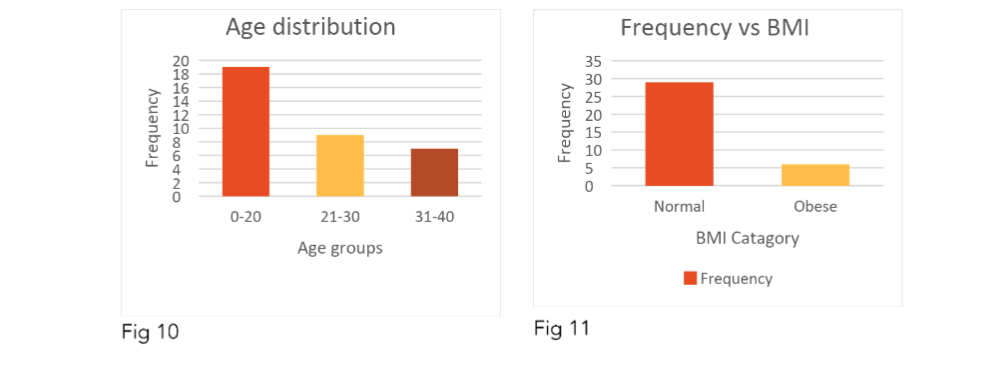
Table 1.
| Parameter | Findings | Remarks |
|---|---|---|
| Age | 2-4 Decade | |
| Sex | M 28 | F 7 |
| BMI | Obese 83% | |
| Smoker | M 6 | F 0 |
| Pre OP Dressing | 6 months – 3 yrs | |
| Sacral PNS Sinus | 1-5 openings | |
| Wound Infection | ||
| Seroma Cellulitis Necrosis Site | 1 | Resolved 2 weeks |
| Dehiscence | 2 | Flap Tip |
| 3 | ||
| 0 | ||
| Revision Sx | 0 | |
| Post Op Pain Score | 5-6/10 | |
| Duration Stay | 3-5 days | |
| Cosmetic Scar Satisfaction | 31 yes 4 No | Females unsatisfied when compared to males |
| Scar outcome 2yr | Hypertropic Scar 3 | |
| Hypoesthesia Flap | 35 | Resolved by 3 months |
| Compliance | Yes | |
| Return to work | 2-3 weeks | |
| Follow Up | 2-3 weeks | 3 months 6months then yearly for 2 years |
| Dressing free life | 2-3 weeks | |
| Recurrence | Nil at 2 year. |
Discussion
Although real pathogenesis is unknown, the aetiology is assumed to be related to trapped hair follicles. The hair within the cyst originates from the surrounding tissue and is follicle free! Based on the fact that these hair from the lower back and even the scalp continue to be found within the granulation and scar tissue. Hence it is considered a chronic inflammatory disease characterized by a foreign body like reaction secondary to lose hairs trapped in the natal cleft. The disease process is a product of microtrauma, penetration, maceration followed by infection in an anaerobic environment and this ultimately leads to sinus formation with pits aligned along the midline²⁵.These pits in sacral pilonidal disease are stretched out epidermal hair follicles that measure 1-3mm in size²⁵˒²⁶. The pits contain the loose hair sans the follicle component that act like barbs that are drilled, propelled, finally imbibed into the subcutaneous tissues along sinus tracts and find their final resting place in pits.
The entry is ‘one way’ tip first thereby preventing them from expulsion as has been confirmed using light microscopy²⁶.It is this orientation of the hair that motivates them to be steered deeper into the subcutaneous tissue²⁷. The mechanism has been proposed to vacuum forces and negative suction created by a deep natal cleft. This suction draws hair and debris into the midline pits²⁶. During standing, the bones lift away initially pulling away from soft tissues thereby creating a vacuum effect²⁸.This subcutaneous vacuum is formed both during repeated standing and sitting. In sitting, the pilonidal opening is pushed closed and the cavity is compressed, creating pressure that drives contents through fat to eventually rupture through sacral skin as secondary openings.
The reason for the chronicity of this clinical disease is the colonising of these wounds by anaerobic bacteria²⁹. The anaerobic bacteria in a hypoxic environment induce collagen accumulation that is proposed to delay normal healing process³⁰˒³¹.The reason for recurrence is the retention of the midline pores that initiate most original pilonidal abscesses. Excessive skin removal leading to wound tension are other contributing factors in recurrences.
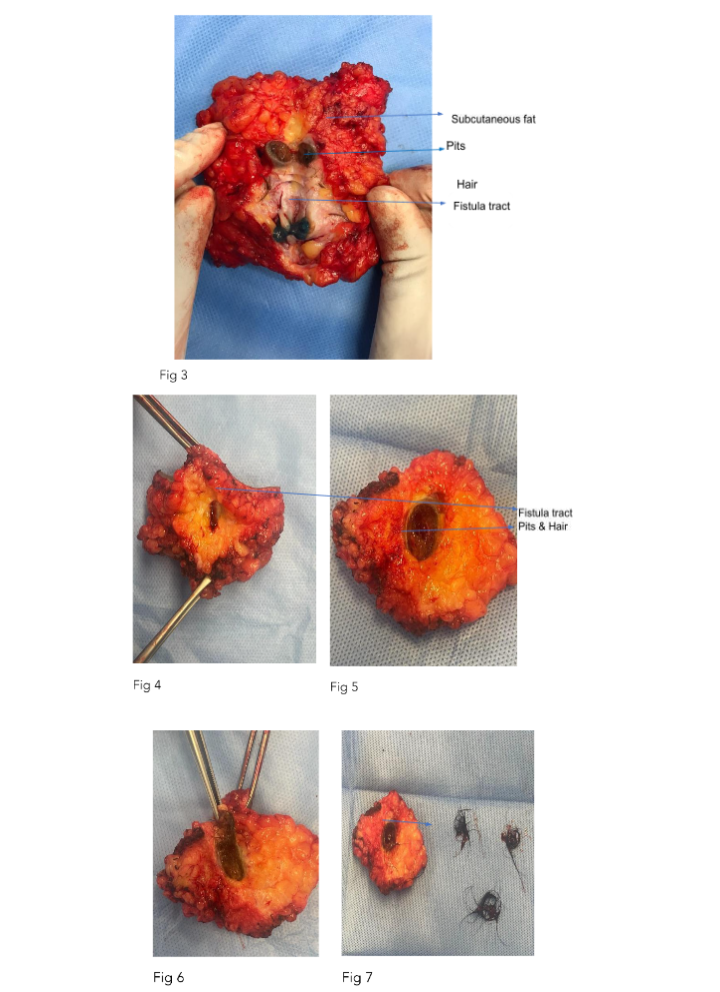
Extensions of these pit cavities lead to sinus tracts formation that are essentially composed of a primary canal lined by squamous cells that begins from the sinus orifice in the skin. The Canals located posterior to the primary canal are secondary canals that are lined by granulation tissue. The abscesses form in secondary canals and then progress to primary canals. Loose Hairs are located in both the primary canal and secondary canals. The other components with hair include keratin flakes & hemosiderin stained macrophages³². The number of hairs correlate to the duration of the disease process, it is not unusual to see tufts of hair within the pits (fig 2) or protruding from sinus tracts. Interestingly It is unusual for these tracts to end on to the coccyx. If Pilonidal sinus tracts encroach on to the coccyx bone Coccygeal osteomyelitis can develop as a rare complication³³˒³⁴.
It is the directional growth of the hair follicle that in majority upto 90% of times is the reason the sinus tracts are located cephalad in direction in which case tracking follicle should approximately be 5-8 cm from the anus. Rarely should the sinus be located caudally the tracking follicle will lie 4-5 cm from the anus. A fistula in ano therefore ought to be considered prior to commencing treatment³⁵.
The race, ethnicity, coarseness and pattern of the hair type straight or kinked including the medullation are important contributors influencing both the development and persistence of chronic sacral pilonidal disease. The individuals of white ethnicity being more affected compared to other races due the fact that the volume of sweat and the number of sweat glands are more predominant in the former when compared to those of African or Asian origin³⁶. Rarely the infection from these long standing tracts involves the coccyx as coccygitis in which case a flap procedure ensures complete excision of the pits with tracts and the coccyx tip bone³⁴.
FOLLICULAR OCCLUSION HYPOTHESIS Pilonidal disease is condition of the hair follicles secondary to follicular occlusion³⁵˒³⁶. The central pathological event in these conditions is thought to be follicular hyperkeratosis leading to obstruction of the infundibulum of a hair follicle that causes dilated and rupture. The secondary events are infection abscesses and the formation of fistulae & tracts³⁷.
The pilonidal cyst disease is frequently associated with Hidradenitis Suppurativa in 30% cases³⁸. The name follicular occlusion tetrad refers to pilonidal cyst disease Hidradenitis Suppurativa, Acne conglobate & dissecting cellulitis of the scalp³⁹. A given patient may have two or more disorders within the tetrad.
Pilonidal cyst disease and Hidradenitis Suppurativica share remarkable clinical and histologically similarities. It has even been suggested that pilonidal cyst is a unlocalized type of hidradenitis suppurativa. A closer link between these disease processes are the end result of the shared alterations of hairs⁴⁰ both these clinical conditions share.
Long standing chronic inflammatory sacral pilonidal disease has been reported to transform to malignancy⁴¹˒⁴².
KARYDAKIS HYPOTHESIS (1970) The fistulae secondary to free hairs that perforate the intact skin⁴². The loose hair can be from the head and neck hairs are fragmented and follicle free⁴³ that find their place in the subcutaneous tissue by implantation in the natal cleft and get dragged deeper into the subcutaneous tissue. The keratin flakes of these hairs function as spurs or barbs that facilitate unidirectional movement⁴²˒⁴³
BASCOM HYPOTHESIS that hyperkeratosis, obstruction, and follicular rupture are the primary events and that the hairs only secondarily come to lie in the preformed openings²⁵. The migration of free hairs by movement of the gluteal musculature leads to negative pressure in the pilonidal sinus was shown experimentally²⁹. The fact that pilonidal disease can arise in the interdigital space of hairdressers seems rather to confirm the theory of Karydakis.
Worldwide the treatment can be divided into two broad categories Conservative and non Conservative.
EPILATION OF HAIR If the primary source is hair epilation of hair may be used as a primary or adjunct treatment in the absence of abscess for Acute Sacral Pilonidal disease. This epilation may take the form of shaving, waxing, laser, or use of creams.
ROLE OF SHAVING- Ritual therapy in the form of weekly shaving a 5cm strip from the anus to the rectum, combined with hygiene education, resulted in decreased operations, and near normal work status⁴⁴. The use of operative techniques in conjunction with shaving skin weekly or biweekly to keep the gluteal cleft free from hair for three to six months also resulted in a good outcome. In the long term however the outcome was not so favorable⁴⁵.
ROLE OF PHENOL AS SCLEROSING AGENT IN SACRAL PILONIDAL DISEASE. Historically phenol was used as a sclerosing agent in the form of liquid or as crystals primarily as non operative form of management in early 1964⁴⁴. It has a reported success rate of 80% with a recurrence of 8.3%⁴⁶The disadvantages include multiple applications Multiple one to four sessions of hair removal with or without cyst curettage.
INCISION AND DRAINAGE Primarily first line treatment in acute presentations of sacral pilonidal sinus disease. If the wound is Curettage to remove dead or infected tissue tracts ninety % achieved completely healed at one month, compared to fifty eight % at 10 weeks with no curettage.
Disadvantage- 10–15% will have abscess recurrence. If the incision and drainage procedure is done prior to definitive surgery the long term recurrence rates are lower sixteen % recurrence rate in the I&D group versus thirty four % recurrence in the primary open treatment group.
EXCISION AND HEALING BY SECONDARY INTENTION It is not cost effective & is inconvenient to patient, time lost from work with persistence of wound and long term dressing with healing time over 2-3 months⁴⁷. Excision and primary closure produces high rates of recurrence 10-15% in the first year.
The German worldwide guideline on pilonidal disease states explicitly that excision and Midline closure are to be avoided due to an increased rate of wound complication and increased recurrence rate⁴⁸. The lower recurrence rate are associated with off midline procedures, such as flap procedures like a Limberg or Rhomboid flap with faster wound healing with return to normal activity and work. Hence a Minimal excision and primary suture is a cost efficient definitive treatment for pilonidal disease with low morbidity.
Recently a nonsurgical option that has been proposed is the use of platelet-rich plasma (PRP). Platelet-rich plasma is derived from autologous blood that is centrifuged and contains a high concentration of platelets and growth factors; it has been used in many subspecialties for its proposed wound healing properties and regenerative factors⁴⁹. The long term results of this modality for treatment evaluated 138 patients with follow up of 60.2 months has reported a success rate of 97.1% after the first month & a recurrence rate of 8.2% at 60.2 months; the mean healing time was 13.3 days, with 82.6% complete healing of tissue. The method includes preparing PRP using 40 cc of the patient’s blood, and once in the gel form the procedure was introduced under local anaesthesia in the outpatient setting.
A meta-analysis of randomized controlled trials of the rhomboid flap versus primary closure concluded that the rhomboid flap was superior to primary closure⁵⁰.
A randomized control study comparing the Limberg flap, to primary closure and deep suturing reported improved wound healing, decreased hospital stay, earlier return to work, and decreased recurrence⁵¹˒⁵³ Another more recent randomized control trial of 200 patients reported less postoperative pain, earlier mobilization, decreased hospital stay, with fewer complications employing the Limberg flap compared to primary closure.
The disadvantage of primary closure techniques is the increased likelihood of dehiscence, distortion of key structures, poor cosmetic outcomes, or less than total graft acceptance. In these situations, local flaps with the pliability, matching texture and color become the best option⁵². Among such flaps, a rhomboid flap is a versatile option for reconstruction.
“THE RECONSTRUCTION LADDER PRINCIPLE” FOR DEFECT CLOSURE.
The reconstruction ladder principle dictates that when considering the options for reconstruction of the defect the use of simple procedure ought to be considered first followed by an increasing complex procedure in a step ladder fashion.
Principle of wound closure ought to ensures a reduction of dead space with even distribution of the tissue pressure in a tension free manner that is cosmetically appealing.
The Limberg flap or rhomboid flap design was first described by Professor Alexander Alexandrovich Limberg of Leningrad, who devoted his life in pursuit of an ideal flap design (1948). The Limberg flap is a transposition & allows for a tension free closure of the rhomboid-shaped defect and the donor site. A rhomboid flap is fashioned as a parallelogram with two angles of 120° & the other two angles of 60°. All the sides of this parallelogram are equal hence theoretically four flaps can be sited from one rhomboid (Fig. 1).
The blood supply of this transposition flap is papillary and sub dermal plexuses based. Larger sized rhomboid flaps may rely on perforator vascular supply. A reduction in tension on the flap decreases the likelihood of flap necrosis along edges. The flap should be positioned in the direction of minimal tension and maximum extensibility. The principles of surgery remain applicable during planning and placement of incisions parallel to Relaxed skin tension lines (RSTL) to ensures the final scar falls within the creases of the skin & along lines of maximal extensibility.
This flap has versatile application and is described for both male and females, children of any age & ethnicity. Its versatile application include use in facial, breast, trunk, hand, eyelid, even perianal and oncological reconstructions. This off midline procedure therefore flattens the natal cleft and reduces distortion of tissues²⁶. The disadvantage is the lower part of the wound crosses the natal cleft and is the common site of wound breakdown and recurrences in some cases. The reason for breakdown include gluteal cleft maceration of the skin, ischemia and tension of the tissue flap inset. A modification of this technique is the modified limbergs flap whereby the flap is modified the technique so that the lower end of the flap lies completely outside the natal cleft.The general outcome of a Limbergs flap in worldwide literature are good⁵³ The alternative flap procedures that can be considered are the Karydakis flap & Bascom I & II procedure.
KARYDAKIS FLAP
The Karydakis flap is designed as off the midline to flatten the natal cleft by performing a sliding type flap following an oblique excision of all pilonidal tracts & sinus down to the presacral fascial plane. The wound is closed in layers so that the final scar is lateral & vertical. The recurrence rate reported was less than 1% on 5000 patients over a period of twenty years. The wound complication rate in their series reported at 9%.Other studies report a recurrence rate of 3–5%⁵⁴.
LIMBERGS/RHOMBOID FLAP
This flap procedure is advocated for flattening of natal cleft by excision of the primary sinus, tracts & secondary tracts with a rim of cutaneous tissue in a rhomboid shaped fashion. The advantages are lower post operative pain, reduced infection with low seroma formation when compared to traditional Karydakis flap⁵⁵. The disadvantages include a long scar flap⁵¹.
The site where the wound crosses the natal cleft is the usual site of the wound breakdown leading to recurrence therefore a current preferred modification is to use an off line based Limbergs flap procedure viz to inset the flap such that lower end of the flap lies outside the natal cleft. The benefit is reduced complications and thereby reduce recurrences⁵⁶.
Other advantages of this flap include good hygiene maintenance, reducing sweating maceration, erosions, and scar formation. This flap procedure found better than simple excision and closure or marsupialization Newer flap procedures include bascoms I & II surgery. Unfortunately there are no long term studies comparing the outcome of Bascoms flap to Limbergs procedure.
BASCOM I PROCEDURE OR BASCOMS SIMPLE SURGERY.
A minimally Invasive procedure that involves the removal of secondary hair follicles using a mini 5 mm incision. The principle includes excision of the infected epithelialized sinus pit using mini incisions thereby minimizing the extent of the midline wound. A lateral incision just parallel to the mini incisions, is made to curette the debris from the cavity connecting the sinus pits with removal of the primary & secondary tracts. All incisions are left open to heal by secondary intention. A follow-up period of over 3 years had a 16% recurrence rate with a healing time of approximately three weeks⁵⁷. As it is minimally invasive the postoperative pain is less.
BASCOM II PROCEDURE also called Cleft Lift or Cleft Closure described in 1987 uses incision, drainage and curettage through a lateral incision combined with excision of midline pits and a small amount of surrounding tissue⁵⁷. A section of the cavity wall opposite the incision, lateral to the midline, is raised as a flap to close the defect. This is accomplished by suturing the flap to the underside of the skin bridge formed between the incision and the midline.
Post Op 6% developed abscesses recurrence rates 10%⁵⁸.
Role of Hygiene & Shaving
Armstrong and Barcia hypothesis (1994) Wide, meticulous shaving is equal and superior to surgical therapy⁵⁹. The individuals who are high risk such as the morbid obese, hirsute and those with poor personal hygiene⁵⁹, Shaving alone has been advocated as the sole alternative treatment for pilonidal disease as an alternative Conservative approach to surgery. There is however no consensus on the timing and frequency of shaving weekly versus monthly. The role of hygiene for sacral pilonidal disease is imperative as it continues to be a decisive risk factor affecting outcome in the post operative period⁶⁰˒⁶¹
VY Flaps
It is a fascio cutaneous advancement flap⁶⁰˒⁶³. It was introduced as early as the 1960s for the management of Sacral Pilonidal disease. It is a feasible option usually deployed by Cosmetic surgeons. It involves excision of the sinus combined using a full-thickness V shaped in. Its final repair flap in the shape of a V with the ultimate post repair suture line giving the flap appears Y in shape. The advantages include feasibility for large defects, similar to surrounding gluteal contour. The disadvantage includes discontent & dissatisfaction in upto 90% of subjects and multiple cosmetic surgery follow up.
Role of laser
Laser treatment for hair removal has been suggested as an alternative to shaving [59]. Laser epilation has been used in pilonidal disease with mixed results. The overall recurrence rate for 60 patients treated with laser therapy as an adjunct to surgery was found to be 13.3%⁶³. A long term follow up of 4.8 years was required for laser as adjunct to surgery to reduce this recurrence rate. Some disadvantages included Pain, Cost, multiple treatment sessions and rashes that were seen in up to 40% of patients⁶⁴. New modifications include the SiLaC procedure Sinus Laser assisted Closure and SMILE procedure Sinus Pilonidal Minimally Invasive Laser Excision.
Role of Vaccum dressing
Due to its notorious chronicity a few studies have investigated on the role of vaccum dressing for chronic sacral pilonidal disease.Vaccuum dressings applied after laying open the sinuses for sacral pilonidal disease have not been shown to be significantly better than simple dressings⁶⁵˒⁶⁶
The Role of Minimally Invasive Surgery (MIS) in Sacral Pilonidal disease
MIS Endoscopic pilonidal sinus treatment (EPSiT) first described by Meinero⁶⁶ in 2014, along with Video Assisted Ablation of Pilonidal Sinus (VAAPS) by Milone⁶⁷ are minimally invasive techniques that target the root cause of the disease process at its entry viz hair invagination driving the pathogenesis of pilonidal sinus disease.
Once the sinus cavity and the secondary canals are identified hair follicles are removed under direct vision using endoscopic forceps followed by cautery ablation of the granulation tissue. The advantages include less pain, patient satisfaction early return to work and less recurrences. Disadvantages include Cost and Multiple sessions and Surgeon Learning curve.
Malignant transformation
Chronic discharging sacral pilonidal disease if neglected and left untreated for a prolonged period of time can transform into malignancy. The first reported case was by Wolff H in 1900⁶⁸ The most frequent tumor type is squamous cell carcinoma⁶⁹.Other tumor types reported are basal cell carcinoma, adenocarcinoma and mixed squamous and basal carcinoma⁷⁰. The reason cited is release of free oxygen radical that induces neoplastic transformation through genetic damage⁷⁴, other causes include Inflammation to Metaplasia transformation theory⁶⁹˒⁷⁰. Immunosuppression and human papilloma virus infection may also be predisposing factors that accelerate the transformation process⁷¹. Currently there is no role for Prophylactic inguinal node dissection⁷³–⁷⁵.
Recurrence rates post resection are 50% and usually appear 9–16 months after surgery. Adjuvant radiotherapy decreases local recurrence to 30%. The role of adjuvant chemotherapy not defined.
Conclusion
Sacral Pilonidal Disease affair will continue to be Shrouded in controversies. The communication network between general practitioner the primary care provider and the dermatologist needs to be re evaluated as an early involvement of the Surgical fraternity implies decreasing the burden of cost associated with Chronic dressings that spans over decades an efficient & effective disease outcome by resolution with cure and patient satisfaction by giving his a dressing free Quality of life. It is time for General Surgeons to be familiar with flap based procedures. Classical Limbergs flap or Off line Limbergs flap are a safe first line surgical option based on the Reconstruction Ladder Principle.
Alexanders Limbergs flap will continue to be a formidable versatile Universal choice of procedure for Sacral Pilonidal Disease.
Conflict of Interest:
None
Funding Statement:
None.
Acknowledgements:
None.
Orchid ID:
Reconnaissance
Concept & Design¹
Supervision Approval of Manuscript¹˒²˒⁴
Data Acquisition⁵˒⁶˒⁷˒⁸˒⁹
Data Analysis with Interpretation¹⁰˒¹¹˒¹²˒¹³˒¹⁴
Critical Review²˒³
Administrative Technical Editor¹⁵˒¹⁶˒¹⁷˒¹⁸˒¹⁹
Statistician³
Sourire en Signe de Reconnaissance
To Dr Khathija Hasan for review & final editing the manuscript.
References
[1].Davage The origin of sacrococcygeal pilonidal sinuses based on an analysis of four hundred sixty-three cases. Am J Pathol. 1954 Nov-Dec;30(6):11 91-205.
[2].Buie LA. Jeep disease. South Med J. 1944;37 :103–109.
[3].Gage M. Pilonidal sinus: sacrococcygeal ectodermal cysts and sinuses. Ann Surg. 1939;109:291–303.
[4].Patey DH, Scarff RW. Pathology of postanal pilonidal sinus; its bearing on treatment. Lancet. 1946;2:484–486.
[5].Sondenaa K, Andersen E. Patient characteristics and symptoms of in chronic pilonidal sinus disease. Int J Colorectal Dis. 1995;10(1):39–42. doi: 10.1007/BF00337585.
[6].Spivak H, Brooks VL, Nussbaum M, Friedman I. Treatment of chronic pilonidal disease. Dis Colon Rectum. 1996 Oct. 39 (10):1136-9.
[7].Lesalnieks I, Deimel S, Zülke C, Schlitt HJ. Smoking increases the risk of pre- and postoperative complications in patients with pilonidal disease. J Dtsch Dermatol Ges. 2013 Oct;11(10):1001-5. doi: 10.1111/ddg.12140. Epub 2013 Aug 15. PMID: 23945165.
[8].Latunde Dada AO, Lee-Elliott CE, Carpenter TT. A rare case of vulval pilonidal sinus diagnosed on ultrasound. J Obstet Gynaecol. 2013 Feb;33(2):211-2.
[9].Kushwaha P, Merritt A, Aslam MB. A rare case of vulval pilonidal sinus: incidental diagnosis. BMJ Case Rep. 2015 Jul 27;2015.
[10].K. Ballas, K. Psarras, S. Rafailidis, et al.Interdigital pilonidal sinus in a hairdresser J. Hand Surg., 31 (3) (2006), pp. 290-2.
[11].Al-Qassim Z, Reddy K, Khan Z, Reddy IS. Pilonidal sinus cyst of the penis: a rare manifestation of a common disease. BMJ Case Rep. 2013 May 21;2013:bcr2013009718. doi: 10.1136/bcr-2013-009718. PMID: 23697453; PMCID: PMC3670004.
[12].Shanmugathas N, Yassin M, Ross C, Minhas S. Pilonidal Sinus Disease of the Penis: A Case Report and Review of the Literature. Andrologia. 2021;53 (1):e13837. doi:10.1111/and.13837
[13].A.Hammood Z, Abdullah H et al. Pilonidal Sinus of Breast, a Case Report with Literature Review. Ann Med Surg (Lond). 2022;73:103138. doi:10.1016/j.amsu.2021.103138
[14].R. Burney Treatment of pilonidal disease by minimal surgical excision under local anesthesia with healing by secondary intention: results in over 500 patients Surgery, 164 (6) (2018), pp. 1217-1222
[15].Clothier PR, Haywood IR. The natural history of the post anal pilonidal sinus. Ann R College Surg England. 1984;66(3):201–203.
[16].Khodakaram, K., Stark, J., Höglund, I., & Andersson, R. E. (2017). Minimal excision and primary suture is a cost-efficient definitive treatment for pilonidal disease with low morbidity: a population-based interventional and a cross-sectional cohort study. World journal of surgery, 41, 1295-1302.
[17].Doll D, Novotny A, Rothe R, Kristiansen JE, Wietelmann K, Boulesteix AL, Düsel W, Petersen S. Methylene Blue halves the long-term recurrence rate in acute pilonidal sinus disease. Int J Colorectal Dis. 2008 Feb;23(2):181-7.
[18].Cihan A, Ucan BH, Comert M, Cesur A, Cakmak GK, Tascilar O. Superiority of asymmetric modified Limberg flap for surgical treatment of pilonidal disease. Dis Colon Rectum 2005;49:244-9.
[19].Ertan T, Koc M, Gocmen E, Aslar K, Keksek M, Kilic M. Does technique alter quality of life after pilonidal sinus surgery? Am J Surg 2005; 190: 388–92.
[20].Schoeller T, Wechselberger G, Otto A, Papp C. Definite surgical treatment of complicated recurrent pilonidal disease with a modified fascio cutaneous V-Y advancement flap. Surgery 1997; 121: 258–63.
[21].Azab AS, Kamal MS, Saad RA, Abou al Atta KA, Ali NA. Radical cure of pilonidal sinus by a transposition rhomboid flap. Br J Surg 1984; 71: 154–5.
[22].Topgül K, Ozdemir E, Kilic K, Gökbayir H, Ferahköşe Z (2003) Log-term results of Limberg procedure for treatment of pilonidal sinus: a report of 200 cases. Dis Colon Rectum 46:1545–1548
[23].Bascom J. Pilonidal disease. Origin from follicles of hairs and results of follicle removal as treatment. Surgery 1980;87:567–72.
[24].Stelzner F. [Causes of pilonidal sinus and pyoderma fistulans sinifica Langenbecks Arch Chir. 1984;362(2):105-18.
[25].Dahl HD, Henrich MH. [Light and scanning electron microscopy study of the pathogenesis of pilonidal sinus and anal fistula]. Langenbecks Arch Chir. 1992;377(2):118-24.
[26].Gosselink MP, Jenkins L, Toh JWT, Cvejic M, Kettle E, Boadle RA, Ctercteko G. Scanning electron microscope imaging of pilonidal disease. Tech Coloproctol. 2017 Nov;21(11):905-906.
[27].Brearley R Pilonidal sinus: a new theory of origin. Br J Surg. 1969;1362- 67
[28].Marks JHarding KGHughes LE Staphylococcal infection of open granulating wounds. Br J Surg. 1987;7495- 97
[29].Hunt TkConolly WBAronson SBGoldstein P Anaerobic metabolism and wound healing: a hypothesis for the initiation and cessation of collagen synthesis in wounds. Am J Surg. 1978;135328- 332
[30].Allen DBMaguire JJMahdavien M et al. Wound hypoxia and acidosis limit neutrophil bacterial killing mechanisms. Arch Surg. 1997; 132991- 996.
[31].Lord PH Millar DM Pilonidal sinus: a simple treatment. Br J Surg. 1965;52298- 300
[32].Coccygeal osteomyelitis managed with wide excision, coccygectomy and perineal musculature reconstruction, with Limberg flap for defect closure. Mugdha Kowli, Pranav Mandovra et al World journal of colorectal surgery 2019:8;1;27-29.
[33].Dill DB, Yousef MK, Goldman A, Hillyard SD, Davis TP. Volume and composition of hand sweat of White and Black men and women in desert walks. Am J Phys Anthropol. 1983 May;61(1):67-73. doi: 10.1002/ajpa.1330610107. PMID: 6869514.
[34].Plewig G, Kligman AM. Berlin Springer-Verlag: 1975. Acne Morphogenesis and treatment; pp. 192–193.
[35].Von Laffert M, Stadie V, Ulrich J, Marsch WC, Wohlrab J. (2011). Morphology of pilonidal sinus disease: some evidence of its being a unilocalized type of hidradenitis suppurativa. Dermatology. 223:349–355.
[36].C orman ML, Nicholls RJ, Fazio VW, Bergamaschi R. Corman’s Colon and Rectal Surgery. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2012. 195-203.
[37].Scheinfeld NS. A case of dissecting cellulitis and a review of the literature. Dermatol Online J. 2003;9:8.
[38].Luiz Fernando Nunes, Antonio Kneipp Pitta de Castro Neto et al, Carcinomatous degeneration of pilonidal cyst with sacrum destruction and invasion of the rectum An Bras Dermatol. 2013 Nov-Dec; 88(6 Suppl 1): 59–62.doi: 10.1590/abd1806-4841. 20132140.
[39].Lerner HJ, Deitrick G. Squamous cell carcinoma of the pilonidal sinus: Report of a case and review of the literature. J Surg Oncol. 1979;11:177–183.
[40].Karydakis GE. Easy and successful treatment of pilonidal sinus after explanation of its causative process. Aust N Z J Surg. 1992;62:385–389.
[41].Bosche F, Luedi MM, van der Zypen D, Moersdorf P, Krapohl B, Doll D. The hair in the sinus: sharp-ended rootless head hair fragments can be found in large amounts in pilonidal sinus nests. World J Surg. 2018;42:567–573.
[42].Johnson EK, Vogel JD, Cowan ML, Feingold DL, Steele SR., Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons. The American Society of Colon and Rectal Surgeons’ Clinical Practice Guidelines for the Management of Pilonidal Disease. Dis Colon Rectum. 2019 Feb;62(2):146-157.
[43].Armstrong JH, Barcia PJ. Pilonidal sinus disease. The conservative approach. Arch Surg. 1994 Sep;129(9):914-7; 917-9.
[44].Sevinç B, Damburacı N, Karahan Ö. Long term results of minimally invasive treatment of pilonidal disease by platelet rich plasma. J Visc Surg. 2020 Feb;157(1):33-35.
[45].Maurice Ba, Greenwood Rk. A Conservative treatment of pilonidal sinus. Br j surg. 1964 Jul;51:510-2.
[46].Kaymakcioglu N, Yagci G, Simsek A, Unlu A, Tekin OF, Cetiner S, Tufan T. Treatment of pilonidal sinus by phenol application and factors affecting the recurrence. Tech Coloproctol. 2005 Apr;9(1):21-4.
[47].Enriquez-Navascues J., Emparanza J., Alkorta M. Meta-analysis of randomized controlled trials comparing different techniques with primary closure for chronic pilonidal sinus. Tech. Coloproctol. 2014;18[10]:863.
[48].Lesalnieks I, Ommer A, Petersen S, Doll D, Herold A. German national guideline on the management of pilonidal disease. Langenbecks Arch Surg. 2016 Aug;401(5):599-609. doi: 10.1007/ s00423-016-1463-7. Epub 2016 Jun 16. PMID: 27311698.
[49].Horwood J., Hanratty D., Chandran P. Primary closure or rhomboid excision and Limberg flap for the management of primary sacrococcygeal pilonidal disease? A meta-analysis of randomized controlled trials. Colorectal Dis. 2012;14(2):143–151.
[50].Abu Galala KH, Salam IM, Abu Samaan KR, El Ashaal YI, Chandran VP, Sabastian M, Sim AJ. Treatment of pilonidal sinus by primary closure with a transposed rhomboid flap compared with deep suturing: a prospective randomised clinical trial. Eur J Surg. 1999 May;165(5):468-72.
[51].Akca T, Colak T, Ustunsoy B, Kanik A, Aydin S. Randomized clinical trial comparing primary closure with the Limberg flap in the treatment of primary sacrococcygeal pilonidal disease. Br J Surg. 2005 Sep;92(9):1081-4.
[52].Townsend J. A template for the planning of rhombic skin flaps. Plast. Reconstr. Surg. 1993;92(5):968–971.
[53].Mentes O, Bagci M, Biglin T, Ozgul O, Ozdemir M. Limberg flap procedure for pilonidal sinus diseased: results of 353 patients. Langenbecks Arch Surg. 2008;393(2):185–189. doi: 10.1007/s00423-007-0227-9.
[54].Kitchen PR. Pilonidal sinus: Experience with the Karydakis flap. Br J Surg 1996;83(10):1452–55
[55].Wolfe SA. Alexander A. Limberg, M.D. 1894–1974. Plast Reconstr Surg 1975;56(2):239–40.
[56].Bali İ, Aziret M, Sözen S, et al. Effectiveness of Limberg and Karydakis flap in recurrent pilonidal sinus disease. Clinics (Sao Paulo) 2015;70(5):350–55. doi: 10.6061/clinics/2015(05)08.
[57].Bascom J. Pilonidal disease: long-term results of follicle removal. Dis Colon Rectum. 1983; 26(12):800–807.
[58].Senapati A., Cripps N.P.J., Thompson M.R. Bascom’s operation in the day‐surgical management of symptomatic pilonidal sinus. BJS. 2000;87(8):1067–1070.
[59].Dupuis A, Christou N, Teterycz D, Balaphas A, Robert-Yap J, Zufferey G, Skala K, Alketbi M, Liot E, Buchs NC, Roche B, Ris F. Sacro-coxxygial hygiene, a key factor in the outcome of pilonidal sinus surgical treatment? BMC Surg. 2021 Apr 17;21(1):197. doi: 10.1186/s12893-021-01204-4. PMID: 33865363; PMCID: PMC8052720
[60].Pronk A, Eppink L, Smakman N, Furnee E. The effect of hair removal after surgery for sacrococcygeal pilonidal sinus disease: A systematic review of the literature. Tech Coloproctol 2018:22(1):7–14. doi: 10.1007/s10151 -017-1722-9.
[61]. Orem Y, Kahraman F, Karincaoğlu Y, Koyuncu E. Evaluation of 60 patients with pilonidal sinus treated with laser epilation after surgery. Dermatol Surg. 2010;36(1):88-91.
[62].McDermott FT. Pilonidal sinus treated by Z-plasty. Aust N Z J Surg. 1967 Aug 01;37(1):64-9.
[63]. Sungur N, Koçer U, Uysal A, Arslan C, Cöloglu H, Ulusoy G. V-Y rotation advancement fasciocutaneous flap for excisional defects of pilonidal sinus. Plast Reconstr Surg. 2006 Jun;117(7):2448-54.
[64].Badawy EA, Kanawati MN. Effect of hair removal by Nd:YAG laser on the recurrence of pilonidal sinus. J Eur Acad Dermatol Venereol. 2009 Aug;23(8):883-6.
[65]. Humphries AE, Duncan JE. Evaluation and management of pilonidal disease. Surg Clin North Am 2010;90(1):113–24. doi: 10.1016/j.suc.2009.09.006.
[66].Khanna A, Rombeau JL. Pilonidal disease. Clin Colon Rectal Surg 2011;24(1):46–53. doi: 10.1055/s -0031-1272823.
[67].Meinero P., Mori L., Gasloli G. et al Endoscopic pilonidal sinus treatment (E.P.Si.T) Tech. Coloproctol. 2014;18:389–392.
[68].Milone M., Musella M., Di Spiezio Sardo A et al, Video-assisted ablation of pilonidal sinus: a new minimally invasive treatment-A pilot study. Ann Surgery. 2014;155:562–566.
[69].Malek MM, Emanuel PO, Divino CM.et al, Malignant degeneration of pilonidal disease in an immunosuppressed patient: report of a case and review of the literature. Dis Colon Rectum. 2007;50:1475–7.
[70].Borges VF, Keating JT, Nasser IA, et al, Clinicopathologic characterization of squamous-cell carcinoma arising from pilonidal disease in association with condylomataacuminatum in HIV-infected patients: report of two cases. Dis Colon Rectum. 2001;44:1873–7.
[71].De Bree E., Zoetmulder F.A., Christodoulakis M. et al Treatment of malignancy arising in pilonidal disease. Ann. Surg. Oncol. 2001;8(19):60–64.
[72].Williamson J, Silverman FJ, Tafra L et al, Fine-needle aspiration cytology of metastatic squamous-cell carcinoma arising in a pilonidal sinus, with literature review. Diagn Cytopath. 1999;20:367–70.
[73].Pilipshen SJ, Gray G, Goldsmith E, Dineen P et al Carcinoma arising in pilonidal sinuses. Ann of Surg. 1981;193:506–12.
[74].Almeida JC. A curative cryosurgical technique for advanced cancer of sacrococcygeal pilonidal sinuses. J Surg Oncol. 2012;106:504–8.
[75].Ramazan E., Tuna B., Ismail O et al. Recurrent squamous cell carcinoma arising in a neglected pilonidal sinus: report of a case and literature review. Int. J. Exp. Med. 2014;7(2):446–450.
Most read articles by the same author(s)
- Dr. Uwais Riaz Ul Hasan, Dr. Khathija Hasan, Dr. Moath AbdulAziz AlMasoud, Dr. Abdul Rahman Al Ghannam, Dr. Shehla Riaz Ul Hasan, Dr. Hafiz Mansoor Ul Haq, Dr. Yaser Attia, Dr. Ammar Al Sulaiman, Dr. Amith Ibrahim, Dr. Aissa Saidi, Dr. Mohammed AbdulMajeed Alghadeer, Dr. Manar Abubaker Ahmed Bahammam, Dr. Ali AbdulMajeed Alghadeer, Dr. Walaa Essa Al Mubarak, Dr. Abdullah Mohammed Albin AlSheikh, Heba Abdullah Alisaleh, Eman Hussain AlBasrawi, Porocarcinoma “A Masquerader as Left InfraClavicular mass” A case report with review of literature , Medical Research Archives: Vol 12 No 8 (2024): Vol 12 No 8 (2024): August ISSUE, Issue 8, VOl.12